
Heart Rate in Patients with SARS-CoV-2 Infection: Prevalence of High Values at Discharge and Relationship with Disease Severity

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
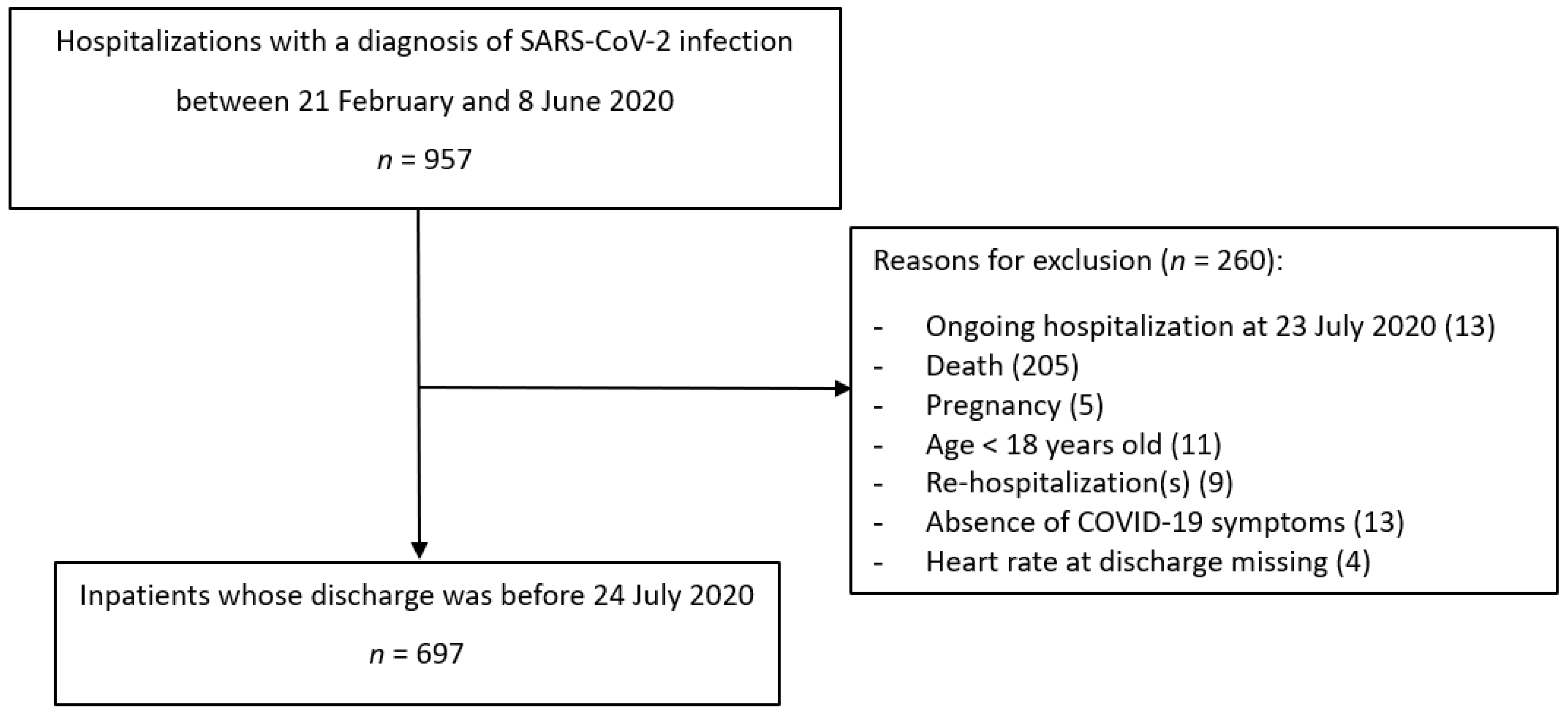
2.1. Study Population
2.2. Outcome and Predictor Measurements
2.3. Compliance with Ethical Standards
2.4. Statistical Analysis
3. Results
3.1. Population Characteristics
