
Incidence of Cancer in Patients with Irritable Bowl Syndrome

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
2.2. Study Population
2.3. Study Outcomes and Covariates
2.4. Statistical Analyses
3. Results
3.1. Basic Characteristics of the Study Sample
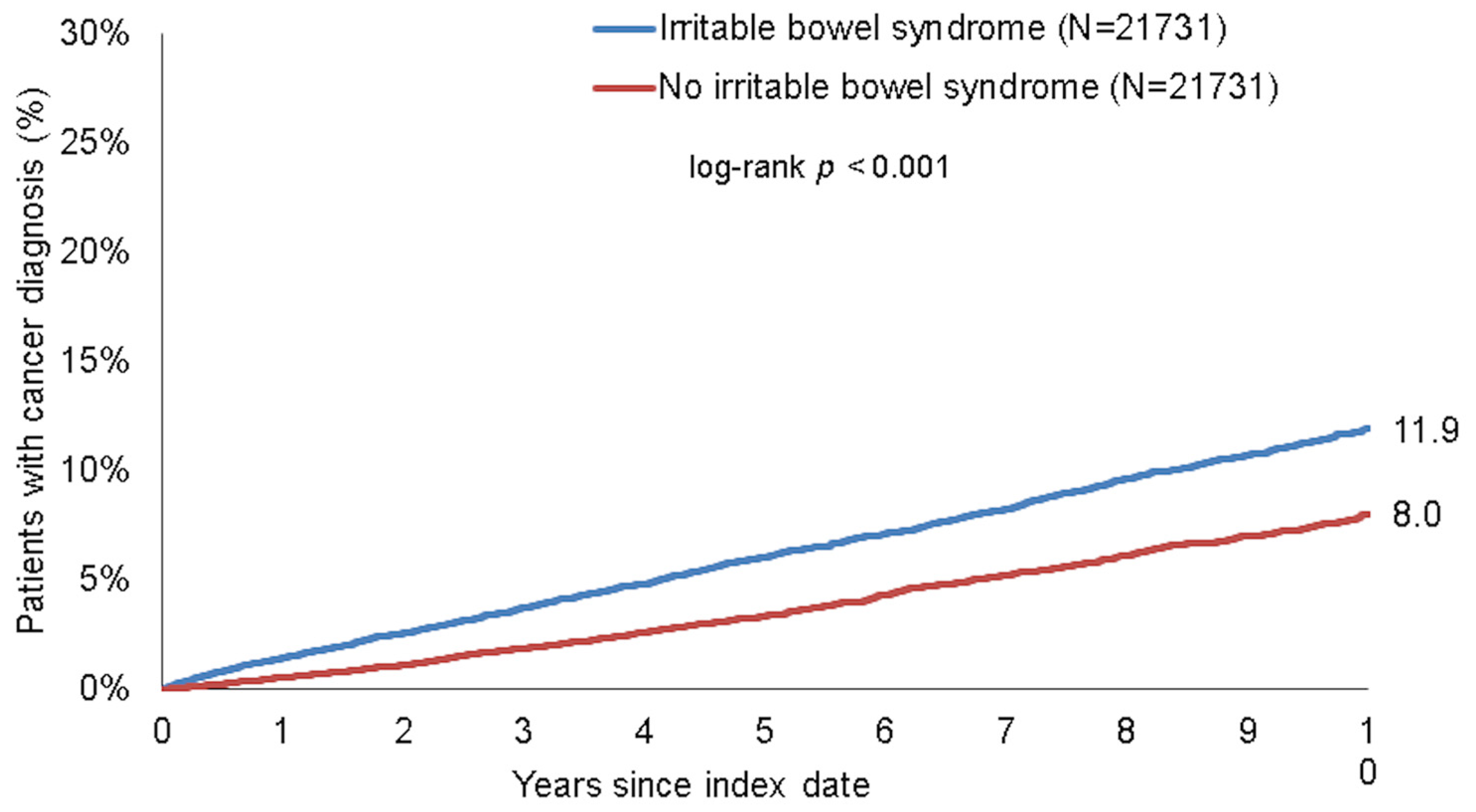
3.2. IBS Is Associated with an Increased Incidence of Cancer
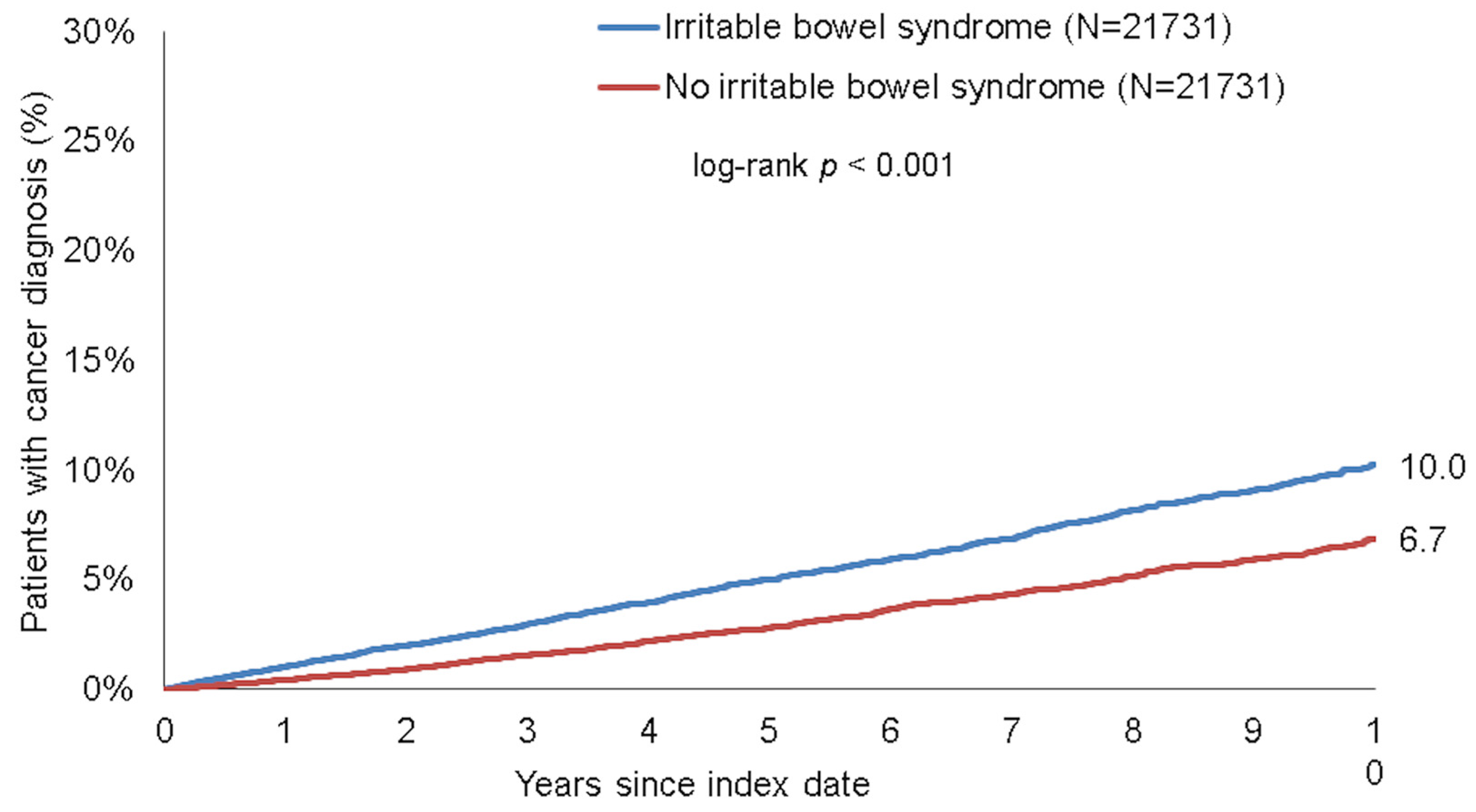
3.3. Association between IBS and Cancer of Digestive Organs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ford, A.C.; Sperber, A.D.; Corsetti, M.; Camilleri, M. Irritable bowel syndrome. Lancet 2020, 396, 1675–1688. [Google Scholar] [CrossRef]
- Layer, P.; Andresen, V.; Pehl, C.; Allescher, H.; Bischoff, S.C.; Classen, M.; Enck, P.; Frieling, T.; Haag, S.; Holtmann, G.; et al. Irritable bowel syndrome: German consensus guidelines on definition, pathophysiology and management. Gastroenterology 2011, 49, 237–293. [Google Scholar] [CrossRef]
- Palsson, O.S.; Whitehead, W.E.; van Tilburg, M.A.; Chang, L.; Chey, W.; Crowell, M.D.; Keefer, L.; Lembo, A.J.; Parkman, H.P.; Rao, S.S.; et al. Rome IV Diagnostic Questionnaires and Tables for Investigators and Clinicians. Gastroenterology 2016, 13, S0016–S5085. [Google Scholar] [CrossRef]
- Mearin, F.; Lacy, B.E.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel Disorders. Gastroenterology 2016, 150, 1393–1407. [Google Scholar] [CrossRef] [Green Version]
- Spiller, R.; Garsed, K. Infection, inflammation, and the irritable bowel syndrome. Dig. Liver Dis. 2009, 41, 844–849. [Google Scholar] [CrossRef] [PubMed]
- Bercik, P.; Verdu, E.F.; Collins, S.M. Is irritable bowel syndrome a low-grade inflammatory bowel disease? Gastroenterol. Clin. N. Am. 2005, 34, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Lazaridis, N.; Germanidis, G. Current insights into the innate immune system dysfunction in irritable bowel syndrome. Ann. Gastroenterol. 2018, 31, 171–187. [Google Scholar] [CrossRef]
- Sheikhesmaili, F.; Jalili, A.; Taghizadeh, E.; Fakhari, S.; Jalili, K.; Ghaderi, E.; Rahimi, E. The CCL28 levels are elevated in the serum of patients with irritable bowel syndrome and associated with the clinical symptoms. Am. J. Clin. Exp. Immunol. 2021, 10, 23–29. [Google Scholar]
