
Diet and Chronic Non-Cancer Pain: The State of the Art and Future Directions

 , ,
, ,
Abstract
:1. Introduction
1.1. Diet, Pain, and Systemic Inflammation
1.2. Diet, Pain, and Comorbidities
1.3. Dietary Intake of People Experiencing Pain
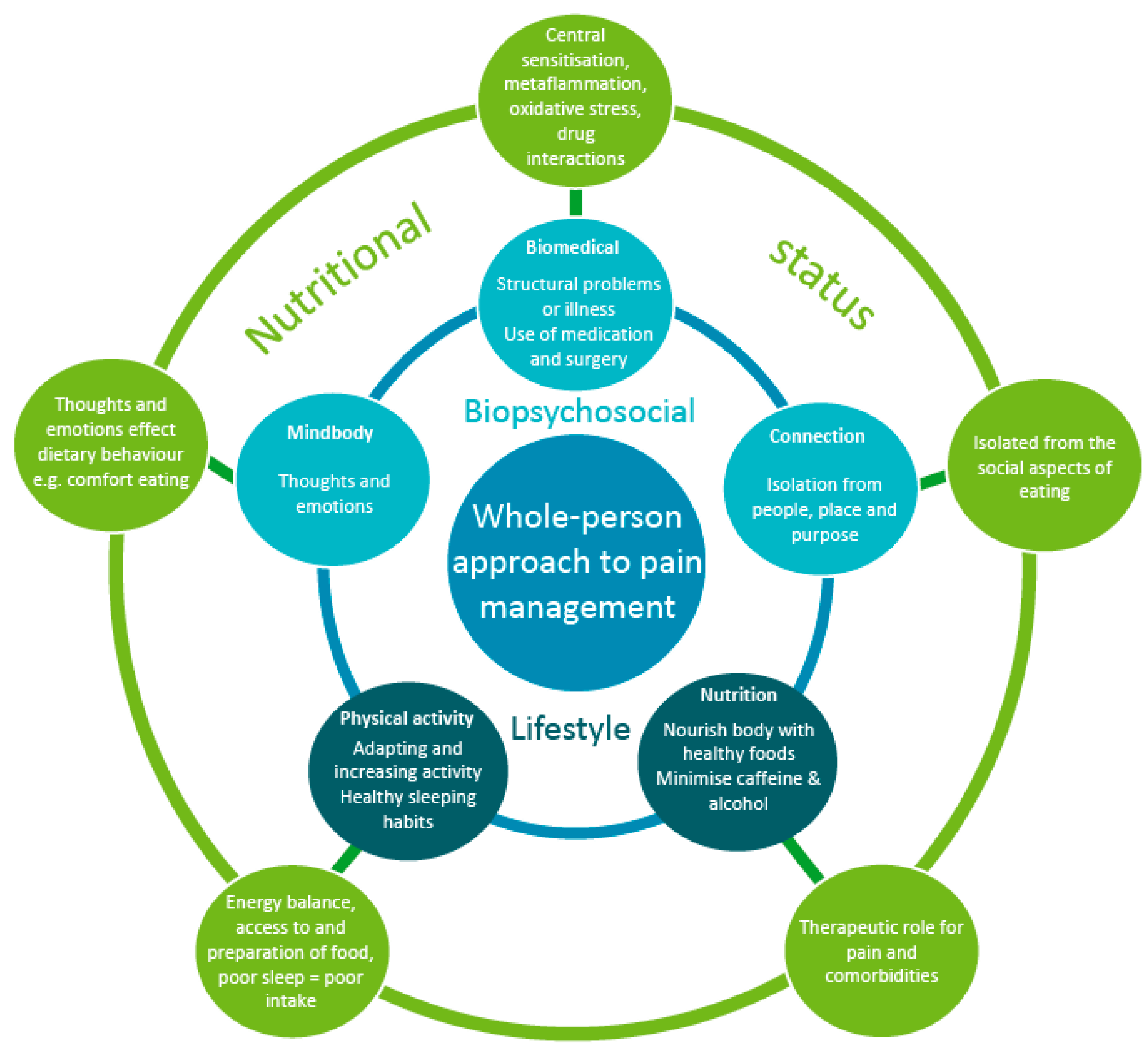
1.4. Diet and the Whole-Person Approach to Pain Management
1.4.1. Diet and Biomedical Aspects
1.4.2. Relationships between Diet, Mental Health, and Lifestyle
1.4.3. Diet and the Whole-Person Approach to Pain Management and Behaviour Change
2. State of the Art
2.1. Nutrition Interventions for People Experiencing Chronic Non-Cancer Pain
2.2. Recommendations for Clinicians
2.2.1. Dietary Assessment
2.2.2. Optimise Diet Quality
2.2.3. Consume Fruit and Vegetables Rich in Phytonutrients to Reduce Oxidative Stress
2.2.4. Consume Long Chain and Monounsaturated Fats (e.g., Omega-3 and Olive Oil)
2.2.5. Increase Fibre and Water Intake
2.2.6. Reduce and Limit Ultra-Processed Food and Added Sugar Intake
2.2.7. Other Nutritional Considerations
2.3. Nutrition Considerations for Vulnerable Groups
2.3.1. Older People
2.3.2. Culturally and Linguistically Diverse Populations
3. Future Directions for Clinical Practice
4. Future Directions for Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Key Messages and Practical Nutrition Tips for Pain Management
- Key Messages:
- People with chronic non-cancer pain (CNCP) should be encouraged to consume:
- A wide range of nutrient-dense foods (e.g., fruits, vegetables, whole grain breads and cereals, meat, dairy, and their alternatives) to ensure they are meeting their nutritional requirements.
- The recommended amount of fruit and vegetables should be based on your country’s dietary guidelines and to focus on consuming a rainbow of colors every day.
- Long chain and monounsaturated fats (e.g., omega-3 and olive oil).
- More fibre and fluid. Adult females should consume 25 g/day of fibre and adult males 30 g/day. Adults should aim for 2–3 L of water per day.
- Less ultra-processed foods and foods containing added sugars.
