
SARS-CoV-2 Infection in Patients on Dialysis: Incidence and Outcomes in the Lazio Region, Italy

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Design and Population
2.3. Covariates
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population by Infection Status
3.2. Infected Patients Considered in the Study
3.3. Risk of SARS-CoV-2 Infection among Hemodialysis Patients and Main Risk Factors
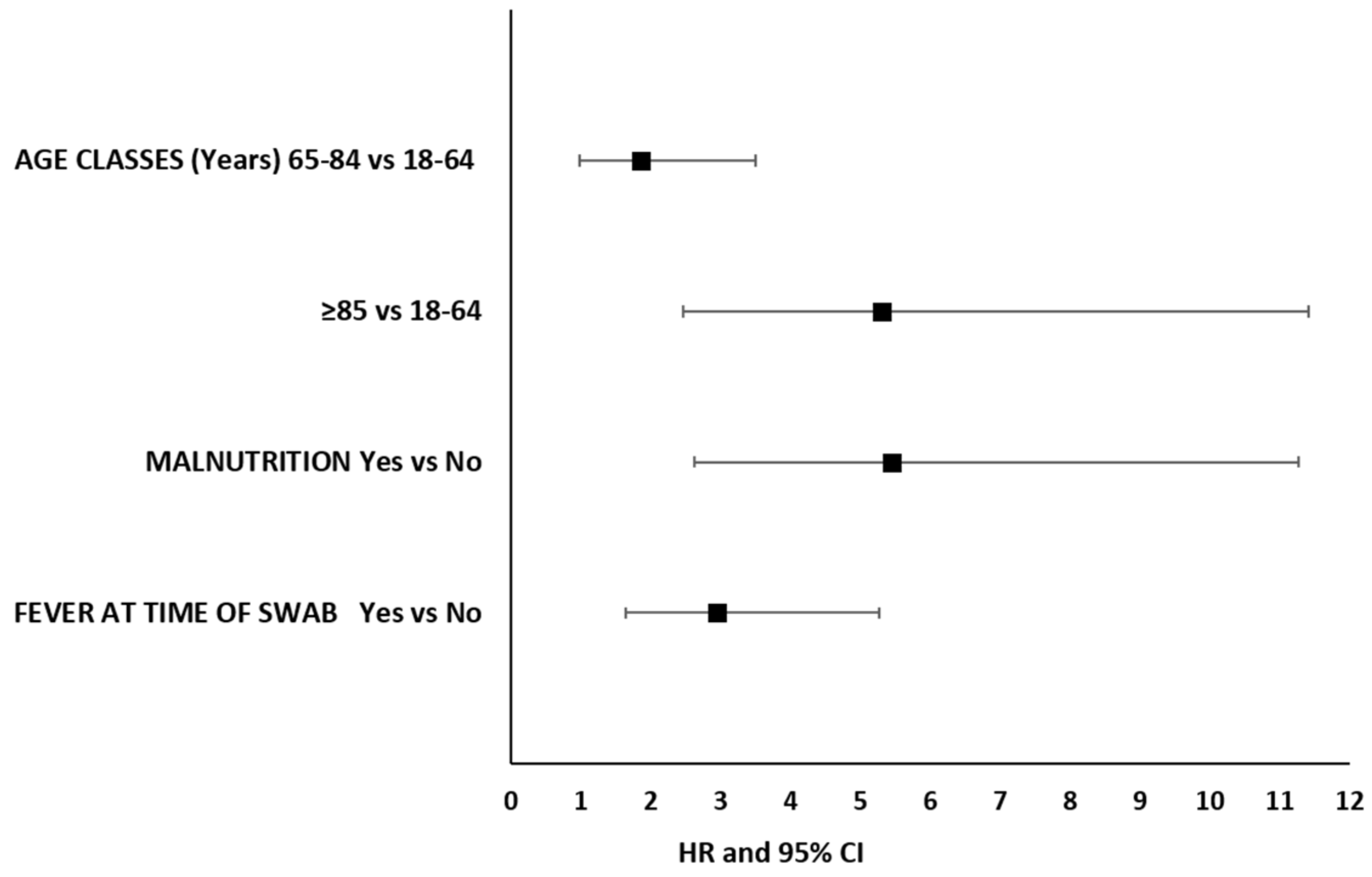
3.4. 30-Day Mortality from Infection Onset and Main Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Novel Coronavirus—China. Available online: https://www.who.int/csr/don/12-january2020-novel-coronavirus-china/en/ (accessed on 17 May 2020).
- Ghinai, I.; McPherson, T.D.; Hunter, J.C.; Kirking, H.L.; Christiansen, D.; Joshi, K.; Rubin, R.; Morales-Estrada, S.; Black, S.R.; Pacilli, M.; et al. First known person-to-person transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in the USA. Lancet 2020, 395, 1137–1144. [Google Scholar] [CrossRef]
- Chan, J.F.W.; Yuan, S.; Kok, K.H.; To, K.K.W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.Y.; Poon, R.W.S.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- WHO. Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019nCoV). Available online: https://www.who.int/newsroom/detail/30012020statementonthesecondmeetingoftheinternationalhealthregulations(2005)emergencycommitteeregardingtheoutbreakofnovelcoronavirus (accessed on 2 May 2020).
