
Other (Non-CNS/Testicular) Extramedullary Localizations of Childhood Relapsed Acute Lymphoblastic Leukemia and Lymphoblastic Lymphoma—A Report from the ALL-REZ Study Group

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Definitions
2.3. Treatment
2.4. Statistical Methods
3. Results
3.1. Clinical Presentation of OEMR Differs Significantly from Non-OEMR Patients
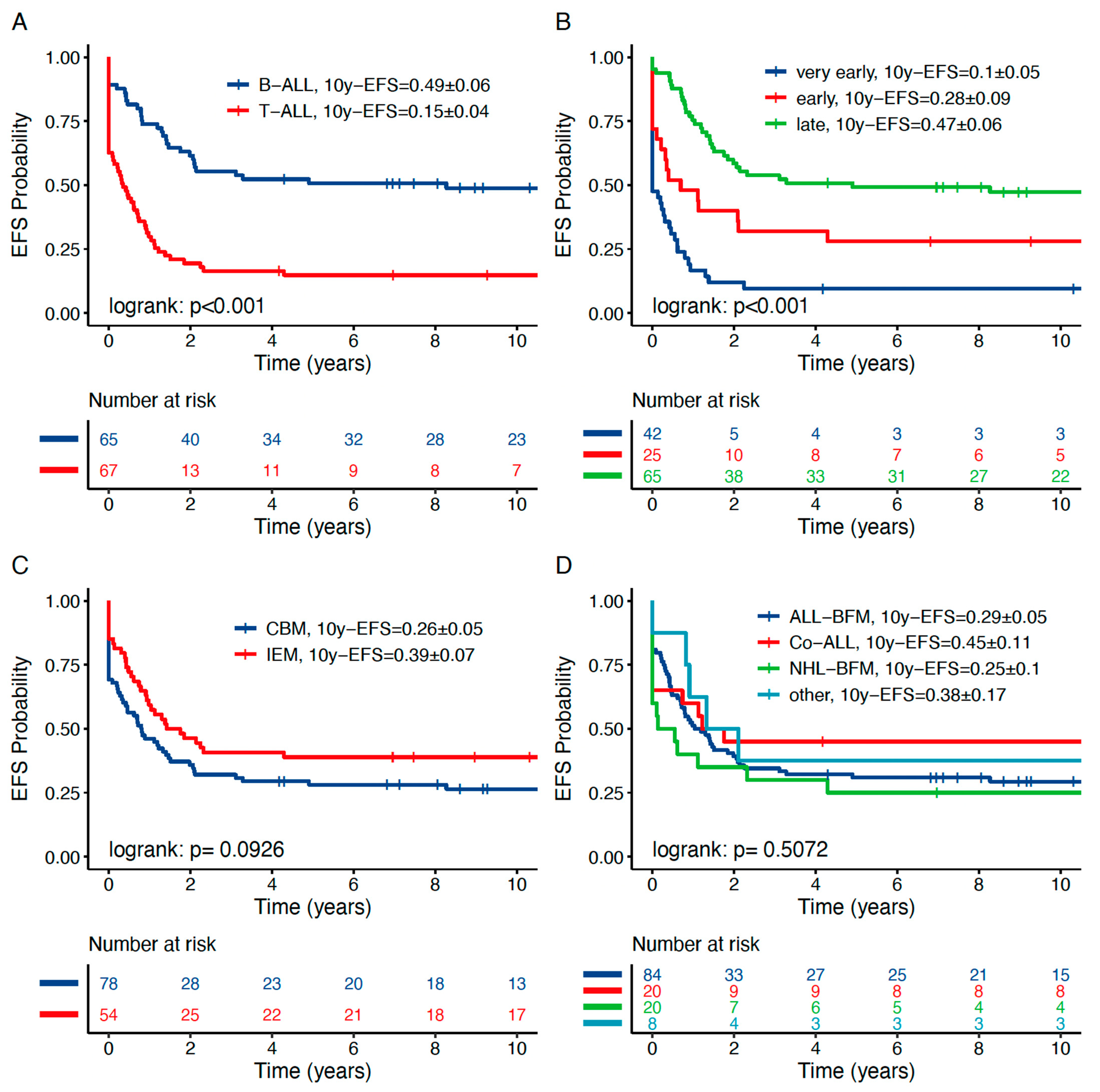
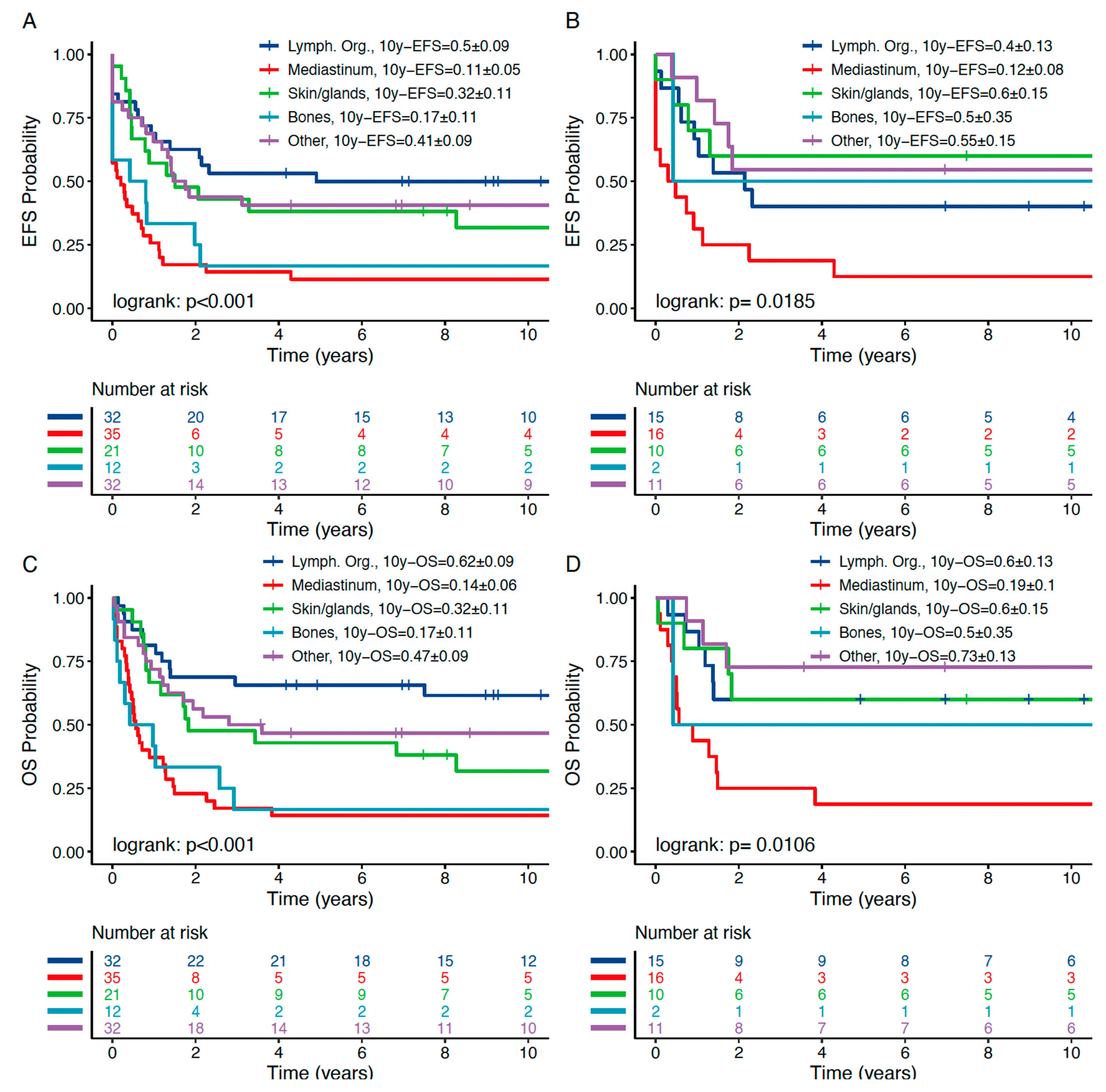
3.2. OEMR Subgroups Demonstrate Distinct Relapse Phenotypes
3.3. OEMR Shows a Distinct Event Pattern Compared to Non-OEMR
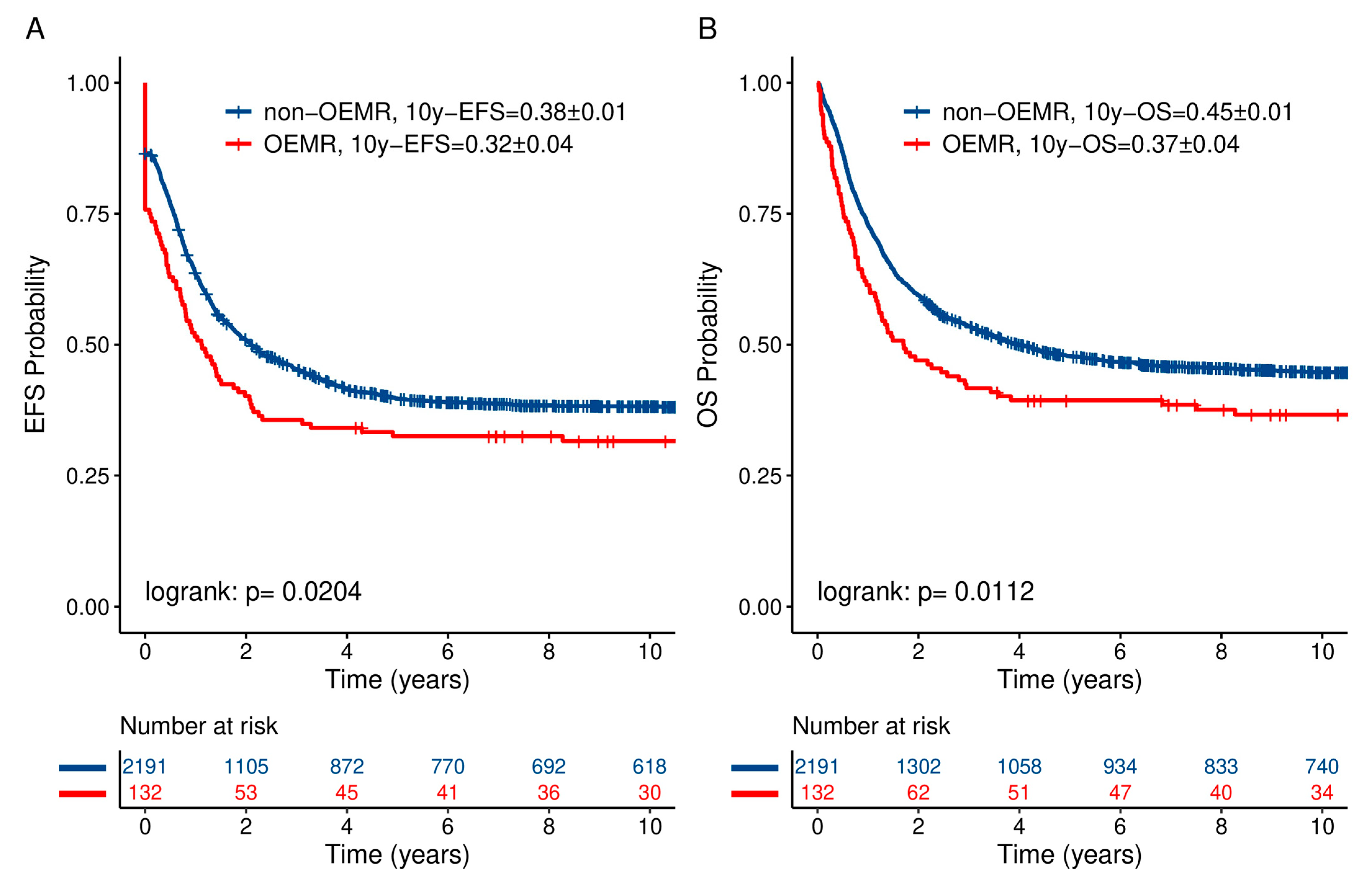
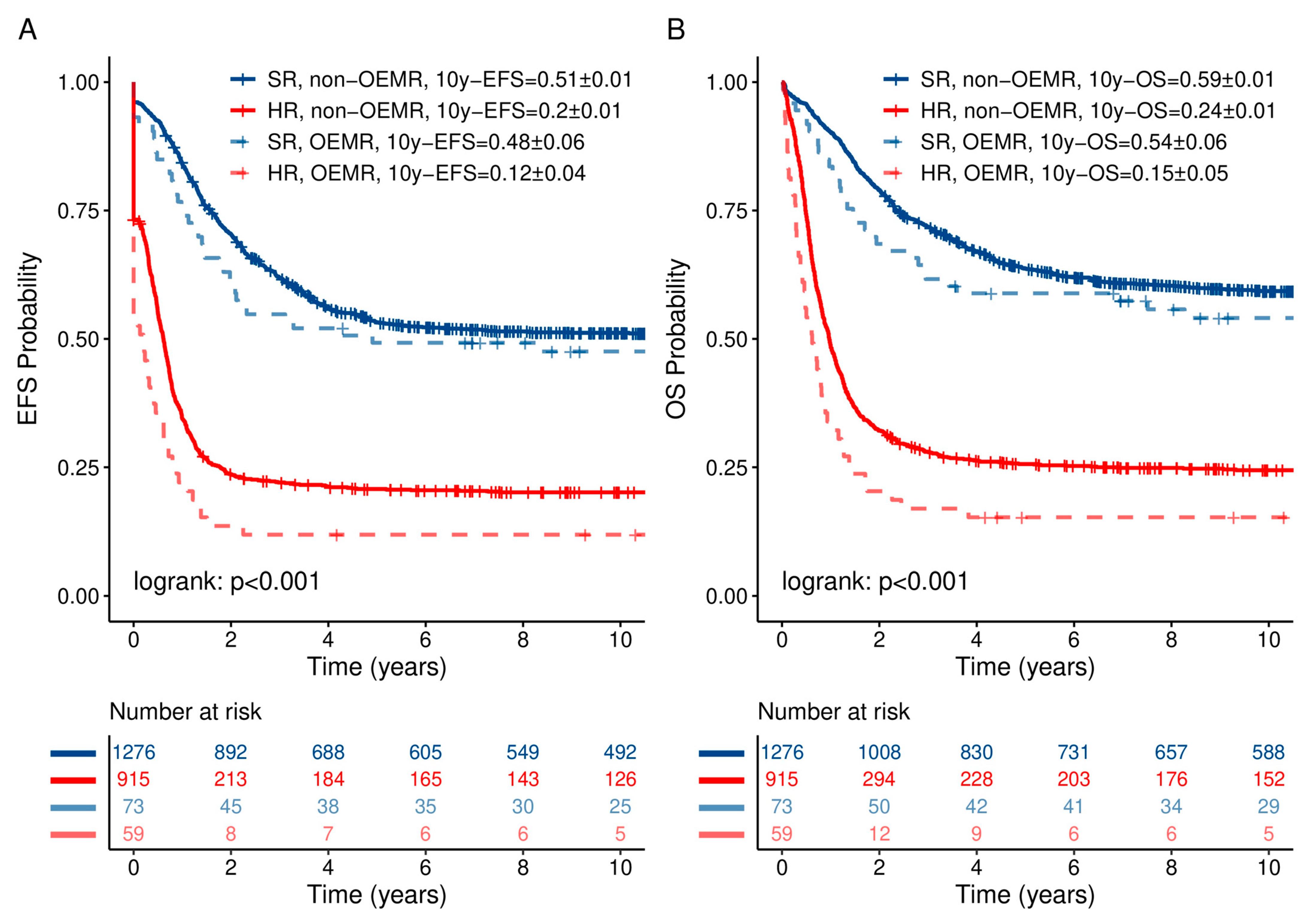
3.4. OEMR Confers an Independent Risk Factor for Decreased Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Gaudichon, J.; Jakobczyk, H.; Debaize, L.; Cousin, E.; Galibert, M.D.; Troadec, M.B.; Gandemer, V. Mechanisms of extramedullary relapse in acute lymphoblastic leukemia: Reconciling biological concepts and clinical issues. Blood Rev. 2019, 36, 40–56. [Google Scholar] [CrossRef] [PubMed]
- Pui, C.H. Central nervous system disease in acute lymphoblastic leukemia: Prophylaxis and treatment. Hematol. Am. Soc. Hematol. Educ. Program 2006, 2006, 142–146. [Google Scholar] [CrossRef] [Green Version]
- Wofford, M.M.; Smith, S.D.; Shuster, J.J.; Johnson, W.; Buchanan, G.R.; Wharam, M.D.; Ritchey, A.K.; Rosen, D.; Haggard, M.E.; Golembe, B.L.; et al. Treatment of occult or late overt testicular relapse in children with acute lymphoblastic leukemia: A Pediatric Oncology Group study. J. Clin. Oncol. 1992, 10, 624–630. [Google Scholar] [CrossRef] [Green Version]
- Murray, J.C.; Gmoser, D.J.; Barnes, D.A.; Oshman, D.; Hawkins, H.K.; Gresik, M.V.; Dreyer, Z.E. Isolated bone relapse during hematologic remission in childhood acute lymphoblastic leukemia: Report of a metatarsal relapse and review of the literature. Med. Pediatr. Oncol. 1994, 23, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Padmanjali, K.S.; Bakhshi, S.; Thavaraj, V.; Karak, A.K.; Arya, L.S. Bone relapse in acute lymphoblastic leukemia. Indian J. Pediatr. 2004, 71, 555–557. [Google Scholar] [CrossRef]
- Curto, M.L.; D’Angelo, P.; Jankovic, M.; Fugardi, M.G.; Ziino, O.; Casale, F. Isolated ocular relapse in childhood acute lymphoblastic leukemia during continuing complete remission. Haematologica 1996, 81, 47–50. [Google Scholar] [PubMed]
- Taylor, C.W.; Taylor, R.E.; Kinsey, S.E. Leukemic infiltration of the orbit: Report of three cases and literature review. Pediatr. Hematol. Oncol. 2005, 22, 415–422. [Google Scholar] [CrossRef]
- MacLean, H.; Clarke, M.P.; Strong, N.P.; Kernahan, J.; Ashraf, S. Primary ocular relapse in acute lymphoblastic leukemia. Eye 1996, 10 Pt 6, 719–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadel, J.; Meredith, T.; Anthony, C.; Sivasubramaniam, V.; Jabbour, A. Isolated myocardial relapse of Philadelphia-positive acute lymphoblastic leukaemia causing myocarditis: A case report. Eur. Heart J. Case Rep. 2018, 2, yty104. [Google Scholar] [CrossRef]
- Veys, D.; Norton, A.; Ainsworth, J.R.; Amrolia, P.; Lucchini, G. Isolated Intraocular Relapse of Pediatric B-cell Precursor Acute Lymphoblastic Leukaemia Following Chimeric Antigen Receptor T-lymphocyte Therapy. Cureus 2020, 12, e10937. [Google Scholar] [CrossRef]
- Dix, D.B.; Anderson, R.A.; McFadden, D.E.; Wadsworth, L.D. Pleural relapse during hematopoietic remission in childhood acute lymphoblastic leukemia. J. Pediatr. Hematol. Oncol. 1997, 19, 470–472. [Google Scholar] [CrossRef] [PubMed]
- Esmaeli, B.; Medeiros, L.J.; Myers, J.; Champlin, R.; Singh, S.; Ginsberg, L. Orbital mass secondary to precursor T-cell acute lymphoblastic leukemia: A rare presentation. Arch. Ophthalmol. 2001, 119, 443–446. [Google Scholar] [CrossRef] [Green Version]
- Hinkle, A.S.; Dinndorf, P.A.; Bulas, D.I.; Kapur, S. Relapse of acute lymphoblastic leukemia in the inferior rectus muscle of the eye. Cancer 1994, 73, 1757–1760. [Google Scholar] [CrossRef]
- Jankovic, M.; Conter, V.; Pretto, G.; Placa, F.; D’Incalci, M.; Masera, G. Isolated bilateral anterior chamber eye relapse in a child with acute lymphoblastic leukemia. Med. Pediatr. Oncol. 1995, 25, 109–112. [Google Scholar] [CrossRef]