- Yang, X.L.; Liu, K.Y.; Lin, F.J.; Shi, H.M.; Ou, Z.L. CCL28 promotes breast cancer growth and metastasis through MAPK-mediated cellular anti-apoptosis and pro-metastasis. Oncol. Rep. 2017, 38, 1393–1401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashidiani, S.; Jalili, A.; Babaei, E.; Sheikhesmaeili, F.; Fakhari, S.; Ataee, P.; Parhizkar, B. The chemokine CCL28 is elevated in the serum of patients with celiac disease and decreased after treatment. Am. J. Clin. Exp. Immunol. 2017, 6, 60–65. [Google Scholar]
- Hu, L.Y.; Ku, F.C.; Lu, T.; Shen, C.C.; Hu, Y.W.; Yeh, C.M.; Tzeng, C.H.; Chen, T.J.; Chen, P.M.; Liu, C.J. Risk of cancer in patients with irritable bowel syndrome: A nationwide population-based study. Ann. Epidemiol. 2015, 25, 924–928. [Google Scholar] [CrossRef] [PubMed]
- Norgaard, M.; Farkas, D.K.; Pedersen, L.; Erichsen, R.; de la Cour, Z.D.; Gregersen, H.; Sorensen, H.T. Irritable bowel syndrome and risk of colorectal cancer: A Danish nationwide cohort study. Br. J. Cancer 2011, 104, 1202–1206. [Google Scholar] [CrossRef] [PubMed]
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, S.; Kostev, K. Basic characteristics and representativeness of the German Disease Analyzer database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Zingel, R.; Bohlken, J.; Riedel-Heller, S.; Barth, S.; Kostev, K. Association Between Low-Density Lipoprotein Cholesterol Levels, Statin Use, and Dementia in Patients followed in German General Practices. J. Alzheimer’s Dis. 2021, 79, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Jacob, L.; Loosen, S.H.; Kalder, M.; Luedde, T.; Roderburg, C.; Kostev, K. Impact of the COVID-19 Pandemic on Cancer Diagnoses in General and Specialized Practices in Germany. Cancers 2021, 13, 408. [Google Scholar] [CrossRef]
- Huber, Y.; Labenz, C.; Michel, M.; Worns, M.A.; Galle, P.R.; Kostev, K.; Schattenberg, J.M. Tumor Incidence in Patients with Non-Alcoholic Fatty Liver Disease. Dtsch. Ärzteblatt Int. 2020, 117, 719–724. [Google Scholar] [CrossRef]
- Sperber, A.D.; Dumitrascu, D.; Fukudo, S.; Gerson, C.; Ghoshal, U.C.; Gwee, K.A.; Hungin, A.P.S.; Kang, J.Y.; Minhu, C.; Schmulson, M.; et al. The global prevalence of IBS in adults remains elusive due to the heterogeneity of studies: A Rome Foundation working team literature review. Gut 2017, 66, 1075–1082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holtmann, G.J.; Ford, A.C.; Talley, N.J. Pathophysiology of irritable bowel syndrome. Lancet Gastroenterol. Hepatol. 2016, 1, 133–146. [Google Scholar] [CrossRef]
