
Variability in Oral Iron Prescription and the Effect on Spanish Mothers’ Health: A Prospective Longitudinal Study

 ,
,  , , ,
, , ,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Iron Prescription
3.2. Actual Consumption
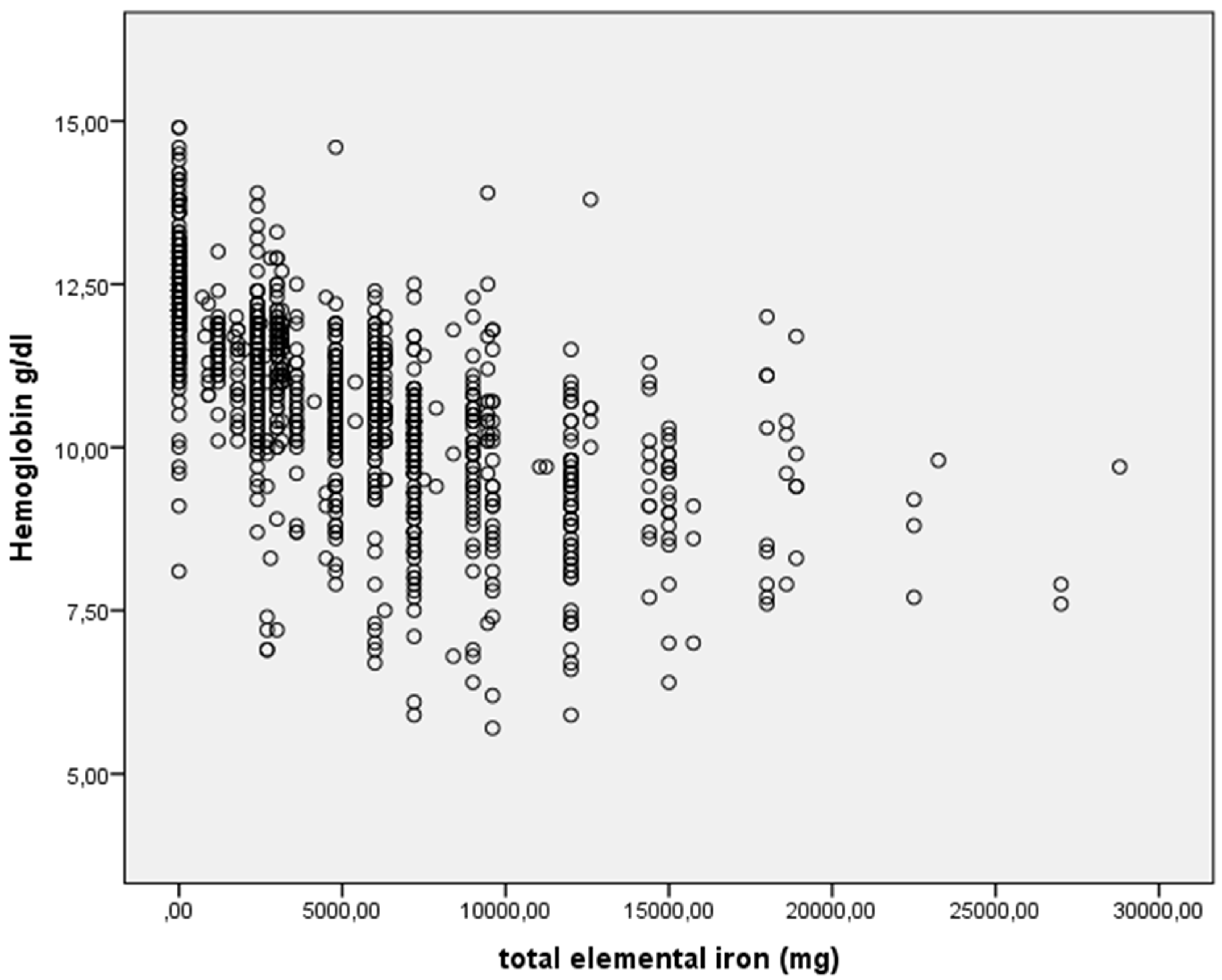
3.3. Association between Iron Consumption and Maternal Health
4. Discussion
5. Conclusions
6. Limits and Strength
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Milman, N. Postpartum anemia I: Definition, prevalence, causes, and consequences. Ann. Hematol. 2011, 90, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- Corwin, E.J.; Murray-Kolb, L.E.; Beard, J.L. Low Hemoglobin Level Is a Risk Factor for Postpartum Depression. J. Nutr. 2003, 133, 4139–4142. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.L.; Hendricks, M.K.; Perez, E.M.; Murray-Kolb, L.E.; Berg, A.; Vernon-Feagans, L.; Irlam, J.; Isaacs, W.; Sive, A.; Tomlinson, M. Maternal Iron Deficiency Anemia Affects Postpartum Emotions and Cognition. J. Nutr. 2005, 135, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Perez, E.M.; Hendricks, M.K.; Beard, J.L.; Murray-Kolb, L.E.; Berg, A.; Tomlinson, M.; Irlam, J.; Isaacs, W.; Njengele, T.; Sive, A.; et al. Mother-infant interactions and infant development are altered by maternal iron deficiency anemia. J. Nutr. 2005, 135, 850–855. [Google Scholar] [CrossRef] [Green Version]
- Murray-kolb, L.E.; Beard, J.L. Iron deficiency and child and maternal health 1–4. Am. J. Clin. Nutr. 2009, 89, 946–950. [Google Scholar] [CrossRef] [Green Version]