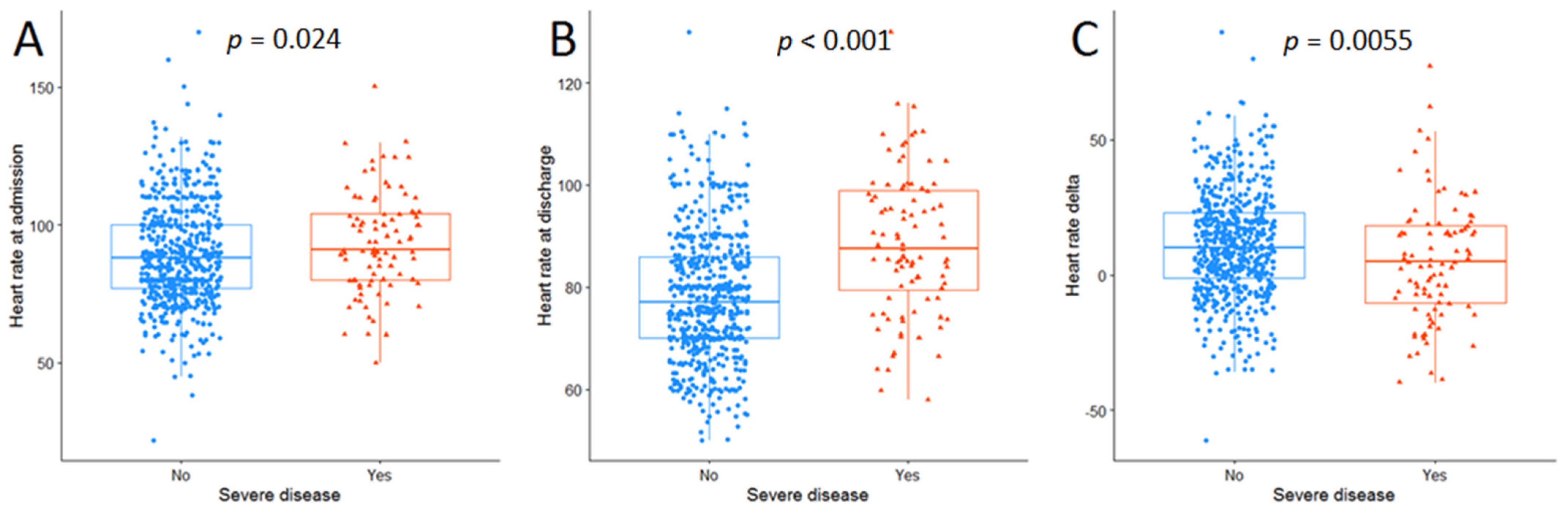
3.2. Elevated Heart Rate at Discharge
3.3. Multipredictor Analysis
4. Discussion
5. Conclusions
6. Future Research
- Post-discharge follow-up with HR evaluation is needed in order to understand persistence over time of sinus tachycardia.
- Furthermore, from post-discharge HR evaluation and subsequent mortality also information on its prognostic implication could be derived.
