
Effect of Dexamethasone Combination with Gentamicin in Chemical Labyrinthectomy on Hearing Preservation and Vertigo Control in Patients with Unilateral Meniere’s Disease: A Randomized Controlled Clinical Trial


Abstract
:1. Introduction
2. Materials and Methods
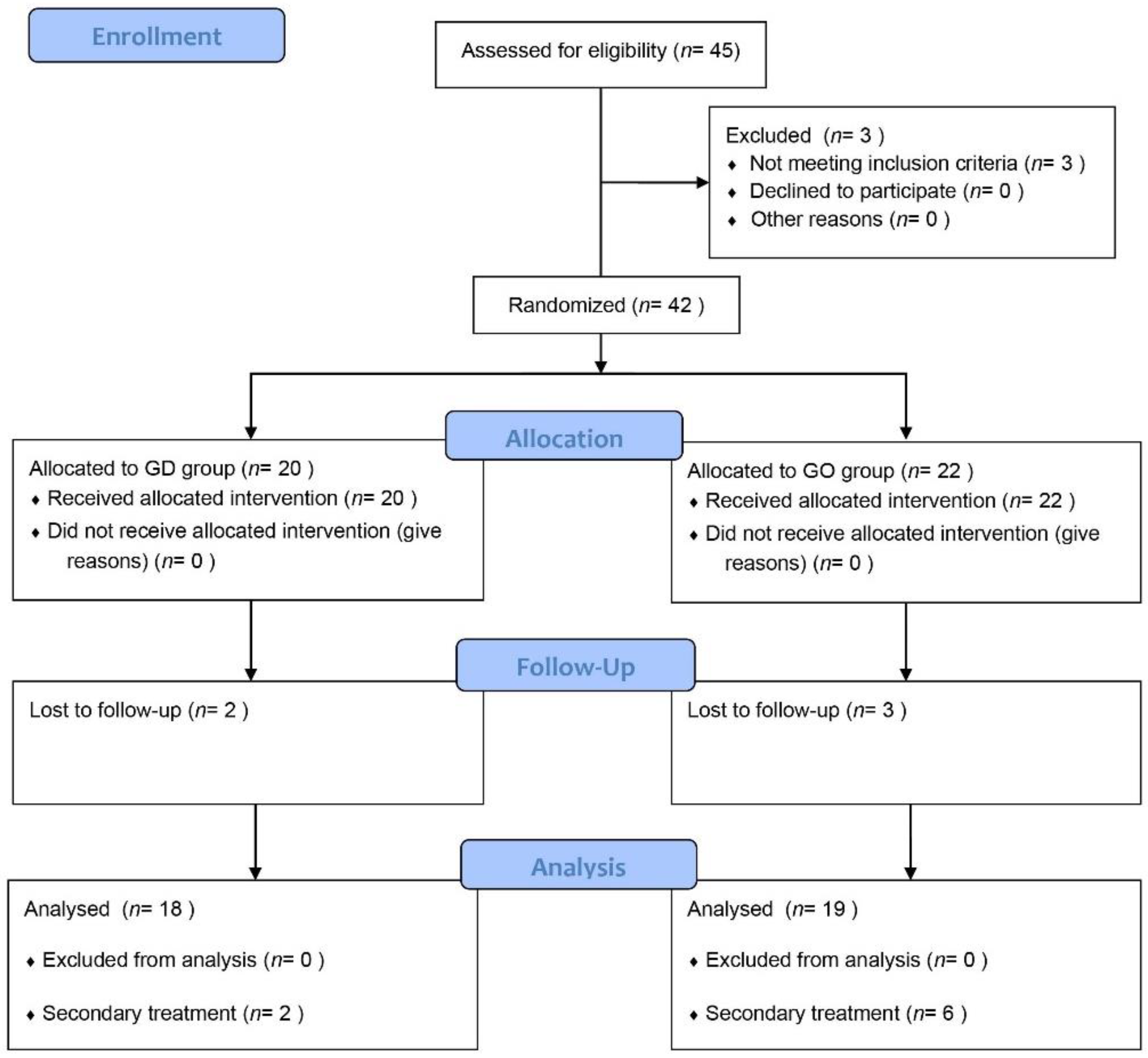
2.1. Patient Enrollment
2.2. Patient Grouping, Randomization, and Power Analysis
2.3. Surgical Procedure and Follow-Up
2.4. Outcome Measurement
2.5. Statistical Analysis
3. Results
3.1. Information of Participants
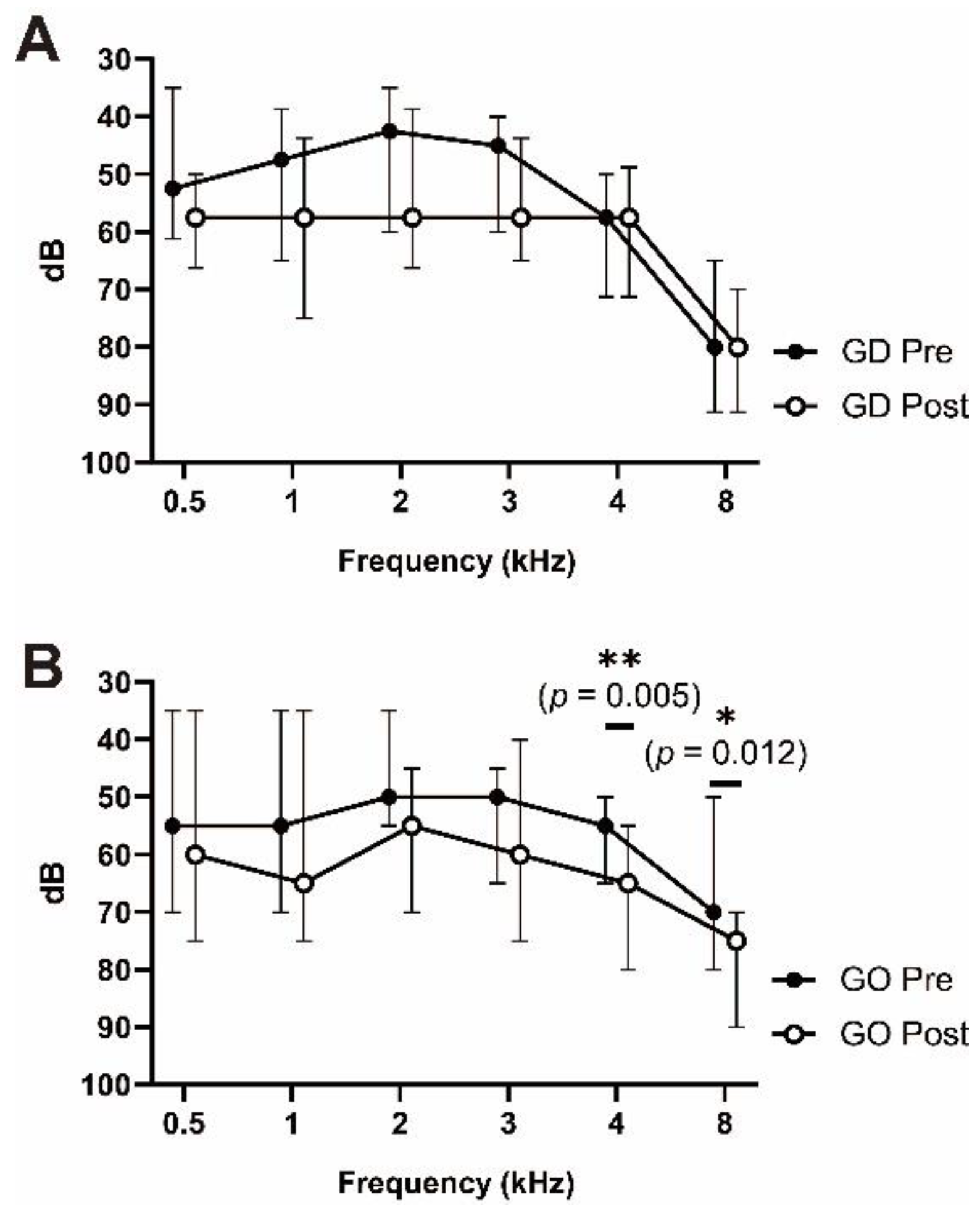
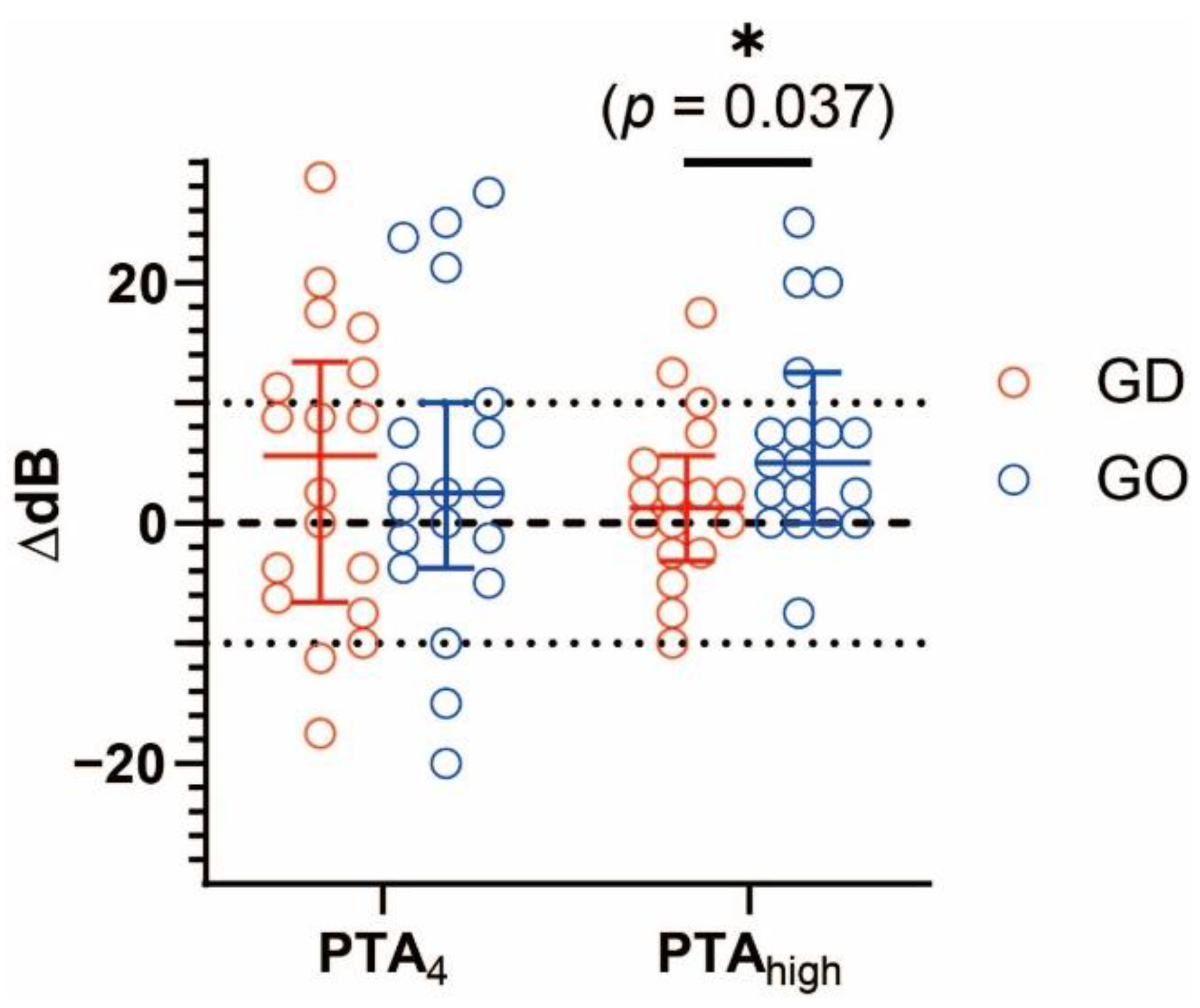
3.2. Hearing Preservation
3.3. Secondary Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lopez-Escamez, J.A.; Carey, J.; Chung, W.H.; Goebel, J.A.; Magnusson, M.; Mandala, M.; Newman-Toker, D.E.; Strupp, M.; Suzuki, M.; Trabalzini, F.; et al. Diagnostic criteria for meniere’s disease. J. Vestibul. Res. 2015, 25, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Espinosa-Sanchez, J.M.; Lopez-Escamez, J.A. The pharmacological management of vertigo in meniere disease. Expert Opin. Pharm. 2020, 21, 1753–1763. [Google Scholar] [CrossRef] [PubMed]
- Basura, G.J.; Adams, M.E.; Monfared, A.; Schwartz, S.R.; Antonelli, P.J.; Burkard, R.; Bush, M.L.; Bykowski, J.; Colandrea, M.; Derebery, J.; et al. Clinical practice guideline: Meniere’s disease. Otolaryngol.-Head Neck Surg. 2020, 162, S1–S55. [Google Scholar] [CrossRef] [Green Version]
- Fowler, E.P., Jr. Streptomycin treatment of vertigo. Trans. Am. Acad. Ophthalmol. Otolaryngol. 1948, 52, 293–301. [Google Scholar] [PubMed]
- Rutka, J. Aminoglycoside vestibulotoxicity. Adv. Otorhinolaryngol. 2019, 82, 101–110. [Google Scholar]
- Kalkandelen, S.; Selimoglu, E.; Erdogran, F.; Ucuncu, H.; Altas, E. Comparative cochlear toxicities of streptomycin, gentamicin, amikacin and netilmicin in guinea-pigs. J. Int. Med. Res. 2002, 30, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Mulheran, M.; Degg, C.; Burr, S.; Morgan, D.W.; Stableforth, D.E. Occurrence and risk of cochleotoxicity in cystic fibrosis patients receiving repeated high-dose aminoglycoside therapy. Antimicrob. Agents Chemother. 2001, 45, 2502–2509. [Google Scholar] [CrossRef] [Green Version]