- Johns Hopkins University. Coronavirus Resource Centre. Johns Hopkins University. 2020. Available online: https://coronavirus.jhu.edu/map.html (accessed on 1 December 2020).
- Andamento Della Mortalità Giornaliera (SiSMG) Nelle Città Italiane in Relazione All’epidemia di COVID-19 Rapporto 1 Settembre 2020–6 Aprile 2021. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_3047_allegato.pdf (accessed on 15 July 2021).
- Naicker, S.; Yang, C.-W.; Hwang, S.J.; Liu, B.C.; Chen, J.H.; Jha, V. The Novel Coronavirus 2019 epidemic and kidneys. Kidney Int. 2020, 97, 824–828. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARSCoV2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Izzedine, H.; Jhaveri, K.D.; Perazella, M.A. Vascular injury and COVID-19 related mortality: What lies below the tip of the iceberg? Clin. Nephrol. 2020, 94, 11–13. [Google Scholar] [CrossRef]
- Madjid, M.; SafaviNaeini, P.; Solomon, S.D.; Vardeny, O. Potential Effects of Coronaviruses on the Cardiovascular System: A Review. JAMA Cardiol. 2020, 5, 831840. [Google Scholar]
- Hirsch, J.S.; Ng, J.H.; Ross, D.W.; Sharma, P.; Shah, H.H.; Barnett, R.L.; Hazzan, A.D.; Fishbane, S.; Jhaveri, K.D. Northwell COVID-19 Research Consortium; et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020, 98, 209–218. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Uppal, N.N.; Wanchoo, R.; Shah, H.H.; Yang, Y.; Parikh, R.; Khanin, Y.; Madireddy, V.; Larsen, C.P.; Jhaveri, K.D.; et al. COVID-19 Associated Kidney Injury: A Case Series of Kidney Biopsy Findings. J. Am. Soc. Nephrol. 2020, 31, 1948–1958. [Google Scholar] [CrossRef] [PubMed]
- Alberici, F.; Delbarba, E.; Manenti, C.; Econimo, L.; Valerio, F.; Pola, A.; Maffei, C.; Possenti, S.; Lucca, B.; Cortinovis, R.; et al. A report from the Brescia Renal COVID Task Force on the clinical characteristics and shortterm outcome of hemodialysis patients with SARSCoV2 infection. Kidney Int. 2020, 98, 20–26. [Google Scholar] [CrossRef]
- Betjes, M.G. Immune cell dysfunction and inflammation in endstage renal disease. Nat. Rev. Nephrol. 2013, 9, 25565. [Google Scholar] [CrossRef]
- Saran, R.; Robinson, B.; Abbott, K.C.; Agodoa, L.Y.C.; Bhave, N.; BraggGresham, J.; Balkrishnan, R.; Dietrich, X.; Eckard, A.; Eggers, P.W.; et al. US Renal Data System 2017 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2018, 71 (Suppl. S1), A7. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhao, M.H.; Zuo, L.; Wang, Y.; Yu, F.; Zhang, H.; Wang, H.; CKNET Work Group. China Kidney Disease Network (CKNET) 2015 Annual Data Report. Kidney Int. Suppl. 2019, 9, e1–e81. [Google Scholar] [CrossRef]
- NICE: COVID-19 Rapid Guideline: Dialysis Service Delivery, London, National Institute for Health and Care Excellence. 2020. Available online: https://www.nice.org.uk/guidance/ng160 (accessed on 15 July 2021).
- Burgner, A.; Ikizler, T.A.; Dwyer, J.P. COVID-19 and the Inpatient Dialysis Unit: Managing Resources during Contingency Planning Pre-Crisis. Clin. J. Am. Soc. Nephrol. 2020, 15, 720722. [Google Scholar] [CrossRef] [PubMed]
- Kliger, A.S.; Silberzweig, J. Mitigating Risk of COVID-19 in Dialysis Facilities. Clin. J. Am. Soc. Nephrol. 2020, 15, 707–709. [Google Scholar] [CrossRef] [PubMed]
- Basile, C.; Combe, C.; Pizzarelli, F.; Covic, A.; Davenport, A.; Kanbay, M.; Kirmizis, D.; Schneditz, D.; Sande, F.; Mitra, S. Recommendations for the prevention, mitigation and containment of the emerging SARSCoV2 (COVID-19) pandemic in haemodialysis centres. Nephrol. Dial. Transplant. 2020, 35, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Su, K.; Ma, Y.; Wang, Y.; Song, Y.; Lv, X.; Wei, Z.; Shi, M.; Ding, G.; Shen, B.; Wang, H. How we mitigated and contained the COVID-19 outbreak in a hemodialysis center: Lessons and experience. Infect. Control Hosp. Epidemiol. 2020, 41, 1240–1242. [Google Scholar] [CrossRef] [Green Version]
- Rombolà, G.; Heidempergher, M.; Pedrini, L.; Farina, M.; Aucella, F.; Messa, P.; Brunori, G. Practical indications for the prevention and management of SARSCoV2 in ambulatory dialysis patients: Lessons from the first phase of the epidemics in Lombardy. J. Nephrol. 2020, 33, 193–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annual Data Report. USRDS COVID-19 Supplement: Chapter 13. Available online: https://adr.usrds.org/2020/covid19supplement/1covid19supplement (accessed on 5 May 2021).
