
Effect of Violet Light-Transmitting Eyeglasses on Axial Elongation in Myopic Children: A Randomized Controlled Trial


 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Organization
2.3. Participants and Sample Size
2.4. Randomization and Masking
2.5. Intervention
2.6. Procedure for Follow-Up Examinations
2.7. Outcomes
2.8. Statistical Analysis
3. Results
3.1. Flow of Participants
3.2. Participant Profiles
3.3. Adverse Events
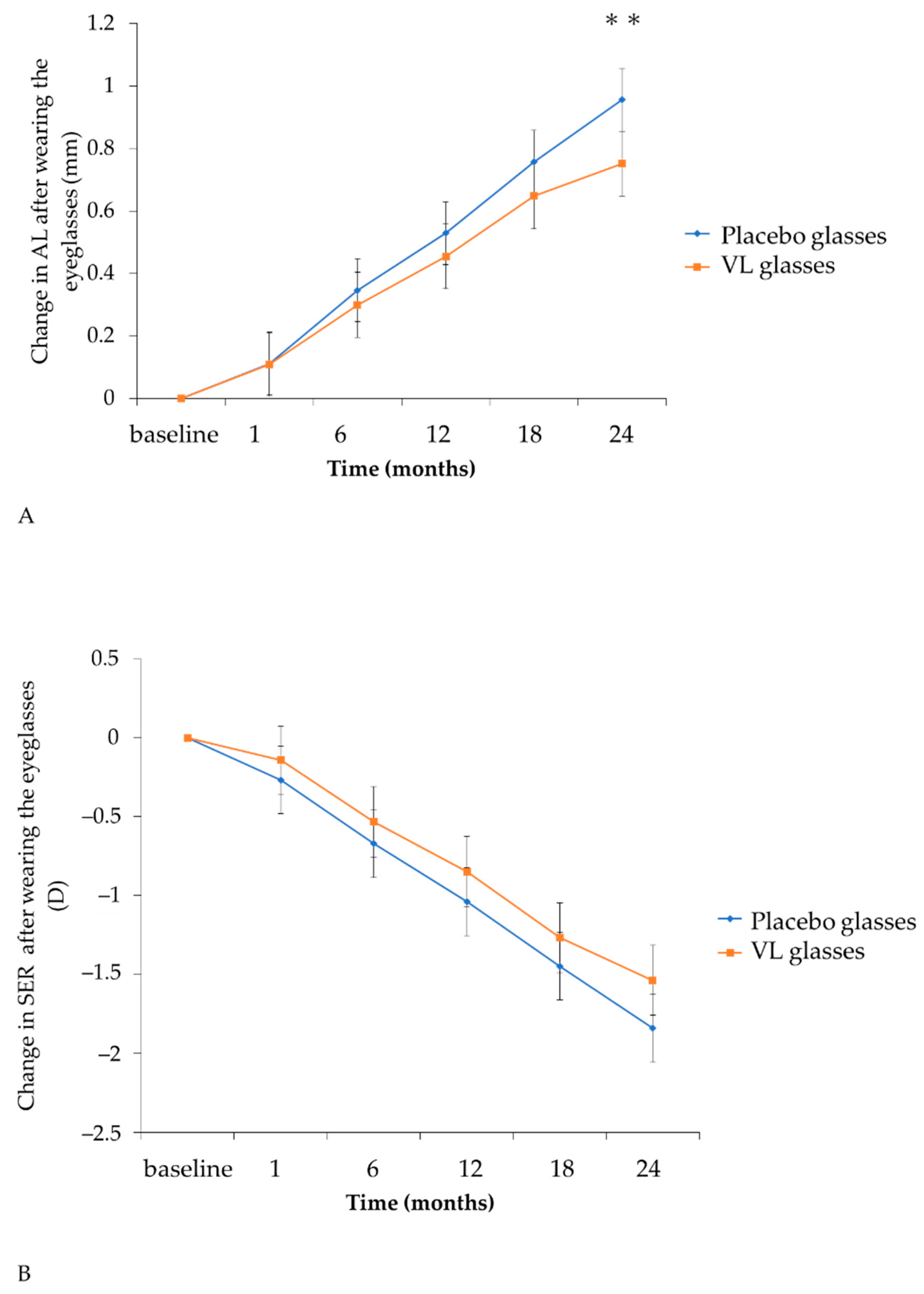
3.4. Comparison of Myopia Progression after 24 Months
4. Discussion
5. Conclusions
6. Patent
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Enthoven, C.A.; Tidessman, J.W.L.; Polling, J.R.; Tedja, M.S.; Raat, H.; Iglesias, A.I.; Verhoeven, V.J.M.; Klaver, C.C.W. Interaction between lifestyle and genetic susceptibility in myopia: The Generation R study. Eur. J. Epidemiol. 2019, 34, 777–784. [Google Scholar] [PubMed] [Green Version]
- Holden, B.A.; Jong, M.; Davis, S.; Wilson, D.; Fricke, T.; Resnikoff, S. Nearly 1 billion myopes at risk of myopia-related sight-threatening conditions by 2050–time to act now. Clin. Exp. Optom. 2015, 98, 491–493. [Google Scholar] [CrossRef] [PubMed]
- Bikbov, M.M.; Gilmanshin, T.R.; Kazakbaeva, G.M.; Zainullin, R.M.; Rakhimova, E.M.; Rusakova, I.A.; Bolshakova, N.I.; Safiullina, K.R.; Zaynetdinov, A.F.; Zinatullin, A.A.; et al. Prevalence of Myopic Maculopathy Among Adults in a Russian Population. JAMA Netw. Open 2020, 3, e200567. [Google Scholar] [CrossRef] [PubMed]
- Bikbov, M.M.; Kazakbaeva, G.M.; Rakhimova, E.M.; Rusakova, I.A.; Fakhretdinova, A.A.; Tuliakova, A.M.; Panda-Jonas, S.; Gilmanshin, T.R.; Zainullin, R.M.; Bolshakova, N.I.; et al. Prevalence Factors Associated With Vision Impairment and Blindness Among Individuals 85 Years and Older in Russia. JAMA Netw. Open 2021, 4, e2121138. [Google Scholar] [CrossRef] [PubMed]
- Iwase, A.; Araie, M.; Tomidokoro, A.; Yamamoto, T.; Shimizu, H.; Kitazawa, Y. Prevalence and causes of low vision and blindness in a Japanese adult population: The Tajimi Study. Ophthalmology 2006, 113, 1354–1362. [Google Scholar] [CrossRef]
- Bullimore, M.A.; Brennan, N.A. Myopia Control: Why Each Diopter Matters. Optom. Vis. Sci. 2019, 96, 463–465. [Google Scholar] [CrossRef] [PubMed]
- Bullimore, M.A.; Richdale, K. Myopia Control 2020: Where are we and where are we heading? Ophthalmic Physiol. Opt. 2020, 40, 254–270. [Google Scholar] [CrossRef]
- Saw, S.M.; Gazzard, G.; Shih-Yen, E.C.; Chua, W.H. Myopia and associated pathological complications. Ophthalmic Physiol. Opt. 2005, 25, 381–391. [Google Scholar] [CrossRef]