- Casani, A.P.; Piaggi, P.; Cerchiai, N.; Seccia, V.; Franceschini, S.S.; Dallan, I. Intratympanic treatment of intractable unilateral meniere disease: Gentamicin or dexamethasone? A randomized controlled trial. Otolaryngol.-Head Neck Surg. 2012, 146, 430–437. [Google Scholar] [CrossRef]
- Vlastarakos, P.V.; Iacovou, E.; Nikolopoulos, T.P. Is gentamycin delivery via sustained-release vehicles a safe and effective treatment for refractory meniere’s disease? A critical analysis of published interventional studies. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 1309–1315. [Google Scholar] [CrossRef]
- Salt, A.N.; Hirose, K. Communication pathways to and from the inner ear and their contributions to drug delivery. Hear. Res. 2018, 362, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Salt, A.N.; Gill, R.M.; Plontke, S.K. Dependence of hearing changes on the dose of intratympanically applied gentamicin: A meta-analysis using mathematical simulations of clinical drug delivery protocols. Laryngoscope 2008, 118, 1793–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Oh, S.H.; Kim, T.H.; Go, Y.Y.; Song, J.J. Anti-apoptotic effect of dexamethasone in an ototoxicity model. Biomater. Res. 2017, 21, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gul, A.; Sengul, E.; Yilmaz, B.; Ozkurt, F.E.; Akdag, M.; Keles, A.; Topcu, I. The protective effect of intratympanic dexamethasone on streptomycin ototoxicity in rats. Ear Nose Throat J. 2017, 96, E12–E17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parnes, L.S.; Sun, A.H.; Freeman, D.J. Corticosteroid pharmacokinetics in the inner ear fluids: An animal study followed by clinical application. Laryngoscope 1999, 109, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Schmuziger, N.; Probst, R.; Smurzynski, J. Test-retest reliability of pure-tone thresholds from 0.5 to 16 khz using sennheiser hda 200 and etymotic research er-2 earphones. Ear Hear. 2004, 25, 127–132. [Google Scholar] [CrossRef]