- Find resources and strategies through your country’s dietetic organisation such as Dietitian Australia, the Academy of Nutrition and Dietetics, The European Federation of the Associations of Dietitians, or the British Dietetics Association that support this information and that you can provide to patients that will assist them.
- Practical Tips for Conducting Dietary Assessments:
- Assist patients to screen their diet quality using tools such as the Healthy Eating Quiz
- If you are concerned about potential nutritional deficiencies consider referring patients to a dietitian for a comprehensive dietary assessment and personalised advice and support.
- Practical Tips to Optimize Diet Quality
- Become familiar and learn about your country’s dietary guidelines.
- Use an inclusive approach, emphasise important foods that should be added (e.g., vegetables), rather than focusing on foods that should be removed (e.g., energy-dense snack foods).
- Ensure that nutrition-based education is aimed at improving diet quality, as this will address systemic inflammation and enhance pain management.
- Be aware that this is a broad approach and there may be individualized variation. For personalized dietary advice patients should be referred to a dietitian.
- Educate patients on the role of vitamins and minerals in pain management and food sources of these nutrients. For example, good dietary-sources of Vitamin D include fish and eggs, good sources of Vitamin B12 are meat, fish, and dairy, and magnesium can be found in green leafy vegetables and whole grains.
- Encourage patients to spend some time outside to obtain Vitamin D from sun exposure. For most people, 10–15 min of sun on the arms and legs most days of the week will provide most of the Vitamin D required. However, this will vary based on location and the time of year.
- Practical Tips for Fruit and Vegetable Consumption Which are Rich in Phytonutrients to Reduce Oxidative Stress
- Educate your patients on the important role of fruits and vegetables in pain management.
- Encourage your patients to buy in-season fruits and vegetables and to try a new fruit or vegetable each week where possible.
- If preparation and cooking is an issue for your patients, encourage them to include variety by using frozen mixed vegetables or reduced-salt canned vegetables (e.g., tomatoes and lentils), which can be easily incorporated into meals such as stir-frys, stews, or pasta dishes. Frozen fruits and vegetables are a great option as they maintain their nutritional quality.
- Work with your patient to come up with ways to incorporate fruit and vegetables into their daily routine, e.g., including vegetables as a snack throughout the day, ensuring half their plate is covered in vegetables at main meals, using frozen berries as a snack, or the addition of yoghurt or cereal.
- Practical Tips for Consuming Long Chain and Monounsaturated Fats (e.g., Omega-3 and Olive Oil)
- Educate patients on the role of omega-3 and olive oil in pain management.
- Communicate, motivate and encourage patients to consume foods high in omega-3 and olive oil.
- ○
- Consume oily fish (e.g., salmon and sardines), flax seed oil or canola oil, linseed, and walnuts to boost omega-3 intake. Aim for a minimum of 2–3 servings of oily fish per week.
- ○
- Use extra virgin olive oil as the preferred oil in cooking and salad dressings.
- ○
- Reduce saturated and trans fats (e.g., butter, processed foods, and hydrogenated vegetable oils).
- ○
- Limit polyunsaturated fats high in omega-6 such as sunflower and safflower oils.
- Supplements: It is preferable to focus on diet quality through food intake rather than via supplements. Seek advice from a dietitian or medical professional if your patient is considering high doses of fish oil supplements. Evidence suggests that 3000 mg of omega-3, over a 3-month period reduces pain experiences, especially in rheumatoid arthritis [106]. There are two types of omega-3 fats in fish oil supplements, EPA and DHA. Supplements which have a ratio of EPA/DHA of ≥1.5 are most beneficial. Suggest good quality brands which contain high doses of omega-3.
- Practical Tips to Increase Fibre and Water Consumption
- Encourage patients to consume the recommended serves of fruits and vegetables to increase fibre intake.
- Provide practical suggestions such as switching to whole meal or whole grain breads, pasta, and breakfast cereals. Keep the skin on fruits and incorporate a variety of mixed vegetables and lentils into meals. Add psyllium husk or bran to meals at breakfast time.
- Fill a large (1.5 L) drinking bottle with water every day and set a goal to consume it throughout the day.
- Practical Tips to Reduce and Limit Ultra-Processed Food and Added Sugar Intake
- Work with patients to swap sugary and energy drinks for water or mineral water flavoured with fresh fruit.
- Encourage consumption of healthy convenient snacks such as fruit, vegetable sticks, or yoghurt.
- Incorporate strategies to help patients cook meals at home rather than relying on highly processed conveniently prepared or take away foods.
- Recommend cooking meals in bulk and freezing the leftovers so patients have a quick, easy, and healthy meal they can have when they have a flare up and do not feel like cooking.
- Practical Nutrition Tips for Vulnerable Populations
- Older People
- Clinicians and aged care facilities should monitor for signs of malnutrition and dehydration. Assist older people and their families to optimise their food and fluid intake to reduce pain experiences in older people. Some practical tips and strategies can be found in Table 2.
- People from CALD Backgrounds
- Be aware of eating patterns and beliefs of the cultural group you are working with (recognising individual variation).
- Adapt your practice accordingly and include family and community where possible.
- Culturally informed approaches enhance engagement [107].