- Group de travail de la ligne directrice sur l’HPP. Association of Ontario Midwives. Hémorragie Post-Partum. 2016. Available online: http://www.ontariomidwives.ca (accessed on 10 May 2021).
- Pavord, S.; Daru, J.; Prasannan, N.; Robinson, S.; Stanworth, S.; Girling, J. UK guidelines on the management of iron deficiency in pregnancy. Br. J. Haematol. 2020, 188, 819–830. [Google Scholar] [CrossRef] [Green Version]
- Beentjes, M.; Jans, S. Revised practice guideline ’Anaemia in midwifery practice’. Ned Tijdschr Geneeske 2012, 156, A3711. Available online: https://www.ntvg.nl/artikelen/herziene-beroepsstandaard-%E2%80%98anemie-de-verloskundige-praktijk%E2%80%99/volledig (accessed on 10 May 2021).
- Simon, E.-G.; Laffon, M. Soins maternels après accouchement voie basse et prise en charge des complications du post-partum immédiat: Recommandations pour la pratique clinique. J. Gynécol. Obstet. Biol. Reprod. 2015, 44, 1101–1110. [Google Scholar] [CrossRef]
- Breymann, C.; Honegger, C.; Hösli, I.; Surbek, D. Diagnosis and treatment of iron-deficiency anaemia in pregnancy and postpartum. Arch. Gynecol. Obstet. 2017, 296, 1229–1234. [Google Scholar] [CrossRef]
- Api, O.; Breyman, C.; Çetiner, M.; Demir, C.; Ecder, T. Diagnosis and treatment of iron deficiency anemia during pregnancy and the postpartum period: Iron deficiency anemia working group consensus report. Turk. J. Obstet. Gynecol. 2015, 12, 173–181. [Google Scholar] [CrossRef]
- World Health Organisation (WHO). Guideline: Iron Supplementation in Postpartum Women; World Health Organisation (WHO): Geneva, Switzerland, 2016; Available online: https://apps.who.int/iris/handle/10665/249242 (accessed on 10 May 2021).