- Kebaili, K.; Manel, A.M.; Chapelon, C.; Taylor, P.; Philippe, N.; Bertrand, Y. Renal enlargement as presentation of isolated renal relapse in childhood leukemia. J. Pediatr. Hematol. Oncol. 2000, 22, 454–456. [Google Scholar] [CrossRef] [PubMed]
- Ly-Sunnaram, B.; Henry, C.; Gandemer, V.; Mee, F.L.; Burtin, F.; Blayau, M.; Cayuela, J.M.; Oster, M.; Clech, P.; Rambeau, M.; et al. Late ovarian relapse of TEL/AML1 positive ALL confirming that TEL deletion is a secondary event in leukemogenesis. Leuk. Res. 2005, 29, 1089–1094. [Google Scholar] [CrossRef]
- Mateo, J.; Abarzuza, R.; Nunez, E.; Cristobal, J.A. Bilateral optic nerve infiltration in acute lymphoblastic leukemia in remission. Arch. Soc. Esp. Oftalmol. 2007, 82, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Millot, F.; Klossek, J.M.; Brizard, F.; Brizard, A.; Vandermarq, P.; Babin, P.; Guilhot, F. Recurrence of childhood acute lymphoblastic leukemia presenting as a tumor of the middle ear: A case report. J. Pediatr. Hematol. Oncol. 1997, 19, 351–353. [Google Scholar] [CrossRef]
- Qamruddin, K.; Hassan, S.; Khurshid, M. Case of pelvic relapse in a child suffering from acute lymphoblastic leukemia. J. Pak. Med. Assoc. 1995, 45, 193–194. [Google Scholar]
- Rush, M.; Toth, B.B.; Pinkel, D. Clinically isolated mandibular relapse in childhood acute leukemia. Cancer 1990, 66, 369–372. [Google Scholar] [CrossRef]
- Todo, K.; Morimoto, A.; Osone, S.; Nukina, S.; Ohtsuka, T.; Ishida, H.; Yoshihara, T.; Todo, S. Isolated relapse of acute lymphoblastic leukemia in the breast of a young female. Pediatr. Hematol. Oncol. 2008, 25, 607–613. [Google Scholar] [CrossRef]
- Tsuruchi, N.; Okamura, J. Childhood acute lymphoblastic leukemia relapse in the uterine cervix. J. Pediatr. Hematol. Oncol. 1996, 18, 311–313. [Google Scholar] [CrossRef] [PubMed]
- Uderzo, C.; Santamaria, M.; Locasciulli, A.; Merati, I.; Di Lelio, A.; Conter, V.; Masera, G. Abdominal mass as manifestation of isolated extramedullary relapse in a child with acute lymphoblastic leukemia (ALL). Haematologica 1987, 72, 545–547. [Google Scholar]
- Gunes, G.; Goker, H.; Demiroglu, H.; Malkan, U.Y.; Buyukasik, Y. Extramedullary relapses of acute leukemias after allogeneic hematopoietic stem cell transplantation: Clinical features, cumulative incidence, and risk factors. Bone Marrow Transplant. 2019, 54, 595–600. [Google Scholar] [CrossRef]
- Bunin, N.J.; Pui, C.H.; Hustu, H.O.; Rivera, G.K. Unusual extramedullary relapses in children with acute lymphoblastic leukemia. J. Pediatr. 1986, 109, 665–668. [Google Scholar] [CrossRef]
- Kim, J.Y.; Im, S.A.; Lee, J.H.; Lee, J.W.; Chung, N.G.; Cho, B. Extramedullary Relapse of Acute Myeloid and Lymphoid Leukemia in Children: A Retrospective Analysis. Iran. J. Pediatr. 2016, 26, e1711. [Google Scholar] [CrossRef] [PubMed]
- Bene, M.C.; Castoldi, G.; Knapp, W.; Ludwig, W.D.; Matutes, E.; Orfao, A.; van’t Veer, M.B. Proposals for the immunological classification of acute leukemias. European Group for the Immunological Characterization of Leukemias (EGIL). Leukemia 1995, 9, 1783–1786. [Google Scholar] [PubMed]
- Seeger, K.; Adams, H.P.; Buchwald, D.; Beyermann, B.; Kremens, B.; Niemeyer, C.; Ritter, J.; Schwabe, D.; Harms, D.; Schrappe, M.; et al. TEL-AML1 fusion transcript in relapsed childhood acute lymphoblastic leukemia. The Berlin-Frankfurt-Munster Study Group. Blood 1998, 91, 1716–1722. [Google Scholar] [CrossRef] [Green Version]
- Einsiedel, H.G.; von Stackelberg, A.; Hartmann, R.; Fengler, R.; Schrappe, M.; Janka-Schaub, G.; Mann, G.; Hahlen, K.; Gobel, U.; Klingebiel, T.; et al. Long-term outcome in children with relapsed ALL by risk-stratified salvage therapy: Results of trial acute lymphoblastic leukemia-relapse study of the Berlin-Frankfurt-Munster Group 87. J. Clin. Oncol. 2005, 23, 7942–7950. [Google Scholar] [CrossRef]
- von Stackelberg, A.; Hartmann, R.; Buhrer, C.; Fengler, R.; Janka-Schaub, G.; Reiter, A.; Mann, G.; Schmiegelow, K.; Ratei, R.; Klingebiel, T.; et al. High-dose compared with intermediate-dose methotrexate in children with a first relapse of acute lymphoblastic leukemia. Blood 2008, 111, 2573–2580. [Google Scholar] [CrossRef] [Green Version]