References
- Classification of Chronic Pain. Descriptions of chronic pain syndromes and definitions of pain terms. Prepared by the Inter-national Association for the Study of Pain, Subcommittee on Taxonomy. Pain Suppl. 1986, 3, S1–S226. [Google Scholar]
- Croft, P.; Blyth, F.M.; van der Windt, D. The global occurrence of chronic pain: An introduction. In Chronic Pain Epidemiology: From Aetiology to Public Health; Academic Press: Cambridge, MA, USA, 2010; pp. 9–18. [Google Scholar]
- Kurita, G.P.; Sjøgren, P.; Juel, K.; Højsted, J.; Ekholm, O. The burden of chronic pain: A cross-sectional survey focussing on diseases, immigration, and opioid use. Pain 2012, 153, 2332–2338. [Google Scholar] [CrossRef]
- Deloitte Access Economics. The Cost of Pain in Australia; Deloitte Access Economics: Sydney, Australia, 2019. [Google Scholar]
- Gaskin, D.J.; Richard, P. The Economic Costs of Pain in the United States. J. Pain 2012, 13, 715–724. [Google Scholar] [CrossRef]
- Allingham, S.; Blanchard, M.; Tardif, H.; Quinsey, K.; Bryce, M.; Cameron, K.; White, J.; Damm, S.; Eagar, K. Electronic Persistent Pain Outcomes Collaboration Annual Data Report 2019; University of Woolongong: Wollongong, Australia, 2020. [Google Scholar]
- Hayes, C.; Hodson, F.J. A Whole-Person Model of Care for Persistent Pain: From Conceptual Framework to Practical Application. Pain Med. 2011, 12, 1738–1749. [Google Scholar] [CrossRef] [Green Version]
- Hayes, C.; Naylor, R.; Egger, G. Understanding Chronic Pain in a Lifestyle Context: The Emergence of a Whole-Person Ap-proach. Am. J. Lifestyle Med. 2012, 6, 421–428. [Google Scholar] [CrossRef]
- Holliday, S.; Hayes, C.; Jones, L.; Gordon, J.; Harris, N.; Nicholas, M. Prescribing wellness: Comprehensive pain management outside specialist services. Aust. Prescr. 2018, 41, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Hansen, K.A.; McKernan, L.C.; Carter, S.D.; Allen, C.; Wolever, R.Q. A Replicable and Sustainable Whole Person Care Model for Chronic Pain. J. Altern. Complement. Med. 2019, 25 (Suppl. 1), S86–S94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaak, E.E.; Antoine, J.; Benton, D.; Björck, I.; Bozzetto, L.; Brouns, F.; Diamant, M.; Dye, L.; Hulshof, T.; Holst, J.J.; et al. Impact of postprandial glycaemia on health and prevention of disease. Obes. Rev. 2012, 13, 923–984. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, N.; Ye, F.; Crumley, E.T.; Bello, A.; Stenvinkel, P.; Tonelli, M. Temporal Associations Among Body Mass Index, Fasting Insulin, and Systemic Inflammation: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e211263. [Google Scholar] [CrossRef]
- Chambers, E.S.; Byrne, C.S.; Morrison, D.; Murphy, K.G.; Preston, T.; Tedford, C.; Garcia-Perez, I.; Fountana, S.; Serrano-Contreras, J.I.; Holmes, E.; et al. Dietary supplementation with inulin-propionate ester or inulin improves insulin sensitivity in adults with overweight and obesity with distinct effects on the gut microbiota, plasma metabolome and systemic inflammatory responses: A randomised cross-over trial. Gut 2019, 68, 1430–1438. [Google Scholar] [CrossRef] [PubMed]
- Marion-Letellier, R.; Savoye, G.; Ghosh, S. Polyunsaturated fatty acids and inflammation. IUBMB Life 2015, 67, 659–667. [Google Scholar] [CrossRef] [Green Version]
- Raphael, W.; Sordillo, L.M. Dietary Polyunsaturated Fatty Acids and Inflammation: The Role of Phospholipid Biosynthesis. Int. J. Mol. Sci. 2013, 14, 21167–21188. [Google Scholar] [CrossRef] [Green Version]
- Simopoulos, A.P.; DiNicolantonio, J.J. The importance of a balanced ω-6 to ω-3 ratio in the prevention and management of obesity. Open Hear. 2016, 3, e000385. [Google Scholar] [CrossRef] [Green Version]
- Bendsen, N.T.; Stender, S.; Szecsi, P.; Pedersen, S.B.; Basu, S.; Hellgren, L.; Newman, J.; Larsen, T.M.; Haugaard, S.B.; Astrup, A. Effect of industrially produced trans fat on markers of systemic inflammation: Evidence from a randomized trial in women. J. Lipid Res. 2011, 52, 1821–1828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oteng, A.-B.; Kersten, S. Mechanisms of Action of trans Fatty Acids. Adv. Nutr. 2020, 11, 697–708. [Google Scholar] [CrossRef]
- Nijs, J.; Yilmaz, S.T.; Elma, Ö.; Tatta, J.; Mullie, P.; Vanderweeën, L.; Clarys, P.; Deliens, T.; Coppieters, I.; Weltens, N.; et al. Nutritional intervention in chronic pain: An innovative way of targeting central nervous system sensitization? Expert Opin. Ther. Targets 2020, 24, 793–803. [Google Scholar] [CrossRef]
- Ji, R.R.; Nackley, A.; Huh, Y.; Terrando, N.; Maixner, W. Neuroinflammation and Central Sensitization in Chronic and Widespread Pain. Anesthesiology 2018, 129, 343–366. [Google Scholar] [CrossRef]
- Rizzetto, L.; Fava, F.; Tuohy, K.M.; Selmi, C. Connecting the immune system, systemic chronic inflammation and the gut microbiome: The role of sex. J. Autoimmun. 2018, 92, 12–34. [Google Scholar] [CrossRef] [PubMed]
- Bjørklund, G.; Aaseth, J.; Doşa, M.D.; Pivina, L.; Dadar, M.; Pen, J.J.; Chirumbolo, S. Does diet play a role in reducing nociception related to inflammation and chronic pain? Nutrition 2019, 66, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Manach, C.; Scalbert, A.; Morand, C.; Rémésy, C.; Jiménez, L. Polyphenols: Food sources and bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chai, S.C.; Davis, K.; Zhang, Z.; Zha, L.; Kirschner, K.F. Effects of Tart Cherry Juice on Biomarkers of Inflammation and Ox-idative Stress in Older Adults. Nutrients 2019, 11, 228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelley, D.S.; Adkins, Y.; Laugero, K.D. A Review of the Health Benefits of Cherries. Nutrients 2018, 10, 368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kent, K.; Charlton, K.; Roodenrys, S.; Batterham, M.; Potter, J.; Traynor, V.; Gilbert, H.; Morgan, O.; Richards, R. Consumption of anthocyanin-rich cherry juice for 12 weeks improves memory and cognition in older adults with mild-to-moderate dementia. Eur. J. Nutr. 2017, 56, 333–341. [Google Scholar] [CrossRef] [Green Version]