- Kshirsagar, N.A. Rational use of medicines: Cost consideration & way forward. Indian J. Med. Res. 2016, 144, 502–505. [Google Scholar] [CrossRef] [PubMed]
- Barroso, F.; Allard, S.; Kahan, B.C.; Connolly, C.; Smethurst, H.; Choo, L.; Khan, K.; Stanworth, S. Prevalence of maternal anaemia and its predictors: A multi-centre study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 159, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Urquizu, X.; Rodriguez, M.; García, A. Anemia en el embarazo y el posparto inmediato. Prevalencia y Factores de Riesgo. Med. Clin. 2016, 146, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Cano-Climent, A.; Oliver-Roig, A.; Cabrero-García, J.; de Vries, J.; Richart-Martínez, M. The Spanish version of the Fatigue Assessment Scale: Reliability and validity assessment in postpartum women. PeerJ 2017, 5, e3832. [Google Scholar] [CrossRef] [Green Version]
- Balestroni, G.; Bertolotti, G. EuroQol-5D (EQ-5D): An instrument for measuring quality of life. Monaldi Arch. Chest Dis. 2015, 78, 155–159. [Google Scholar] [CrossRef]
- Calje, E.; Skinner, J. The challenge of defining and treating anemia and iron deficiency in pregnancy: A study of New Zealand midwives’ management of iron status in pregnancy and the postpartum period. Birth 2017, 44, 181–190. [Google Scholar] [CrossRef]
- Paganini, D.; Zimmermann, M.B. The effects of iron fortification and supplementation on the gut microbiome and diarrhea in infants and children: A review. Am. J. Clin. Nutr. 2017, 106 (Suppl. S6), 1688S–1693S. [Google Scholar] [CrossRef] [Green Version]
- Tolkien, Z.; Stecher, L.; Mander, A.P.; Pereira, D.I.A. Ferrous Sulfate Supplementation Causes Significant Gastrointestinal Side-Effects in Adults: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0117383. [Google Scholar] [CrossRef] [Green Version]
- Turawa, E.B.; Musekiwa, A.; Rohwer, A.C. Interventions for treating postpartum constipation. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Milman, N.; Bergholt, T.; Byg, K.-E.; Eriksen, L.; Hvas, A.-M. Reference intervals for haematological variables during normal pregnancy and postpartum in 434 healthy Danish women. Eur. J. Haematol. 2007, 79, 39–46. [Google Scholar] [CrossRef]
- Miller, E.M. The reproductive ecology of iron in women. Am. J. Phys. Anthr. 2016, 159, 172–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milman, N. Postpartum anemia II: Prevention and treatment. Ann. Hematol. 2012, 91, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Bjørke-Monsen, A.-L.; Torsvik, I.K.; Ueland, P.M.; Sætran, H.A.; Sandberg, S. Increased yet iron-restricted erythropoiesis in postpartum mothers. Ann. Hematol. 2012, 91, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Markova, V.; Norgaard, A.; Jorgensen, K.; Langhoff-Roos, J. Treatment for women with postpartum iron deficiency anaemia (Review). Cochrane Database Syst. Rev. 2015, 1–38. [Google Scholar] [CrossRef]