- Eckert, C.; von Stackelberg, A.; Seeger, K.; Groeneveld, T.W.; Peters, C.; Klingebiel, T.; Borkhardt, A.; Schrappe, M.; Escherich, G.; Henze, G. Minimal residual disease after induction is the strongest predictor of prognosis in intermediate risk relapsed acute lymphoblastic leukaemia—Long-Term results of trial ALL-REZ BFM P95/96. Eur. J. Cancer 2013, 49, 1346–1355. [Google Scholar] [CrossRef]
- Eckert, C.; Henze, G.; Seeger, K.; Hagedorn, N.; Mann, G.; Panzer-Grumayer, R.; Peters, C.; Klingebiel, T.; Borkhardt, A.; Schrappe, M.; et al. Use of allogeneic hematopoietic stem-cell transplantation based on minimal residual disease response improves outcomes for children with relapsed acute lymphoblastic leukemia in the intermediate-risk group. J. Clin. Oncol. 2013, 31, 2736–2742. [Google Scholar] [CrossRef]
- Meyr, F.; Escherich, G.; Mann, G.; Klingebiel, T.; Kulozik, A.; Rossig, C.; Schrappe, M.; Henze, G.; von Stackelberg, A.; Hitzler, J. Outcomes of treatment for relapsed acute lymphoblastic leukaemia in children with Down syndrome. Br. J. Haematol. 2013, 162, 98–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, C.; Schrappe, M.; von Stackelberg, A.; Schrauder, A.; Bader, P.; Ebell, W.; Lang, P.; Sykora, K.W.; Schrum, J.; Kremens, B.; et al. Stem-cell transplantation in children with acute lymphoblastic leukemia: A prospective international multicenter trial comparing sibling donors with matched unrelated donors-The ALL-SCT-BFM-2003 trial. J. Clin. Oncol. 2015, 33, 1265–1274. [Google Scholar] [CrossRef]
- van der Wijk, A.E.; Canning, P.; van Heijningen, R.P.; Vogels, I.M.C.; van Noorden, C.J.F.; Klaassen, I.; Schlingemann, R.O. Glucocorticoids exert differential effects on the endothelium in an in vitro model of the blood-retinal barrier. Acta Ophthalmol. 2019, 97, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Gaynon, P.S.; Qu, R.P.; Chappell, R.J.; Willoughby, M.L.; Tubergen, D.G.; Steinherz, P.G.; Trigg, M.E. Survival after relapse in childhood acute lymphoblastic leukemia: Impact of site and time to first relapse--the Children’s Cancer Group Experience. Cancer 1998, 82, 1387–1395. [Google Scholar] [CrossRef]
- Tallen, G.; Ratei, R.; Mann, G.; Kaspers, G.; Niggli, F.; Karachunsky, A.; Ebell, W.; Escherich, G.; Schrappe, M.; Klingebiel, T.; et al. Long-term outcome in children with relapsed acute lymphoblastic leukemia after time-point and site-of-relapse stratification and intensified short-course multidrug chemotherapy: Results of trial ALL-REZ BFM 90. J. Clin. Oncol. 2010, 28, 2339–2347. [Google Scholar] [CrossRef]
- Ninane, J.; Taylor, D.; Day, S. The eye as a sanctuary in acute lymphoblastic leukaemia. Lancet 1980, 1, 452–453. [Google Scholar] [CrossRef]
- Burkhardt, B.; Reiter, A.; Landmann, E.; Lang, P.; Lassay, L.; Dickerhoff, R.; Lakomek, M.; Henze, G.; von Stackelberg, A. Poor outcome for children and adolescents with progressive disease or relapse of lymphoblastic lymphoma: A report from the berlin-frankfurt-muenster group. J. Clin. Oncol. 2009, 27, 3363–3369. [Google Scholar] [CrossRef]
- Burkhardt, B.; Taj, M.; Garnier, N.; Minard-Colin, V.; Hazar, V.; Mellgren, K.; Osumi, T.; Fedorova, A.; Myakova, N.; Verdu-Amoros, J.; et al. Treatment and Outcome Analysis of 639 Relapsed Non-Hodgkin Lymphomas in Children and Adolescents and Resulting Treatment Recommendations. Cancers 2021, 13, 2075. [Google Scholar] [CrossRef]
- Khanam, T.; Sandmann, S.; Seggewiss, J.; Ruether, C.; Zimmermann, M.; Norvil, A.B.; Bartenhagen, C.; Randau, G.; Mueller, S.; Herbrueggen, H.; et al. Integrative genomic analysis of pediatric T-cell lymphoblastic lymphoma reveals candidates of clinical significance. Blood 2021, 137, 2347–2359. [Google Scholar] [CrossRef]
- Burkhardt, B.; Hermiston, M.L. Lymphoblastic lymphoma in children and adolescents: Review of current challenges and future opportunities. Br. J. Haematol. 2019, 185, 1158–1170. [Google Scholar] [CrossRef]
