
Relationship between Adipokines and Cardiovascular Ultrasound Parameters in Metabolic-Dysfunction-Associated Fatty Liver Disease

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
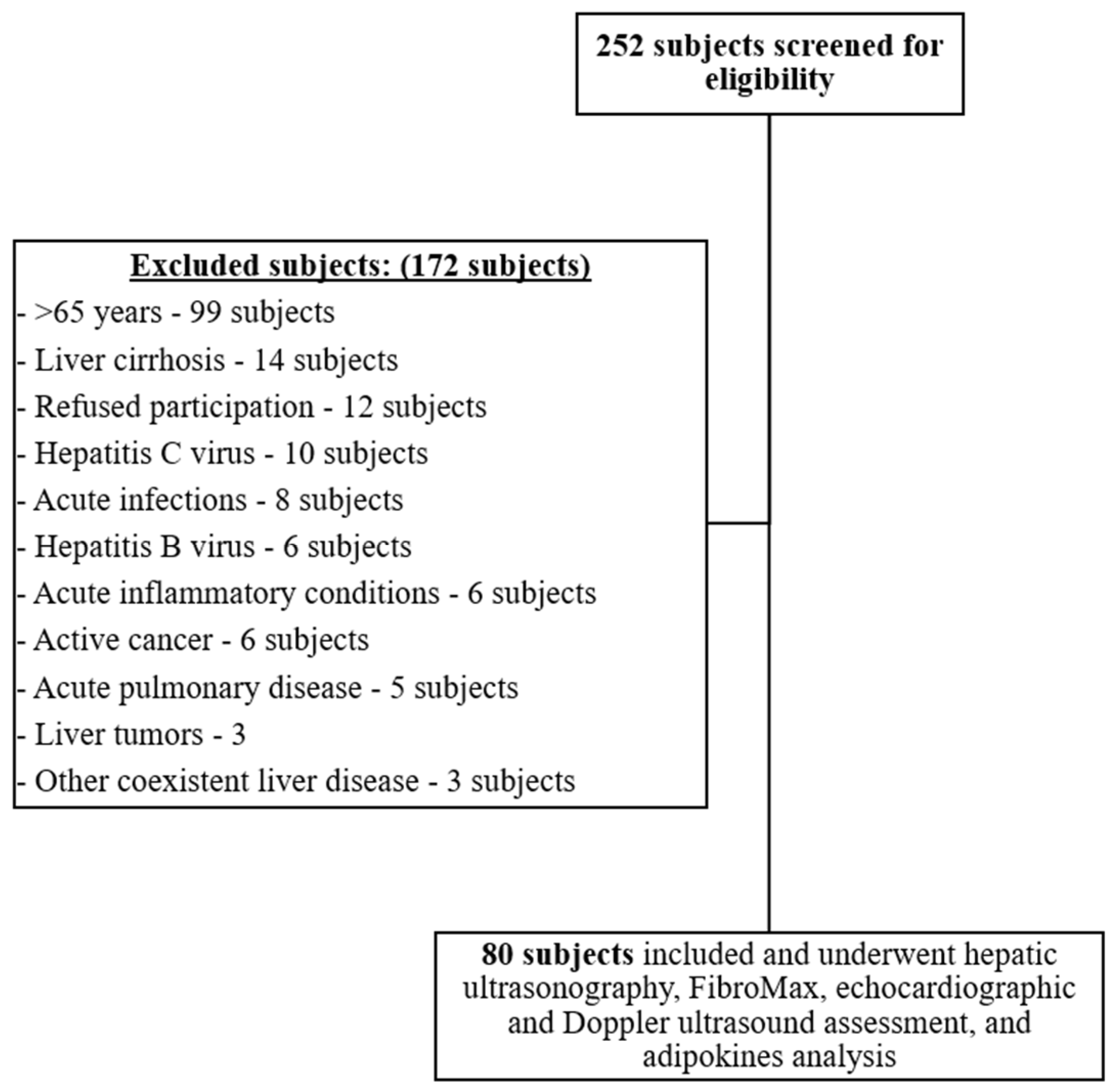
2.1. Study Participants and Setting
2.2. General Definitions
2.3. Hepatic Ultrasonography
2.4. Echocardiography
2.5. Laboratory Analysis
2.5.1. Adipokines
2.5.2. FibroMax
2.6. Statistical Analysis
3. Results
3.1. General Characteristics and Laboratory Results
3.2. Hepatic Steatosis and Fibrosis Evaluation
3.3. Adipokine Levels
3.4. Cardiovascular Assessment
3.5. Adipokines and Cardiovascular Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dumitrascu, D.L.; Neuman, M.G. Non-alcoholic fatty liver disease: An update on diagnosis. Clujul Med. 2018, 91, 147–150. [Google Scholar] [CrossRef] [Green Version]
- Sporea, I.; Popescu, A.; Dumitrașcu, D.; Brisc, C.; Nedelcu, L.; Trifan, A.; Gheorghe, L.; Braticevici, C.F. Nonalcoholic Fatty Liver Disease: Status Quo. J. Gastrointest. Liver Dis. 2018, 27, 439–448. [Google Scholar] [CrossRef]
- Mantovani, A.; Scorletti, E.; Mosca, A.; Alisi, A.; Byrne, C.D.; Targher, G. Complications, morbidity and mortality of nonalcoholic fatty liver disease. Metabolism 2020, 111, 154170. [Google Scholar] [CrossRef] [PubMed]
- Francque, S.M.; van der Graaff, D.; Kwanten, W. Non-alcoholic fatty liver disease and cardiovascular risk: Pathophysiological mechanisms and implications. J. Hepatol. 2016, 65, 425–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirza, M.S. Obesity, Visceral Fat, and NAFLD: Querying the Role of Adipokines in the Progression of Nonalcoholic Fatty Liver Disease. ISRN Gastroenterol. 2011, 2011, 592404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ando, Y.; Jou, J.H. Nonalcoholic Fatty Liver Disease and Recent Guideline Updates. Clin. Liver Dis. 2021, 17, 23–28. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wong, V.W.-S.; Dufour, J.-F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Eslam, M.; Sanyal, A.J.; George, J.; Neuschwander-Tetri, B.; Tiribelli, C.; Kleiner, D.E.; Brunt, E.; Bugianesi, E.; Yki-Järvinen, H.; Grønbæk, H.; et al. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014. [Google Scholar] [CrossRef]