- Schell, J.; Scofield, R.H.; Barrett, J.R.; Kurien, B.T.; Betts, N.; Lyons, T.J.; Zhao, Y.D.; Basu, A. Strawberries Improve Pain and Inflammation in Obese Adults with Radiographic Evidence of Knee Osteoarthritis. Nutrients 2017, 9, 949. [Google Scholar] [CrossRef] [PubMed]
- Guan, V.X.; Mobasheri, A.; Probst, Y.C. A systematic review of osteoarthritis prevention and management with dietary phytochemicals from foods. Maturitas 2019, 122, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Brain, K.; Burrows, T.; Rollo, M.E.; Hayes, C.; Hodson, F.J.; Collins, C.E. Population Characteristics in a Tertiary Pain Service Cohort Experiencing Chronic Non-Cancer Pain: Weight Status, Comorbidities, and Patient Goals. Healthcare 2017, 5, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruggink, L.; Hayes, C.; Lawrence, G.; Brain, K.; Holliday, S. Chronic pain: Overlap and specificity in multimorbidity man-agement. Aust. J. Gen. Pract. 2019, 48, 689–692. [Google Scholar] [CrossRef]
- Minihane, A.M.; Vinoy, S.; Russell, W.R.; Baka, A.; Roche, H.M.; Tuohy, K.M.; Teeling, J.L.; Blaak, E.E.; Fenech, M.; Vauzour, D.; et al. Low-grade inflammation, diet composition and health: Current research evidence and its translation. Br. J. Nutr. 2015, 114, 999–1012. [Google Scholar] [CrossRef] [Green Version]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef]
- Naylor, R.; Hayes, C.; Egger, G. The Relationship Between Lifestyle, Metaflammation, and Chronic Pain: A Systematic Review. Am. J. Lifestyle Med. 2012, 7, 130–137. [Google Scholar] [CrossRef]
- Aghasafari, P.; George, U.; Pidaparti, R. A review of inflammatory mechanism in airway diseases. Inflamm. Res. 2019, 68, 59–74. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, A.S.; Strath, L.J.; Sorge, R.E. Dietary Interventions for Treatment of Chronic Pain: Oxidative Stress and Inflammation. Pain Ther. 2020, 9, 487–498. [Google Scholar] [CrossRef]
- Charles-Messance, H.; Mitchelson, K.A.; Castro, E.D.M.; Sheedy, F.J.; Roche, H.M. Regulating metabolic inflammation by nutritional modulation. J. Allergy Clin. Immunol. 2020, 146, 706–720. [Google Scholar] [CrossRef] [PubMed]
- Potenza, M.A.; Nacci, C.; De Salvia, M.A.; Sgarra, L.; Collino, M.; Montagnani, M. Targeting endothelial metaflammation to counteract diabesity cardiovascular risk: Current and perspective therapeutic options. Pharmacol. Res. 2017, 120, 226–241. [Google Scholar] [CrossRef]
- Donnelly, C.R.; Andriessen, A.S.; Chen, G.; Wang, K.; Jiang, C.; Maixner, W.; Ji, R.-R. Central Nervous System Targets: Glial Cell Mechanisms in Chronic Pain. Neurotherapeutics 2020, 17, 846–860. [Google Scholar] [CrossRef] [PubMed]
- Kaur, N.; Chugh, H.; Sakharkar, M.K.; Dhawan, U.; Chidambaram, S.B.; Chandra, R. Neuroinflammation Mechanisms and Phytotherapeutic Intervention: A Systematic Review. ACS Chem. Neurosci. 2020, 11, 3707–3731. [Google Scholar] [CrossRef]
- Malta, I.; Moraes, T.; Rodrigues, G.; Franco, P.; Galdino, G. The role of oligodendrocytes in chronic pain: Cellular and molecular mechanisms. J. Physiol. Pharmacol. 2019, 70, 70. [Google Scholar]
- Robinson, W.H.; Lepus, C.M.; Wang, Q.; Raghu, H.; Mao, R.; Lindstrom, T.M.; Sokolove, J. Low-grade inflammation as a key mediator of the pathogenesis of osteoarthritis. Nat. Rev. Rheumatol. 2016, 12, 580–592. [Google Scholar] [CrossRef] [PubMed]
- Bjurström, M.F.; Bodelsson, M.; Montgomery, A.; Harsten, A.; Waldén, M.; Janelidze, S.; Hall, S.; Hansson, O.; Irwin, M.R.; Mattsson-Carlgren, N. Differential expression of cerebrospinal fluid neuroinflammatory mediators depending on osteoarthritis pain phenotype. Pain 2020, 161, 2142–2154. [Google Scholar] [CrossRef]
- Barnett, K.; Mercer, S.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Ohayon, M.M.; Stingl, J. Prevalence and comorbidity of chronic pain in the German general population. J. Psychiatr. Res. 2012, 46, 444–450. [Google Scholar] [CrossRef]
- Oliveira, C.B.; Maher, C.G.; Franco, M.R.; Kamper, S.J.; Williams, C.; Silva, F.G.; Pinto, R.Z. Co-occurrence of Chronic Musculoskeletal Pain and Cardiovascular Diseases: A Systematic Review with Meta-analysis. Pain Med. 2019, 21, 1106–1121. [Google Scholar] [CrossRef] [PubMed]
- Pozzobon, D.; Ferreira, P.H.; Dario, A.B.; Almeida, L.; Vesentini, G.; Harmer, A.R.; Ferreira, M.L. Is there an association be-tween diabetes and neck and back pain? A systematic review with meta-analyses. PLoS ONE 2019, 14, e0212030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hitt, H.C.; McMillen, R.C.; Thornton-Neaves, T.; Koch, K.; Cosby, A.G. Comorbidity of obesity and pain in a general popu-lation: Results from the Southern Pain Prevalence Study. J. Pain 2007, 8, 430–436. [Google Scholar] [CrossRef]
- Stone, A.A.; Broderick, J. Obesity and Pain Are Associated in the United States. Obesity 2012, 20, 1491–1495. [Google Scholar] [CrossRef]
- Dean, E.; Hansen, R.G. Prescribing Optimal Nutrition and Physical Activity as “First-Line” Interventions for Best Practice Management of Chronic Low-Grade Inflammation Associated with Osteoarthritis: Evidence Synthesis. Arthritis 2012, 2012, 1–28. [Google Scholar] [CrossRef] [PubMed]
- VanDenKerkhof, E.G.; Macdonald, H.M.; Jones, G.T.; Power, C.; Macfarlane, G. Diet, Lifestyle and Chronic Widespread Pain: Results from the 1958 British Birth Cohort Study. Pain Res. Manag. 2011, 16, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Collins, C.E.; Young, A.F.; Hodge, A. Diet quality is associated with higher nutrient intake and self-rated health in mid-aged women. J. Am. Coll. Nutr. 2008, 27, 146–157. [Google Scholar] [CrossRef]
- Meleger, A.L.; Froude, C.K.; Walker, J., 3rd. Nutrition and eating behavior in patients with chronic pain receiving long-term opioid therapy. PM&R 2014, 6, 7–12.e1. [Google Scholar]
- Brain, K.; Burrows, T.L.; Rollo, M.E.; Hayes, C.; Hodson, F.J.; Collins, C.E. The Effect of a Pilot Dietary Intervention on Pain Outcomes in Patients Attending a Tertiary Pain Service. Nutrients 2019, 11, 181. [Google Scholar] [CrossRef] [Green Version]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013.