- Cortelazzo, S.; Intermesoli, T.; Oldani, E.; Ciceri, F.; Rossi, G.; Pogliani, E.M.; Mattei, D.; Romani, C.; Cortelezzi, A.; Borlenghi, E.; et al. Results of a lymphoblastic leukemia-like chemotherapy program with risk-adapted mediastinal irradiation and stem cell transplantation for adult patients with lymphoblastic lymphoma. Ann. Hematol. 2012, 91, 73–82. [Google Scholar] [CrossRef] [Green Version]
- Dabaja, B.S.; Ha, C.S.; Thomas, D.A.; Wilder, R.B.; Gopal, R.; Cortes, J.; Bueso-Ramos, C.; Hess, M.A.; Cox, J.D.; Kantarjian, H.M. The role of local radiation therapy for mediastinal disease in adults with T-cell lymphoblastic lymphoma. Cancer 2002, 94, 2738–2744. [Google Scholar] [CrossRef] [Green Version]
- Karrman, K.; Johansson, B. Pediatric T-cell acute lymphoblastic leukemia. Genes Chromosomes Cancer 2017, 56, 89–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bader, P.; Kreyenberg, H.; Henze, G.H.; Eckert, C.; Reising, M.; Willasch, A.; Barth, A.; Borkhardt, A.; Peters, C.; Handgretinger, R.; et al. Prognostic value of minimal residual disease quantification before allogeneic stem-cell transplantation in relapsed childhood acute lymphoblastic leukemia: The ALL-REZ BFM Study Group. J. Clin. Oncol. 2009, 27, 377–384. [Google Scholar] [CrossRef]
- Zhao, J.; Qiao, W.; Wang, C.; Wang, T.; Xing, Y. Therapeutic evaluation and prognostic value of interim hybrid PET/CT with (18)F-FDG after three to four cycles of chemotherapy in non-Hodgkin’s lymphoma. Hematology 2007, 12, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Eckert, P.; Johs, A.; Semrau, J.D.; DiSpirito, A.A.; Richardson, J.; Sarangi, R.; Herndon, E.; Gu, B.; Pierce, E.M. Spectroscopic and computational investigations of organometallic complexation of group 12 transition metals by methanobactins from Methylocystis sp. SB2. J. Inorg. Biochem. 2021, 223, 111496. [Google Scholar] [CrossRef]
- Bride, K.L.; Vincent, T.L.; Im, S.Y.; Aplenc, R.; Barrett, D.M.; Carroll, W.L.; Carson, R.; Dai, Y.; Devidas, M.; Dunsmore, K.P.; et al. Preclinical efficacy of daratumumab in T-cell acute lymphoblastic leukemia. Blood 2018, 131, 995–999. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, F.; Zugmaier, G.; Rizzari, C.; Morris, J.D.; Gruhn, B.; Klingebiel, T.; Parasole, R.; Linderkamp, C.; Flotho, C.; Petit, A.; et al. Effect of Blinatumomab vs Chemotherapy on Event-Free Survival Among Children With High-risk First-Relapse B-Cell Acute Lymphoblastic Leukemia: A Randomized Clinical Trial. JAMA 2021, 325, 843–854. [Google Scholar] [CrossRef] [PubMed]
- Bhojwani, D.; Sposto, R.; Shah, N.N.; Rodriguez, V.; Yuan, C.; Stetler-Stevenson, M.; O’Brien, M.M.; McNeer, J.L.; Quereshi, A.; Cabannes, A.; et al. Inotuzumab ozogamicin in pediatric patients with relapsed/refractory acute lymphoblastic leukemia. Leukemia 2019, 33, 884–892. [Google Scholar] [CrossRef] [PubMed]
- Maude, S.L.; Laetsch, T.W.; Buechner, J.; Rives, S.; Boyer, M.; Bittencourt, H.; Bader, P.; Verneris, M.R.; Stefanski, H.E.; Myers, G.D.; et al. Tisagenlecleucel in Children and Young Adults with B-Cell Lymphoblastic Leukemia. N. Engl. J. Med. 2018, 378, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Pui, C.H.; Tang, J.Y.; Yang, J.J.; Chen, S.J.; Chen, Z. International Collaboration to Save Children With Acute Lymphoblastic Leukemia. J. Glob. Oncol. 2019, 5, 1–2. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Group | n | % |
|---|---|---|---|
| LN | Lymphat. organs | 32 | 24.2 |
| Skin | Skin/glands | 14 | 10.6 |
| Mediastinum/thymus | Mediastinum | 35 | 26.5 |
| Tonsils | Skin/glands | 2 | 1.5 |
| Female genital organs | Other | 6 | 4.5 |
| Eye/nervus opticus | Other | 4 | 3.0 |
| Bones | Bone | 12 | 9.1 |
| Paranasal sinuses/ENT | Other | 2 | 1.5 |
| Kidney | Other | 9 | 6.8 |
| Liver | Other | 3 | 2.3 |
| Pancreas | Other | 1 | 0.8 |
| Serosae (pleural/cardial/joints) | Skin/glands | 1 | 0.8 |
| Glands (mammae/g. parotis/g. lacrimae) | Skin/glands | 4 | 3.0 |
| Spleen | Other | 1 | 0.8 |
| Colon/intestine | Other | 1 | 0.8 |
| Epidural | Other | 1 | 0.8 |
| Abdomen | Other | 2 | 1.5 |
| Other | Other | 2 | 1.5 |
| Total | 132 | 100.0 | |
| ALL Relapse Trial Patients | Other Extramedullary Relapse Patients | Other Extramedullary Relapse Subgroups | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | Lymph. Organs | Mediast. Organs | Other Compartment | Skin/Glands | Bone | ||||||||||||
