
Awareness and Perspectives among Asian Anesthesiologists on Postoperative Delirium: A Multinational Survey

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Development
2.2. Questionnaire
2.3. Statistical Analysis
2.4. Ethics Statement
3. Results
3.1. Demographics of Study Participants
3.2. Knowledge and Perspectives Regarding POD
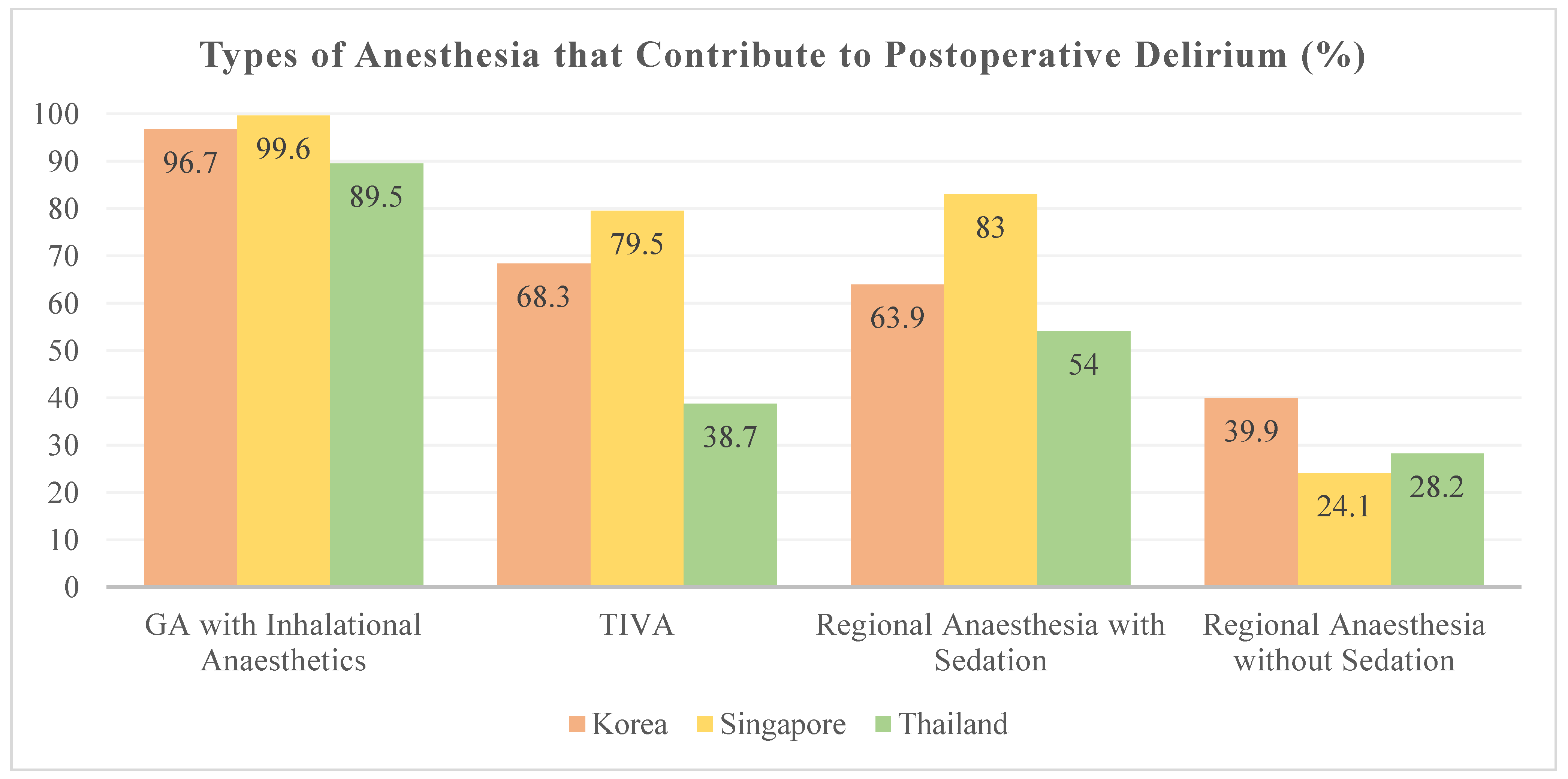
3.3. Awareness of Patient and Anesthetic Risk Factors for POD
3.4. Perspectives on Testing and Monitoring
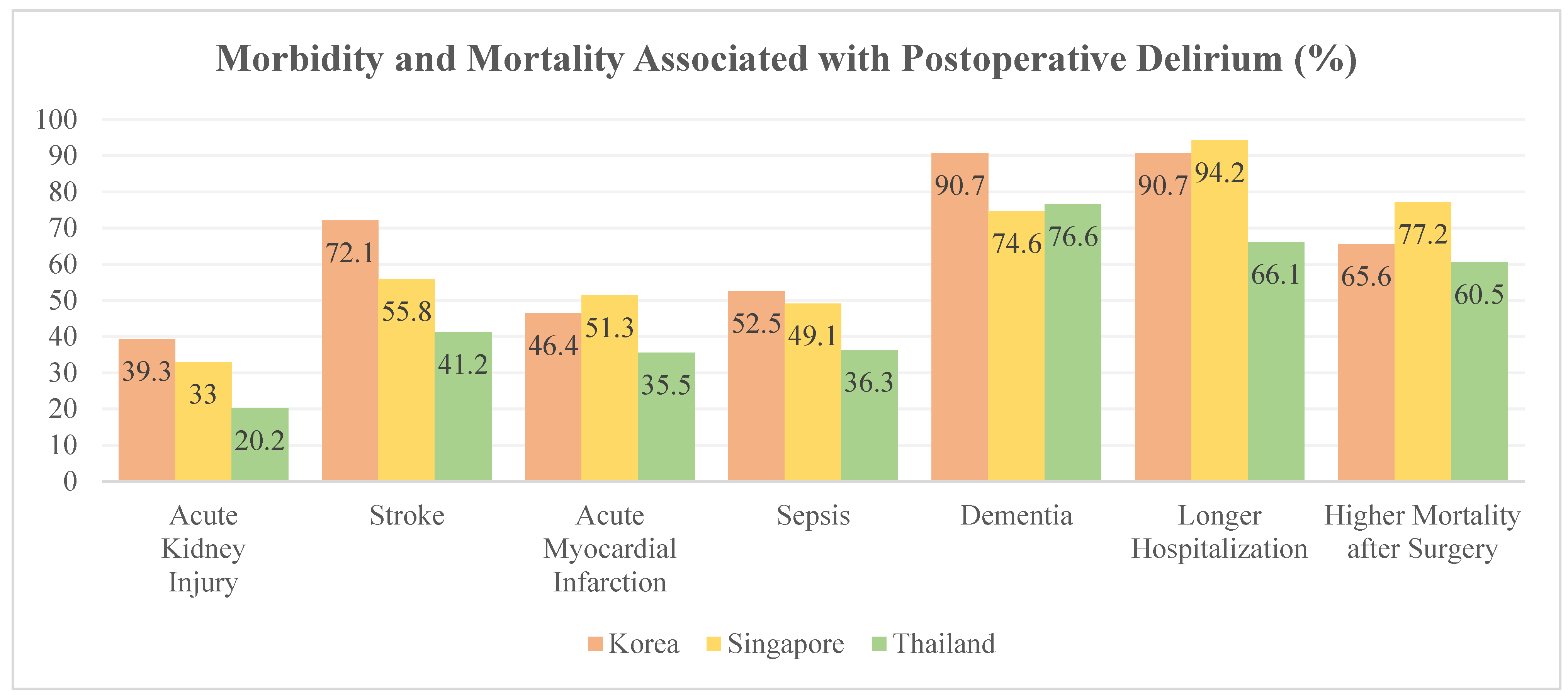
3.5. Morbidity and Mortality Associated with POD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mahanna-Gabrielli, E.; Schenning, K.J.; Eriksson, L.I.; Browndyke, J.N.; Wright, C.B.; Culley, D.J.; Evered, L.; Scott, D.A.; Wang, N.Y.; Brown, C.H.T.; et al. State of the clinical science of perioperative brain health: Report from the American Society of Anesthesiologists Brain Health Initiative Summit 2018. Br. J. Anaesth. 2019, 123, 464–478. [Google Scholar] [CrossRef] [Green Version]
- Abelha, F.J.; Luis, C.; Veiga, D.; Parente, D.; Fernandes, V.; Santos, P.; Botelho, M.; Santos, A.; Santos, C. Outcome and quality of life in patients with postoperative delirium during an ICU stay following major surgery. Crit. Care 2013, 17, R257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bickel, H.; Gradinger, R.; Kochs, E.; Forstl, H. High risk of cognitive and functional decline after postoperative delirium. A three-year prospective study. Dement Geriatr. Cogn. Disord. 2008, 26, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Radtke, F.M.; Franck, M.; MacGuill, M.; Seeling, M.; Lutz, A.; Westhoff, S.; Neumann, U.; Wernecke, K.D.; Spies, C.D. Duration of fluid fasting and choice of analgesic are modifiable factors for early postoperative delirium. Eur. J. Anaesthesiol. 2010, 27, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Aya, A.G.M.; Pouchain, P.H.; Thomas, H.; Ripart, J.; Cuvillon, P. Incidence of postoperative delirium in elderly ambulatory patients: A prospective evaluation using the FAM-CAM instrument. J. Clin. Anesth. 2019, 53, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Koebrugge, B.; van Wensen, R.J.; Bosscha, K.; Dautzenberg, P.L.; Koning, O.H. Delirium after emergency/elective open and endovascular aortoiliac surgery at a surgical ward with a high-standard delirium care protocol. Vascular 2010, 18, 279–287. [Google Scholar] [CrossRef]
