
Comparison between Dexamethasone and Methylprednisolone Therapy in Patients with COVID-19 Pneumonia Admitted to Non-Intensive Medical Units

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Primary and Secondary Outcomes
2.3. Statistical Analysis
3. Results
3.1. Study Population
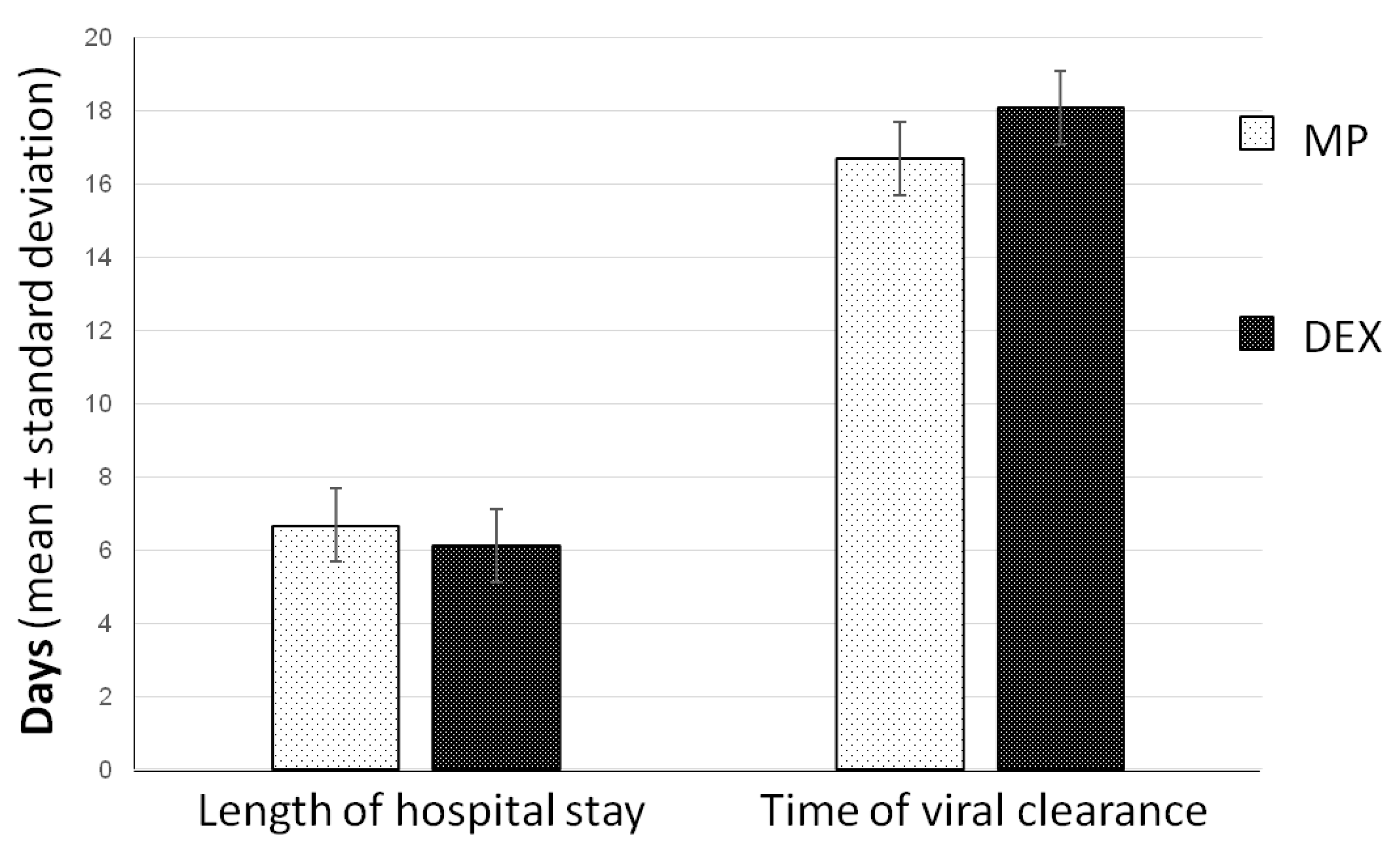
3.2. Clinical Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Weekly Epidemiological Update on COVID-19—21 September 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---21-september-2021 (accessed on 10 September 2021).