| n | % | n | % | n | % | p ** | n | % | n | % | n | % | n | % | n | % | p ** | |
| Total group | 2323 | 100 | 2191 | 100 | 132 | 100 | 32 | 24.2 | 35 | 26.6 | 32 | 24.2 | 21 | 15.9 | 12 | 9.1 | ||
| Patient characteristics | ||||||||||||||||||
| Sex | 0.37 | 0.71 | ||||||||||||||||
| Male | 1474 | 63 | 1395 | 63.7 | 79 | 59.8 | 19 | 59.4 | 24 | 68.6 | 19 | 59.4 | 11 | 52.4 | 6 | 50 | ||
| Female | 849 | 37 | 796 | 36.3 | 53 | 40.2 | 13 | 40.6 | 11 | 31.4 | 13 | 40.6 | 10 | 47.6 | 6 | 50 | ||
| Time point of relapse | 0.01 | 0.04 | ||||||||||||||||
| Very early | 565 | 24.3 | 523 | 23.9 | 42 | 31.9 | 11 | 34.4 | 15 | 42.9 | 5 | 15.6 | 6 | 28.6 | 5 | 41.7 | ||
| Early | 691 | 29.8 | 666 | 30.4 | 25 | 18.9 | 5 | 15.6 | 11 | 31.4 | 5 | 15.6 | 2 | 7.1 | 2 | 16.6 | ||
| Late | 1067 | 45.9 | 1002 | 45.7 | 65 | 49.2 | 16 | 50 | 9 | 25.7 | 22 | 68.8 | 13 | 46.4 | 5 | 41.7 | ||
| Age at relapse | 0.38 | 0.25 | ||||||||||||||||
| ≤5 years | 386 | 16.6 | 369 | 16.8 | 17 | 12.9 | 4 | 12.5 | 5 | 14.3 | 2 | 6.3 | 2 | 9.5 | 4 | 33.3 | ||
| ≥5 years and ≤10 years | 1011 | 43.5 | 955 | 43.7 | 56 | 42.4 | 14 | 43.8 | 17 | 48.5 | 17 | 53.1 | 6 | 28.6 | 2 | 16.7 | ||
| >10 years and ≤15 years | 648 | 27.9 | 610 | 27.8 | 38 | 28.8 | 9 | 28.1 | 10 | 28.6 | 9 | 28.1 | 6 | 28.6 | 4 | 33.3 | ||
| >15 years and <20 years | 278 | 12.0 | 257 | 11.7 | 21 | 15.9 | 5 | 15.6 | 3 | 8.6 | 4 | 12.5 | 7 | 33.3 | 2 | 16.7 | ||
| Site of relapse | <0.001 | 0.32 | ||||||||||||||||
| Isolated BM | 1439 | 62.0 | 1439 | 65.7 | 0 | 0 | ||||||||||||
| Combined BM and EM | 505 | 21.7 | 427 | 19.5 | 78 | 59.1 | 17 | 53.1 | 19 | 54.3 | 21 | 65.6 | 11 | 52.4 | 10 | 83.3 | ||
| Isolated extramedullary | 379 | 16.3 | 325 | 14.8 | 54 | 40.9 | 15 | 46.9 | 16 | 45.7 | 11 | 34.4 | 10 | 47.6 | 2 | 16.7 | ||
| Immunophenotype | <0.001 | <0.001 | ||||||||||||||||
| Precursor B cell | 2014 | 86.7 | 1949 | 89 | 65 | 49.2 | 14 | 43.8 | 2 | 5.7 | 23 | 71.9 | 15 | 71.4 | 11 | 91.7 | ||
| T cell | 309 | 13.3 | 242 | 11 | 67 | 50.8 | 18 | 56.2 | 33 | 94.3 | 9 | 28.1 | 6 | 28.6 | 1 | 8.3 | ||
| Therapy | 0.29 | 0.23 | ||||||||||||||||
| Chemotherapy/radiotherapy exclusively | 1550 | 66.7 | 1459 | 66.7 | 91 | 68.9 | 18 | 56.2 | 26 | 74.3 | 23 | 71.9 | 14 | 66.7 | 10 | 83.4 | ||
| Allogeneic SCT | 664 | 28.6 | 632 | 28.8 | 32 | 24.2 | 12 | 37.5 | 7 | 20 | 5 | 15.6 | 7 | 33.3 | 1 | 8.3 | ||
| Autologous SCT | 57 | 2.5 | 51 | 2.3 | 6 | 4.6 | 0 | 0 | 2 | 5.7 | 3 | 9.4 | 0 | 0 | 1 | 8.3 | ||
| No data | 52 | 2.2 | 49 | 2.2 | 3 | 2.3 | 2 | 6.3 | 0 | 0 | 1 | 3.1 | 0 | 0 | 0 | 0 | ||
| NHL Therapy | <0.001 | 0.08 | ||||||||||||||||
| Other | 2247 | 96.7 | 2135 | 97.4 | 112 | 84.8 | 25 | 78.1 | 26 | 74.3 | 30 | 93.8 | 20 | 95.2 | 11 | 91.7 | ||
| NHL-BFM | 62 | 2.7 | 42 | 1.9 | 20 | 15.2 | 7 | 21.9 | 9 | 25.7 | 2 | 6.2 | 1 | 4.8 | 1 | 8.3 | ||
| No data | 14 | 0.06 | 14 | 0.7 | 0 | 0 | ||||||||||||
| (a) All Events | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OEM | OEM Group | |||||||||||||||||||||||||||
| No | Yes | Lymphat. Organs | Skin/Glands | Mediastinum | Bone | Other | ||||||||||||||||||||||
| n | % | n | % | p * | n | % | n | % | n | % | n | % | n | % | p * | |||||||||||||
| Total | 2191 | 100.0 | 132 | 100.0 | 0.036 | 32 | 100.0 | 21 | 100.0 | 35 | 100.0 | 12 | 100.0 | 32 | 100.0 | 0.025 | ||||||||||||
| Event | 821 | 37.5 | 42 | 31.8 | 0.23 | 16 | 50.0 | 7 | 33.3 | 4 | 11.4 | 2 | 16.7 | 13 | 40.6 | |||||||||||||
| in CCR | ||||||||||||||||||||||||||||
| Died in CR | 138 | 6.3 | 7 | 5.3 | 0.78 | 1 | 3.1 | 2 | 9.5 | 3 | 8.6 | 1 | 8.3 | . | . | |||||||||||||
| 2nd malignoma | 29 | 1.3 | 3 | 2.3 | 0.60 | 1 | 3.1 | . | . | 1 | 2.9 | 1 | 8.3 | . | . | |||||||||||||
| Another relapse | 889 | 40.6 | 48 | 36.4 | 0.39 | 9 | 28.1 | 11 | 52.4 | 12 | 34.3 | 3 | 25.0 | 13 | 40.6 | |||||||||||||
| Nonresponder/progr. disease | 215 | 9.8 | 21 | 15.9 | 0.03 | 4 | 12.5 | . | . | 11 | 31.4 | 2 | 16.7 | 4 | 12.5 | |||||||||||||
| Death in induction | 81 | 3.7 | 11 | 8.3 | 0.02 | 1 | 3.1 | 1 | 4.8 | 4 | 11.4 | 3 | 25.0 | 2 | 6.3 | |||||||||||||
| Death of unknown origin | 4 | 0.2 | 0 | 0 | 1 | . | . | . | . | . | . | . | . | . | . | |||||||||||||