- Henry, B.M.; Lippi, G. Chronic kidney disease is associated with severe coronavirus disease 2019 (COVID-19) infection. Int. Urol. Nephrol. 2020, 52, 1193–1194. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; Liao, C.; He, H.; Hu, C.; Wei, Z.; Hong, Z.; Zhang, C.; Liao, M.; Shui, H. COVID-19 in Hemodialysis Patients: A Report of 5 Cases. Am. J. Kidney Dis. 2020, 76, 141–143. [Google Scholar] [CrossRef]
- Ferrey, A.J.; Choi, G.; Hanna, R.M.; Chang, Y.; Tantisattamo, E.; Ivaturi, K.; Park, E.; Nguyen, L.; Wang, B.; Tonthat, S.; et al. A Case of Novel Coronavirus Disease 19 in a Chronic Hemodialysis Patient Presenting with Gastroenteritis and Developing Severe Pulmonary Disease. Am. J. Nephrol. 2020, 51, 337–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, B.; Li, S.; Xiong, Y.; Tian, M.; Yu, J.; Xu, L.; Zhang, L.; Li, Z.; Ma, J.; Wen, F.; et al. COVID-19 Pneumonia in a Hemodialysis Patient. Kidney Med. 2020, 2, 354–358. [Google Scholar] [CrossRef]
- El Shamy, O.; Sharma, S.; Winston, J.; Uribarri, J. Peritoneal Dialysis During the Coronavirus Disease2019 (COVID-19) Pandemic: Acute Inpatient and Maintenance Outpatient Experiences. Kidney Med. 2020, 2, 377–380. [Google Scholar] [CrossRef]
- Dudreuilh, C.; Kumar, N.; Moxham, V.; Hemsley, C.; Goldenberg, S.; Moutzouris, D.A. Deisolation of COVID-19 positive hemodialysis patients in the outpatient setting: A singlecenter experience. Kidney Int. 2020, 98, 236–237. [Google Scholar] [CrossRef]
- Valeri, A.M.; Robbins-Juarez, S.Y.; Stevens, J.S.; Ahn, W.; Rao, M.K.; Radhakrishnan, J.; Gharavi, A.G.; Mohan, S.; Husain, S.A. Presentation and Outcomes of Patients with ESKD and COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1409–1415. [Google Scholar] [CrossRef]
- Ng, J.H.; Hirsch, J.S.; Wanchoo, R.; Sachdeva, M.; Sakhiya, V.; Hong, S.; Jhaveri, K.D.; Fishbane, S. Northwell COVID-19 Research Consortium and the Northwell Nephrology COVID-19 Research Consortium. Outcomes of patients with end-stage kidney disease hospitalized with COVID-19. Kidney Int. 2020, 98, 1530–1539. [Google Scholar] [CrossRef]
- Ma, Y.; Diao, B.; Lv, X.; Zhu, J.; Liang, W.; Liu, L.; Bu, W.; Cheng, H.; Zhang, S.; Shi, M.; et al. Novel Coronavirus Disease in Hemodialysis (HD) Patients: Report from One HD Centre in Wuhan China. medRxiv 2019. (submitted). [Google Scholar] [CrossRef] [Green Version]
- Rombolà, G.; Brunini, F. COVID-19 and dialysis: Why we should be worried. J. Nephrol. 2020, 33, 401–403. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.D.; Calabro-Kailukaitis, N. COVID-19 and ESKD, A Rapid Review. Rhode Isl. Med. J. 2020, 103, 29–33. [Google Scholar]
- Sánchez-Álvarez, J.E.; Fontán, M.P.; Martín, C.J.; Pelícano, M.B.; Reina, C.J.C.; Prieto, Á.M.S.; Melilli, E.; Barrios, M.C.; Heras, M.M.; Pino, M.D. Status of SARS-CoV-2 Infection in Patients on Renal Replacement Therapy. Report of the COVID-19 Registry of the Spanish Society of Nephrology (SEN). Nefrología 2020, 40, 272–278. [Google Scholar] [CrossRef]
- Couchoud, C.; Bayer, F.; Ayav, C.; Béchade, C.; Brunet, P.; Chantrel, F.; Frimat, L.; Galland, R.; Hourmant, M.; Laurain, E.; et al. Low Incidence of SARS-CoV-2, Risk Factors of Mortality and the Course of Illness in the French National Cohort of Dialysis Patients. Kidney Int. 2020, 98, 1519–1529. [Google Scholar] [CrossRef]
- Palumbo, R.; Morosetti, M.; Foniciello, M.; Ribaldi, S.; Botti, R.; Spiga, G. Emergenza COVID-19. Percorso per la presa in Carico dei Pazienti con Malattia Renale Cronica. Available online: https://www.anedonlus.it/wpcontent/uploads/2020/11/REGLAZIO.REGISTROUFFICIALE.2020.0937837.pdf (accessed on 10 October 2020).