- National Health and Medical Research Council. Eat for Health; National Health and Medical Research Council: Canberra, Australia, 2013.
- Wiss, D. A Biopsychosocial Overview of the Opioid Crisis: Considering Nutrition and Gastrointestinal Health. Front. Public Health 2019, 7, 193. [Google Scholar] [CrossRef] [PubMed]
- Bjarnason, I.; Scarpignato, C.; Holmgren, E.; Olszewski, M.; Rainsford, K.D.; Lanas, A. Mechanisms of Damage to the Gas-trointestinal Tract from Nonsteroidal Anti-Inflammatory Drugs. Gastroenterology 2018, 154, 500–514. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Tang, Q.; Hou, H.; Zhang, W.; Li, M.; Chen, D.; Gu, Y.; Wang, B.; Hou, J.; Liu, Y.; et al. Gut Microbiota in NSAID Enteropathy: New Insights from Inside. Front. Cell. Infect. Microbiol. 2021, 11, 572. [Google Scholar] [CrossRef] [PubMed]
- Jahromi, S.R.; Togha, M.; Fesharaki, S.H.; Najafi, M.; Moghadam, N.B.; Kheradmand, J.A.; Kazemi, H.; Gorji, A. Gastrointestinal adverse effects of antiepileptic drugs in intractable epileptic patients. Seizure 2011, 20, 343–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliva, V.; Lippi, M.; Paci, R.; Del Fabro, L.; Delvecchio, G.; Brambilla, P.; De Ronchi, D.; Fanelli, G.; Serretti, A. Gastrointestinal side effects associated with antidepressant treatments in patients with major depressive disorder: A systematic review and meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 109, 110266. [Google Scholar] [CrossRef]
- Camilleri, M.; Drossman, D.A.; Becker, G.; Webster, L.R.; Davies, A.N.; Mawe, G.M. Emerging treatments in neurogastroen-terology: A multidisciplinary working group consensus statement on opioid-induced constipation. Neurogastroenterol. Motil. 2014, 26, 1386–1395. [Google Scholar] [CrossRef] [Green Version]
- Kumar, L.; Barker, C.; Emmanuel, A. Opioid-Induced Constipation: Pathophysiology, Clinical Consequences, and Management. Gastroenterol. Res. Pract. 2014, 2014, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Bannon, S.; Greenberg, J.; Mace, R.A.; Locascio, J.J.; Vranceanu, A.-M. The role of social isolation in physical and emotional outcomes among patients with chronic pain. Gen. Hosp. Psychiatry 2021, 69, 50–54. [Google Scholar] [CrossRef]
- Karayannis, N.V.; Baumann, I.; Sturgeon, J.; Melloh, M.; Mackey, S. The Impact of Social Isolation on Pain Interference: A Longitudinal Study. Ann. Behav. Med. 2019, 53, 65–74. [Google Scholar] [CrossRef] [Green Version]
- Menec, V.H.; Newall, N.E.; Mackenzie, C.S.; Shooshtari, S.; Nowicki, S. Examining social isolation and loneliness in combi-nation in relation to social support and psychological distress using Canadian Longitudinal Study of Aging (CLSA) data. PLoS ONE 2020, 15, e0230673. [Google Scholar] [CrossRef]
- Amy Janke, E.; Kozak, A.T. “The more pain I have, the more I want to eat”: Obesity in the context of chronic pain. Obesity 2012, 20, 2027–2034. [Google Scholar] [CrossRef]
- Gibson-Smith, D.; Bot, M.; Brouwer, I.A.; Visser, M.; Penninx, B.W. Diet quality in persons with and without depressive and anxiety disorders. J. Psychiatr. Res. 2018, 106, 1–7. [Google Scholar] [CrossRef]
- Teasdale, S.B.; Ward, P.; Samaras, K.; Firth, J.; Stubbs, B.; Tripodi, E.; Burrows, T.L. Dietary intake of people with severe mental illness: Systematic review and meta-analysis. Br. J. Psychiatry 2019, 214, 251–259. [Google Scholar] [CrossRef] [Green Version]
- Wirt, A.; Collins, C.E. Diet quality—What is it and does it matter? Public Health Nutr. 2009, 12, 2473–2492. [Google Scholar] [CrossRef] [Green Version]
- Bigand, T.; Wilson, M. Overeating during painful episodes among adults with chronic pain: A preliminary study. Appetite 2019, 137, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Masheb, R.M.; Douglas, M.; Kutz, A.M.; Marsh, A.G.; Driscoll, M. Pain and emotional eating: Further investigation of the Yale Emotional Overeating Questionnaire in weight loss seeking patients. J. Behav. Med. 2020, 43, 479–486. [Google Scholar] [CrossRef]
- Emami, A.S.; Woodcock, A.; Swanson, H.E.; Kapphahn, T.; Pulvers, K. Distress tolerance is linked to unhealthy eating through pain catastrophizing. Appetite 2016, 107, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Agency for Clinical Innovation Pain: Lifestyle and Nutrition. Available online: https://www.aci.health.nsw.gov.au/chronic-pain/for-everyone/pain-lifestyle-and-nutrition (accessed on 19 September 2021).