- American Psychiatric Association; DSM-5 Task Force. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Dahmani, S.; Delivet, H.; Hilly, J. Emergence delirium in children: An update. Curr. Opin. Anaesthesiol. 2014, 27, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Mason, K.P. Paediatric emergence delirium: A comprehensive review and interpretation of the literature. Br. J. Anaesth. 2017, 118, 335–343. [Google Scholar] [CrossRef] [Green Version]
- The American Geriatrics Society Expert Panel on Postoperative Delirium in Older Adults. American Geriatrics Society abstracted clinical practice guideline for postoperative delirium in older adults. J. Am. Geriatr. Soc. 2015, 63, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Evered, L.; Silbert, B.; Knopman, D.S.; Scott, D.A.; DeKosky, S.T.; Rasmussen, L.S.; Oh, E.S.; Crosby, G.; Berger, M.; Eckenhoff, R.G.; et al. Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery-2018. Br. J. Anaesth. 2018, 121, 1005–1012. [Google Scholar] [CrossRef] [Green Version]
- Rudolph, J.L.; Marcantonio, E.R. Review articles: Postoperative delirium: Acute change with long-term implications. Anesth Analg. 2011, 112, 1202–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosker, C.; Ward, D. Hypoactive delirium. BMJ 2017, 357, j2047. [Google Scholar] [CrossRef] [Green Version]
- Krewulak, K.D.; Stelfox, H.T.; Leigh, J.P.; Ely, E.W.; Fiest, K.M. Incidence and Prevalence of Delirium Subtypes in an Adult ICU: A Systematic Review and Meta-Analysis. Crit. Care Med. 2018, 46, 2029–2035. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Hu, Y.; Yan, E.; Zhan, G.; Liu, C.; Yang, C. Perioperative neurocognitive dysfunction: Thinking from the gut? Aging 2020, 12, 15797–15817. [Google Scholar] [CrossRef]
- Mason, S.E.; Noel-Storr, A.; Ritchie, C.W. The impact of general and regional anesthesia on the incidence of post-operative cognitive dysfunction and post-operative delirium: A systematic review with meta-analysis. J. Alzheimers Dis. 2010, 22 (Suppl. S3), S67–S79. [Google Scholar] [CrossRef]
