
Effectiveness of Magnetic Stimulation in the Treatment of Urinary Incontinence: A Systematic Review and Results of Our Study


Abstract
:1. Introduction
Magnetic Stimulation and UI
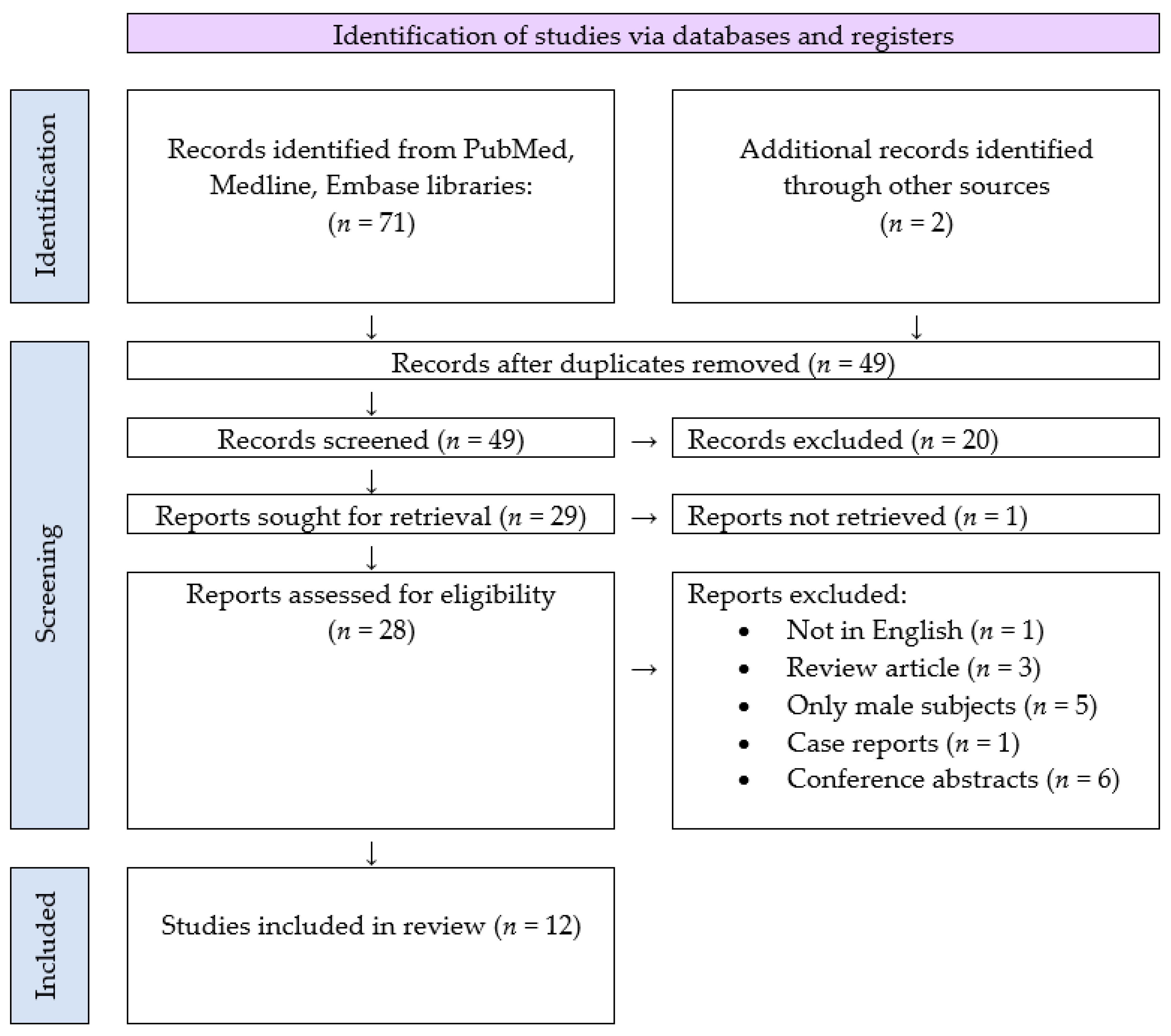
2. Methodology of the Systemic Review
Search Strategy and Selection Criteria
3. Results of the Systematic Review
4. Materials and Methods of the Clinical Study
5. Results of the Clinical Study
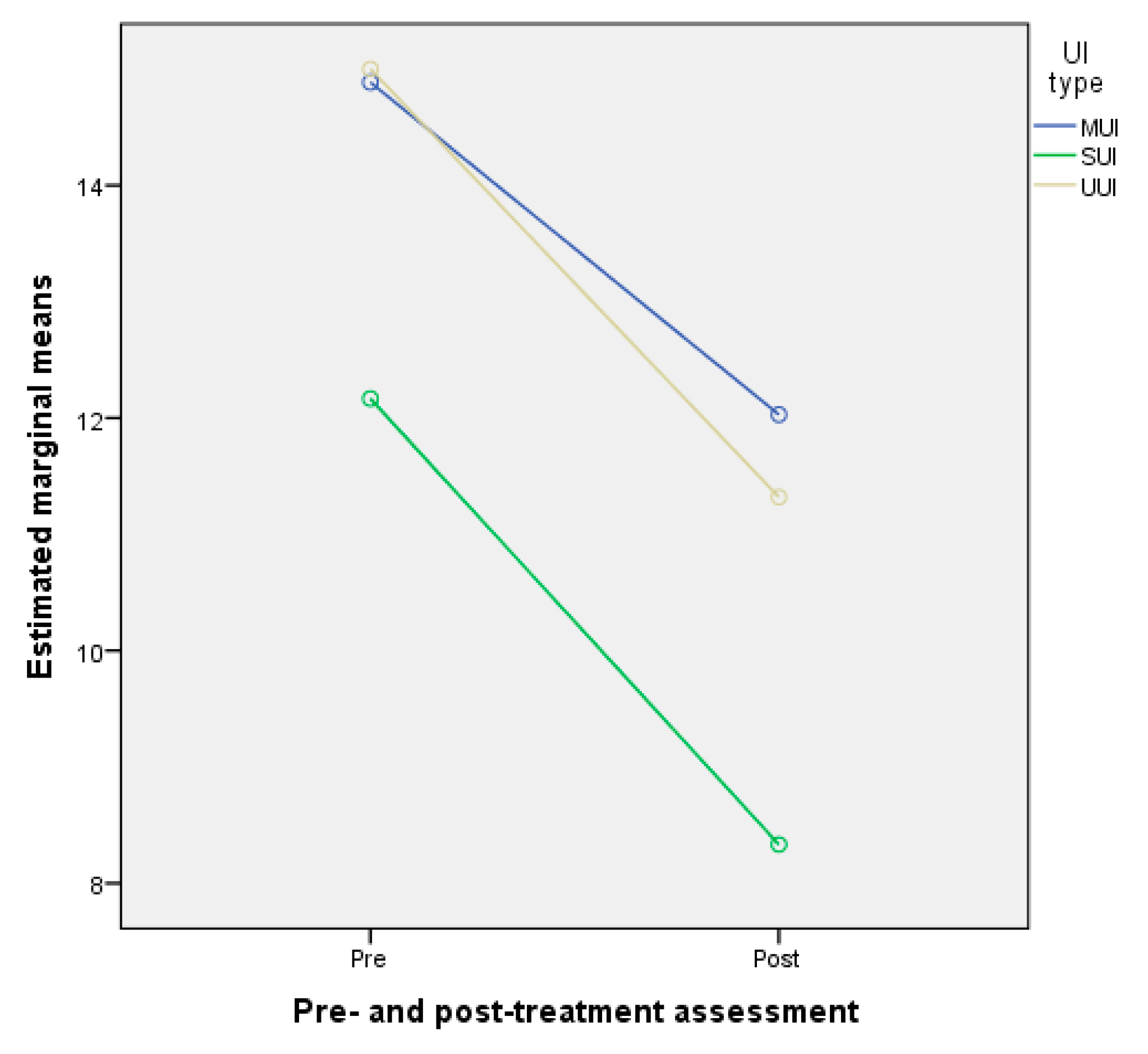
5.1. Differences between Pre- and Post-Treatment Assessment of ICIQ-UI SF Scores by UI Type
5.2. Correlation between Pre- and Post-Treatment Assessment ICIQ-UI SF Scores by UI Type
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abrams, P.; Blaivas, J.G.; Stanton, S.L.; Andersen, J.T. The International Continence Society Committee on Standardisation of Terminology. The standardisation of terminology of lower urinary tract function. Scand. J. Urol. Nephrol. Suppl. 1988, 114, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Haylen, B.T.; de Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K.; et al. International Urogynecological Association; International Continence Society. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol. Urodyn. 2010, 29, 4–20. [Google Scholar] [CrossRef]
- Shamliyan, T.; Wyman, J.; Kane, R.L. Nonsurgical Treatments for Urinary Incontinence in Adult Women: Diagnosis and Comparative Effectiveness; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2012.