- Choudhary, A.; Das Biswas, K.; Basak, B.; Ghosh, S.K.; Bhattacharya, D. Intratympanic low dose gentamicin in intractable meniere’s disease- chemical labyrinthectomy revisited. J. Evol. Med. Dent. Sci. 2019, 8, 1843–1847. [Google Scholar] [CrossRef]
- Monsell, E.M.; Balkany, T.A.; Gates, G.A.; Goldenberg, R.A.; Meyerhoff, W.L.; House, J.W. Committee on hearing and equilibrium guidelines for the diagnosis and evaluation of therapy in menieres-disease. Otolaryngol.-Head Neck Surg. 1995, 113, 181–185. [Google Scholar]
- Lee, J.J.; Jang, J.H.; Choo, O.S.; Lim, H.J.; Choung, Y.H. Steroid intracochlear distribution differs by administration method: Systemic versus intratympanic injection. Laryngoscope 2018, 128, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Carey, J. Intratympanic gentamicin for the treatment of meniere’s disease and other forms of peripheral vertigo. Otolaryngol. Clin. N. Am. 2004, 37, 1075–1090. [Google Scholar] [CrossRef]
- Plontke, S.K.; Wood, A.W.; Salt, A.N. Analysis of gentamicin kinetics in fluids of the inner ear with round window administration. Otol. Neurotol. 2002, 23, 967–974. [Google Scholar] [CrossRef]
- Jensen-Smith, H.C.; Hallworth, R.; Nichols, M.G. Gentamicin rapidly inhibits mitochondrial metabolism in high-frequency cochlear outer hair cells. PLoS ONE 2012, 7, e38471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Himeno, C.; Komeda, M.; Izumikawa, M.; Takemura, K.; Yagi, M.; Weiping, Y.; Doi, T.; Kuriyama, H.; Miller, J.M.; Yamashita, T. Intra-cochlear administration of dexamethasone attenuates aminoglycoside ototoxicity in the guinea pig. Hear. Res. 2002, 167, 61–70. [Google Scholar] [CrossRef]