- A better autonomic function assessment should be done in the acute phase and post-discharge in order to confirm the hypothesis that autonomic dysfunction could be implicated in persistent sinus tachycardia.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lakkireddy, D.R.; Chung, M.K.; Gopinathannair, R.; Patton, K.K.; Gluckman, T.J.; Turagam, M.; Cheung, J.; Patel, P.; Sotomonte, J.; Lampert, R.; et al. Guidance for Cardiac Elec-trophysiology During the COVID-19 Pandemic from the Heart Rhythm Society COVID-19 Task Force; Electrophysiology Section of the American College of Cardiology; and the Electrocardiography and Arrhythmias Committee of the Council on Clinical Cardiology, American Heart Association. Circulation 2020, 141, e823–e831. [Google Scholar]
- Genovesi, S.; Rebora, P.; Occhino, G.; Rossi, E.; Maloberti, A.; Belli, M.; Bonfanti, P.; Giannattasio, C.; Rossetti, C.; Epis, O.M.; et al. Atrial Fibrillation and Clinical Outcomes in a Cohort of Hospitalized Patients with SARS-CoV-2 Infection and Chronic Kidney Disease. J. Clin. Med. 2021, 10, 4108. [Google Scholar] [CrossRef] [PubMed]
- Xiong, T.-Y.; Redwood, S.; Prendergast, B.; Chen, M. Coronaviruses and the cardiovascular system: Acute and long-term implications. Eur. Hear. J. 2020, 41, 1798–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kochi, A.N.; Tagliari, A.P.; Forleo, G.B.; Fassini, G.M.; Tondo, C. Cardiac and arrhythmic complications in patients with COVID-19. J. Cardiovasc. Electrophysiol. 2020, 31, 1003–1008. [Google Scholar] [CrossRef] [Green Version]
- Barnaby, D.P.; Fernando, S.M.; Herry, C.L.; Scales, N.B.; Gallagher, E.J.; Seely, A.J.E. Heart Rate Variability, Clinical and Laboratory Measures to Predict Future Deterioration in Patients Presenting with Sepsis. Shock. 2019, 51, 416–422. [Google Scholar] [CrossRef]
- De Castilho, F.M.; Ribeiro, A.L.P.; Nobre, V.; Barros, G.; de Sousa, M.R. Heart rate variability as predictor of mortality in sepsis: A systematic review. PLoS ONE 2018, 13, e0203487. [Google Scholar] [CrossRef]
- Bhattacharjee, P.; Edelson, D.P.; Churpek, M.M. Identifying Patients with Sepsis on the Hospital Wards. Chest 2017, 151, 898–907. [Google Scholar] [CrossRef] [Green Version]
- Wei, C.; Al Kattani, N.; Louis, H.; Albuisson, E.; Levy, B.; Kimmoun, A. If Channel Inhibition with Ivabradine Does Not Im-prove Cardiac and Vascular Function in Experimental Septic Shock. Shock 2016, 46, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Schortgen, F.; Charles-Nelson, A.; Bouadma, L.; Bizouard, G.; Brochard, L.; Katsahian, S. Respective impact of lowering body temperature and heart rate on mortality in septic shock: Mediation analysis of a randomized trial. Intensiv. Care Med. 2015, 41, 1800–1808. [Google Scholar] [CrossRef]
- Badke, C.M.; Marsillio, L.E.; Weese-Mayer, D.E.; Sanchez-Pinto, L.N. Autonomic Nervous System Dysfunction in Pediatric Sepsis. Front. Pediatr. 2018, 6. [Google Scholar] [CrossRef]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic dysfunction in ‘long COVID’: Rationale, physiology and management strategies. Clin. Med. 2021, 21, e63–e67. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the man-agement of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Olshansky, B.; Sullivan, R.M. Inappropriate sinus tachycardia. Europace 2019, 21, 194–207. [Google Scholar] [CrossRef] [PubMed]