- Dipartimento di Epidemiologia del Servizio Sanitario Regionale Regione Lazio; Rilevazione straordinaria COVID-19. 2020. Available online: http://www.deplazio.net/images/stories/files/RRDTL/manualerrdtlcovid19.pdf (accessed on 15 February 2021).
- Marino, C.; Pignocco, M.; Calandrini, E.; Dei Bardi, L.; Angelici, L.; Bargagli, A.M.; Cascini, S.; Agabiti, N.; Davoli, M. Registro Dialisi e Trapianto Lazio Rapporto annuale e rilevazione straordinaria COVID19. Available online: http://www.deplazio.net/images/stories/files/RRDTL/rapporto_rrdtl2020_def_20210628.pdf (accessed on 15 May 2021).
- Tazza, L.; Angelici, L.; Marino, C.; Di Napoli, A.; Bossola, M.; De Cicco, C.; Davoli, M.; Agabiti, N. Determinants of Venous Catheter Hemodialysis Onset and Subsequent Switch to Arteriovenous Fistula: An Epidemiological Study in Lazio Region. J. Vasc. Access 2021, 22, 749–758. [Google Scholar] [CrossRef] [PubMed]
- Bossola, M.; Marino, C.; Di Napoli, A.; Agabiti, N.; Tazza, L.; Davoli, M.; On behalf of the Dialysis and Transplant Lazio Region Registry Scientific Committee. Functional impairment and risk of mortality in patients on chronic hemodialysis: Results of the Lazio Dialysis Registry. J. Nephrol. 2018, 31, 593–602. [Google Scholar] [CrossRef]
- Tazza, L.; Di Napoli, A.; Bossola, M.; Valle, S.; Pezzotti, P.; Luciani, G.; Di Lallo, D.; on behalf of Lazio Dialysis Registry. Ageing of Patients on Chronic Dialysis: Effects on Mortality-A 12-Year Study. Nephrol. Dial. Transplant. 2008, 24, 940–947. [Google Scholar] [CrossRef] [Green Version]
- Di Napoli, A.; Lapucci, E.; Baglio, G.; Di Giulio, S. Lazio dialysis registry: Natives vs foreigners. G. Ital. Nefrol. 2015, 32. [Google Scholar]
- Di Napoli, A.; Tazza, L.; Chicca, S.; Lapucci, E.; Silvestri, P.; Di Lallo, D.; Michelozzi, P.; Davoli, M. Survival among chronic hemodialysis patients for each type of first vascular access. In Proceedings of the 51st Era-Edta Congress, Amsterdam, The Netherlands, 31 May–3 June 2014; 29 (Suppl. S3), p. iii246. [Google Scholar] [CrossRef] [Green Version]
- Guidelines and procedures for the implementation of a new Mortality Information System (SIM), and the Institution at the Local Health Units of the Nominative Causes of Death Registry (Rencam) in the Lazio Region. (Resolution of the Regional Council n.4302 3 July 1984). Official Bulletin of the Lazio Region n.23. [Iin Italian]. 1984. Available online: https://www.regione.lazio.it/bur (accessed on 15 May 2021).
- Further Urgent Civil Protection Interventions in Relation to the Emergency Related to the Health Risk Related to the Onset of Diseases Arising from Communicable Viral Agents. (Order of Civil Protection Department Presidency of the Council of Ministers no. 640 27 February 2020). Official Journal Serie Generale n.50. [In Italian]; 2020. Available online: https://www.trovanorme.salute.gov.it/norme/dettaglioAtto?id=73469 (accessed on 20 April 2021).
- Kooman, J.P.; van der Sande, F.M. COVID-19 in ESRD and Acute Kidney Injury. Blood Purif. 2021, 50, 610–620. [Google Scholar] [CrossRef] [PubMed]
- Savino, M.; Casula, A.; Santhakumaran, S.; Pitcher, D.; Wong, E.; Magadi, W.; Evans, K.M.; Benoy-Deeney, F.; Griffin, J.; Plumb, L.; et al. Sociodemographic Features and Mortality of Individuals on Haemodialysis Treatment Who Test Positive for SARS-CoV-2: A UK Renal Registry Data Analysis. PLoS ONE 2020, 15, e0241263. [Google Scholar] [CrossRef]
- Meyerowitz-Katz, G.; Merone, L. A Systematic Review and Meta-Analysis of Published Research Data on COVID-19 Infection Fatality Rates. Int. J. Infect. Dis. 2020, 101, 138–148. [Google Scholar] [CrossRef]
- Marino, C.; Angelici, L.; Calandrini, E.; Cascini, S.; Bargagli, A.M.; Morabito, S.; Petrosillo, N.; Agabiti, N.; Davoli, M. Incidenza ed esiti dell’infezione da SARS-CoV-2 nella popolazione in trattamento dialitico nel Lazio. XLIV Convegno AIE—2020. Available online: https://www.epidemiologia.it/wp-content/uploads/2020/09/Libro-degli-abstract.pdf (accessed on 29 November 2021).