- Park, M.K.; Lee, B.D.; Chae, S.W.; Chi, J.; Kwon, S.K.; Song, J.J. Protective effect of necrox, a novel necroptosis inhibitor, on gentamicin-induced ototoxicity. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 1265–1269. [Google Scholar] [CrossRef] [PubMed]
- Sha, S.H.; Schacht, J. Antioxidants attenuate gentamicin-induced free radical formation in vitro and ototoxicity in vivo: D-methionine is a potential protectant. Hear. Res. 2000, 142, 34–40. [Google Scholar] [CrossRef]
- Tahera, Y.; Meltser, I.; Johansson, P.; Bian, Z.; Stierna, P.; Hansson, A.C.; Canlon, B. Nf-kappab mediated glucocorticoid response in the inner ear after acoustic trauma. J. Neurosci. Res. 2006, 83, 1066–1076. [Google Scholar] [CrossRef] [PubMed]
- Kolls, J.; Xie, J.; LeBlanc, R.; Malinski, T.; Nelson, S.; Summer, W.; Greenberg, S.S. Rapid induction of messenger rna for nitric oxide synthase ii in rat neutrophils in vivo by endotoxin and its suppression by prednisolone. Proc. Soc. Exp. Biol. Med. 1994, 205, 220–229. [Google Scholar] [CrossRef]
- Nevoux, J.; Viengchareun, S.; Lema, I.; Lecoq, A.L.; Ferrary, E.; Lombes, M. Glucocorticoids stimulate endolymphatic water reabsorption in inner ear through aquaporin 3 regulation. Pflüg. Arch.-Eur. J. Physiol. 2015, 467, 1931–1943. [Google Scholar] [CrossRef] [PubMed]
- Curtis, L.M.; Ten Cate, W.J.; Rarey, K.E. Dynamics of na,k-atpase sites in lateral cochlear wall tissues of the rat. Eur. Arch. Otorhinolaryngol. 1993, 250, 265–270. [Google Scholar] [CrossRef]
- Kim, S.H.; Marcus, D.C. Regulation of sodium transport in the inner ear. Hear. Res. 2011, 280, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Phillips, J.S.; Westerberg, B. Intratympanic steroids for meniere’s disease or syndrome. Cochrane Database Syst. Rev. 2011, 6, CD008514. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Fu, J.; Lin, H.; Shen, C.; Wang, X.; Wu, J. The clinical outcomes after intratympanic gentamicin injection to treat meniere’s disease: A meta-analysis. Otol. Neurotol. 