- Aguilera-Lizarraga, J.; Florens, M.V.; Viola, M.F.; Jain, P.; Decraecker, L.; Appeltans, I.; Cuende-Estevez, M.; Fabre, N.; Van Beek, K.; Perna, E.; et al. Local immune response to food antigens drives meal-induced abdominal pain. Nature 2021, 590, 151–156. [Google Scholar] [CrossRef]
- Jalanka-Tuovinen, J.; Salojarvi, J.; Salonen, A.; Immonen, O.; Garsed, K.; Kelly, F.M.; Zaitoun, A.; Palva, A.; Spiller, R.C.; de Vos, W.M. Faecal microbiota composition and host-microbe cross-talk following gastroenteritis and in postinfectious irritable bowel syndrome. Gut 2014, 63, 1737–1745. [Google Scholar] [CrossRef]
- Rinttila, T.; Lyra, A.; Krogius-Kurikka, L.; Palva, A. Real-time PCR analysis of enteric pathogens from fecal samples of irritable bowel syndrome subjects. Gut Pathog. 2011, 3, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parkes, G.C.; Rayment, N.B.; Hudspith, B.N.; Petrovska, L.; Lomer, M.C.; Brostoff, J.; Whelan, K.; Sanderson, J.D. Distinct microbial populations exist in the mucosa-associated microbiota of sub-groups of irritable bowel syndrome. Neurogastroenterol. Motil. 2012, 24, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Rajilic-Stojanovic, M.; Biagi, E.; Heilig, H.G.; Kajander, K.; Kekkonen, R.A.; Tims, S.; de Vos, W.M. Global and deep molecular analysis of microbiota signatures in fecal samples from patients with irritable bowel syndrome. Gastroenterology 2011, 141, 1792–1801. [Google Scholar] [CrossRef]
- Sundin, J.; Rangel, I.; Kumawat, A.K.; Hultgren-Hornquist, E.; Brummer, R.J. Aberrant mucosal lymphocyte number and subsets in the colon of post-infectious irritable bowel syndrome patients. Scand. J. Gastroenterol. 2014, 49, 1068–1075. [Google Scholar] [CrossRef] [PubMed]
- Dahmus, J.D.; Kotler, D.L.; Kastenberg, D.M.; Kistler, C.A. The gut microbiome and colorectal cancer: A review of bacterial pathogenesis. J. Gastrointest. Oncol. 2018, 9, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Abdulamir, A.S.; Hafidh, R.R.; Abu Bakar, F. The association of Streptococcus bovis/gallolyticus with colorectal tumors: The nature and the underlying mechanisms of its etiological role. J. Exp. Clin. Cancer Res. 2011, 30, 11. [Google Scholar] [CrossRef] [Green Version]