- Quintaliani, G.; Reboldi, G.; Di Napoli, A.; Nordio, M.; Limido, A.; Aucella, F.; Messa, P.; Brunori, G.; Italian Society of Nephrology COVID-19 Research Group. Exposure to novel coronavirus in patients on renal replacement therapy during the exponential phase of COVID-19 pandemic: Survey of the Italian Society of Nephrology. J. Nephrol. 2020, 33, 725–736. [Google Scholar] [CrossRef]
- Nordio, M.; Reboldi, G.; Di Napoli, A.; Quintaliani, G.; Alberici, F.; Postorino, M.; Aucella, F.; Messa, P.; Brunori, G.; Italian Society of Nephrology COVID-19 Research Group. Risk factors and action thresholds for the novel coronavirus pandemic. Insights from the Italian Society of Nephrology COVID-19 Survey. J. Nephrol. 2021, 34, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Keller, N.; Chantrel, F.; Krummel, T.; Bazin-Kara, D.; Faller, A.L.; Muller, C.; Nussbaumer, T.; Ismer, M.; Benmoussa, A.; Brahim-Bouna, M.; et al. Impact of First-Wave COronaVIrus Disease 2019 Infection in Patients on HaemoDIALysis in Alsace: The Observational COVIDIAL Study. Nephrol. Dial. Transplant. 2020, 35, 1338–1411. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.M.; Weiner, D.E.; Aweh, G.; Miskulin, D.C.; Manley, H.J.; Stewart, C.; Ladik, V.; Hosford, J.; Lacson, E.C.; Johnson, D.S.; et al. COVID-19 among US Dialysis Patients: Risk Factors and Outcomes from a National Dialysis Provider. Am. J. Kidney Dis. 2021, 77, 748–756.e1. [Google Scholar] [CrossRef]
- Lano, G.; Braconnier, A.; Bataille, S.; Cavaille, G.; Moussi-Frances, J.; Gondouin, B.; Bindi, P.; Nakhla, M.; Mansour, J.; Halin, P.; et al. Risk Factors for Severity of COVID-19 in Chronic Dialysis Patients from a Multicentre French Cohort. Clin. Kidney J. 2020, 13, 878–888. [Google Scholar] [CrossRef] [PubMed]
- Taji, L.; Thomas, D.; Oliver, M.J.; Ip, J.; Tang, Y.; Yeung, A.; Cooper, R.; House, A.A.; McFarlane, P.; Blake, P.G. COVID-19 in Patients Undergoing Long-Term Dialysis in Ontario. CMAJ 2021, 193, E278–E284. [Google Scholar] [CrossRef] [PubMed]
- Department of Epidemiology Lazio Regional Health Service ASL Roma 1 (DEPLAZIO) and Regional Service for Epidemiology, Surveillance and Control of Infectious Diseases INMI Lazzaro Spallanzani (SERESMI). Maps of Lazio. Crude Rates of Cumulative Incidence of Cases COVID19 per Municipality of Residence. Available online: https://www.dep.lazio.it/covid/covid_map.php (accessed on 10 October 2020).
- Goicoechea, M.; Cámara, L.A.S.; Macías, N.; Muñoz de Morales, A.; Rojas, Á.G.; Bascuñana, A.; Arroyo, D.; Vega, A.; Abad, S.; Verde, E.; et al. COVID-19: Clinical Course and Outcomes of 36 Hemodialysis Patients in Spain. Kidney Int. 2020, 98, 27–34. [Google Scholar] [CrossRef]
- Weinhandl, E.D.; Wetmore, J.B.; Peng, Y.; Liu, J.; Gilbertson, D.T.; Johansen, K.L. Initial Effects of COVID-19 on Patients with ESKD. J. Am. Soc. Nephrol. 2021, 32, 1444–1453. [Google Scholar] [CrossRef]
- Jager, K.J.; Kramer, A.; Chesnaye, N.C.; Couchoud, C.; Sánchez-Álvarez, J.E.; Garneata, L.; Collart, F.; Hemmelder, M.H.; Ambühl, P.; Kerschbaum, J.; et al. Results from the ERA-EDTA Registry Indicate a High Mortality Due to COVID-19 in Dialysis Patients and Kidney Transplant Recipients across Europe. Kidney Int. 2020, 98, 1540–1548. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total | Non-Infected | Infected | p-Value χ2 | |||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Total | 4942 | 4686 | 256 | |||||