| (b) OEM Subsequent Relapse Sites | ||||||||||||||||||||||||||||
| OEM | OEM Group | |||||||||||||||||||||||||||
| No | Yes | Lymphat. Organs | Skin/Glands | Mediastinum | Bone | Other | ||||||||||||||||||||||
| n | % | n | % | p * | n | % | n | % | n | % | n | % | n | % | ||||||||||||||
| Subs. relapse | 889 | 100.0 | 48 | 100.0 | 9 | 100.0 | 11 | 100.0 | 12 | 100.0 | 3 | 100.0 | 13 | 100.0 | ||||||||||||||
| Subseq_site | <0.001 | |||||||||||||||||||||||||||
| IBM | 680 | 76.5 | 20 | 41.7 | 4 | 44.4 | 5 | 45.5 | 6 | 50.0 | 1 | 33.3 | 4 | 30.8 | ||||||||||||||
| CBM | 94 | 10.6 | 8 | 16.7 | 1 | 11.1 | 2 | 18.2 | 2 | 16.7 | 2 | 66.7 | 1 | 7.7 | ||||||||||||||
| IEM | 115 | 12.9 | 20 | 41.7 | 4 | 44.4 | 4 | 36.4 | 4 | 33.3 | . | . | 8 | 61.5 | ||||||||||||||
| (c) Subsequent Relapse Sites Compared to OEMR First Relapse Sites | ||||||||||||||||||||||||||||
| Total | Subsequent OEMR | Subsequent Relapse CNS/Testis Only | Subsequent Relapse Site | n | ||||||||||||||||||||||||
| OEM | OEM group | 32 | ||||||||||||||||||||||||||
| LN | Lymphat. organs | 5 | 0 | LN | 4 | |||||||||||||||||||||||
| Mediastinum | 1 | |||||||||||||||||||||||||||
| Skin | Skin/glands | 14 | 3 | 3 | LN | 1 | ||||||||||||||||||||||
| glands | 1 | |||||||||||||||||||||||||||
| skin | 1 | |||||||||||||||||||||||||||
| CNS/testis | 3 | |||||||||||||||||||||||||||
| Mediastinum/thymus | Mediastinum | 35 | 3 | 3 | LN | 3 | ||||||||||||||||||||||
| CNS/testis | 3 | |||||||||||||||||||||||||||
| Tonsils | Skin/glands | 2 | 0 | 0 | 0 | |||||||||||||||||||||||
| Female genital organs | Other | 6 | 0 | 1 | CNS/testis | 1 | ||||||||||||||||||||||
| Eye/nervus opticus | Other | 4 | 0 | 0 | 0 | |||||||||||||||||||||||
| Bones | Bone | 12 | 1 | 1 | Bones | 1 | ||||||||||||||||||||||
| CNS/testis | 1 | |||||||||||||||||||||||||||
| Paranasal sinuses/ENT | Other | 2 | 0 | 1 | CNS/testis | 1 | ||||||||||||||||||||||
| Kidney | Other | 9 | 1 | 1 | Paranasal sinus | 1 | ||||||||||||||||||||||
| CNS/testis | 1 | |||||||||||||||||||||||||||
| Liver | Other | 3 | 1 | 0 | Liver | 1 | ||||||||||||||||||||||
| Pancreas | Other | 1 | 1 | 0 | Pancreas | 1 | ||||||||||||||||||||||
| Serosae (pleural/cardial/joints) | Skin/glands | 1 | 0 | 0 | 0 | |||||||||||||||||||||||
| Glands (mammae/g. parotis/g. lacrimae) | Skin/glands | 4 | 0 | 0 | 0 | |||||||||||||||||||||||
| Spleen | Other | 1 | 0 | 0 | 0 | |||||||||||||||||||||||
| Colon/intestine | Other | 1 | 1 | 0 | Skin | 1 | ||||||||||||||||||||||
| Epidural | Other | 1 | 1 | 0 | Kidney | 1 | ||||||||||||||||||||||
| Abdomen | Other | 2 | 0 | 0 | 0 | |||||||||||||||||||||||
| Other | Other | 2 | 1 | 0 | Other | 1 | ||||||||||||||||||||||
| Total | 132 | 18 | 10 | 28 | ||||||||||||||||||||||||
| (a) HSCT Performed Per Risk Group in OEMR and Non-OEMR Patients | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HSCT—OEMR | ||||||||||||||||||||||||||||||
| Total | S1 | S2 | S4 | |||||||||||||||||||||||||||
| n | % | n | % | n | % | n | % | |||||||||||||||||||||||
| Total * | 132 | 100 | 30 | 100 | 59 | 100 | 43 | 100 | ||||||||||||||||||||||
| No HSCT | 91 | 68.9 | 20 | 66.6 | 39 | 66.1 | 32 | 74.5 | ||||||||||||||||||||||
| Allogeneic HSCT | 32 | 24.2 | 5 | 16.7 | 18 | 30.5 | 9 | 20.9 | ||||||||||||||||||||||
| Autologous HSCT | 6 | 4.5 | 3 | 10 | 2 | 3.4 | 1 | 2.3 | ||||||||||||||||||||||
| Unknown | 3 | 2.4 | 2 | 6.7 | 1 | 2.3 | ||||||||||||||||||||||||
| HSCT—Non-OEMR | ||||||||||||||||||||||||||||||
| Total | S1 | S2 | S3 | S4 | ||||||||||||||||||||||||||
| n | % | n | % | n | % | n | % | n | % | |||||||||||||||||||||
| Total * | 2190 | 100 | 71 | 100 | 1299 | 100 | 320 | 100 | 500 | 100 | ||||||||||||||||||||
| No HSCT | 1459 | 66.7 | 67 | 94.3 | 915 | 70.4 | 162 | 50.6 | 315 | 63.0 | ||||||||||||||||||||
| Allogeneic HSCT | 631 | 28.8 | 0 | 0 | 326 | 25.1 | 145 | 45.3 | 160 | 32.0 | ||||||||||||||||||||
| Autologous HSCT | 51 | 2.3 | 1 | 1.4 | 26 | 2 | 9 | 2.8 | 15 | 3.0 | ||||||||||||||||||||
| Unknown | 49 | 2.2 | 3 | 4.2 | 32 | 2.5 | 4 | 1.3 | 10 | 2.0 | ||||||||||||||||||||
| (b) HSCT, All Events in Non-OEMR and OEMR Groups | ||||||||||||||||||||||||||||||
| HSCT—Events | ||||||||||||||||||||||||||||||