- Burns, C.A.; McCaughey, R.; Lauter, C.B. The association of Streptococcus bovis fecal carriage and colon neoplasia: Possible relationship with polyps and their premalignant potential. Am. J. Gastroenterol. 1985, 80, 42–46. [Google Scholar]
- Boleij, A.; Muytjens, C.M.; Bukhari, S.I.; Cayet, N.; Glaser, P.; Hermans, P.W.; Swinkels, D.W.; Bolhuis, A.; Tjalsma, H. Novel clues on the specific association of Streptococcus gallolyticus subsp gallolyticus with colorectal cancer. J. Infect. Dis. 2011, 203, 1101–1109. [Google Scholar] [CrossRef]
- Ellmerich, S.; Scholler, M.; Duranton, B.; Gosse, F.; Galluser, M.; Klein, J.P.; Raul, F. Promotion of intestinal carcinogenesis by Streptococcus bovis. Carcinogenesis 2000, 21, 753–756. [Google Scholar] [CrossRef] [Green Version]
- Gold, J.S.; Bayar, S.; Salem, R.R. Association of Streptococcus bovis bacteremia with colonic neoplasia and extracolonic malignancy. Arch. Surg. 2004, 139, 760–765. [Google Scholar] [CrossRef] [Green Version]
- Baba, Y.; Iwatsuki, M.; Yoshida, N.; Watanabe, M.; Baba, H. Review of the gut microbiome and esophageal cancer: Pathogenesis and potential clinical implications. Ann. Gastroenterol. Surg. 2017, 1, 99–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porter, C.M.; Shrestha, E.; Peiffer, L.B.; Sfanos, K.S. The microbiome in prostate inflammation and prostate cancer. Prostate Cancer Prostatic Dis. 2018, 21, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Douglass, J.; Prasath, V.; Neace, M.; Atrchian, S.; Manjili, M.H.; Shokouhi, S.; Habibi, M. The microbiome and breast cancer: A review. Breast Cancer Res. Treat. 2019, 178, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Borella, F.; Carosso, A.R.; Cosma, S.; Preti, M.; Collemi, G.; Cassoni, P.; Bertero, L.; Benedetto, C. Gut Microbiota and Gynecological Cancers: A Summary of Pathogenetic Mechanisms and Future Directions. ACS Infect. Dis. 2021, 4, 449–457. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Proportion Affected among Patients with IBS (%) N = 21,731 | Proportion affected among Patients without IBS (%)N = 21,731 | p-Value |
|---|---|---|---|
| Age (Mean, SD) | 48.4 (17.3) | 48.4 (17.3) | 1.000 |