- Grant, M.C.; Geoghegan, L.; Arbyn, M.; Mohammed, Z.; McGuinness, L.; Clarke, E.L.; Wade, R.G. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): A systematic review and meta-analysis of 148 studies from 9 countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Siddiqi, H.K.; Mehra, M.R. COVID-19 illness in native and immunosuppressed states: A clinical–therapeutic staging proposal. J. Hear. Lung Transplant. 2020, 39, 405–407. [Google Scholar] [CrossRef] [Green Version]
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: A two-centre descriptive study. Lancet Infect. Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients with COVID-19 in Wuhan, China. SSRN Electron. J. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Gustine, J.N.; Jones, D. Immunopathology of Hyperinflammation in COVID-19. Am. J. Pathol. 2020, 191, 4–17. [Google Scholar] [CrossRef] [PubMed]
- Felice, C.; Nardin, C.; Di Tanna, G.L.; Grossi, U.; Bernardi, E.; Scaldaferri, L.; Romagnoli, M.; Tonon, L.; Cavasin, P.; Novello, S.; et al. Use of RAAS Inhibitors and Risk of Clinical Deterioration in COVID-19: Results from an Italian Cohort of 133 Hypertensives. Am. J. Hypertens. 2020, 33, 944–948. [Google Scholar] [CrossRef] [PubMed]
- Morena, V.; Milazzo, L.; Oreni, L.; Bestetti, G.; Fossali, T.; Bassoli, C.; Torre, A.; Cossu, M.V.; Minari, C.; Ballone, E.; et al. Off-label use of tocilizumab for the treatment of SARS-CoV-2 pneumonia in Milan, Italy. Eur. J. Intern. Med. 2020, 76, 36–42. [Google Scholar] [CrossRef]
- Di Castelnuovo, A.; Costanzo, S.; Antinori, A.; Berselli, N.; Blandi, L.; Bruno, R.; Cauda, R.; Guaraldi, G.; Menicanti, L.; My, I.; et al. Use of hydroxychloroquine in hospitalised COVID-19 patients is associated with reduced mortality: Findings from the observational multicentre Italian CORIST study. Eur. J. Intern. Med. 2020, 82, 38–47. [Google Scholar] [CrossRef]
- Pasin, L.; Cavalli, G.; Navalesi, P.; Sella, N.; Landoni, G.; Yavorovskiy, A.G.; Likhvantsev, V.V.; Zangrillo, A.; Dagna, L.; Monti, G. Anakinra for patients with COVID-19: A meta-analysis of non-randomized cohort studies. Eur. J. Intern. Med. 2021, 86, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef] [PubMed]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—preliminary report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Boulware, D.R.; Pullen, M.; Bangdiwala, A.S.; Pastick, K.A.; Lofgren, S.M.; Okafor, E.C.; Skipper, C.P.; Nascene, A.A.; Nicol, M.R.; Abassi, M.; et al. A Randomized Trial of Hydroxychloroquine as Postexposure Prophylaxis for Covid-19. N. Engl. J. Med. 2020, 383, 517–525. [Google Scholar] [CrossRef]
- Simonovich, V.A.; Pratx, L.D.B.; Scibona, P.; Beruto, M.V.; Vallone, M.G.; Vázquez, C.; Savoy, N.; Giunta, D.H.; Pérez, L.G.; Sánchez, M.D.L.; et al. A Randomized Trial of Convalescent Plasma in Covid-19 Severe Pneumonia. N. Engl. J. Med. 2021, 384, 619–629. [Google Scholar] [CrossRef]
- The RECOVERY Collaborative Group Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2021, 384, 693–704. [CrossRef]
- Wagner, C.; Griesel, M.; Mikolajewska, A.; Mueller, A.; Nothacker, M.; Kley, K.; Metzendorf, M.-I.; Fischer, A.-L.; Kopp, M.; Stegemann, M.; et al. Systemic corticosteroids for the treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 2021. [Google Scholar] [CrossRef]