- Mutti, D.O.; Mitchell, G.L.; Moeschberger, M.L.; Jones, L.A.; Zadnik, K. Parental myopia, near work, school achievement, and children’s refractive error. Investig. Ophthalmol. Vis. Sci. 2002, 43, 3633–3640. [Google Scholar]
- Saw, S.M.; Shankar, A.; Tan, S.B.; Taylor, H.; Tan, D.T.; Stone, R.A.; Wong, T.Y. A cohort study of incident myopia in Singaporean children. Investig. Ophthalmol. Vis. Sci. 2006, 47, 1839–1844. [Google Scholar] [CrossRef] [Green Version]
- Ip, J.M.; Rose, K.A.; Morgan, I.G.; Burlutsky, G.; Mitchell, P. Myopia and the urban environment: Findings in a sample of 12-year-old Australian school children. Investig. Ophthalmol. Vis. Sci. 2008, 49, 3858–3863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ip, J.M.; Saw, S.M.; Rose, K.A.; Morgan, I.G.; Kifley, A.; Wang, J.J.; Mitchell, P. Role of near work in myopia: Findings in a sample of Australian school children. Investig. Ophthalmol. Vis. Sci. 2008, 49, 2903–2910. [Google Scholar] [CrossRef]
- Jones, L.A.; Sinnott, L.T.; Mutti, D.O.; Mitchell, G.L.; Moeschberger, M.L.; Zadnik, K. Parental history of myopia, sports and outdoor activities, and future myopia. Investig. Ophthalmol. Vis. Sci. 2007, 48, 3524–3532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, P.C.; Chen, C.T.; Lin, K.K.; Sun, C.C.; Kuo, C.N.; Huang, H.M.; Poon, Y.C.; Yang, M.L.; Chen, C.Y.; Huang, J.C.; et al. Myopia Prevention and Outdoor Light Intensity in a School-Based Cluster Randomized Trial. Ophthalmology 2018, 125, 1239–1250. [Google Scholar] [CrossRef] [Green Version]
- Cao, K.; Wan, Y.; Yusufu, M.; Wang, N. Significance of Outdoor Time for Myopia Prevention: A Systematic Review and Meta-Analysis Based on Randomized Controlled Trials. Ophthalmic Res. 2020, 63, 97–105. [Google Scholar] [CrossRef]
- Jin, J.X.; Hua, W.J.; Jiang, X.; Wu, X.Y.; Yang, J.W.; Gao, G.P.; Fang, Y.; Pei, C.L.; Wang, S.; Zhang, J.Z.; et al. Effect of outdoor activity on myopia onset and progression in school-aged children in northeast China: The Sujiatun Eye Care Study. BMC Ophthalmol. 2015, 15, 73. [Google Scholar] [CrossRef] [Green Version]
- He, M.; Xiang, F.; Zeng, Y.; Mai, J.; Chen, Q.; Zhang, J.; Smith, W.; Rose, K.; Morgan, I.G. Effect of Time Spent Outdoors at School on the Development of Myopia Among Children in China: A Randomized Clinical Trial. JAMA 2015, 314, 1142–1148. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.C.; Chen, C.T.; Chang, L.C.; Niu, Y.Z.; Chen, M.L.; Liao, L.L.; Rose, K.; Morgan, I.G. Increased Time Outdoors Is Followed by Reversal of the Long-Term Trend to Reduced Visual Acuity in Taiwan Primary School Students. Ophthalmology 2020, 127, 1462–1469. [Google Scholar] [CrossRef] [Green Version]