- Sheldon, R.S.; Grubb, B.P.; Olshansky, B.; Shen, W.K.; Calkins, H.; Brignole, M.; Raj, S.R.; Krahn, A.D.; Morillo, C.A.; Stewart, J.M.; et al. 2015 heart rhythm society expert con-sensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm 2015, 12, e41–e63. [Google Scholar] [CrossRef] [Green Version]
- Baig, A.M. Chronic COVID syndrome: Need for an appropriate medical terminology for long-COVID and COVID long-haulers. J. Med. Virol. 2021, 93, 2555–2556. [Google Scholar] [CrossRef] [PubMed]
- Halpin, S.; O’Connor, R.; Sivan, M. Long COVID and chronic COVID syndromes. J. Med. Virol. 2021, 93, 1242–1243. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.-T.; Yu, W.-C.; Mok, N.-S.; Tsui, P.-T.; Tong, W.-L.; Stella, W.C. Tachycardia amongst subjects recovering from severe acute respiratory syndrome (SARS). Int. J. Cardiol. 2005, 100, 167–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, C.-M.; Wong, R.S.-M.; Wu, E.B.; Kong, S.-L.; Wong, J.; Yip, G.W.-K.; Soo, Y.O.Y.; Chiu, M.L.S.; Chan, Y.-S.; Hui, D.; et al. Cardiovascular complications of severe acute respiratory syndrome. Postgrad. Med. J. 2006, 82, 140–144. [Google Scholar] [CrossRef] [Green Version]
- Lo, Y.L. COVID-19, fatigue, and dysautonomia. J. Med. Virol. 2020, 93, 1213. [Google Scholar] [CrossRef]
- Raj, S.R.; Arnold, A.C.; Barboi, A.; Claydon, V.E.; Limberg, J.K.; Lucci, V.E.M.; Numan, M.; Peltier, A.; Snapper, H.; Vernino, S. Long-COVID postural tachycardia syndrome: An American Autonomic Society statement. Clin. Auton. Res. 2021, 31, 365–368. [Google Scholar] [CrossRef]
- Carod-Artal, F.J. Infectious diseases causing autonomic dysfunction. Clin. Auton. Res. 2017, 28, 67–81. [Google Scholar] [CrossRef]
- Katz, B.Z.; Stewart, J.M.; Shiraishi, Y.; Mears, C.J.; Taylor, R. Autonomic symptoms at baseline and following infectious mon-onucleosis in a prospective cohort of adolescents. Arch. Pediatr. Adolesc. Med. 2011, 165, 765–766. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, D.S. The extended autonomic system, dyshomeostasis, and COVID-19. Clin. Auton. Res. 2020, 30, 299–315. [Google Scholar] [CrossRef] [PubMed]
- Guilmot, A.; Slootjes, S.M.; Sellimi, A.; Bronchain, M.; Hanseeuw, B.; Belkhir, L.; Yombi, J.C.; De Greef, J.; Pothen, L.; Yildiz, H.; et al. Immune-mediated neurological syndromes in SARS-CoV-2-infected patients. J. Neurol. 2021, 268, 751–757. [Google Scholar] [CrossRef]
- Porzionato, A.; Emmi, A.; Barbon, S.; Boscolo-Berto, R.; Stecco, C.; Stocco, E.; Macchi, V.; De Caro, R. Sympathetic activation: A potential link be-tween comorbidities and COVID-19. FEBS J. 2020, 287, 3681–3688. [Google Scholar] [CrossRef] [PubMed]
- Del Rio, R.; Marcus, N.J.; Inestrosa, N.C. Potential Role of Autonomic Dysfunction in COVID-19 Morbidity and Mortality. Front. Physiol. 2020, 11, 561749. [Google Scholar] [CrossRef] [PubMed]