- Corral-Gudino, L.; Bahamonde, A.; Arnaiz-Revillas, F.; Gómez-Barquero, J.; Abadía-Otero, J.; García-Ibarbia, C.; Mora, V.; Cerezo-Hernández, A.; Hernández, J.L.; López-Muñíz, G.; et al. Methylprednisolone in adults hospitalized with COVID-19 pneumonia: An open-label randomized trial (GLUCOCOVID). Wien. Klin. Wochenschr. 2021, 133, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Jeronimo, C.M.P.; Farias, M.E.L.; Val, F.F.A.; Sampaio, V.S.; Alexandre, M.A.A.; Melo, G.C.; Safe, I.P.; Borba, M.G.S.; Netto, R.L.A.; Maciel, A.B.S.; et al. Methylprednisolone as Adjunctive Therapy for Patients Hospitalized with Coronavirus Disease 2019 (COVID-19; Metcovid): A Randomized, Double-blind, Phase IIb, Placebo-controlled Trial. Clin. Infect. Dis. 2020, 72, e373–e381. [Google Scholar] [CrossRef] [PubMed]
- Ranjbar, K.; Moghadami, M.; Mirahmadizadeh, A.; Fallahi, M.J.; Khaloo, V.; Shahriarirad, R.; Erfani, A.; Khodamoradi, Z.; Saadi, M.H.G. Methylprednisolone or dexamethasone, which one is superior corticosteroid in the treatment of hospitalized COVID-19 patients: A triple-blinded randomized controlled trial. BMC Infect. Dis. 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Sun, Y.; Sun, J.; Liang, H.; Ding, X.; Sun, X.; Wang, D.; Sun, T. Efficacy and Safety of Corticosteroid Use in Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis. Infect. Dis. Ther. 2021, 10, 2447–2463. [Google Scholar] [CrossRef] [PubMed]
- Pulakurthi, Y.S.; Pederson, J.M.; Saravu, K.; Gupta, N.; Balasubramanian, P.; Kamrowski, S.; Schmidt, M.; Vegivinti, C.T.R.; Dibas, M.; Reierson, N.L.; et al. Corticosteroid therapy for COVID-19: A systematic review and meta-analysis of randomized controlled trials. Medicine 2021, 100, e25719. [Google Scholar] [CrossRef] [PubMed]
- Mager, D.E.; Lin, S.X.; Blum, R.A.; Lates, C.D.; Jusko, W.J. Dose Equivalency Evaluation of Major Corticosteroids: Pharmacokinetics and Cell Trafficking and Cortisol Dynamics. J. Clin. Pharmacol. 2003, 43, 1216–1227. [Google Scholar] [CrossRef] [PubMed]
- Braude, A.; Rebuck, A. Prednisone and methylprednisolone disposition in the lung. Lancet 1983, 322, 995–997. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Methylprednisolone (n = 136) | Dexamethasone (n = 110) | p | |
|---|---|---|---|
| Age, years (mean, SD) | 74.4 (13.2) | 72.1 (12.1) | 0.166 |
| Gender—male, n (%) | 92 (67.6) | 74 (67.3) | 0.950 |
| Active smoker *, n (%) | 5 (3.7) | 2 (1.8) | 0.383 |
| Comorbidities, n (%) | 119 (87.5) | 101 (91.8) | 0.273 |
| Hypertension, n (%) | 85 (62.5) | 80 (72.7) | 0.090 |
| Obesity, n (%) | 22 (16.2) | 19 (17.3) | 0.819 |
| Diabetes, n (%) | 29 (21.3) | 29 (26.4) | 0.354 |
| Dyslipidemia, n (%) | 39 (28.7) | 24 (21.8) | 0.220 |
| Neoplasm, n (%) | 23 (16.9) | 33 (30.0) | 0.015 |
| CAD, n (%) | 16 (11.8) | 11 (10.0) | 0.660 |
| Atrial fibrillation, n (%) | 16 (11.8) | 11 (10.0) | 0.660 |
| VTE, n (%) | 8 (5.9) | 4 (3.6) | 0.416 |
| COPD, n (%) | 9 (6.6) | 4 (3.6) | 0.299 |
| CKD, n (%) | 6 (4.4) | 13 (11.8) | 0.031 |
| Concomitant chronic medications, n (%) | 112 (82.4) | 99 (90.0) | 0.088 |