- Lukanović, D.; Blaganje, M.; Barbic, M. Urinary incontinence treatment algorithm. Zdrav Vestn. 2021, 90, 275–287. [Google Scholar]
- Abrams, P.; Andersson, K.E.; Birder, L.; Brubaker, L.; Cardozo, L.; Chapple, C.; Cottenden, A.; Davila, W.; De Ridder, D.; Dmochowski, R.; et al. Members of Committees; Fourth International Consultation on Incontinence. Fourth International Consultation on Incontinence Recommendations of the International Scientific Committee: Evaluation and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Neurourol. Urodyn. 2010, 29, 213–240. [Google Scholar] [CrossRef] [PubMed]
- Kralj, B. Epidemiology of female urinary incontinence, classification of urinary incontinence, urinary incontinence in elderly women. Eur. J. Obstet. Gynecol. Reprod. Biol. 1994, 55, 39–41. [Google Scholar] [CrossRef]
- Lukanović, A. Urinary incontinence. In Gynecology and Perinatology; Takač, I., Geršak, K., Eds.; Medicinska Fakulteta: Maribor, Slovenia, 2016; pp. 223–230. [Google Scholar]
- Keršič, M.; Keršič, M.; Kunič, T.; Garzon, S.; Laganà, A.S.; Barbič, M.; Lukanović, A.; Lukanović, D. Single-incision mini-sling for the treatment of female stress urinary incontinence: Is it actually inferior to transobturator vaginal tape and tension-free vaginal tape? Gynecol. Minim. Invasive Ther. 2020, 9, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; La Rosa, V.L.; Rapisarda, A.M.; Laganà, A.S. The importance of a multidisciplinary approach for women with pelvic organ prolapse and cystocele. Oman Med. J. 2017, 32, 263–264. [Google Scholar] [CrossRef]
- Galloway, N.T.M.; El-Galley, R.E.S.; Sand, P.K.; Appell, R.A.; Russell, H.W.; Carlan, S.J. Extracorporeal magnetic innervation therapy for stress urinary incontinence. Urology 1999, 53, 1108–1111. [Google Scholar] [CrossRef]
- Voorham-van der Zalm, P.J.; Pelger, R.C.M.; Stiggelbout, A.M.; Elzevier, H.W.; Lycklama à Nijeholt, G.A.B. Effects of magnetic stimulation in the treatment of pelvic floor dysfunction. BJU Int. 2006, 97, 1035–1038. [Google Scholar] [CrossRef] [Green Version]
- Galloway, N.T.; El-Galley, R.E.; Sand, P.K.; Appell, R.A.; Russell, H.W.; Carlin, S.J. Update on extracorporeal magnetic innervation (EXMI) therapy for stress urinary incontinence. Urology 2000, 56 (Suppl. 6), 82–86. [Google Scholar] [CrossRef]
- Yamanishi, T.; Yasuda, K.; Sakakibara, R.; Hattori, T.; Ito, H.; Murakami, S. Pelvic floor electrical stimulation in the treatment of stress incontinence: An investigational study and placebo controlled double-blind trial. J. Urol. 1997, 158, 2127–2131. [Google Scholar] [CrossRef]
- Vodusek, D.B. Anatomy and neurocontrol of the pelvic floor. Digestion 2004, 69, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Fall, M.; Lindström, S. Functional electrical stimulation: Physiological basis and clinical principles. Review article. Int. Urogynecol. J. 1994, 5, 296–304. [Google Scholar] [CrossRef]