- Grassi, G.; Ram, V.S. Evidence for a critical role of the sympathetic nervous system in hypertension. J. Am. Soc. Hypertens. 2016, 10, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Gronda, E.; Brambilla, G.; Seravalle, G.; Maloberti, A.; Cairo, M.; Costantino, G.; Lovett, E.; Vanoli, E.; Mancia, G.; Grassi, G. Effects of chronic carotid baroreceptor activation on arterial stiffness in severe heart failure. Clin. Res. Cardiol. 2016, 105, 838–846. [Google Scholar] [CrossRef]
- Seravalle, G.; Quarti-Trevano, F.; Dell’Oro, R.; Gronda, E.; Spaziani, D.; Facchetti, R.; Cuspidi, C.; Mancia, G.; Grassi, G. Sympathetic and baroreflex alterations in congestive heart failure with preserved, midrange and reduced ejection fraction. J. Hypertens. 2019, 37, 443–448. [Google Scholar] [CrossRef]
- Ruzzenenti, G.; Maloberti, A.; Giani, V.; Biolcati, M.; Leidi, F.; Monticelli, M.; Grasso, E.; Cartella, I.; Palazzini, M.; Garatti, L.; et al. COVID and Cardiovascular Diseases: Direct and Indirect Damages and Future Perspective. High Blood Press. Cardiovasc. Prev. 2021, 28, 439–445. [Google Scholar] [CrossRef]
- Trevano, F.Q.; Seravalle, G.; Macchiarulo, M.; Villa, P.; Valena, C.; Dell’Oro, R.; Mancia, G.; Grassi, G. Reliability of heart rate as neuroad-renergic marker in the metabolic syndrome. J. Hypertens. 2017, 35, 1685–1690. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villareal, R.P.; Liu, B.C.; Massumi, A. Heart rate variability and cardiovascular mortality. Curr. Atheroscler. Rep. 2002, 4, 120–127. [Google Scholar] [CrossRef]
- Hirten, R.P.; Danieletto, M.; Tomalin, L.; Choi, K.H.; Zweig, M.; Golden, E.; Kaur, S.; Helmus, D.; Biello, A.; Pyzik, R.; et al. Use of Physiological Data from a Wearable Device to Identify SARS-CoV-2 Infection and Symptoms and Predict COVID-19 Diagnosis: Observational Study. J. Med. Internet Res. 2021, 23, e26107. [Google Scholar] [CrossRef] [PubMed]
- Bajić, D.; Đajić, V.; Milovanović, B. Entropy Analysis of COVID-19 Cardiovascular Signals. Entropy 2021, 23, 87. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall n = 697 | HR ≤ 100 bpm 659 (94.5%) | HR > 100 bpm 38 (5.5%) | p * | |
|---|---|---|---|---|
| Gender, female, n (%) | 278 (39.9) | 266 (40.4) | 12 (31.6) | 0.365 |
| Age, years, median (Q1, Q3) | 59 (49, 74) | 60 (50, 74) | 54 (37, 65) | 0.004 |
| Symptom onset before hospital admission, days, median (Q1, Q3) | 7 (4, 10) | 7 (4, 10) | 7 (4, 10) | 0.545 |
| COVID-19 pulmonary disease, n (%) | 590 (84.6) | 558 (84.7) | 32 (84.2) | 0.99 |
| Severe disease, n (%) | 92 (13.2) | 78 (11.8) | 14 (36.8) | <0.001 |
| Thrombotic event, n (%) | 93 (13.3) | 85 (12.9) | 8 (21.1) | 0.233 |
| Length of hospitalization, days, median (Q1, Q3) | 15 (10, 25) | 15 (9, 24) | 21.5 (10.5, 34) | 0.036 |
| Charlson Comorbidity Index, median (Q1, Q3) | 2 (1, 4) | 2 (1, 4) | 1 (0, 3) | 0.002 |
| History of myocardial infarction, n (%) | 46 (6.6) | 45 (6.8) | 1 (2.6) | 0.497 |
| Congestive heart failure, n (%) | 32 (4.6) | 32 (4.9) | 0 (0.0) | 0.32 |
| Permanent atrial fibrillation, n (%) | 54 (7.7) | 53 (8.0) | 1 (2.6) | 0.368 |
| Chronic obstructive pulmonary disease, n (%) | 41 (5.9) | 39 (5.9) | 2 (5.3) | 0.99 |