- Torii, H.; Kurihara, T.; Seko, Y.; Negishi, K.; Ohnuma, K.; Inaba, T.; Kawashima, M.; Jiang, X.; Kondo, S.; Miyauchi, M.; et al. Violet Light Exposure Can Be a Preventive Strategy Against Myopia Progression. EBioMedicine 2017, 15, 210–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, L.F.; Arumugam, B.; She, Z.; Ostrin, L.; Smith, E.L., 3rd. Narrow-band, long-wavelength lighting promotes hyperopia and retards vision-induced myopia in infant rhesus monkeys. Exp. Eye Res. 2018, 176, 147–160. [Google Scholar]
- Gawne, T.J.; Ward, A.H.; Norton, T.T. Long-wavelength (red) light produces hyperopia in juvenile and adolescent tree shrews. Vis. Res. 2017, 140, 55–65. [Google Scholar] [CrossRef]
- Foulds, W.S.; Barathi, V.A.; Luu, C.D. Progressive myopia or hyperopia can be induced in chicks and reversed by manipulation of the chromaticity of ambient light. Investig. Ophthalmol. Vis. Sci. 2013, 54, 8004–8012. [Google Scholar] [CrossRef] [Green Version]
- Kröger, R.H.; Fernald, R.D. Regulation of eye growth in the African cichlid fish Haplochromis burtoni. Vis. Res. 1994, 34, 1807–1814. [Google Scholar] [CrossRef]
- Strickland, R.; Landis, E.G.; Pardue, M.T. Short-Wavelength (Violet) Light Protects Mice From Myopia Through Cone Signaling. Investig. Ophthalmol. Vis. Sci. 2020, 61, 13. [Google Scholar] [CrossRef] [Green Version]
- Zou, L.; Zhu, X.; Liu, R.; Ma, F.; Yu, M.; Liu, H.; Dai, J. Effect of Altered Retinal Cones/Opsins on Refractive Development under Monochromatic Lights in Guinea Pigs. J. Ophthalmol. 2018, 2018, 9197631. [Google Scholar] [CrossRef]
- Jiang, X.; Pardue, M.T.; Mori, K.; Ikeda, S.I.; Torii, H.; D’Souza, S.; Lang, R.A.; Kurihara, T.; Tsubota, K. Violet light suppresses lens-induced myopia via neuropsin (OPN5) in mice. Proc. Natl. Acad. Sci. USA 2021, 118, e2018840118. [Google Scholar] [CrossRef]
- Nguyen, M.T.; Vemaraju, S.; Nayak, G.; Odaka, Y.; Buhr, E.D.; Alonzo, N.; Tran, U.; Batie, M.; Upton, B.A.; Darvas, M.; et al. An opsin 5-dopamine pathway mediates light-dependent vascular development in the eye. Nat. Cell Biol. 2019, 21, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Torii, H.; Ohnuma, K.; Kurihara, T.; Tsubota, K.; Negishi, K. Violet Light Transmission is Related to Myopia Progression in Adult High Myopia. Sci. Rep. 2017, 7, 14523. [Google Scholar] [CrossRef] [Green Version]
- Tarttelin, E.E.; Bellingham, J.; Hankins, M.W.; Foster, R.G.; Lucas, R.J. Neuropsin (Opn5): A novel opsin identified in mammalian neural tissue. FEBS Lett. 2003, 554, 410–416. [Google Scholar] [CrossRef]