- Fisher, A.L.; Nemeth, E. Iron homeostasis during pregnancy. Am. J. Clin. Nutr. 2017, 106 (Suppl. S6), 1567S–1574S. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, S.-R.; McHugh, K.; Drakesmith, H. Regulation of Hepcidin by Erythropoiesis: The Story So Far. Annu. Rev. Nutr. 2016, 36, 417–434. [Google Scholar] [CrossRef]
- Moretti, D.; Goede, J.S.; Zeder, C.; Jiskra, M.; Chatzinakou, V.; Tjalsma, H.; Melse-Boonstra, A.; Brittenham, G.; Swinkels, D.W.; Zimmermann, M.B. Oral iron supplements increase hepcidin and decrease iron absorption from daily or twice-daily doses in iron-depleted young women. Blood 2015, 126, 1981–1989. [Google Scholar] [CrossRef]
- Stoffel, N.U.; I Cercamondi, C.; Brittenham, G.; Zeder, C.; Geurts-Moespot, A.J.; Swinkels, D.W.; Moretti, D.; Zimmermann, M.B. Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: Two open-label, randomised controlled trials. Lancet Haematol. 2017, 4, e524–e533. [Google Scholar] [CrossRef]
- Jansen, A.G.; Duvekot, J.J.; Hop, W.C.; Essink-Bot, M.-L.; Beckers, E.A.; Karsdorp, V.H.; Scherjon, S.A.; Steegers, E.A.; Van Rhenen, D.J. New insights into fatigue and health-related quality of life after delivery. Acta Obstet. Gynecol. Scand. 2007, 86, 579–584. [Google Scholar] [CrossRef]
- Miller, C.M.; Ramachandran, B.; Akbar, K.; Carvalho, B.; Butwick, A.J. The impact of postpartum hemoglobin levels on maternal quality of life after delivery: A prospective exploratory study. Ann. Hematol. 2016, 95, 2049–2055. [Google Scholar] [CrossRef] [Green Version]
- Güven, Z.; Holm, C.; Rosthoej, S.; Langhoff-Roos, J. Association between blood loss at delivery and fatigue in the puerperium: A prospective longitudinal study. J. Matern. Fetal Neonatal Med. 2020, 33, 606–611. [Google Scholar] [CrossRef]
- Van Der Woude, D.; Pijnenborg, J.M.; Verzijl, J.M.; Van Wijk, E.M.; De Vries, J. Health status and fatigue of postpartum anemic women: A prospective cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 181, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Rioux, F.M.; Savoie, N.; Allard, J. Is there a link between postpartum anemia and discontinuation of breastfeeding? Can. J. Diet. Pr. Res. 2006, 67, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Horie, S.; Nomura, K.; Takenoshita, S.; Nakagawa, J.; Kido, M.; Sugimoto, M. A relationship between a level of hemoglobin after delivery and exclusive breastfeeding initiation at a baby friendly hospital in Japan. Environ. Health Prev. Med. 2017, 22, 40. [Google Scholar] [CrossRef] [PubMed]
- Chessman, J.; Patterson, J.; Nippita, T.; Drayton, B.; Ford, J. Haemoglobin concentration following postpartum haemorrhage and the association between blood transfusion and breastfeeding: A retrospective cohort study. BMC Res. Notes 2018, 11, 686. [Google Scholar] [CrossRef]
- Abe, S.K.; Balogun, O.O.; Ota, E.; Takahashi, K.; Mori, R. Supplementation with multiple micronutrients for breastfeeding women for improving outcomes for the mother and baby. Cochrane Database Syst. Rev. 2016, 2016, CD010647. [Google Scholar] [CrossRef] [PubMed]