- Fenton, S.; Burrows, T.L.; Skinner, J.A.; Duncan, M.J. The influence of sleep health on dietary intake: A systematic review and meta-analysis of intervention studies. J. Hum. Nutr. Diet. 2020, 34, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Haack, M.; Simpson, N.; Sethna, N.; Kaur, S.; Mullington, J. Sleep deficiency and chronic pain: Potential underlying mecha-nisms and clinical implications. Neuropsychopharmacology 2020, 45, 205–216. [Google Scholar] [CrossRef]
- Depner, C.M.; Stothard, E.R.; Wright, K.P. Metabolic Consequences of Sleep and Circadian Disorders. Curr. Diabetes Rep. 2014, 14, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, R.L.; Rollo, M.E.; Schumacher, T.; Collins, C.E. Diet Quality Scores of Australian Adults Who Have Completed the Healthy Eating Quiz. Nutrients 2017, 9, 880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philpot, U.; Johnson, M. Diet therapy in the management of chronic pain: Better diet less pain? Pain Manag. 2019, 9, 335–338. [Google Scholar] [CrossRef]
- Towery, P.; Guffey, J.S.; Doerflein, C.; Stroup, K.; Saucedo, S.; Taylor, J. Chronic musculoskeletal pain and function improve with a plant-based diet. Complement. Ther. Med. 2018, 40, 64–69. [Google Scholar] [CrossRef] [PubMed]
- The Joanna Briggs Institute Levels of Evidence and Grades of Recommendation Working Party Joanna Briggs Institute Levels of Evidence and Grades of Recommendation. Available online: https://jbi.global/sites/default/files/2019–05/JBI-Levels-of-evidence_2014_0.pdf (accessed on 19 September 2021).
- Field, R.; Pourkazemi, F.; Turton, J.; Rooney, K. Dietary Interventions Are Beneficial for Patients with Chronic Pain: A Sys-tematic Review with Meta-Analysis. Pain Med. 2021, 22, 694–714. [Google Scholar] [CrossRef]
- Elma, Ö.; Yilmaz, S.T.; Deliens, T.; Coppieters, I.; Clarys, P.; Nijs, J.; Malfliet, A. Do Nutritional Factors Interact with Chronic Musculoskeletal Pain? A Systematic Review. J. Clin. Med. 2020, 9, 702. [Google Scholar] [CrossRef] [Green Version]
- Genel, F.; Kale, M.; Pavlovic, N.; Flood, V.M.; Naylor, J.M.; Adie, S. Health effects of a low-inflammatory diet in adults with arthritis: A systematic review and meta-analysis. J. Nutr. Sci. 2020, 9, 37. [Google Scholar] [CrossRef]
- Brain, K.; Burrows, T.L.; Rollo, M.E.; Chai, L.K.; Clarke, E.D.; Hayes, C.; Hodson, F.J.; Collins, C.E. A systematic review and meta-analysis of nutrition interventions for chronic noncancer pain. J. Hum. Nutr. Diet. 2018, 32, 198–225. [Google Scholar] [CrossRef]
- Silva, A.R.; Bernardo, A.; Costa, J.; Cardoso, A.; Santos, P.; De Mesquita, M.F.; Patto, J.V.; Moreira, P.; Silva, M.L.; Padrão, P. Dietary interventions in fibromyalgia: A systematic review. Ann. Med. 2019, 51 (Suppl. 1), 2–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dragan, S.; Șerban, M.C.; Damian, G.; Buleu, F.; Valcovici, M.; Christodorescu, R. Dietary Patterns and Interventions to Al-leviate Chronic Pain. Nutrients 2020, 12, 2510. [Google Scholar] [CrossRef]
- Rondanelli, M.; Faliva, M.A.; Miccono, A.; Naso, M.; Nichetti, M.; Riva, A.; Guerriero, F.; De Gregori, M.; Peroni, G.; Perna, S. Food pyramid for subjects with chronic pain: Foods and dietary constituents as anti-inflammatory and antioxidant agents. Nutr. Res. Rev. 2018, 31, 131–151. [Google Scholar] [CrossRef]
- Brain, K.; Burrows, T.L.; Rollo, M.; Collins, C. Nutrition and Chronic Pain. Available online: https://www.iasp-pain.org/resources/fact-sheets/nutrition-and-chronic-pain/ (accessed on 19 September 2021).
- Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [CrossRef] [Green Version]
- Krebs-Smith, S.M.; Guenther, P.M.; Subar, A.F.; Kirkpatrick, S.I.; Dodd, K.W. Americans do not meet federal dietary recom-mendations. J. Nutr. 2010, 140, 1832–1838. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare (AIHW). Diet; AIHW: Canberra, Australia, 2020.
- Elizabeth, L.; Machado, P.; Zinöcker, M.; Baker, P.; Lawrence, M. Ultra-Processed Foods and Health Outcomes: A Narrative Review. Nutrients 2020, 12, 1955. [Google Scholar] [CrossRef]
- World Health Organisation Guideline: Sugar Intake for Adults and Children; World Health Organisation: Geneva, Switzerland, 2015.