| Gender | 0.609 | |||||||
| Male | 3239 | 65.5 | 3075 | 65.6 | 164 | 64.1 | ||
| Female | 1703 | 34.5 | 1611 | 34.4 | 92 | 35.9 | ||
| Age (years) | 0.843 | |||||||
| 18–64 | 1710 | 34.6 | 1618 | 34.5 | 92 | 35.9 | ||
| 65–84 | 2713 | 54.9 | 2577 | 55.0 | 136 | 53.1 | ||
| ≥85 | 519 | 10.5 | 491 | 10.5 | 28 | 10.9 | ||
| Site of birth | 0.001 | |||||||
| Italy | 4379 | 88.6 | 4169 | 89.0 | 210 | 82.0 | ||
| Abroad | 563 | 11.4 | 517 | 11.0 | 46 | 18.0 | ||
| Residence | 0.171 | |||||||
| Rome municipality | 2403 | 48.6 | 2264 | 48.3 | 139 | 54.3 | ||
| Rome province | 1243 | 25.2 | 1187 | 25.3 | 56 | 21.9 | ||
| Other Lazio municipalities | 1296 | 26.2 | 1235 | 26.4 | 61 | 23.8 | ||
| Educational level (years) | 0.049 | |||||||
| Illiterate | 198 | 4.0 | 181 | 3.9 | 17 | 6.6 | ||
| 1–8 | 2757 | 55.8 | 2610 | 55.7 | 147 | 57.4 | ||
| ≥9 | 1987 | 40.2 | 1895 | 40.4 | 92 | 35.9 | ||
| Self-sufficiency | 0.351 | |||||||
| Total autonomy | 3073 | 62.2 | 2919 | 62.3 | 154 | 60.2 | ||
| Autonomy in some activities | 1118 | 22.6 | 1051 | 22.4 | 67 | 26.2 | ||
| Non self-sufficient | 751 | 15.2 | 716 | 15.3 | 35 | 13.7 | ||
| Nephropathy | ||||||||
| Diabetic nephropathy | 969 | 19.6 | 912 | 19.5 | 57 | 22.3 | 0.271 | |
| Renal vascular disease | 915 | 18.5 | 863 | 18.4 | 52 | 20.3 | 0.447 | |
| Glomerulonephritis | 452 | 9.1 | 430 | 9.2 | 22 | 8.6 | 0.753 | |
| Cystic renal disease or familial nephropathy | 389 | 7.9 | 358 | 7.6 | 31 | 12.1 | 0.010 | |
| Interstitial and toxic nephritis/pyelonephritis | 183 | 3.7 | 175 | 3.7 | 8 | 3.1 | 0.615 | |
| Systemic disease | 152 | 3.1 | 143 | 3.1 | 9 | 3.5 | 0.675 | |
| Renal malformation | 52 | 1.1 | 50 | 1.1 | 2 | 0.8 | 0.663 | |
| Other nephropathies | 621 | 12.6 | 596 | 12.7 | 25 | 9.8 | 0.165 | |
| Unknown | 1209 | 24.5 | 1159 | 24.7 | 50 | 19.5 | 0.059 | |
| Comorbidity | ||||||||
| Heart disease | 1711 | 34.6 | 1616 | 34.5 | 95 | 37.1 | 0.390 | |
| Diabetes | 1379 | 27.9 | 1307 | 27.9 | 72 | 28.1 | 0.935 | |
| Severe hypertension | 785 | 15.9 | 737 | 15.7 | 48 | 18.8 | 0.198 | |
| Obesity | 772 | 15.6 | 723 | 15.4 | 49 | 19.1 | 0.111 | |
| Vascular disease | 749 | 15.2 | 724 | 15.5 | 25 | 9.8 | 0.014 | |
| Cerebrovascular disease | 684 | 13.8 | 644 | 13.7 | 40 | 15.6 | 0.396 | |
| Cancer | 670 | 13.6 | 639 | 13.6 | 31 | 12.1 | 0.487 | |
| COPD | 609 | 12.3 | 573 | 12.2 | 36 | 14.1 | 0.385 | |
| Thyroid disease | 607 | 12.3 | 580 | 12.4 | 27 | 10.5 | 0.385 | |
| Lipid metabolism’s alteration | 447 | 9.0 | 427 | 9.1 | 20 | 7.8 | 0.480 | |
| Renal transplant | 400 | 8.1 | 381 | 8.1 | 19 | 7.4 | 0.686 | |
| Malnutrition | 293 | 5.9 | 275 | 5.9 | 18 | 7.0 | 0.443 | |
| Liver disease | 215 | 4.4 | 208 | 4.4 | 7 | 2.7 | 0.193 | |
| Motor deficit | 142 | 2.9 | 134 | 2.9 | 8 | 3.1 | 0.805 | |
| Extra-uremic anemia | 131 | 2.7 | 127 | 2.7 | 4 | 1.6 | 0.266 | |
| IBD | 129 | 2.6 | 119 | 2.5 | 10 | 3.9 | 0.182 | |
| Peptic ulcer | 90 | 1.8 | 86 | 1.8 | 4 | 1.6 | 0.751 | |
| Psychiatric disease | 89 | 1.8 | 81 | 1.7 | 8 | 3.1 | 0.102 | |
| Dementia | 83 | 1.7 | 75 | 1.6 | 8 | 3.1 | 0.065 | |
| LHA of dialysis centre | 0.014 | |||||||