- Cantor, A.G.; Bougatsos, C.; Dana, T.; Blazina, I.; McDonagh, M. Routine Iron Supplementation and Screening for Iron Deficiency Anemia in Pregnancy: A Systematic Review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2015, 162, 566–576. [Google Scholar] [CrossRef] [Green Version]
- Abraha, I.; Bonacini, M.I.; Montedori, A.; Di Renzo, G.C.; Angelozzi, P.; Micheli, M.; Germani, A.; Carloni, D.; Scaccetti, A.; Palmieri, G.; et al. Oral iron-based interventions for prevention of critical outcomes in pregnancy and postnatal care: An overview and update of systematic reviews. J. Evid. Based Med. 2019, 12, 155–166. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Puerperal | |||
|---|---|---|---|---|
| First Visit (N = 1066) | Second Visit | |||
| With Blood Analysis * (N = 966) | Without Blood Analysis ** (N = 100) | p | ||
| Age (X, SD) | 33.4 (5.3) | 33.6 (5.2) | 31.4 (6.5) | <0.01 |
| Place of residence ***, (n, %) | ||||
| Urban Zone: High socioeconomic status | 195 (18.3) | 176 (18.2) | 19 (19.0) | 0.05 |
| Urban Zone: Medium socioeconomic status | 363 (34.1) | 337 (34.9) | 26 (26.0) | |
| Low level: Low socioeconomic status | 250 (23.5) | 237 (24.5) | 21 (21.0) | |
| Rural zone | 258 (24.2) | 216 (22.4) | 34 (34.0) | |
| Country (n, %) | ||||
| Spain | 823 (77.2) | 759 (78.6) | 64 (64.0) | <0.01 |
| Others | 243 (22.8) | 207 (21.4) | 36 (36.0) | |
| Delivery (n, %) | ||||
| Primiparous | 540 (50.7) | 498 (51.6) | 42 (42.0) | 0.07 |
| Multiparous | 526 (49.3) | 468 (48.4) | 58 (58.0) | |
| Type of delivery (n, %) | ||||
| Eutocid delivery | 702 (65.9) | 634 (65.5) | 68 (68.0) | 0.95 |
| Vacuum extraction | 81 (7.6) | 74 (7.7) | 7 (7.0) | |
| Forceps | 70 (6.6) | 63 (6.5) | 7 (7.0) | |
| Caesarean delivery | 213 (20.0) | 195 (20.2) | 18 (18.0) | |
| Iron deficiency first trimester (n, %) | ||||
| No | 972 (93.2) | 886 (93.7) | 86 (88.7) | 0.06 |
| Yes | 71 (6.8) | 60 (6.3) | 11(11.3) | |
| First trimester anemia (n, %) | ||||
| No | 1028 (98.3) | 934 (98.5) | 94 (95.9) | 0.06 |
| Yes | 18 (1.7) | 14 (1.5) | 4 (4.1) | |
| Iron deficiency second trimester (n, %) | ||||
| No | 562 (53.6) | 513 (53.9) | 49 (50.5) | 0.52 |
| Yes | 486 (46.4) | 438 (46.1) | 48 (49.5) | |
| Second trimester anemia (n, %) | ||||
| No | 932 (88.6) | 844 (88.4) | 88 (90.7) | 0.49 |
| Yes | 120 (11.4) | 111 (11.6) | 9 (9.3) | |
| Third trimester anemia (n, %) | ||||
| No | 920 (88.0) | 836 (88.1) | 84 (86.6) | 0.67 |
| Yes | 126 (12.0) | 113 (11.9) | 13 (13.4) | |
| Anemia at 24 h postpartum (n, %) | ||||
| No | 805 (75.5) | 724 (74.9) | 81 (81.0) | 0.180 |
| Yes | 261 (24.5) | 242 (25.1) | 19 (19.0) | |
| Prescription of iron in pregnancy (n, %) | ||||
| No | 180 (16.9) | 159 (16.5) | 21 (21.0) | 0.25 |
| Yes | 886 (83.1) | 807 (83.5) | 79 (79.0) | |
| Postpartum iron prescription (n, %) | ||||
| No | 200 (18.8) | 160 (16.6) | 40 (40.0) | <0.01 |
| Yes | 866 (81.2) | 806 (83.4) | 60 (60.0) | |