- Evans, B.A.; Daube, J.R.; Litchy, W.J. A comparison of magnetic and electrical stimulation of spinal nerves. Muscle Nerve 1990, 13, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Olney, R.K.; So, Y.T.; Goodin, D.S.; Aminoff, M.J. A comparison of magnetic and electrical stimulation of peripheral nerves. Muscle Nerve 1990, 13, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Burkhard, F.C.; Bosch, J.L.H.R.; Lemack, G.E.; Nambiar, A.K.; Thiruchelvam, N.; Tubaro, A. EAU Guidelines on Urinary Incontinence in Adults; European Association of Urology: Arnhem, The Netherlands, 2020. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Lim, R.; Liong, M.L.; Leong, W.S.; Khan, N.A.K.; Yuen, K.H. Magnetic stimulation for stress urinary incontinence: Study protocol for a randomized controlled rial. Trials 2015, 16, 279. [Google Scholar] [CrossRef] [Green Version]
- Lim, R.; Liong, M.L.; Leong, W.S.; Khan, N.A.K.; Yuen, K.H. Pulsed magnetic stimulation for stress urinary incontinence: 1-year follow up results. J. Urol. 2017, 197, 130–138. [Google Scholar] [CrossRef]
- Yamanishi, T.; Suzuki, T.; Sato, R.; Kaga, K.; Kaga, M.; Fuse, M. Effects of magnetic stimulation on urodynamic stress incontinence refractory to pelvic floor muscle training in a randomized sham-controlled study. Low Urin. Tract Sympt. 2017, 11, 1–5. [Google Scholar] [CrossRef]
- Weber-Rajek, M.; Radzimińska, A.; Strączyńska, A.; Strojek, K.; Piekorz, Z.; Kozakiewicz, M.; Styczyńska, H. A randomized-controlled trial pilot study examining the effect of pelvic floor muscle training on the irisin concentration in overweight or obese elderly women with stress urinary incontinence. Biomed. Res. Int. 2019, 2019, 7356187. [Google Scholar] [CrossRef] [Green Version]
- Weber-Rajek, M.; Strączyńska, A.; Strojek, K.; Piekorz, Z.; Pilarska, B.; Podhorecka, M.; Sobieralska-Michalak, K.; Goch, A.; Radzimińska, A. Assessment of the effectiveness of pelvic floor muscle training (PFMT) and extracorporeal magnetic innervation (ExMI) in treatment of stress urinary incontinence in women: A randomized controlled trial. Biomed. Res. Int. 2020, 2020, 1019872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özengin, N.; Bakar, Y.; Cinar Özdemir, Ö.; Duran, B. The comparison of EMG-biofeedback and extracorporeal magnetic innervation treatments in women with urinary incontinence. Clin. Exp. Obstet. Gynecol. 2016, 43, 550–554. [Google Scholar] [PubMed]
- Sylantieva, E.; Zarkovic, D.; Soldatskaia, R.; Evgeniia, A.; Orazov, M. Electromyographic evaluation of the pelvic muscles activity after high-intensity focused electromagnetic procedure and electrical stimulation in women with pelvic floor dysfunction. Sex. Med. 2020, 8, 282–289. [Google Scholar]
- Samuels, J.B.; Pezzella, A.; Berenholz, J.; Alinsod, R. Safety and efficacy of a non-invasive high-intensity focused electromagnetic field (HIFEM) device for treatment of urinary incontinence and enhancement of quality of life. Lasers Surg. Med. 2019, 51, 760–766. [Google Scholar] [CrossRef]
- Vadalà, M.; Palmieri, B.; Malagoli, A.; Laurino, C. High-power magnetotherapy: A new weapon in urinary incontinence? Low Urin. Tract Symptoms. 2018, 10, 266–270. [Google Scholar] [CrossRef]
- Doğanay, M.; Kılıç, S.; Yılmaz, N. Long-term effects of extracorporeal magnetic innervations in the treatment of women with urinary incontinence: Results of 3-year follow-up. Arch. Gynecol. Obstet. 2010, 282, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.J.; Sun, R.; Chen, L.J. The therapeutic efficiency of extracorporeal magnetic innervation treatment in women with urinary tract dysfunction following radical hysterectomy. J. Obstet. Gynaecol. 2015, 35, 74–78. [Google Scholar] [CrossRef]