- Van Dam, R.M.; Hu, F.B.; Willett, W.C. Coffee, Caffeine, and Health. N. Engl. J. Med. 2020, 383, 369–378. [Google Scholar] [CrossRef]
- Witkiewitz, K.; Vowles, K.E. Alcohol and Opioid Use, Co-Use, and Chronic Pain in the Context of the Opioid Epidemic: A Critical Review. Alcohol. Clin. Exp. Res. 2018, 42, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Roehrs, T.; Roth, T. Sleep, Sleepiness, and Alcohol Use. Alcohol Res. Health 2001, 25, 101–109. [Google Scholar] [PubMed]
- Marouf, B.H.; Hussain, S.A.; Ali, Z.S.; Ahmmad, R.S. Resveratrol Supplementation Reduces Pain and Inflammation in Knee Osteoarthritis Patients Treated with Meloxicam: A Randomized Placebo-Controlled Study. J Med Food 2018, 21, 1253–1259. [Google Scholar] [CrossRef]
- Commonwealth of Australia. Australian Guidelines to Reduce Health Risks from Drinking Alcohol; National Health and Medical Research Council: Canberra, Australia, 2020.
- Schumacher, T.; Burrows, T.L.; Rollo, M.; Collins, C. Pain and nutrition. In Pain in Residental Aged Care Guidelines, 2nd ed.; Gouke, R., Ed.; Australian Pain Society: Sydney, Australia, 2018; pp. 125–134. [Google Scholar]
- Carbone, J.W.; Pasiakos, S.M. Dietary Protein and Muscle Mass: Translating Science to Application and Health Benefit. Nutrients 2019, 11, 1136. [Google Scholar] [CrossRef] [Green Version]
- National Health and Medical Research Council; New Zealand Ministry of Health. Nutrient Reference Values for Australia and New Zealand; National Health and Medical Research Council: Canberra, Australia, 2006.
- Loenneke, J.P.; Loprinzi, P.D.; Murphy, C.H.; Phillips, S.M. Per meal dose and frequency of protein consumption is associated with lean mass and muscle performance. Clin Nutr 2016, 35, 1506–1511. [Google Scholar] [CrossRef] [PubMed]
- Brady, B.; Veljanova, I.; Chipchase, L. Are multidisciplinary interventions multicultural? A topical review of the pain literature as it relates to culturally diverse patient groups. Pain 2016, 157, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.T.; Allman-Farinelli, M.; Chen, J.; Partridge, S.R.; Collins, C.; Rollo, M.; Haslam, R.; Diversi, T.; Campbell, K.L. Dietitians Australia position statement on telehealth. Nutr. Diet 2020, 77, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Senftleber, N.K.; Nielsen, S.M.; Andersen, J.R.; Bliddal, H.; Tarp, S.; Lauritzen, L.; Furst, D.E.; Suarez-Almazor, M.E.; Lyddiatt, A.; Christensen, R. Marine Oil Supplements for Arthritis Pain: A Systematic Review and Meta-Analysis of Randomized Trials. Nutrients 2017, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Brady, B.; Veljanova, I.; Schabrun, S.; Chipchase, L. Integrating culturally informed approaches into physiotherapy assessment and treatment of chronic pain: A pilot randomised controlled trial. BMJ Open 2018, 8, 021999. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Experimental Study Designs | Level of Evidence [81] | Study Type | Target Population | Intervention(s) | Length of Intervention | Risk of Bias (ROB)/Methodological Quality | Results | Evidence Gaps |
| Field et al., 2021 [82] | 1b | SR and MA (exp); n = 43 | Chronic non-cancer MSK pain | Veg/vegan (n = 11), single food changes (n = 11), elimination (n-11), energy or macronutrient restriction (n = 8), omega-3 (n = 5), Mediterranean diet (n = 2) | Ave 18 weeks (2 weeks–2 years) | RCT’s and pre-post studies: Good (n = 7), fair (n = 19), poor (n = 11) | N= 23/32 controlled studies included in MA. SMD −0.44; 95% CI: −0.63 to −0.24; p < 0.0001; I2 = 62% (high heterogeneity) | Poor methodological quality, heterogeneity, most common pain measure unidimensional |
| Elma et al., 2020 [83] | 1b | SR (exp and obs); n = 12 | Chronic MSK pain | Exp studies: Veg/vegan (n = 4), weight loss (n = 2), peptide diet (n = 1), aspartame elimination (n = 1), low FODMAP (n = 1) | Exp studies: Ave 16 weeks (4 weeks–1 year) | RCT’s: Good (n = 1), fair (n = 1), poor (n = 3) | 7/9 exp studies reported pain relieving effect of dietary changes. Two studies reported no effect (aspartame elimination and vegetarian). | Poor methodological quality, heterogeneity, most common pain measure unidimensional |
| Genel et al., 2020 [84] | 1b | SR and MA (exp); n = 7 | Arthritis | Mediterranean diet (n = 4), anti-inflammatory food (n = 2), low inflammatory diet (n = 1) | Ave 17 weeks (12–24 weeks) | RCTs: low ROB (n = 1), high ROB (n = 4), non RCTs: moderate risk (n = 1), serious risk (n = 1) | Overall no significant change in pain. Subgroup analysis for RA had reduction, SMD −2.81 (95 % CI −3.60, −2.02), p <0.00001 | Small sample size, poor methodological quality, heterogeneity |
| Brain et al., 2019 [85] | 1b | SR and MA (exp); n = 71 | CNCP | Altered overall diet (n = 16), altered specific nutrient (n = 5), supplement-based (n = 46), fasting (n = 4) | Ave 17 weeks (2 to 2 years) | Positive (n =3 1), neutral (n = 36), negative (n = 4) | MA (n = 23): −0.905 (95% CI −0.537 to −1.272), p < 0.001 Qual synthesis: 12/16, 2/5, 11/46 and 1/4 studies from each respective group had significant reduction in pain | Poor methodological quality, small sample size, heterogeneity, most common pain measure unidimensional |
| Silva et al., 2019 [86] | 1b | SR (exp); n = 7 | Fibromyalgia | Weight loss (n = 2), vegetarian (n = 2), low FODMAP (n = 1), gluten free (n = 1), MSG and aspartame free diet (n = 1) | Ave 18 weeks (4 weeks to 6 months) | All very low or low uncertainty of evidence, except n = 1 moderate | All but 2 studies (gluten free and MSG/aspartame free diet) had significant reduction in pain | Poor methodological quality, small sample size |