- Zhang, K.X.; D’Souza, S.; Upton, B.A.; Kernodle, S.; Vemaraju, S.; Nayak, G.; Gaitonde, K.D.; Holt, A.L.; Linne, C.D.; Smith, A.N.; et al. Violet-light suppression of thermogenesis by opsin 5 hypothalamic neurons. Nature 2020, 585, 420–425. [Google Scholar] [CrossRef]
- Kanda, H.; Oshika, T.; Hiraoka, T.; Hasebe, S.; Ohno-Matsui, K.; Ishiko, S.; Hieda, O.; Torii, H.; Varnas, S.R.; Fujikado, T. Effect of spectacle lenses designed to reduce relative peripheral hyperopia on myopia progression in Japanese children: A 2-year multicenter randomized controlled trial. Jpn. J. Ophthalmol. 2018, 62, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Li, S.M.; Wu, S.S.; Kang, M.T.; Liu, Y.; Jia, S.M.; Li, S.Y.; Zhan, S.Y.; Liu, L.R.; Li, H.; Chen, W.; et al. Atropine slows myopia progression more in Asian than white children by meta-analysis. Optom. Vis. Sci. 2014, 91, 342–350. [Google Scholar] [CrossRef]
- Hsu, C.C.; Huang, N.; Lin, P.Y.; Fang, S.Y.; Tsai, D.C.; Chen, S.Y.; Tsai, C.Y.; Woung, L.C.; Chiou, S.H.; Liu, C.J. Risk factors for myopia progression in second-grade primary school children in Taipei: A population-based cohort study. Br. J. Ophthalmol. 2017, 101, 1611–1617. [Google Scholar] [CrossRef]
- Matsumura, S.; Lanca, C.; Htoon, H.M.; Brennan, N.; Tan, C.S.; Kathrani, B.; Chia, A.; Tan, D.; Sabanayagam, C.; Saw, S.M. Annual Myopia Progression and Subsequent 2-Year Myopia Progression in Singaporean Children. Transl. Vis. Sci. Technol. 2020, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.L., 3rd; Hung, L.F.; Arumugam, B.; Holden, B.A.; Neitz, M.; Neitz, J. Effects of Long-Wavelength Lighting on Refractive Development in Infant Rhesus Monkeys. Investig. Ophthalmol. Vis. Sci. 2015, 56, 6490–6500. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Qian, Y.F.; He, J.C.; Hu, M.; Zhou, X.T.; Dai, J.H.; Qu, X.M.; Chu, R.Y. Effects of different monochromatic lights on refractive development and eye growth in guinea pigs. Exp. Eye Res. 2011, 92, 447–453. [Google Scholar] [CrossRef]
- Jiang, L.; Zhang, S.; Schaeffel, F.; Xiong, S.; Zheng, Y.; Zhou, X.; Lu, F.; Qu, J. Interactions of chromatic and lens-induced defocus during visual control of eye growth in guinea pigs (Cavia porcellus). Vis. Res. 2014, 94, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Fujikado, T.; Ninomiya, S.; Kobayashi, T.; Suzaki, A.; Nakada, M.; Nishida, K. Effect of low-addition soft contact lenses with decentered optical design on myopia progression in children: A pilot study. Clin. Ophthalmol. 2014, 8, 1947–1956. [Google Scholar] [CrossRef] [Green Version]
- Lam, C.S.Y.; Tang, W.C.; Tse, D.Y.; Lee, R.P.K.; Chun, R.K.M.; Hasegawa, K.; Qi, H.; Hatanaka, T.; To, C.H. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: A 2-year randomised clinical trial. Br. J. Ophthalmol. 2020, 104, 363–368. [Google Scholar] [CrossRef] [Green Version]