- Bakar, Y.; Çinar Özdemir, Ö.; Özengin, N.; Duran, B. The use of extracorporeal magnetic innervation for the treatment of stress urinary incontinence in older women: A pilot study. Arch. Gynecol. Obstet. 2011, 284, 1163–1168. [Google Scholar] [CrossRef]
- Tsai, P.Y.; Wang, C.P.; Hsieh, C.Y.; Tsai, Y.A.; Yeh, S.C.; Chuang, T.Y. Long-term sacral magnetic stimulation for refractory stress urinary incontinence. Arch. Phys. Med. Rehabil. 2014, 95, 2231–2238. [Google Scholar] [CrossRef]
- Rotar, M.; Tršinar, B.; Kisner, K.; Barbič, M.; Sedlar, A.; Gruden, J.; Vodušek, D.B. Correlations between the ICIQ-UI short form and urodynamic diagnosis. Neurourol. Urodynam. 2009, 28, 501–505. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Yamanishi, T.; Yasuda, K.; Suda, S.; Ishikawa, N.; Sakakibara, R.; Hattori, T. Effect of functional continuous magnetic stimulation for urinary incontinence. J. Urol. 2000, 163, 456–459. [Google Scholar] [CrossRef]
- Yokoyama, T.; Fujita, O.; Nishiguchi, J.; Nozaki, K.; Nose, H.; Inoue, M.; Ozawa, H.; Kumon, H. Extracorporeal magnetic innervation treatment for urinary incontinence. Int. J. Urol. 2004, 11, 602–606. [Google Scholar] [CrossRef] [PubMed]
- Elfil, M.; Negida, A. Sampling methods in clinical research; an educational review. Emergency 2017, 5, e52. [Google Scholar]
- Dumas-Mallet, E.; Button, K.S.; Boraud, T.; Gonon, F.; Munafò, M.R. Low statistical power in biomedical science: A review of three human research domains. R. Soc. Open Sci. 2017, 4, 160254. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Vitale, S.G.; La Rosa, V.L.; Rapisarda, A.M.; Laganà, A.S. Sexual life in women with stress urinary incontinence. Oman Med. J. 2017, 32, 174–175. [Google Scholar] [CrossRef]
- Laganà, A.S.; La Rosa, V.L.; Rapisarda, A.M.; Vitale, S.G. Pelvic organ prolapse: The impact on quality of life and psychological well-being. J. Psychosom. Obstet. Gynaecol. 2018, 39, 164–166. [Google Scholar] [CrossRef]
- Lim, R.; Liong, M.L.; Leong, S.; Lau, Y.K.; Leong, W.S.; Khan, N.A.K.; Yuen, K.H. Effect of pulsed magnetic stimulation on sexual function in couples with female stress urinary incontinence partners. J. Sex Marital Ther. 2018, 44, 260–268. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Study Type | Diagnostic Method(s) |
|---|---|---|
| Lim et al., 2015, 2017 [20,21] | Multicenter, randomized, double-blind, sham-controlled (1:1 ratio) |
|
| Yamanishi et al., 2017 [22] | Pilot, randomized, sham-controlled (active: sham = 2:1) |
|
| Weber-Rajek et al., 2019 [23] | Randomized, double-blind, controlled pilot study |
|
| Weber-Rajek et al., 2020 [24] | Randomized, double-blind, controlled trial |
|
| Özengin et al., 2016 [25] | Open-label, not controlled, data on randomization N/A |
|
| Sylantieva et al., 2020 [26] |
| |
| Samuels et al., 2019 [27] | Prospective, multi-center, open-label, single-arm study; data on randomization N/A |
|
| Vadalà et al., 2017 [28] | Retrospective observational study |