| Age 18–40 | 34.8 | 34.8 | 1.000 |
| Age 41–50 | 20.1 | 20.1 | |
| Age 51–65 | 26.4 | 26.4 | |
| Age > 65 | 18.7 | 18.7 | |
| Women | 67.2 | 67.2 | 1.000 |
| Men | 32.8 | 32.8 | |
| Obesity | 6.7 | 6.7 | 1.000 |
| Yearly consultation frequency | 3.7 (4.1) | 3.7 (4.1) | 1.000 |
| Cohort | Proportion Affected among Patients with IBS (%) | Proportion Affected among Patients without IBS (%) | HR (95% CI) | p Value |
|---|---|---|---|---|
| Total | 11.9 | 8.0 | 1.64 (1.51–1.78) | <0.001 |
| Women | 11.4 | 7.4 | 1.68 (1.52–1.87) | <0.001 |
| Men | 13.0 | 9.3 | 1.57 (1.37–1.80 | <0.001 |
| Age 18–40 | 4.0 | 2.5 | 1.77 (1.36–2.29) | <0.001 |
| Age 41–50 | 8.9 | 6.3 | 1.48 (1.21–1.81) | <0.001 |
| Age 51–65 | 14.7 | 10.6 | 1.63 (1.42–1.86) | <0.001 |
| Age > 65 | 24.4 | 17.0 | 1.69 (1.41–1.84) | <0.001 |
| Cancer Site | Proportion Affected among Patients with IBS (%) | Proportion Affected among Patients without IBS (%) | HR (95% CI) | p Value |
|---|---|---|---|---|
| Digestive organs | 1.9 | 1.3 | 1.75 (1.42–2.14) | <0.001 |
| No digestive organs | 10.0 | 6.7 | 1.62 (1.48–1.78) | <0.001 |
| Respiratory organs | 0.7 | 0.6 | 1.17 (0.85–1.61) | 0.327 |
| Skin | 3.0 | 1.9 | 1.87 (1.55–2.24) | <0.001 |
| Female breast (women) | 2.9 | 1.7 | 1.80 (1.45–2.24) | <0.001 |
| Prostate (men) | 3.2 | 1.9 | 1.81 (1.33–2.45) | <0.001 |
| Urinary tract | 0.6 | 0.5 | 1.25 (0.87–1.78) | 0.225 |
| Lymphoid and hematopoietic tissue | 1.6 | 1.0 | 1.40 (1.12–1.75) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loosen, S.H.; Jördens, M.S.; Luedde, M.; Modest, D.P.; Labuhn, S.; Luedde, T.; Kostev, K.; Roderburg, C. Incidence of Cancer in Patients with Irritable Bowl Syndrome. J. Clin. Med. 2021, 10, 5911. https://doi.org/10.3390/jcm10245911
Loosen SH, Jördens MS, Luedde M, Modest DP, Labuhn S, Luedde T, Kostev K, Roderburg C. Incidence of Cancer in Patients with Irritable Bowl Syndrome. Journal of Clinical Medicine. 2021; 10(24):5911. https://doi.org/10.3390/jcm10245911
Chicago/Turabian StyleLoosen, Sven H., Markus S. Jördens, Mark Luedde, Dominik P. Modest, Simon Labuhn, Tom Luedde, Karel Kostev, and Christoph Roderburg. 2021. "Incidence of Cancer in Patients with Irritable Bowl Syndrome" Journal of Clinical Medicine 10, no. 24: 5911. https://doi.org/10.3390/jcm10245911