| Rome 1 | 967 | 19.6 | 920 | 19.6 | 47 | 18.4 | ||
| Rome 2 | 1026 | 20.8 | 949 | 20.3 | 77 | 30.1 | ||
| Rome 3 | 489 | 9.9 | 468 | 10.0 | 21 | 8.2 | ||
| Rome 4 | 275 | 5.6 | 262 | 5.6 | 13 | 5.1 | ||
| Rome 5 | 425 | 8.6 | 403 | 8.6 | 22 | 8.6 | ||
| Rome 6 | 523 | 10.6 | 505 | 10.8 | 18 | 7.0 | ||
| Viterbo | 199 | 4.0 | 193 | 4.1 | 6 | 2.3 | ||
| Latina | 88 | 1.8 | 86 | 1.8 | 2 | 0.8 | ||
| Rieti | 501 | 10.1 | 479 | 10.2 | 22 | 8.6 | ||
| Frosinone | 449 | 9.1 | 421 | 9.0 | 28 | 10.9 | ||
| Weekly hours of dialysis | 0.104 | |||||||
| 3–9 | 1008 | 20.4 | 966 | 20.6 | 42 | 16.4 | ||
| ≥10 | 3934 | 79.6 | 3720 | 79.4 | 214 | 83.6 | ||
| Hemodialysis vintage (years) | 0.214 | |||||||
| 0–1 | 1900 | 38.4 | 1811 | 38.6 | 89 | 34.8 | ||
| ≥2 | 3042 | 61.6 | 2875 | 61.4 | 167 | 65.2 | ||
| Total | Alive | Dead | p-Value χ2 | |||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Total | 256 | 197 | 59 | |||||
| Period of infection incidence | 0.006 | |||||||
| March-July | 37 | 14.5 | 22 | 11.2 | 15 | 25.4 | ||
| August-November | 219 | 85.5 | 175 | 88.8 | 44 | 74.6 | ||
| Gender | 0.950 | |||||||
| Male | 164 | 64.1 | 126 | 64.0 | 38 | 64.4 | ||
| Female | 92 | 35.9 | 71 | 36.0 | 21 | 35.6 | ||
| Age (years) | 0.005 | |||||||
| 18–64 | 90 | 35.2 | 76 | 38.6 | 14 | 23.7 | ||
| 65–84 | 134 | 52.3 | 103 | 52.3 | 31 | 52.5 | ||
| ≥85 | 32 | 12.5 | 18 | 9.1 | 14 | 23.7 | ||
| Site of birth | 0.075 | |||||||
| Italy | 210 | 82.0 | 157 | 79.7 | 53 | 89.8 | ||
| Abroad | 46 | 18.0 | 40 | 20.3 | 6 | 10.2 | ||
| Residence | 0.114 | |||||||
| Rome municipality | 139 | 54.3 | 100 | 50.8 | 39 | 66.1 | ||
| Rome province | 56 | 21.9 | 46 | 23.4 | 10 | 16.9 | ||
| Other Lazio municipalities | 61 | 23.8 | 51 | 25.9 | 10 | 16.9 | ||
| Educational level (years) | 0.622 | |||||||
| Illiterate | 17 | 6.6 | 14 | 7.1 | 3 | 5.1 | ||
| 1–8 | 147 | 57.4 | 110 | 55.8 | 37 | 62.7 | ||
| ≥9 | 92 | 35.9 | 73 | 37.1 | 19 | 32.2 | ||
| Self-sufficiency | 0.705 | |||||||
| Total autonomy | 154 | 60.2 | 120 | 60.9 | 34 | 57.6 | ||
| Autonomy in some activities | 67 | 26.2 | 52 | 26.4 | 15 | 25.4 | ||
| Non self-sufficient | 35 | 13.7 | 25 | 12.7 | 10 | 16.9 | ||
| Nephropathy | ||||||||
| Diabetic nephropathy | 57 | 22.3 | 48 | 24.4 | 9 | 15.3 | 0.140 | |
| Renal vascular disease | 52 | 20.3 | 38 | 19.3 | 14 | 23.7 | 0.457 | |
| Cystic renal disease or familial nephropathy | 31 | 12.1 | 22 | 11.2 | 9 | 15.3 | 0.399 | |
| Glomerulonephritis | 22 | 8.6 | 16 | 8.1 | 6 | 10.2 | 0.623 | |
| Systemic disease | 9 | 3.5 | 8 | 4.1 | 1 | 1.7 | 0.387 | |
| Interstitial and toxic nephritis/pyelonephritis | 8 | 3.1 | 4 | 2.0 | 4 | 6.8 | 0.066 | |
| Renal malformation | 2 | 0.8 | 1 | 0.5 | 1 | 1.7 | 0.364 | |
| Other nephropathies | 25 | 9.8 | 18 | 9.1 | 7 | 11.9 | 0.536 | |
| Unknown | 52 | 20.3 | 42 | 21.3 | 8 | 13.6 | 0.187 | |
| Comorbidity | ||||||||
| Heart disease | 95 | 37.1 | 72 | 36.5 | 23 | 39.0 | 0.734 | |
| Diabetes | 72 | 28.1 | 57 | 28.9 | 15 | 25.4 | 0.599 | |
| Obesity | 49 | 19.1 | 39 | 19.8 | 10 | 16.9 | 0.626 | |
| Severe hypertension | 48 | 18.8 | 43 | 21.8 | 5 | 8.5 | 0.021 | |
| Cerebrovascular disease | 40 | 15.6 | 27 | 13.7 | 13 | 22.0 | 0.122 | |
| COPD | 36 | 14.1 | 26 | 13.2 | 10 | 16.9 | 0.467 | |