| Systemic steroids, n (%) | 6 (4.4) | 5 (4.5) | 0.960 |
| Antihypertensive, n (%) | 90 (66.2) | 80 (72.7) | 0.269 |
| Antidiabetic, n (%) | 25 (18.4) | 26 (23.6) | 0.312 |
| Oral anticoagulant, n (%) | 24 (17.6) | 17 (15.5) | 0.646 |
| Antiplatelet, n (%) | 38 (27.9) | 31 (28.2) | 0.967 |
| Statins, n (%) | 39 (28.7) | 36 (32.7) | 0.493 |
| Clinical Characteristics at Admission | |||
| Days from the onset to admission, mean (SD) | 7.00 (3.5) | 5.54 (3.8) | 0.002 |
| SOFA score, mean (SD) | 3.85 (1.4) | 4.20 (1.5) | 0.330 |
| Methylprednisolone (n = 136) | Dexamethasone (n = 110) | p | |
|---|---|---|---|
| PaO2/FiO2 (mmHg) | 250 (84) | 261 (76) | 0.298 |
| PaO2 (mmHg) | 68 (19) | 69 (22) | 0.770 |
| WBC (103/μL) | 7.25 (3.82) | 8.28 (10.85) | 0.306 |
| CRP (mg/dL) | 8.91 (7.09) | 8.34 (6.81) | 0.529 |
| Procalcitonin (ng/mL) | 0.69 (3.2) | 0.38 (0.57) | 0.553 |
| Lactate (mmol/L) | 1.4 (0.6) | 1.4 (0.6) | 0.723 |
| Ferritin (ng/mL) | 970 (914) | 961 (706) | 0.946 |
| Hemoglobin | 134 (15) | 134 (14) | 0.865 |
| Creatinin (mg/dL) | 1.01 (0.43) | 1.06 (0.62) | 0.448 |
| D-Dimer (ng/mL) | 3234 (11261) | 2530 (5808) | 0.585 |
| NT-ProBNP (pg/L) | 1982 (5267) | 1943 (4781) | 0.955 |
| T Troponin (ng/L) | 32 (65) | 31 (46) | 0.941 |
| Treatment | Methylprednisolone (n = 136) | Dexamethasone (n = 110) | p |
|---|---|---|---|
| Antibiotics, n (%) | 108 (79.4) | 67 (60.9) | 0.001 |
| Anticoagulant prophylaxis, n (%) | 107 (78.7) | 93 (84.5) | 0.240 |
| Anticoagulant therapy, n (%) | 29 (21.3) | 17 (15.5) | 0.240 |
| Antiplatelet, n (%) | 35 (25.7) | 27 (24.5) | 0.530 |
| Remdesivir, n (%) | 74 (54.4) | 46 (41.8) | 0.049 |
| Convalescent plasma, n (%) | 4 (2.9) | 3 (2.7) | 0.920 |
| 30-Day Mortality | ||||
| Unadjusted | Adjusted * | |||
| Treatment | OR (95% CI) | p | OR (95% CI) | p |
| DEX vs. MP | 1.35 (0.71–2.56) | 0.351 | 0.78 (0.35–1.72) | 0.544 |
| s-ICU/ICU Admission | ||||
| Unadjusted | Adjusted * | |||
| Treatment | OR (95% CI) | p | OR (95% CI) | p |
| DEX vs. MP | 1.94 (0.81–4.66) | 0.136 | 1.37 (0.54–3.46) | 0.503 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buso, R.; Cinetto, F.; Dell’Edera, A.; Veneran, N.; Facchini, C.; Biscaro, V.; Schiavon, S.; Vian, E.; Grossi, U.; Zanus, G.; et al. Comparison between Dexamethasone and Methylprednisolone Therapy in Patients with COVID-19 Pneumonia Admitted to Non-Intensive Medical Units. J. Clin. Med. 2021, 10, 5812. https://doi.org/10.3390/jcm10245812
Buso R, Cinetto F, Dell’Edera A, Veneran N, Facchini C, Biscaro V, Schiavon S, Vian E, Grossi U, Zanus G, et al. Comparison between Dexamethasone and Methylprednisolone Therapy in Patients with COVID-19 Pneumonia Admitted to Non-Intensive Medical Units. Journal of Clinical Medicine. 2021; 10(24):5812. https://doi.org/10.3390/jcm10245812
Chicago/Turabian StyleBuso, Roberta, Francesco Cinetto, Alessandro Dell’Edera, Nicola Veneran, Cesarina Facchini, Valeria Biscaro, Stefania Schiavon, Elisa Vian, Ugo Grossi, Giacomo Zanus, and et al. 2021. "Comparison between Dexamethasone and Methylprednisolone Therapy in Patients with COVID-19 Pneumonia Admitted to Non-Intensive Medical Units" Journal of Clinical Medicine 10, no. 24: 5812. https://doi.org/10.3390/jcm10245812