- Moyce, Z.; Rodseth, R.N.; Biccard, B.M. The efficacy of peri-operative interventions to decrease postoperative delirium in non-cardiac surgery: A systematic review and meta-analysis. Anaesthesia 2014, 69, 259–269. [Google Scholar] [CrossRef]
- O’Donnell, C.M.; McLoughlin, L.; Patterson, C.C.; Clarke, M.; McCourt, K.C.; McBrien, M.E.; McAuley, D.F.; Shields, M.O. Perioperative outcomes in the context of mode of anaesthesia for patients undergoing hip fracture surgery: Systematic review and meta-analysis. Br. J. Anaesth. 2018, 120, 37–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, V.; Champaneria, R.; Dretzke, J.; Yeung, J. Effect of regional versus general anaesthesia on postoperative delirium in elderly patients undergoing surgery for hip fracture: A systematic review. BMJ Open 2018, 8, e020757. [Google Scholar] [CrossRef] [PubMed]
- Avidan, M.S.; Maybrier, H.R.; Abdallah, A.B.; Jacobsohn, E.; Vlisides, P.E.; Pryor, K.O.; Veselis, R.A.; Grocott, H.P.; Emmert, D.A.; Rogers, E.M.; et al. Intraoperative ketamine for prevention of postoperative delirium or pain after major surgery in older adults: An international, multicentre, double-blind, randomised clinical trial. Lancet 2017, 390, 267–275. [Google Scholar] [CrossRef]
- Duan, X.; Coburn, M.; Rossaint, R.; Sanders, R.D.; Waesberghe, J.V.; Kowark, A. Efficacy of perioperative dexmedetomidine on postoperative delirium: Systematic review and meta-analysis with trial sequential analysis of randomised controlled trials. Br. J. Anaesth. 2018, 121, 384–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieri, M.; De Simone, A.; Rose, S.; De Domenico, P.; Lembo, R.; Denaro, G.; Landoni, G.; Monaco, F. Trials Focusing on Prevention and Treatment of Delirium After Cardiac Surgery: A systematic Review of Randomized Evidence. J. Cardiothorac. Vasc. Anesth. 2020, 34, 1641–1654. [Google Scholar] [CrossRef]
- Aldecoa, C.; Bettelli, G.; Bilotta, F.; Sanders, R.D.; Audisio, R.; Borozdina, A.; Cherubini, A.; Jones, C.; Kehlet, H.; MacLullich, A.; et al. European Society of Anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur. J. Anaesthesiol. 2017, 34, 192–214. [Google Scholar] [CrossRef]