| Cancer | 31 | 12.1 | 23 | 11.7 | 8 | 13.6 | 0.697 | |
| Thyroid disease | 27 | 10.5 | 16 | 8.1 | 11 | 18.6 | 0.021 | |
| Vascular disease | 25 | 9.8 | 16 | 8.1 | 9 | 15.3 | 0.106 | |
| Lipid metabolism’s alteration | 20 | 7.8 | 16 | 8.1 | 4 | 6.8 | 0.736 | |
| Renal transplant | 19 | 7.4 | 14 | 7.1 | 5 | 8.5 | 0.725 | |
| Malnutrition | 18 | 7.0 | 8 | 4.1 | 10 | 16.9 | 0.001 | |
| IBD | 10 | 3.9 | 6 | 3.0 | 4 | 6.8 | 0.194 | |
| Motor deficit | 8 | 3.1 | 5 | 2.5 | 3 | 5.1 | 0.324 | |
| Dementia | 8 | 3.1 | 5 | 2.5 | 3 | 5.1 | 0.324 | |
| Psychiatric disease | 8 | 3.1 | 6 | 3.0 | 2 | 3.4 | 0.894 | |
| Liver disease | 7 | 2.7 | 4 | 2.0 | 3 | 5.1 | 0.207 | |
| Extra-uremic anemia | 4 | 1.6 | 3 | 1.5 | 1 | 1.7 | 0.926 | |
| Peptic ulcer | 4 | 1.6 | 4 | 2.0 | 0 | 0.0 | 0.270 | |
| LHA of dialysis centre | 0.033 | |||||||
| Rome 1 | 47 | 18.4 | 35 | 17.8 | 12 | 20.3 | ||
| Rome 2 | 77 | 30.1 | 58 | 29.4 | 19 | 32.2 | ||
| Rome 3 | 21 | 8.2 | 15 | 7.6 | 6 | 10.2 | ||
| Rome 4 | 13 | 5.1 | 9 | 4.6 | 4 | 6.8 | ||
| Rome 5 | 22 | 8.6 | 20 | 10.2 | 2 | 3.4 | ||
| Rome 6 | 18 | 7.0 | 11 | 5.6 | 7 | 11.9 | ||
| Viterbo | 6 | 2.3 | 4 | 2.0 | 2 | 3.4 | ||
| Latina | 2 | 0.8 | 0 | 0.0 | 2 | 3.4 | ||
| Rieti | 22 | 8.6 | 19 | 9.6 | 3 | 5.1 | ||
| Frosinone | 28 | 10.9 | 26 | 13.2 | 2 | 3.4 | ||
| Weekly hours of dialysis | 0.501 | |||||||
| 3–9 | 42 | 16.4 | 34 | 17.3 | 8 | 13.6 | ||
| ≥10 | 214 | 83.6 | 163 | 82.7 | 51 | 86.4 | ||
| Hemodialysis vintage (years) | 0.155 | |||||||
| 0–1 | 80 | 31.3 | 66 | 33.5 | 14 | 23.7 | ||
| ≥2 | 176 | 68.8 | 131 | 66.5 | 45 | 76.3 | ||
| Symptoms at time of swab | ||||||||
| Fever | 141 | 55.1 | 100 | 50.8 | 41 | 69.5 | 0.011 | |
| Cough | 83 | 32.4 | 61 | 31.0 | 22 | 37.3 | 0.363 | |
| Respiratory distress | 52 | 20.3 | 34 | 17.3 | 18 | 30.5 | 0.027 | |
| Colds | 11 | 4.3 | 9 | 4.6 | 2 | 3.4 | 0.695 | |
| Gastrointestinal disease | 7 | 2.7 | 5 | 2.5 | 2 | 3.4 | 0.725 | |
| Conjunctivitis | 5 | 2.0 | 4 | 2.0 | 1 | 1.7 | 0.870 | |
| Loss of taste and smell | 2 | 0.8 | 2 | 1.0 | 0 | 0.0 | 0.437 | |
| Hospitalization for infection | 0.549 | |||||||
| No | 64 | 25.0 | 51 | 25.9 | 13 | 22.0 | ||
| Yes | 192 | 75.0 | 146 | 74.1 | 46 | 78.0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marino, C.; Angelici, L.; Pistolesi, V.; Morabito, S.; Di Napoli, A.; Calandrini, E.; Cascini, S.; Bargagli, A.M.; Petrosillo, N.; Agabiti, N.; et al. SARS-CoV-2 Infection in Patients on Dialysis: Incidence and Outcomes in the Lazio Region, Italy. J. Clin. Med. 2021, 10, 5818. https://doi.org/10.3390/jcm10245818
Marino C, Angelici L, Pistolesi V, Morabito S, Di Napoli A, Calandrini E, Cascini S, Bargagli AM, Petrosillo N, Agabiti N, et al. SARS-CoV-2 Infection in Patients on Dialysis: Incidence and Outcomes in the Lazio Region, Italy. Journal of Clinical Medicine. 2021; 10(24):5818. https://doi.org/10.3390/jcm10245818
Chicago/Turabian StyleMarino, Claudia, Laura Angelici, Valentina Pistolesi, Santo Morabito, Anteo Di Napoli, Enrico Calandrini, Silvia Cascini, Anna Maria Bargagli, Nicola Petrosillo, Nera Agabiti, and et al. 2021. "SARS-CoV-2 Infection in Patients on Dialysis: Incidence and Outcomes in the Lazio Region, Italy" Journal of Clinical Medicine 10, no. 24: 5818. https://doi.org/10.3390/jcm10245818