| COVID-19 treatments | 517 (74.2) | 493 (74.8) | 24 (63.2) | 0.160 |
| Lopinavir/ritonavir, n (%) | 257 (36.9) | 245 (37.2) | 12 (31.6) | 0.601 |
| Azithromycin, n (%) | 167 (24.0) | 160 (24.3) | 7 (18.4) | 0.531 |
| Hydroxychloroquine or chloroquine, n (%) | 488 (70.0) | 466 (70.7) | 22 (57.9) | 0.135 |
| Tocilizumab, n (%) | 73 (10.5) | 65 (9.9) | 8 (21.1) | 0.055 |
| Corticosteroids, n (%) | 278 (39.9) | 261 (39.7) | 17 (44.7) | 0.653 |
| Drugs acting on heart rate | 216 (31.0) | 209 (31.7) | 7 (18.4) | 0.123 |
| Beta-blockers, n (%) | 201 (28.8) | 194 (29.4) | 7 (18.4) | 0.203 |
| Antiarrhythmic, n (%) | 40 (5.7) | 39 (5.9) | 1 (2.6) | 0.625 |
| Ivabradine, n (%) | 3 (0.4) | 3 (0.5) | 0 (0.0) | 0.99 |
| Digoxin, n (%) | 16 (2.3) | 15 (2.3) | 1 (2.6) | 0.99 |
| Heart rate at admission, bpm, median (Q1, Q3) | 88 (78, 101) | 88 (77, 101) | 95 (80, 104) | 0.037 |
| Oxygen saturation at admission, %, median (Q1, Q3) | 96 (93, 98) | 96 (93, 98) | 94 (92, 97) | 0.253 |
| Systolic blood pressure at admission, mmHg, median (Q1, Q3) | 130 (120, 149) | 130 (120, 150) | 123 (119, 140) | 0.174 |
| Diastolic blood pressure at admission, mmHg, median (Q1, Q3) | 75 (70, 80) | 75 (70, 80) | 80 (70, 80) | 0.862 |
| Body-temperature at admission, Celsius, median (Q1, Q3) | 36.8 (36.1, 37.7) | 36.7 (36.1, 37.6) | 37.2 (36.5, 38.0) | 0.044 |
| Hemoglobin at admission, g/dL, median (Q1, Q3) | 13.5 (12.1, 14.5) | 13.5 (12.2, 14.6) | 12.9 (11.9, 13.8) | 0.099 |
| C-reactive protein at admission, mg/dL, median (Q1, Q3) | 4.6 (1.4, 9.5) | 4.3 (1.4, 9.3) | 8.4 (4.7, 13.3) | 0.002 |
| White blood cell count at admission, 103/mm3, median (Q1, Q3) | 6.64 (4.84, 9.25) | 6.53 (4.82, 9.31) | 7.77 (5.62, 9.20) | 0.16 |
| Oxygen saturation at discharge, %, median (Q1, Q3) | 97 (96, 98) | 97 (96, 98) | 97 (95, 98) | 0.052 |
| Systolic blood pressure at discharge, mmHg, median (Q1, Q3) | 120 (110, 130) | 120 (110, 130) | 120 (110, 128.75) | 0.169 |
| Diastolic blood pressure at discharge, mmHg, median (Q1, Q3) | 70 (70, 80) | 70 (70, 80) | 70 (65, 80) | 0.516 |
| Body-temperature at discharge, Celsius, median (Q1, Q3) | 36.0 (36.0, 36.2) | 36.0 (36.0, 36.2) | 36.0 (36.0, 36.5) | 0.09 |
| Hemoglobin at discharge, g/dL, median (Q1, Q3) | 12.1 (10.7, 13.2) | 12.1 (10.8, 13.2) | 11.6 (10.0, 12.7) | 0.103 |
| C-reactive protein at discharge, mg/dL, median (Q1, Q3) | 0.7 (0.2, 2.0) | 0.6 (0.2, 1.9) | 0.9 (0.2, 3.2) | 0.787 |
| White blood cell count at discharge, 103/mm3, median (Q1, Q3) | 6.59 (5.24, 8.10) | 6.46 (5.24, 8.05) | 7.43 (6.83, 8.46) | 0.066 |
| At Admission | At Discharge | Mean Variation * (95% CI) | |
|---|---|---|---|
| Heart rate, bpm, median (Q1, Q3) | 88 (78, 101) | 79 (70, 88) | −10 (−12, −9) |
| Mean (SD) | 90 (18) | 80 (2) | |
| Oxygen saturation, %, median (Q1, Q3) | 96 (93, 98) | 97 (96, 98) | +1.9 (+1.6, +2.2) |
| Mean (SD) | 95 (4) | 97 (2) | |
| Systolic blood pressure, mmHg, median (Q1, Q3) | 130 (120, 149] | 120 (110, 130] | −12 (−14, −10) |
| Mean (SD) | 133 (23) | 122 (15) | |
| Diastolic blood pressure, mmHg, median (Q1, Q3) | 75 (70, 80) | 70 (70, 80) | −2 (−3, −1) |