- Gaudreau, J.D.; Gagnon, P.; Harel, F.; Tremblay, A.; Roy, M.A. Fast, systematic, and continuous delirium assessment in hospitalized patients: The nursing delirium screening scale. J. Pain. Symptom. Manag. 2005, 29, 368–375. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Punjasawadwong, Y.; Chau-In, W.; Laopaiboon, M.; Punjasawadwong, S.; Pin-On, P. Processed electroencephalogram and evoked potential techniques for amelioration of postoperative delirium and cognitive dysfunction following non-cardiac and non-neurosurgical procedures in adults. Cochrane Database Syst. Rev. 2018, 5, CD011283. [Google Scholar] [CrossRef] [PubMed]
- Bendahan, N.; Neal, O.; Ross-White, A.; Muscedere, J.; Boyd, J.G. Relationship Between Near-Infrared Spectroscopy-Derived Cerebral Oxygenation and Delirium in Critically Ill Patients: A Systematic Review. J. Intensive Care Med. 2019, 34, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Zhang, K.; Zhang, L.; Zong, H.; Meng, L.; Han, R. Cerebral near-infrared spectroscopy (NIRS) for perioperative monitoring of brain oxygenation in children and adults. Cochrane Database Syst. Rev. 2018, 1, CD010947. [Google Scholar] [CrossRef]
- Hamilton, G.M.; Wheeler, K.; Di Michele, J.; Lalu, M.M.; McIsaac, D.I. A Systematic Review and Meta-analysis Examining the Impact of Incident Postoperative Delirium on Mortality. Anesthesiology 2017, 127, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Sprung, J.; Roberts, R.O.; Weingarten, T.N.; Nunes Cavalcante, A.; Knopman, D.S.; Petersen, R.C.; Hanson, A.C.; Schroeder, D.R.; Warner, D.O. Postoperative delirium in elderly patients is associated with subsequent cognitive impairment. Br. J. Anaesth. 2017, 119, 316–323. [Google Scholar] [CrossRef]
- Kim, J.; Byun, S.H.; Kim, J.W.; Kim, J.Y.; Kim, Y.J.; Choi, N.; Lee, B.S.; Yu, S.; Kim, E. Behavioral changes after hospital discharge in preschool children experiencing emergence delirium after general anesthesia: A prospective observational study. Paediatr. Anaesth. 2021, 31, 1056–1064. [Google Scholar] [CrossRef]
- Urits, I.; Peck, J.; Giacomazzi, S.; Patel, R.; Wolf, J.; Mathew, D.; Schwartz, R.; Kassem, H.; Urman, R.D.; Kaye, A.D.; et al. Emergence Delirium in Perioperative Pediatric Care: A Review of Current Evidence and New Directions. Adv. Ther. 2020, 37, 1897–1909. [Google Scholar] [CrossRef] [PubMed]
- Safe Brain Initiative. Available online: http://safebraininitiative.com/ (accessed on 5 November 2021).