| Initial Hb (g/dL) | Women n (%) | Treatment Prescription: n (%) | Oral Iron Regimen (mg of Elemental Iron) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Without Treatment | With Prescribed Treatment | Dose/Day (mg) | Duration (Days) | Total Fe (mg) | ||||||||
| T + IV + O | T + O | IV + O | O | P50 | Range | P50 | Range | P50 | Range | |||
| <6 | 3 (0.3) | 3 (100) | 160 | 120 | 60 | 30 | 9600 | 4800 | ||||
| 6–6.9 | 14 (1.3) | 4 (28.6) | 8 (57.1) | 1 (7.1) | 1 (7.1) | 100 | 170 | 82.5 | 45 | 9000 | 12,300 | |
| 7–7.9 | 34 (3.2) | 1 (2.9) | 8 (23.6) | 19 (55.9) | 6 (17.6) | 160 | 280 | 75 | 60 | 9600 | 24,300 | |
| 8–8.9 | 69 (6.5) | 1 (1.4) | 1 (1.4) | 19 (27.5) | 48 (69.6) | 130 | 260 | 75 | 152 | 9000 | 20,100 | |
| 9–9.9 | 141 (13.2) | 4 (2.8) | 2 (1.4) | 135 (95.7) | 100 | 280 | 75 | 150 | 9000 | 26,400 | ||
| <10 | 261 (24,5) | 5 (1.9) | 5 (1.9) | 20 (7.6) | 41 (15.7) | 190 (72.8) | 100 | 280 | 75 | 152 | 9000 | 26,400 |
| 10–10.9 | 286 (26.8) | 5 (1.7) | 281 (98.3) | 80 | 280 | 60 | 150 | 6000 | 177,000 | |||
| 11–11.9 | 308 (28.9) | 35 (11.4) | 273 (88.6) | 80 | 270 | 30 | 164 | 3000 | 18,100 | |||
| 12–12.9 | 161 (15.1) | 115 (71.4) | 46 (28.6) | 80 | 270 | 30 | 72 | 3000 | 17,280 | |||
| 13–13.9 | 39 (3.7) | 30 (76.9) | 9 (23.1) | 80 | 65 | 30 | 90 | 2400 | 11,400 | |||
| 14–14.9 | 11 (1.1) | 10 (90.9) | 1 (9.1) | 80 | – | 60 | – | 4800 | – | |||
| ≥10 | 805 (75.5) | 195 (24.2) | 610 (75.8) | 80 | 280 | 30 | 180 | 3000 | 18,180 | |||
| Initial Hb (g/dL) | Prescription (p) vs. Consumption (C) | Dose/Day | Days | Fe Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | n | % (95% CI) | p# | P50 | IQR | p## | P50 | Range | p## | P50 | Range | p## | |
| <8 | 51 | P = 51 | 100 | 0.13 | 160 | 280 | 0.01 | 75 | 75 | <0.01 | 9600 | 24,300 | <0.01 |
| C = 47 | 92.2 (81.1–97.8) | 80 | 270 | 34 | 31 | 2960 | 9480 | ||||||
| 8–8.9 | 64 | P = 63 | 98.4 (91.6–100) | 0.07 | 160 | 260 | 0.06 | 75 | 152 | <0.01 | 9000 | 20,100 | <0.01 |
| C = 57 | 89.1 (80.6–97.5) | 80 | 180 | 33 | 33 | 2640 | 7000 | ||||||
| 9–9.9 | 133 | P = 129 | 97.0 (92.5–99.2) | 0.03 | 100 | 280 | 0.08 | 75 | 150 | <0.01 | 9000 | 26,400 | <0.01 |
| C = 119 | 89.5 (83.9–95.1) | 80 | 280 | 34 | 29 | 2900 | 9170 | ||||||
| <10 | 248 | P = 243 | 98.0 (95.4–99.3) | <0.01 | 100 | 280 | <0.01 | 75 | 152 | <0.01 | 9000 | 26,400 | <0.01 |
| C = 223 | 89.9 (86.0–93.9) | 80 | 280 | 34 | 34 | 2800 | 9760 | ||||||
| 10–10.9 | 273 | P = 268 | 98.2 (95.8–99.4) | <0.01 | 80 | 280 | 0.03 | 60 | 150 | <0.01 | 6000 | 17,700 | <0.01 |
| C = 172 | 63.0 (57.1–68.9) | 80 | 173 | 30 | 38 | 2050 | 5910 | ||||||
| 11–11.9 | 299 | P = 265 | 88.6 (84.9–92.4) | <0.01 | 80 | 270 | 0.09 | 60 | 60 | <0.01 | 3150 | 17,100 | <0.01 |
| C = 91 | 30.4 (25.1–35.8) | 80 | 75 | 30 | 38 | 1800 | 3580 | ||||||
| ≥12 | 199 | P = 53 | 26.6 (20.2–33.0) | <0.01 | 100 | 220 | <0.01 | 30 | 30 | <0.01 | 3000 | 15,600 | <0.01 |
| C = 10 | 5.01 (1.7–8.3) | 100 | 25 | 30 | 7 | 3000 | 1380 | ||||||
| ≥10 | 771 | P = 586 | 76.0 (72.9–79.1) | <0.01 | 80 | 280 | <0.01 | 60 | 150 | <0.01 | 4800 | 17,700 | <0.01 |