2019, 40, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Perez-Garrigues, H.; Lopez-Escamez, J.A.; Perez, P.; Sanz, R.; Orts, M.; Marco, J.; Barona, R.; Tapia, M.C.; Aran, I.; Cenjor, C.; et al. Time course of episodes of definitive vertigo in meniere’s disease. Arch. Otolaryngol. 2008, 134, 1149–1154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atrache Al Attrache, N.; Krstulovic, C.; Perez Guillen, V.; Morera Perez, C.; Perez Garrigues, H. Response over time of vertigo spells to intratympanic dexamethasone treatment in meniere’s disease patients. J. Int. Adv. Otol. 2016, 12, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Wu, H.; Zhang, P.; Hou, D.M.; Chen, J.; Zhang, S.G. The pharmacokinetic profiles of dexamethasone and methylprednisolone concentration in perilymph and plasma following systemic and local administration. Acta Otolaryngol. 2008, 128, 496–504. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | GO Group (n = 19) | GD Group (n = 18) | * p-Value |
|---|---|---|---|
| Age, mean (SD), years | 55.05 (16.06) | 54.78 (15.13) | 0.958 a |
| Sex, male (%) | 7 (36.8) | 8 (44.4) | 0.743 |
| PTA4, mean (SD), dB | 51.38 (18.39) | 49.17 (16.56) | 0.703 a |
| 0.5 kHz | 53.42 (21.48) | 51.67 (17.90) | 0.789 a |
| 1 kHz | 53.16 (20.63) | 50.83 (18.81) | 0.723 a |
| 2 kHz | 47.89 (18.66) | 45.83 (16.56) | 0.725 a |
| 3 kHz | 51.05 (17.92) | 48.33 (17.41) | 0.643 a |
| PTAhigh | 59.34 (21.55) | 67.36 (19.26) | 0.223 b |
| 4 kHz | 52.89 (20.02) | 56.94 (18.56) | 0.580 b |
| 8 kHz | 65.79 (24.28) | 77.78 (22.18) | 0.126 a |
| CP value in caloric test before surgery, mean (SD), % | 44.15 (27.19) | 39.57 (24.22) | 0.593 a |
| Frequency of vertigo attacks, mean (SD), per month | 1.70 (1.27) | 1.97 (1.46) | 0.512 b |
| Disease duration to surgery (SD), days | 1723 (1524) | 1908 (1619) | 0.663 b |
| Characteristic | GO Group (n = 19) | GD Group (n = 18) | * p-Value |
|---|---|---|---|
| PTA4, mean (SD), ΔdB | 3.95 (13.22) | 4.17 (12.51) | 0.959 a |
| 0.5 kHz | 2.63 (18.44) | 3.61 (15.79) | 0.864 a |