| Mean (SD) | 75 (12) | 73 (9) | |
| Body-temperature, Celsius, median (Q1, Q3) | 36.8 (36.1, 37.7) | 36.0 (36.0, 36.2) | −0.9 (−1.0, −0.8) |
| Mean (SD) | 37.0 (1.0) | 36.1 (0.4) | |
| Hemoglobin, g/dL, median (Q1, Q3) | 13.5 (12.1, 14.5) | 12.1 (10.7, 13.2) | −1.2 (−1.3, −1.1) |
| Mean (SD) | 13.2 (1.9) | 12.0 (1.8) | |
| C-reactive protein, mg/dL, median (Q1, Q3) | 4.6 (1.4, 9.67) | 0.7 (0.2, 2.0) | −5.1 (−5.6, −4.5) |
| Mean (SD) | 6.7 (6.9) | 1.8 (2.8) | |
| White blood cell count, 103/mm3, median (Q1, Q3) | 6.64 (4.85, 9.25) | 6.59 (5.24, 8.10) | −0.64 (−0.95, −0.34) |
| Mean (SD) | 7.66 (4.73) | 7.06 (3.94) |
| Models Adjusted Only by Heart Rate at Admission | Fully Adjusted Model * | |||
|---|---|---|---|---|
| Coefficient (95% CI) | p | Coefficient (95% CI) | p | |
| Heart rate at admission, per bpm increase | 0.17 (0.13; 0.23) | <0.001 | 0.17 (0.11; 0.22) | <0.001 |
| Age, per year increase | −0.10 (−0.16; −0.04) | <0.001 | −0.03 (−0.12; 0.06) | 0.511 |
| Gender, female as reference | 0.15 (−1.78; 2.08) | 0.878 | −0.08 (−2.11; 1.94) | 0.935 |
| Charlson Comorbidity Index, per unit increase | −0.77 (−1.13; −0.41) | <0.001 | −0.36 (−0.91; 0.19) | 0.195 |
| Oxygen saturation, %, per unit increase | −0.23 (−0.48; −0.02) | 0.073 | −0.09 (−0.36; 0.18) | 0.506 |
| Systolic blood pressure, per 1 mmHg increase | −0.041 (−0.081; −0.001) | 0.046 | −0.010 (−0.051; 0.032) | 0.640 |
| Body-temperature Celsius, per unit increase | 0.19 (−0.80; 1.18) | 0.703 | −0.47 (−1.47; 0.52) | 0.348 |
| Hemoglobin, per g/dL increase | −0.52 (−1.02; −0.03) | 0.039 | −0.64 (−1.19; −0.09) | 0.023 |
| Severe disease, absence as reference | 9.64 (6.94; 12.35) | <0.001 | 8.42 (5.39; 11.45) | <0.001 |
| COVID-19 pulmonary disease, absence as reference | 1.58 (−1.05; 4.22) | 0.239 | 1.36 (−1.48; 4.20) | 0.348 |
| Drugs acting on heart rate, absence as reference | −2.67 (−4.73; −0.62) | 0.011 | −1.84 (−4.01; 0.33) | 0.097 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maloberti, A.; Ughi, N.; Bernasconi, D.P.; Rebora, P.; Cartella, I.; Grasso, E.; Lenoci, D.; Del Gaudio, F.; Algeri, M.; Scarpellini, S.; et al. Heart Rate in Patients with SARS-CoV-2 Infection: Prevalence of High Values at Discharge and Relationship with Disease Severity. J. Clin. Med. 2021, 10, 5590. https://doi.org/10.3390/jcm10235590
Maloberti A, Ughi N, Bernasconi DP, Rebora P, Cartella I, Grasso E, Lenoci D, Del Gaudio F, Algeri M, Scarpellini S, et al. Heart Rate in Patients with SARS-CoV-2 Infection: Prevalence of High Values at Discharge and Relationship with Disease Severity. Journal of Clinical Medicine. 2021; 10(23):5590. https://doi.org/10.3390/jcm10235590
Chicago/Turabian StyleMaloberti, Alessandro, Nicola Ughi, Davide Paolo Bernasconi, Paola Rebora, Iside Cartella, Enzo Grasso, Deborah Lenoci, Francesca Del Gaudio, Michela Algeri, Sara Scarpellini, and et al. 2021. "Heart Rate in Patients with SARS-CoV-2 Infection: Prevalence of High Values at Discharge and Relationship with Disease Severity" Journal of Clinical Medicine 10, no. 23: 5590. https://doi.org/10.3390/jcm10235590