- Hasebe, S.; Jun, J.; Varnas, S.R. Myopia control with positively aspherized progressive addition lenses: A 2-year, multicenter, randomized, controlled trial. Investig. Ophthalmol. Vis. Sci. 2014, 55, 7177–7188. [Google Scholar] [CrossRef]
- Yang, Z.; Lan, W.; Ge, J.; Liu, W.; Chen, X.; Chen, L.; Yu, M. The effectiveness of progressive addition lenses on the progression of myopia in Chinese children. Ophthalmic Physiol. Opt. 2009, 29, 41–48. [Google Scholar] [PubMed]
- Yam, J.C.; Jiang, Y.; Tang, S.M.; Law, A.K.P.; Chan, J.J.; Wong, E.; Ko, S.T.; Young, A.L.; Tham, C.C.; Chen, L.J.; et al. Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control. Ophthalmology 2019, 126, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Hieda, O.; Hiraoka, T.; Fujikado, T.; Ishiko, S.; Hasebe, S.; Torii, H.; Takahashi, H.; Nakamura, Y.; Sotozono, C.; Oshika, T.; et al. Efficacy and safety of 0.01% atropine for prevention of childhood myopia in a 2-year randomized placebo-controlled study. Jpn. J. Ophthalmol. 2021, 65, 315–325. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Category | All | Placebo | VL | p Value | |
|---|---|---|---|---|---|---|
| Number of cases | 113 | 57 | 56 | |||
| Age (years) | 9.4 ± 1.5 | 9.5 ± 1.5 | 9.3 ± 1.5 | 0.478 | † | |
| Sex | boys | 43 (38.1%) | 22 (38.6%) | 21 (37.5%) | 1.000 | †† |
| girls | 70 (61.9%) | 35 (61.4%) | 35 (62.5%) | |||
| Parental myopia | both parents | 56 (51.9%) | 24 (45.3%) | 32 (58.2%) | ||
| only father | 22 (20.4%) | 10 (18.9%) | 12 (21.8%) | 0.196 | †† | |
| only mother | 30 (17.4%) | 19 (35.8%) | 11 (20.0%) | |||
| Height (cm) | 135.3 ± 10.9 | 135.8 ± 9.9 | 134.7 ± 11.9 | 0.989 | † | |
| Weight (kg) | 31.16 ± 7.35 | 31.15 ± 6.86 | 31.17 ± 7.88 | 0.629 | † | |
| Best corrected visual acuity (log MAR) | right eyes | −0.09 ± 0.03 | −0.09 ± 0.03 | −0.09 ± 0.03 | 0.985 | |
| left eyes | −0.08 ± 0.03 | −0.08 ± 0.03 | −0.09 ± 0.03 | 0.718 | ||
| Axial length (mm) | right eyes | 24.49 ± 0.81 | 24.53 ± 0.67 | 24.45 ± 0.93 | 0.724 | |
| left eyes | 24.50 ± 0.83 | 24.54 ± 0.67 | 24.45 ± 0.97 | 0.658 | ||
| SER (D) | right eyes | −2.74 ± 0.86 | −2.66 ± 0.85 | −2.82 ± 0.87 | 0.328 | |
| left eyes | −2.78 ± 0.90 | −2.66 ± 0.87 | −2.90 ± 0.92 | 0.156 | ||
| Number of participants with glasses at the first visit | 59 (52.2%) | 28 (49.1%) | 31 (55.4%) | 0.574 | †† | |
| Environmental factors | ||||||
| Near-work time (min/day) | 193.45 ± 93.13 | 214.50 ± 104.11 | 172.02 ± 75.48 | 0.015 | † | |
| Sunlight exposure time (min/day) | 58.75 ± 52.18 | 54.52 ± 47.34 | 63.03 ± 56.80 | 0.388 | † | |