| Brain et al., 2019 [53] | 1c | Pilot RCT (n = 60) | CNCP | Personalised dietary assessment, education (i.e., F&V, good quality fats, antioxidants and micronutrients and fibre) and advice using the Behaviour Change Wheel and provided by a dietitian +/− antioxidant supplement | 6 weeks | N/A | All groups had statastically signigicant improvement in pain interference, pain self-efficacy and pain catastrophizing. Personalised dietary support groups had clinically meaningful improvement in pain interference and pain self-efficacy | Small sample size, loss to follow up (30%), placebo effect |
| Dragan et al., 2020 [87] | 2b | Literature Review (exp); n = 38 | CNCP | Antioxidant, vitamin and minerals (n = 9), elimination diet (n = 7), energy restriction (n = 5), low-fat/plant based (n = 5), pre and probiotics (n = 5), fruit and fibre (n = 4), enriched PUFA (n = 2), high protein (n = 1) | Ave 15 weeks (4 weeks–1.5 years) | Not reported | Antioxidants, vitamins and minerals: 8 improvement in pain (IP), 1 no difference (ND) Elimination: 4 IP, 3 ND Energy restriction: 5 IP Low fat/plant based: 5 IP Pre/probiotics: 3 IP, 2 ND Fruit/fibre: 4 IP Enriched PUFA: 2 IP High protein: 1 IP (Note IP included a variety of measures e.g., severity or frequency and strength of improvements ranged from trends to significant improvements) | Small sample size, poor methodological quality |
| Kaushik et al., 2020 [35] | 2b | Literature review (n = 8) | CNCP | Antioxidant (n = 3), Mediterranean diet (n = 2), low carbohydrate (n = 2), saturated fat (n = 1) | Ave 17 weeks (1 day–1 year) | Not reported | Summary of oxidative stress and inflammation provided. Low carbohydrate, 2/3 antioxidant and Mediterranean diet had reduction in oxidative stress and inflammation. 1 antioxidant study showed no change and saturated fat showed increase in oxidative stress and inflammation | Small number of clinical studies, only 2 studies were specifically measured pain, hard to compare dietary studies when variety of interventions |
| Rondanelli et al., 2018 [88] | 2b | Narrative review (n = 172) | CNCP | Red wine (n = 26), olive oil (n = 24), zinc and selenium (n = 18), oil seeds (n = 14), yoghurt (n = 11), F&V (n = 10), spices (n = 8), vitamin D (n = 7), fibre in opioid induced constipation (n = 7), cheese (n = 7), legumes (n = 6), sweets (n = 6), omega-3 (n = 6), meat and fish (n = 5), eggs (n = 4), vitamin B12 (n = 3), water (n = 3), fibre (n = 2) | Not reported | Level of evidence: n = 1 SR, n = 6 RCT or obs study with dramatic effect, n = 7 non-RCT, cohort/follow-up studies, n = 3 case series, case-control or historically controlled studies, n = 149 mechanism based reasoning | A food pyramid was developed and presented as the results of the paper. This divided foods into those that should be consumed daily, consumed 1, 2, or 4 times per week and foods to be eaten occasionally. | Combination of human, in vitro and animal models included, reliance on lower levels of evidence, casual relationships unknown |
| Towery et al., 2018 [80] | 2d | Quasi-exp cohort study (n = 14) | Chronic MSK pain | Education on plant based diet and sample menu cycle. Included grains, F&V, legumes, dairy products and eggs. Meat, poultry, seafood and fish not allowed and processed foods and drinks discouraged | 8 weeks | N/A | Pain: mean change 3.14 on NPRS (95% CI 2.16–4.12), p = 0.0001. Quality of life: mean change 24.991 on SF-36 (95% CI 18.16–31.97), p = 0.0001 | Small sample (although powered), unable to blind, accuracy of reported intake, convenience sample, self-reported food intake can increase motivation to change eating habits |
| Expert Consensus Papers | Level of Evidence | Study Type | Population | Summary | Evidence Gaps | |||
| Brain et al., 2020 [89] | 5b | Expert opinion factsheet | CNCP |
| N/A | |||
| Nijs J et al., 2020 [19] | 5b | Expert opinion review | CNCP (animal and human studies) |
| Need to explore interactions in human studies | |||
| Philpot et al., 2019 [79] | 5b | Expert opinion editorial | CNCP |
| Lack of research on the efficacy of diet therapy for people with CNCP and on the barriers to implementing diet therapy into clinical practice. | |||
| Bjørklund. 2019 [22] | 5b | Expert opinion review | CNCP |
| More research on the best dietary program for CNCP is needed | |||
| Monitor Signs for Malnutrition and Risk of Malnutrition | Monitor Signs for Reduced Fluid Intake and Risk of Dehydration | Stimulate Appetite | Increase Fluid Intake | Improve Eating Experience | Reduce Constipation |
|---|---|---|---|---|---|
|
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brain, K.; Burrows, T.L.; Bruggink, L.; Malfliet, A.; Hayes, C.; Hodson, F.J.; Collins, C.E. Diet and Chronic Non-Cancer Pain: The State of the Art and Future Directions. J. Clin. Med. 2021, 10, 5203. https://doi.org/10.3390/jcm10215203
Brain K, Burrows TL, Bruggink L, Malfliet A, Hayes C, Hodson FJ, Collins CE. Diet and Chronic Non-Cancer Pain: The State of the Art and Future Directions. Journal of Clinical Medicine. 2021; 10(21):5203. https://doi.org/10.3390/jcm10215203
Chicago/Turabian StyleBrain, Katherine, Tracy L. Burrows, Laura Bruggink, Anneleen Malfliet, Chris Hayes, Fiona J. Hodson, and Clare E. Collins. 2021. "Diet and Chronic Non-Cancer Pain: The State of the Art and Future Directions" Journal of Clinical Medicine 10, no. 21: 5203. https://doi.org/10.3390/jcm10215203