|
| Doğanay 2010 [29] | Prospective, open-label, single-center, not controlled |
|
| Sun et al., 2014 [30] | Open-label, single-center, not controlled |
|
| Bakar et al., 2010 [31] | Open-label, single-center |
|
| Tsai et al., 2014 [32] | Sham-controlled, double-blind, parallel study |
|
| Study | UI Type | Sample Size | Control Group | Length of Intervention Period and Frequency |
|---|---|---|---|---|
| Lim et al., 2015, 2017 [20,21] | SUI | 120 | Yes, 1:1 ratio | 20 min stimulation twice a week for 8 weeks (16 sessions total) |
| Yamanishi et al., 2017 [22] | SUI | 39 | Yes, active stimulation and sham stimulation group, 2:1 ratio | 20 min stimulation once a week for 10 weeks (10 sessions total) |
| Weber-Rajek et al., 2019 [23] | SUI | 52 | Yes, active: control = 28:24 | 15 min stimulation three times a week for 4 weeks (12 sessions total) |
| Weber-Rajek et al., 2020 [24] | SUI | 111 | Yes, PFMT (40), MS (37), control (34) | PFMT: 45 min sessions three times a week for 4 weeks (12 sessions total) |
| Özengin et al., 2016 [25] | SUI | 67 | No | MS: 20 min sessions three times a week for 8 weeks (24 sessions), EMG-BF: three sessions of 20 min in 8 weeks, PFMT: N/A |
| Sylantieva et al., 2020 [26] | SUI? | 95 | Yes | MS: 28 min sessions two to three times a week (10 sessions total) |
| Samuels et al., 2019 [27] | SUI (49%), UUI (11%), MUI (40%) | 75 | No | 28 min twice a week, for 3 weeks (six sessions total) |
| Vadalà et al., 2017 [28] | SUI (50%), UUI (20%), MUI (30%) | 20 | No | 20 min stimulation twice a week for 3 weeks (six sessions total) |
| Doğanay 2010 [29] | SUI, UUI | 137; SUI: 68, UUI: 69 | No | 20 min sessions twice a week for 8 weeks (16 sessions total) |
| Sun et al., 2014 [30] | SUI, UUI, MUI | 32 | No | 20 min sessions twice a week for 12 weeks (24 sessions total) |
| Bakar et al., 2010 [31] | SUI | 13 | No | 20 min sessions twice a week for 6 weeks (12 sessions total) |
| Tsai et al., 2014 [32] | SUI | 30 | Yes, active group: 18, sham group: 12 | 20 min every weekday for 12 days (12 sessions total) |
| Study | Device | Outcomes (Changes) |
|---|---|---|
| Lim et al., 2015, 2017 [20,21] | QRS-1010 PelviCenter (QRS International, Ruggell, Liechtenstein) |
|
| Yamanishi et al., 2017 [22] | Armchair-type magnetic stimulator (Nihon Kohden, Tokyo, Japan) |
|
| Weber-Rajek et al., 2019 [23] | NeoControl chair (Neotonus Inc., Marietta, GA, USA) |
|
| Weber-Rajek et al., 2020 [24] | MS: NeoControl chair (Neotonus Inc., Marietta, GA, USA) |
|
| Özengin et al., 2016 [25] | N/A |
|
| Sylantieva et al., 2020 [26] | N/A |
|
| Samuels et al., 2019 [27] | BTL EMSELLA (BTL Industries Inc., Boston, MA, USA) |
|
| Vadalà et al., 2017 [28] | Magneto STYM (Iskra Medical, Ljubljana, Slovenia) |
|
| Doğanay 2010 [29] | Neotonus Inc., (Marietta, GA, USA) |
|
| Sun et al., 2014 [30] | BioCon-2000WTM, Mcube Technology Co. (Korea) |
|
| Bakar et al., 2010 [31] | EMD, E-6000 MAGTHER, TR |
|
| Tsai et al., 2014 [32] | Magstim Rapid2 and a 70 mm figure-8 coil/sham coil |
|
| Study | Follow-Up Period | Benefits (Statistically Significant) |
|---|---|---|
| Lim et al., 2015, 2017 [20,21] | 1, 2, 5, 8, 14 months |
|