| Total Non-OEMR | Total OEMR | No HSCT Non-OEMR | No HSCT OEMR | Allogeneic HSCT Non-OEMR | Allogeneic HSCT OEMR | Autologous Non-OEMR | Autologous OEMR | Unknown Non-OEMR | Unknown OEMR | |||||||||||||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | |||||||||||||||||
| Total ** | 1877 | 100 | 100 | 100 | 1150 | 100 | 60 | 100 | 628 | 100 | 32 | 100 | 51 | 100 | 6 | 100 | 48 | 100 | 2 | 100.0 | ||||||||||
| Event | 821 | 43.7 | 42 | 42.0 | 426 | 37 | 23 | 38.3 | 337 | 53.6 | 14 | 43.8 | 13 | 25.5 | 3 | 50 | 45 | 93.8 | 2 | 100.0 | ||||||||||
| in CCR | ||||||||||||||||||||||||||||||
| Died in CR | 138 | 7.3 | 7 | 7.0 | 41 | 3.6 | 3 | 5.0 | 96 | 15.3 | 4 | 12.5 | 1 | 2 | ||||||||||||||||
| 2nd malignoma | 29 | 1.5 | 3 | 3.0 | 13 | 1.1 | 1 | 1,7 | 15 | 2.4 | 2 | 6.3 | 1 | 2 | ||||||||||||||||
| Subsequent relapse | 889 | 47.3 | 48 | 48.0 | 670 | 58.3 | 33 | 55.0 | 180 | 28.7 | 12 | 37.5 | 36 | 70.5 | 3 | 50 | 3 | 6.2 | ||||||||||||
| (a) pEFS | |||||
|---|---|---|---|---|---|
| OEMR | |||||
| No—2191 | Yes—132 | ||||
| pEFS ± SE (10 Years) | p * | pEFS ± SE (10 Years) | p * | ||
| Total group | 0.38 ± 0.01 | 0.32 ± 0.04 | 0.0204 | ||
| Patient characteristics | |||||
| Sex | 0.49 | 0.18 | |||
| Male | 0.38 ± 0.01 | 0.28 ± 0.05 | |||
| Female | 0.39 ± 0.02 | 0.38 ± 0.07 | |||
| Time point of relapse | <0.001 | <0.001 | |||
| Very early | 0.20 ± 0.02 | 0.10 ± 0.05 | |||
| Early | 0.29 ± 0.02 | 0.28 ± 0.09 | |||
| Late | 0.54 ± 0.02 | 0.47 ± 0.06 | |||
| Age at relapse | <0.001 | 0.60 | |||
| ≤5 years | 0.31 ± 0.02 | 0.29 ± 0.11 | |||
| ≥5 years and ≤10 years | 0.42 ± 0.02 | 0.37 ± 0.07 | |||
| >10 years and ≤15 years | 0.37 ± 0.02 | 0.24 ± 0.07 | |||
| >15 years and <20 years | 0.38 ± 0.03 | 0.33 ± 0.10 | |||
| Site of relapse | <0.001 | 0.093 | |||
| Isolated BM | 0.34 ± 0.01 | -- | |||
| Combined BM and EM | 0.45 ± 0.02 | 0.26 ± 0.05 | |||
| Isolated extramedullary | 0.49 ± 0.03 | 0.39 ± 0.07 | |||
| Immunophenotype | <0.001 | <0.001 | |||
| Precursor B cell | 0.40 ± 0.01 | 0.49 ± 0.06 | |||
| T cell | 0.20 ± 0.03 | 0.15 ± 0.04 | |||
| Therapy | <0.001 | 0.010 | |||
| Chemotherapy/radiotherapy only | 0.30 ± 0.01 | ||||
| 0.25 ± 0.05 | |||||
| Allogeneic SCT | 0.54 ± 0.02 | 0.42 ± 0.09 | |||
| Autologous SCT | 0.25 ± 0.06 | 0.50 ± 0.20 | |||
| No data | 0.92 ± 0.04 | 0.67 ± 27 | |||
| NHL Therapy | 0.0043 | 0.76 | |||
| Other | 0.38 ± 0.01 | 0.33 ± 0.04 | |||
| NHL-BFM | 0.26 ± 0.07 | 0.25 ± 0.10 | |||
| (b) pOS | |||||
| OEMR | |||||
| No—2191 | Yes—132 | ||||
| pOS ± SE (10 years) | p * | pOS ± SE (10 years) | p * | ||
| Total group | 0.45 ± 0.01 | 0.37 ± 0.04 | 0.0112 | ||
| Patient characteristics | |||||
| Sex | 0.888 | 0.114 | |||
| Male | 0.45 ± 0.01 | 0.31 ± 0.0 | |||
| Female | 0.44 ± 0.02 | 0.45 ± 0.02 | |||
| Time point of relapse | <0.001 | <.001 | |||
| Very early | 0.23 ± 0.02 | 0.14 ± 0.05 | |||
| Early | 0.34 ± 0.02 | 0.32 ± 0.09 | |||
| Late | 0.63 ± 0.02 | 0.53 ± 0.06 | |||
| Age at relapse | <0.001 | 0.656 | |||
| ≤5 years | 0.37 ± 0.03 | 0.35 ± 0.12 | |||
| ≥5 years and ≤10 years | 0.50 ± 0.02 | 0.42 ± 0.07 | |||
| >10 years and ≤15 years | 0.43 ± 0.02 | 0.29 ± 0.07 | |||
| >15 years and <20 years | 0.41 ± 0.03 | 0.37 ± 0.11 | |||
| Site of relapse | <0.001 | 0.014 | |||
| Isolated BM | 0.41 ± 0.01 | -- | |||
| Combined BM and EM | 0.49 ± 0.02 | 0.27 ± 0.05 | |||
| Isolated extramedullary | 0.56 ± 0.03 | 0.50 ± 0.07 | |||
| Immunophenotype | <0.001 | <0.001 | |||
| Precursor B cell | 0.47 ± 0.01 | 0.52 ± 0.06 | |||
| T cell | 0.23 ± 0.03 | 0.22 ± 0.05 | |||
| Therapy | <.001 | 0.0055 | |||
| Chemotherapy/radiotherapy exclusively | 0.38 ± 0.01 | ||||
| 0.30 ± 0.05 | |||||
| Allogeneic SCT | 0.59 ± 0.02 | 0.47 ± 0.09 | |||
| Autologous SCT | 0.33 ± 0.07 | 0.50 ± 0.20 | |||
| No data | 096 ± 0.03 | 0.67 ± 0.27 | |||
| NHL Therapy | 0.0069 | 0.7645 | |||
| Other | 0.45 ± 0.01 | 0.36 ± 0.05 | |||
| NHL-BFM | 0.31 ± 0.07 | 0.40 ± 0.11 | |||
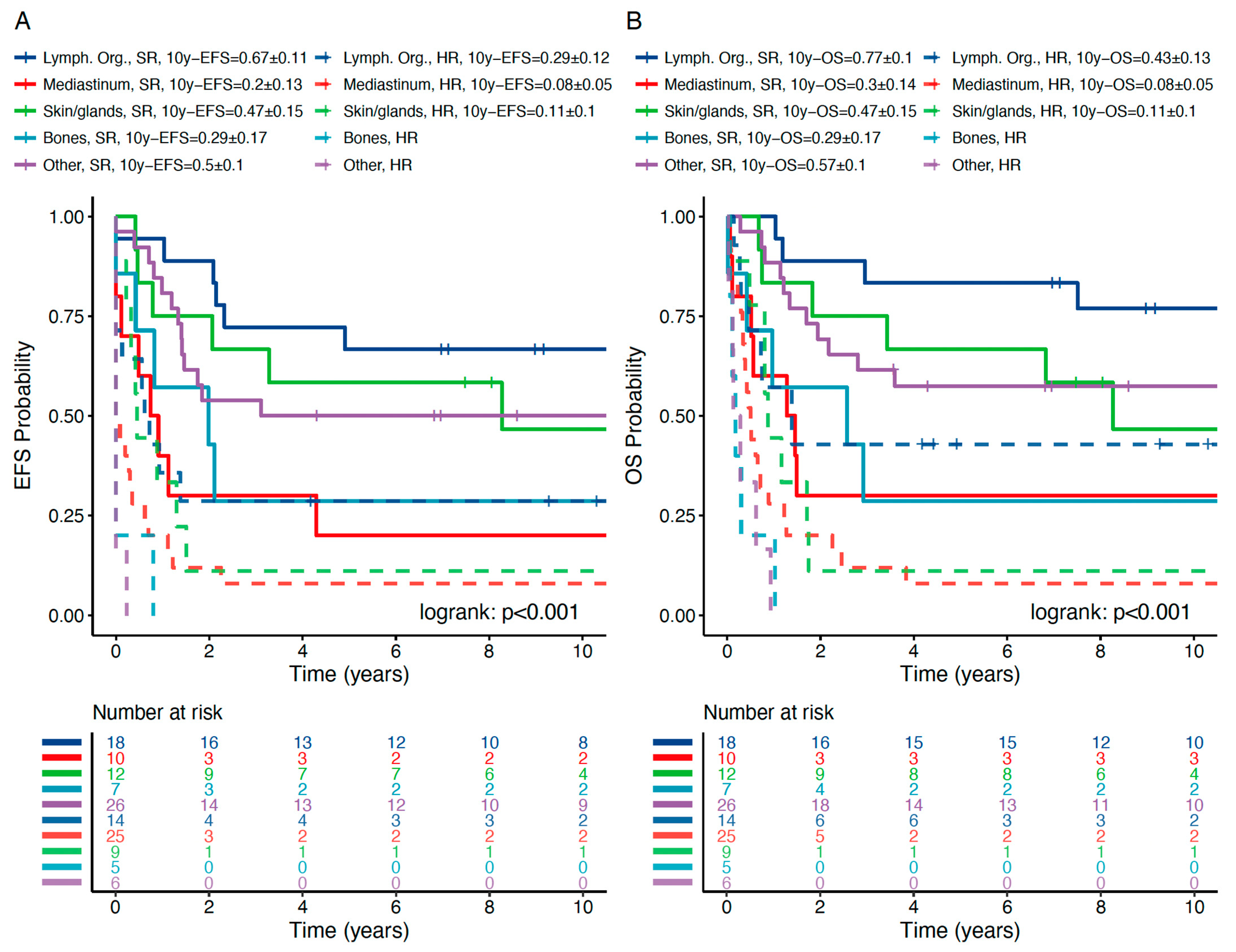
| (c) pEFS and pOS in OEMR Subgroups | |||||
| OEMR Subgroups | |||||
| n | pEFS ± SE (10 years) | p * | pOS ± SE (10 years) | p * | |
| <0.001 | <0.001 | ||||
| Lymph. organs | 32 | 0.50 ± 0.09 | 0.62 ± 0.09 | ||