| Sleeping hours (hours/day) | 8.56 ± 0.67 | 8.57 ± 0.63 | 8.54 ± 0.72 | 0.841 | † | |
| Placebo | VL | Difference in Amount of Change from the Baseline | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| PPS n = 46 | PPS n = 45 | |||||||||
| LS Mean | 95% CI | LS Mean | 95% CI | Difference | 95% CI | p-Value | ||||
| Axial length | ||||||||||
| PPS | ||||||||||
| first visit (baseline) | 24.54 | 24.31 | 24.77 | 24.63 | 24.4 | 24.87 | ||||
| 24 months | 25.30 | 25.07 | 25.53 | 25.36 | 25.13 | 25.59 | ||||
| change from baseline | 0.76 | 0.71 | 0.81 | 0.73 | 0.68 | 0.78 | −0.03 | −0.10 | 0.04 | 0.381 |
| SER | ||||||||||
| PPS | ||||||||||
| first visit (baseline) | −2.73 | −2.97 | −2.49 | −2.96 | −3.2 | −2.71 | ||||
| 24 months | −4.26 | −4.56 | −3.96 | −4.38 | −4.68 | −4.08 | ||||
| change from baseline | −1.53 | −1.73 | −1.33 | −1.42 | −1.62 | −1.23 | 0.11 | −0.17 | 0.39 | 0.434 |
| Univariate Logistic Regression | |||||
|---|---|---|---|---|---|
| OR | 95% CI | p-Value | |||
| Age (y) | 0.28 | 0.16 | 0.51 | <0.0001 | |
| Female | 0.56 | 0.19 | 1.60 | 0.279 | |
| Change in BMI | 0.54 | 0.30 | 0.98 | 0.044 | |
| Continuous near-work time (min) | 1.00 | 0.99 | 1.02 | 0.643 | |
| Continuous near-work time (digital devices) (min) | 1.00 | 0.99 | 1.02 | 0.556 | |
| Already wearing glasses at first visit | 4.67 | 1.28 | 17.06 | 0.020 | |
| Near-work time (min) | 1.00 | 0.99 | 1.00 | 0.617 | |
| Near-work time (digital devices) (min) | 1.00 | 0.99 | 1.01 | 0.907 | |
| Near-work time (books) (min) | 0.99 | 0.97 | 1.00 | 0.171 | |
| Outdoor activity time (min) | 1.00 | 0.98 | 1.01 | 0.410 | |
| Birth weight (kg) | 1.00 | 1.00 | 1.00 | 0.403 | |
| Birth height (cm) | 1.05 | 0.84 | 1.32 | 0.648 | |
| Parental myopia | |||||
| Only father | 1.00 | ref | |||
| Only mother | 0.00 | 0.00 | 0.997 | ||
| Both parents | 0.17 | 0.05 | 0.55 | 0.003 | |
| Distance from the television (cm) | 0.87 | 0.48 | 1.57 | 0.652 | |
| Near-working distance (cm) | 1.00 | 0.93 | 1.09 | 0.930 | |
| Brightness of the bedroom while sleeping | |||||
| Bright | 0.00 | 0.00 | 0.999 | ||
| Dim | 0.73 | 0.25 | 2.15 | 0.570 | |
| Dark | 1.00 | ref | |||
| Bedtime (hr) | 0.38 | 0.15 | 0.96 | 0.041 | |
| Sleeping hours (hr) | 1.86 | 0.84 | 4.09 | 0.124 | |
| Extracurricular activities (outside) (min) | 0.60 | 0.13 | 2.75 | 0.507 | |
| Univariate Logistic Regression | |||||
|---|---|---|---|---|---|
| OR | 95% CI | p-Value | |||
| Age (y) | 0.47 | 0.31 | 0.72 | 0.0004 | |
| Female | 0.85 | 0.30 | 2.37 | 0.750 | |
| Change in BMI | 0.35 | 0.18 | 0.70 | 0.003 | |
| Continuous near-work time (min) | 1.00 | 0.99 | 1.02 | 0.718 | |
| Continuous near-work time (digital devices) (min) | 1.01 | 0.99 | 1.02 | 0.496 | |