- Wong, C.; Lim, J.K. The Association Between Nonalcoholic Fatty Liver Disease and Cardiovascular Disease Outcomes. Clin. Liver Dis. 2018, 12, 39–44. [Google Scholar] [CrossRef]
- Targher, G.; Marra, F.; Marchesini, G. Increased risk of cardiovascular disease in non-alcoholic fatty liver disease: Causal effect or epiphenomenon? Diabetologia 2008, 51, 1947–1953. [Google Scholar] [CrossRef] [Green Version]
- Ismaiel, A.; Dumitraşcu, D.L. Cardiovascular Risk in Fatty Liver Disease: The Liver-Heart Axis—Literature Review. Front. Med. 2019, 6, 202. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; Konyn, P.; Sandhu, K.K.; Dennis, B.B.; Cheung, A.C.; Ahmed, A. Metabolic dysfunction-associated fatty liver disease is associated with increased all-cause mortality in the United States. J. Hepatol. 2021. [Google Scholar] [CrossRef]
- Lee, H.; Lee, Y.-H.; Kim, S.U.; Kim, H.C. Metabolic Dysfunction-Associated Fatty Liver Disease and Incident Cardiovascular Disease Risk: A Nationwide Cohort Study. Clin. Gastroenterol. Hepatol. 2021, 19, 2138–2147.e10. [Google Scholar] [CrossRef] [PubMed]
- Funcke, J.-B.; Scherer, P.E. Beyond adiponectin and leptin: Adipose tissue-derived mediators of inter-organ communication. J. Lipid Res. 2019, 60, 1648–1697. [Google Scholar] [CrossRef] [PubMed]
- Achari, A.E.; Jain, S.K. Adiponectin, a Therapeutic Target for Obesity, Diabetes, and Endothelial Dysfunction. Int. J. Mol. Sci. 2017, 18, 1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polyzos, S.A.; Toulis, K.A.; Goulis, D.G.; Zavos, C.; Kountouras, J. Serum total adiponectin in nonalcoholic fatty liver disease: A systematic review and meta-analysis. Metabolism 2011, 60, 313–326. [Google Scholar] [CrossRef]
- Samal, B.; Sun, Y.; Stearns, G.; Xie, C.; Suggs, S.; Mcniece, I. Cloning and characterization of the cDNA encoding a novel human pre-B-cell colony-enhancing factor. Mol. Cell. Biol. 1994, 14, 1431–1437. [Google Scholar] [CrossRef]
- Wang, T.; Zhang, X.; Bheda, P.; Revollo, J.R.; Imai, S.-I.; Wolberger, C. Structure of Nampt/PBEF/visfatin, a mammalian NAD+ biosynthetic enzyme. Nat. Struct. Mol. Biol. 2006, 13, 661–662. [Google Scholar] [CrossRef]