| SR | 18 | 0.67 ± 0.11 | 0.005 | 0.77 ± 0.10 | 0.015 |
| HR | 14 | 0.29 ± 12 | 0.43 ± 0.13 | ||
| Mediast. organs | 35 | 0.11 ± 0.05 | 0.14 ± 0.06 | ||
| SR | 10 | 0.20 ± 0.13 | 0.113 | 0.30 ± 0.14 | 0.117 |
| HR | 25 | 0.08 ± 0.05 | 0.08 ± 0.05 | ||
| Other compartment | 32 | 0.41 ± 0.09 | 0.47 ± 0.09 | ||
| SR | 26 | 0.50 ± 0.10 | <0.001 | 0.57 ± 0.10 | <0.001 |
| HR | 6 | ** | ** | ||
| Skin/glands | 21 | 0.32 ± 0.11 | 0.32 ± 0.11 | ||
| SR | 12 | 0.47 ± 0.15 | 0.010 | 0.47 ± 0.15 | 0.01 |
| HR | 9 | 0.11 ± 0.10 | 0.11 ± 0.10 | ||
| Bone | 12 | 0.17 ± 0.11 | 0.17 ± 0.11 | ||
| SR | 7 | 0.29 ± 0.17 | 0.01 | 0.29 ± 0.17 | 0.035 |
| HR | 5 | ** | ** | ||
| (a) EFS; Cox Regression; Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|
| Univariate Analysis | Mulitvariate Analysis | |||||
| HR | 95% CI | p (chi) | HR | 95% CI | p (chi) | |
| Gender: ref. male | ||||||
| female | 0.95 | 0.85–1.06 | 0.33 | |||
| Age: ref. < 5 years | ||||||
| age > 5 to ≤ 10 years | 0.7 | 0.6–0.8 | 0.009 | 1.13 | 0.97–1.31 | 0.13 |
| age > 10 to ≤ 15 years | 0.81 | 0.7–0.95 | 0.03 | 1.33 | 1.13–1.56 | <0.001 |
| age > 15 years | 0.81 | 0.67–0.98 | 0.017 | 1.24 | 1.02–1.52 | 0.03 |
| OEM: ref. no OEMR | ||||||
| OEMR | 1.30 | 1.05–1.06 | <0.001 | 1.76 | 1.39–2.23 | <0.001 |
| Time: ref. very early | ||||||
| early | 0.57 | 0.5–0.64 | <0.001 | 0.65 | 0.57–0.075 | <0.001 |
| late | 0.26 | 0.23–0.29 | <0.001 | 0.24 | 0.21–0.028 | <0.001 |
| Site: ref. IBM | ||||||
| CBM | 0.81 | 0.71–0.92 | <0.001 | 0.68 | .059–0.78 | <0.001 |
| IEM | 0.67 | 0.57–0.78 | <0.001 | 0.40 | 0.34–0.47 | <0.001 |
| Phenotype: ref. BCP | ||||||
| T-ALL | 2.37 | 2.06–2.72 | <0.001 | 1.61 | 1.38–1.88 | <0.001 |
| NHL protocol: ref. no | ||||||
| NHL-BFM | 1.68 | 1.25–2.23 | <0.001 | 1.25 | 0.92–1.70 | 0.80 |
| (b) OS; Cox Regression; Multivariate Analysis | ||||||
| Univariable Analysis | Mulitvariable Analysis | |||||
| HR | 95% CI | p (chi) | HR | 95% CI | p (chi) | |
| Gender: ref. male | ||||||
| female | 0.99 | 0.88–1.11 | 0.821 | |||
| Age: ref. < 5 years | ||||||
| age > 5 to ≤ 10 years | 0.66 | 0.57–0.77 | <0.001 | 1.08 | 0.92–1.27 | 0.33 |
| age > 10 to ≤ 15 years | 0.82 | 0.69–0.96 | 0.013 | 1.33 | 1.12–1.57 | <0.001 |
| age > 15 years | 0.88 | 0.72–1.07 | 0.205 | 1.41 | 1.15–1.73 | <0.001 |
| OEM: ref. no OEMR | ||||||
| OEMR | 1.33 | 1.07–1.66 | 0.011 | 1.71 | 1.33–1.29 | <0.001 |
| Time: ref. very early | ||||||
| early | 0.57 | 0.5–0.65 | <0.001 | 0.65 | 0.57–0.75 | <0.001 |
| late | 0.24 | 0.21–0.27 | <0.001 | 0.22 | 0.19–0.75 | <0.001 |
| Site: ref. IBM | ||||||
| CBM | 0.87 | 0.76–0.99 | 0.042 | 0.72 | 0.62–0.84 | <0.001 |
| IEM | 0.63 | 0.54–0.75 | <0.001 | 0.38 | 0.32–0.45 | <0.001 |
| Phenotype: ref. BCP | ||||||
| T-ALL | 2.41 | 2.09–2.78 | <0.001 | 1.62 | 1.38–1.89 | <0.001 |
| NHL protocol: ref. no | ||||||
| NHL-BFM | 1.56 | 1.14–2.13 | 0.005 | 1.21 | 0.88–1.70 | 0.82 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lissat, A.; van Schewick, C.; Steffen, I.G.; Arakawa, A.; Bourquin, J.-P.; Burkhardt, B.; Henze, G.; Mann, G.; Peters, C.; Sramkova, L.; et al. Other (Non-CNS/Testicular) Extramedullary Localizations of Childhood Relapsed Acute Lymphoblastic Leukemia and Lymphoblastic Lymphoma—A Report from the ALL-REZ Study Group. J. Clin. Med. 2021, 10, 5292. https://doi.org/10.3390/jcm10225292
Lissat A, van Schewick C, Steffen IG, Arakawa A, Bourquin J-P, Burkhardt B, Henze G, Mann G, Peters C, Sramkova L, et al. Other (Non-CNS/Testicular) Extramedullary Localizations of Childhood Relapsed Acute Lymphoblastic Leukemia and Lymphoblastic Lymphoma—A Report from the ALL-REZ Study Group. Journal of Clinical Medicine. 2021; 10(22):5292. https://doi.org/10.3390/jcm10225292
Chicago/Turabian StyleLissat, Andrej, Claudia van Schewick, Ingo G. Steffen, Ayumu Arakawa, Jean-Pierre Bourquin, Birgit Burkhardt, Guenter Henze, Georg Mann, Christina Peters, Lucie Sramkova, and et al. 2021. "Other (Non-CNS/Testicular) Extramedullary Localizations of Childhood Relapsed Acute Lymphoblastic Leukemia and Lymphoblastic Lymphoma—A Report from the ALL-REZ Study Group" Journal of Clinical Medicine 10, no. 22: 5292. https://doi.org/10.3390/jcm10225292