| Yamanishi et al., 2017 [22] | 10 weeks |
|
| Weber-Rajek et al., 2019 [23] | 4 weeks | Reduction of:
|
| Weber-Rajek et al., 2020 [24] | 4 weeks |
|
| Özengin et al., 2016 [25] | 8 weeks |
|
| Sylantieva et al., 2020 [26] | 4 weeks |
|
| Samuels et al., 2019 [27] | 3 weeks, 3 months |
|
| Vadalà et al., 2017 [28] | 3 weeks |
|
| Doğanay 2010 [29] | 2, 4, 6, 8 weeks, 6 months, 1, 2, 3 years |
|
| Sun et al., 2014 [30] | 4 weeks, 12 weeks |
|
| Bakar et al., 2010 [31] | 6 weeks |
|
| Tsai et al., 2014 [32] | 18 weeks (4.5 months) |
|
| Study | Limitations |
|---|---|
| Lim et al., 2015, 2017 [20,21] |
|
| Yamanishi et al., 2017 [22] |
|
| Weber-Rajek et al., 2019 [23] |
|
| Weber-Rajek et al., 2020 [24] |
|
| Özengin et al., 2016 [25] |
|
| Sylantieva et al., 2020 [26] |
|
| Samuels et al., 2019 [27] |
|
| Vadalà et al., 2017 [28] |
|
| Doğanay 2010 [29] |
|
| Sun et al., 2014 [30] |
|
| Bakar et al., 2010 [31] |
|
| Tsai et al., 2014 [32] |
|
| Programs | Step | Frequency of Magnetic Stimulation | Time | Active Time | Pause Time | Therapy Time |
|---|---|---|---|---|---|---|
| UUI | 1/1 | 10 Hz | 12 s | 6 s | 6 s | 20 min |
| SUI | 1/1 | 35 Hz | 12 s | 6 s | 6 s | 20 min |
| MUI | 1/2 | 10 Hz | 12 s | 6 s | 6 s | 10 min |
| 2/2 | 35 Hz | 12 s | 6 s | 6 s | 10 min |
| Variable | UI Type | ||
|---|---|---|---|
| MUI (n = 35) | SUI (n = 17) | UUI (n = 23) | |
| Age (years) | |||
| Median | 73.0 | 63.0 | 73.0 |
| IQR (Q1–Q3) | 15.0 (14.0–17.0) | 21.0 (14.0–17.0) | 12.0 (14.0–17.0) |
| Duration of problems (years) | |||
| Median | 6.0 | 6.0 | 5.0 |
| IQR (Q1–Q3) | 7.0 (3.0–10.0) | 19.5 (3.0–22.5) | 8.0 (2.0–10.0) |
| BMI (kg/m2) | |||
| Median | 25.7 | 23.6 | 26.0 |
| IQR (Q1–Q3) | 10.3 (21.6–31.9) | 4.0 (22.3–26.3) | 7.4 (24.2–31.6) |
| Menopause (% yes) | 30 (85.7) | 13 (76.5) | 21 (92.9) |
| Diabetes (% yes) | 1 (2.9) | 0 (0.0) | 5 (20.0) |
| Previous gynecological surgeries (% yes) | 16 (45.7) | 5 (27.8) | 11 (48.0) |
| Variable | UI Type | ||
|---|---|---|---|
| MUI (n = 35) | SUI (n = 17) | UUI (n = 23) | |
| Pre-treatment (ICIQ-UI SF score) | |||
| Median | 16.0 | 10.0 | 16.0 |
| IQR (Q1–Q3) | 3.0 (14.0–17.0) | 5.5 (9.5–15.0) | 3.0 (13.0–16.0) |
| Post-treatment (ICIQ-UI SF score) | |||
| Median | 11.0 | 8.0 | 11.0 |
| IQR (Q1–Q3) | 7.0 (9.0–16.0) | 4.5 (6.0–10.5) | 6.0 (8.0–14.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lukanović, D.; Kunič, T.; Batkoska, M.; Matjašič, M.; Barbič, M. Effectiveness of Magnetic Stimulation in the Treatment of Urinary Incontinence: A Systematic Review and Results of Our Study. J. Clin. Med. 2021, 10, 5210. https://doi.org/10.3390/jcm10215210
Lukanović D, Kunič T, Batkoska M, Matjašič M, Barbič M. Effectiveness of Magnetic Stimulation in the Treatment of Urinary Incontinence: A Systematic Review and Results of Our Study. Journal of Clinical Medicine. 2021; 10(21):5210. https://doi.org/10.3390/jcm10215210
Chicago/Turabian StyleLukanović, David, Tina Kunič, Marija Batkoska, Miha Matjašič, and Matija Barbič. 2021. "Effectiveness of Magnetic Stimulation in the Treatment of Urinary Incontinence: A Systematic Review and Results of Our Study" Journal of Clinical Medicine 10, no. 21: 5210. https://doi.org/10.3390/jcm10215210