| 1 kHz | 3.68 (16.15) | 4.72 (15.38) | 0.843 a |
| 2 kHz | 4.21 (11.82) | 5.28 (12.77) | 0.817 b |
| 3 kHz | 5.26 (13.49) | 3.06 (12.85) | 0.963 b |
| PTAhigh, mean (SD), ΔdB | 8.82 (12.81) | −0.42 (12.52) | 0.037 b* |
| 4 kHz | 8.42 (14.25) | −1.39 (13.91) | 0.049 b* |
| 8 kHz | 9.21 (15.12) | 0.56 (13.49) | 0.174 b |
| Change of CP value in caloric test, mean (SD), Δ% | 6.24 (31.95) | 21.05 (23.30) | 0.118 a |
| Characteristic | GO Group (n = 19) | GD Group (n = 18) | * p-Value |
|---|---|---|---|
| Secondary treatment required (%) | |||
| 2–6 months | 4 (21.05) | 1 (5.56) | 0.340 |
| 2–12 months | 6 (31.58) | 2 (11.11) | 0.232 |
| Complete control (%) a | |||
| 2–6 months | 8 (42.11) | 11 (61.11) | 0.330 |
| 2–12 months | 3 (15.79) | 9 (50.00) | 0.038 * |
| Treatment success (%) b | |||
| 2–6 months | 11 (57.89) | 17 (94.44) | 0.019 * |
| 2–12 months | 10 (52.63) | 15 (83.33) | 0.079 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, S.-H.; Lee, J.-M.; Lee, H.-J.; Na, G.; Kim, S.-H. Effect of Dexamethasone Combination with Gentamicin in Chemical Labyrinthectomy on Hearing Preservation and Vertigo Control in Patients with Unilateral Meniere’s Disease: A Randomized Controlled Clinical Trial. J. Clin. Med. 2021, 10, 5581. https://doi.org/10.3390/jcm10235581
Bae S-H, Lee J-M, Lee H-J, Na G, Kim S-H. Effect of Dexamethasone Combination with Gentamicin in Chemical Labyrinthectomy on Hearing Preservation and Vertigo Control in Patients with Unilateral Meniere’s Disease: A Randomized Controlled Clinical Trial. Journal of Clinical Medicine. 2021; 10(23):5581. https://doi.org/10.3390/jcm10235581
Chicago/Turabian StyleBae, Seong-Hoon, Jeon-Mi Lee, Hyun-Jin Lee, Gina Na, and Sung-Huhn Kim. 2021. "Effect of Dexamethasone Combination with Gentamicin in Chemical Labyrinthectomy on Hearing Preservation and Vertigo Control in Patients with Unilateral Meniere’s Disease: A Randomized Controlled Clinical Trial" Journal of Clinical Medicine 10, no. 23: 5581. https://doi.org/10.3390/jcm10235581