| Already wearing glasses at first visit | 3.47 | 1.08 | 11.13 | 0.037 | |
| Near-work time (min) | 1.00 | 1.00 | 1.01 | 0.539 | |
| Near-work time (digital devices) (min) | 1.00 | 1.00 | 1.01 | 0.189 | |
| Near-work time (books) (min) | 0.99 | 0.97 | 1.00 | 0.145 | |
| Outdoor activity time (min) | 0.99 | 0.98 | 1.01 | 0.257 | |
| Birth weight (kg) | 1.00 | 1.00 | 1.00 | 0.783 | |
| Birth height (cm) | 1.07 | 0.85 | 1.33 | 0.573 | |
| Parental myopia | |||||
| Only father | 1.00 | ref | |||
| Only mother | 0.28 | 0.07 | 1.15 | 0.077 | |
| Both parents | 0.28 | 0.09 | 0.90 | 0.033 | |
| Distance from the television (cm) | 0.80 | 0.43 | 1.49 | 0.481 | |
| Near-working distance (cm) | 0.98 | 0.90 | 1.06 | 0.583 | |
| Brightness of the bedroom while sleeping | |||||
| Bright | 0.00 | 0.00 | 0.999 | ||
| Dim | 1.11 | 0.37 | 3.34 | 0.854 | |
| Dark | 1.00 | ref | |||
| Bedtime (hr) | 0.72 | 0.32 | 1.64 | 0.438 | |
| Sleeping hours (hr) | 1.13 | 0.53 | 2.41 | 0.761 | |
| Extracurricular activities (outside) (min) | 0.55 | 0.12 | 2.52 | 0.441 | |
| Placebo | VL | Difference in Amount of Change from the Baseline | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | LS Mean | 95% CI | n | LS Mean | 95% CI | Difference | 95% CI | p-Value | |||
| Axial length | |||||||||||
| Change after wearing the eyeglasses for 24 months | |||||||||||
| 11 | 0.96 | 0.86 | 1.06 | 11 | 0.75 | 0.65 | 0.86 | −0.21 | −0.35 | −0.06 | 0.006 |
| SER | |||||||||||
| Change after wearing the eyeglasses for 24 months | |||||||||||
| 11 | −1.84 | −2.06 | −1.63 | 11 | −1.54 | −1.76 | −1.32 | 0.30 | −0.01 | 0.61 | 0.055 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, K.; Torii, H.; Hara, Y.; Hara, M.; Yotsukura, E.; Hanyuda, A.; Negishi, K.; Kurihara, T.; Tsubota, K. Effect of Violet Light-Transmitting Eyeglasses on Axial Elongation in Myopic Children: A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 5462. https://doi.org/10.3390/jcm10225462
Mori K, Torii H, Hara Y, Hara M, Yotsukura E, Hanyuda A, Negishi K, Kurihara T, Tsubota K. Effect of Violet Light-Transmitting Eyeglasses on Axial Elongation in Myopic Children: A Randomized Controlled Trial. Journal of Clinical Medicine. 2021; 10(22):5462. https://doi.org/10.3390/jcm10225462
Chicago/Turabian StyleMori, Kiwako, Hidemasa Torii, Yutaka Hara, Michiko Hara, Erisa Yotsukura, Akiko Hanyuda, Kazuno Negishi, Toshihide Kurihara, and Kazuo Tsubota. 2021. "Effect of Violet Light-Transmitting Eyeglasses on Axial Elongation in Myopic Children: A Randomized Controlled Trial" Journal of Clinical Medicine 10, no. 22: 5462. https://doi.org/10.3390/jcm10225462