| C = 273 | 35.4 (32.0–38.8) | 80 | 173 | 30 | 38 | 2080 | 5910 | ||||||
| Initial Hb | Iron Intake | Iron Deficiency (SF < 15 µg/L) | Anemia (Hb < 12 g/dL) | Breastfeeding | Fatigue | Health Condition | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NOT n (%) | YES n (%) | OR (CI) | NOT n (%) | YES n (%) | OR (CI) | NOT n (%) | YES n (%) | OR (CI) | P50 (Range) | p# | P50 (Range) | p# | ||
| <10 | NO | 17 (73.9) | 6 (26.1) | 3.6 (1.3–10.3) * | 12 (52.2) | 11 (47.8) | 3.0 (1.3–7.2) * | 10 (43.5) | 13 (56.5) | 2.4 (1.0–5.9) * | 19 (20) | 0.34 | 75 (50) | 0.48 |
| YES | 195 (91.1) | 19 (8.9) | 177 (76.6) | 54 (23.4) | 52 (24.1) | 164 (75.9) | 19 (30) | 75 (60) | ||||||
| 10–10.9 | NO | 94 (95.9) | 4 (4.1) | 2.4 (0.6–10.8) | 91 (91.0) | 9 (9.0) | 4.2 (1.2–13.9) * | 13 (13.0) | 87 (87.0) | 0.7 (0.4–1.4) | 18 (21) | 0.43 | 80 (40) | 0.70 |
| YES | 168 (98.2) | 3 (1.8) | 168 (97.8) | 4 (2.2) | 30 (17.4) | 142 (82.6) | 18 (21) | 78 (40) | ||||||
| 11–11.9 | NO | 195 (98.0) | 4 (2.0) | 1.8 (0.2–16.4) | 199 (99.5) | 1 (0.5) | 0.2 (0.0–2.4) | 22 (11.2) | 175 (88.8) | 0.7 (0.4–1.4) | 18 (31) | 0.45 | 80 (45) | 0.01 ** |
| YES | 88 (98.9) | 1 (1.1) | 88 (97.8) | 2 (2.2) | 22 (25.6) | 64 (74.4) | 18 (24) | 75 (40) | ||||||
| ≥12 | NO | 153 (100) | 0 (0.0) | – | 153 (99.4) | 1 (0.6) | – | 27 (17.0) | 124 (83.0) | – | 18 (24) | 0.65 | 80 (46) | 0.44 |
| YES | 9 (100) | 0 (0.0) | 9 (100) | 0 (0.0) | 0 (0.0) | 8 (100) | 18 (3) | 82.5 (35) | ||||||
| ≥10 | NO | 442 (98.2) | 8 (1.8) | 1.2 (0.4–4.0) | 443 (97.6) | 11 (2.4) | 0.8 (0.3–2.1) | 62 (13.8) | 386 (86.2) | 0.7 (0.4–0.9) * | 18 (31) | 0.42 | 80 (46) | 0.02 |
| YES | 265 (98.5) | 4 (1.5) | 263 (97.8) | 6 (2.2) | 52 (19.6) | 214 (80.4) | 18 (24) | 78 (40) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz de Viñaspre-Hernández, R.; García-Erce, J.A.; Rodríguez-Velasco, F.J.; Gea-Caballero, V.; Sufrate-Sorzano, T.; Garrote-Cámara, M.E.; Urra-Martínez, R.; Juárez-Vela, R.; Czapla, M.; Santolalla-Arnedo, I. Variability in Oral Iron Prescription and the Effect on Spanish Mothers’ Health: A Prospective Longitudinal Study. J. Clin. Med. 2021, 10, 5212. https://doi.org/10.3390/jcm10215212
Ruiz de Viñaspre-Hernández R, García-Erce JA, Rodríguez-Velasco FJ, Gea-Caballero V, Sufrate-Sorzano T, Garrote-Cámara ME, Urra-Martínez R, Juárez-Vela R, Czapla M, Santolalla-Arnedo I. Variability in Oral Iron Prescription and the Effect on Spanish Mothers’ Health: A Prospective Longitudinal Study. Journal of Clinical Medicine. 2021; 10(21):5212. https://doi.org/10.3390/jcm10215212
Chicago/Turabian StyleRuiz de Viñaspre-Hernández, Regina, José Antonio García-Erce, Francisco José Rodríguez-Velasco, Vicente Gea-Caballero, Teresa Sufrate-Sorzano, María Elena Garrote-Cámara, Raquel Urra-Martínez, Raúl Juárez-Vela, Michał Czapla, and Iván Santolalla-Arnedo. 2021. "Variability in Oral Iron Prescription and the Effect on Spanish Mothers’ Health: A Prospective Longitudinal Study" Journal of Clinical Medicine 10, no. 21: 5212. https://doi.org/10.3390/jcm10215212