{kind=link}
{kind=link}
{kind=link}
| Demographics | Number | Proportion | |
|---|---|---|---|
| Country | Singapore | 224 | 42.2% |
| Thailand | 124 | 23.3% | |
| Korea | 183 | 34.5% | |
| Age (years) | Less than 30 | 114 | 21.5% |
| 31 to 40 | 215 | 40.5% | |
| 41 to 50 | 115 | 21.6% | |
| More than 50 | 87 | 16.4% | |
| Sex | Male | 235 | 44.3% |
| Female | 296 | 55.7% | |
| Main Location of Practice | University Hospital | 335 | 63.1% |
| City Hospital | 154 | 29.0% | |
| Regional or Rural Hospital | 42 | 7.9% | |
| Years of Practice | Less than 5 | 184 | 34.7% |
| 5 to 10 | 145 | 27.3% | |
| 11 to 20 | 118 | 22.2% | |
| More than 20 | 84 | 15.8% |
| Survey Questions | Korea | Singapore | Thailand | |
|---|---|---|---|---|
| Rank in order of importance the following postoperative complications (1—most important; 8—least important) | Myocardial infarction | 2 | 2 | 1 |
| Stroke | 3 | 1 | 2 | |
| Hypoventilation & CO2 Retention | 1 | 3 | 3 | |
| Hypothermia | 5 | 5 | 4 | |
| Postoperative Delirium | 6 | 4 | 5 | |
| Pain (Visual Analog Scale score > 3) | 4 | 7 | 7 | |
| Postoperative Nausea and Vomiting | 8 | 6 | 6 | |
| Surgical Site Infection | 7 | 8 | 8 | |
| Rank in order of importance the following cognitive states (1—most important; 4—least important) | Intraoperative awareness | 1 | 1 | 1 |
| Postoperative cognitive dysfunction | 2 | 2 | 3 | |
| Postoperative delirium | 3 | 3 | 4 | |
| Emergence agitation | 4 | 4 | 2 |
| Survey Question | Number | Proportion | |
|---|---|---|---|
| What are the risk factors for developing postoperative delirium? Tick all that apply. | Age > 65 years | 521 | 98.1% |
| Only primary school education | 212 | 39.9% | |
| Poor nutritional status | 404 | 76.1% | |
| Frailty | 306 | 57.6% | |
| Anemia | 299 | 56.3% | |
| Diabetes | 258 | 48.6% | |
| Renal insufficiency | 280 | 52.7% | |
| Cognitive impairment | 482 | 90.8% | |
| Genetics | 238 | 44.8% | |
| Gut microbiome | 92 | 17.3% | |
| Others | 22 | 4.1% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Kim, J.; Lee, K.-Y.; Gan, T.J.; Lekprasert, V.; Laosuwan, P.; Chew, S.T.H.; Seet, E.; Lim, V.; Ti, L.K. Awareness and Perspectives among Asian Anesthesiologists on Postoperative Delirium: A Multinational Survey. J. Clin. Med. 2021, 10, 5769. https://doi.org/10.3390/jcm10245769
Lee H, Kim J, Lee K-Y, Gan TJ, Lekprasert V, Laosuwan P, Chew STH, Seet E, Lim V, Ti LK. Awareness and Perspectives among Asian Anesthesiologists on Postoperative Delirium: A Multinational Survey. Journal of Clinical Medicine. 2021; 10(24):5769. https://doi.org/10.3390/jcm10245769
Chicago/Turabian StyleLee, Hyungmook, Jeongmin Kim, Ki-Young Lee, Tong J. Gan, Varinee Lekprasert, Prok Laosuwan, Sophia Tsong Huey Chew, Edwin Seet, Vera Lim, and Lian Kah Ti. 2021. "Awareness and Perspectives among Asian Anesthesiologists on Postoperative Delirium: A Multinational Survey" Journal of Clinical Medicine 10, no. 24: 5769. https://doi.org/10.3390/jcm10245769