- Revollo, J.R.; Grimm, A.A.; Imai, S.-I. The NAD Biosynthesis Pathway Mediated by Nicotinamide Phosphoribosyltransferase Regulates Sir2 Activity in Mammalian Cells. J. Biol. Chem. 2004, 279, 50754–50763. [Google Scholar] [CrossRef] [Green Version]
- Adolph, T.E.; Grander, C.; Grabherr, F.; Tilg, H. Adipokines and Non-Alcoholic Fatty Liver Disease: Multiple Interactions. Int. J. Mol. Sci. 2017, 18, 1649. [Google Scholar] [CrossRef] [Green Version]
- Ismaiel, A.; Leucuta, D.-C.; Popa, S.-L.; Dumitrascu, D. Serum Visfatin Levels in Nonalcoholic Fatty Liver Disease and Liver Fibrosis: Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3029. [Google Scholar] [CrossRef] [PubMed]
- Duman, H.; Özyıldız, A.G.; Bahçeci, I.; Duman, H.; Uslu, A.; Ergül, E. Serum visfatin level is associated with complexity of coronary artery disease in patients with stable angina pectoris. Ther. Adv. Cardiovasc. Dis. 2019, 13, 1753944719880448. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.-Y.; Xu, X.; Wan, R.-H.; Xia, S.; Lu, J.; Huang, Q. Association between serum visfatin levels and atherosclerotic plaque in patients with type 2 diabetes. Diabetol. Metab. Syndr. 2019, 11, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hognogi, L.D.M.; Simiti, L.V. The cardiovascular impact of visfatin—An inflammation predictor biomarker in metabolic syndrome. Clujul Med. 2016, 89, 322–326. [Google Scholar] [CrossRef]
- Romacho, T.; Sánchez-Ferrer, C.F.; Peiro, C. Visfatin/Nampt: An Adipokine with Cardiovascular Impact. Mediat. Inflamm. 2013, 2013, 946427. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Day, C.P.; Bonora, E. Risk of Cardiovascular Disease in Patients with Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2010, 363, 1341–1350. [Google Scholar] [CrossRef] [Green Version]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62 (Suppl. 1), S47–S64. [Google Scholar] [CrossRef] [Green Version]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2020, 44 (Suppl. 1), S15–S33. [Google Scholar] [CrossRef]
- Grundy, S.M. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar]
- Pan, J.-J.; Fisher-Hoch, S.P.; Chen, C.; Feldstein, A.E.; McCormick, J.B.; Rahbar, M.H.; Beretta, L.; Fallon, M.B. Burden of nonalcoholic fatty liver disease and advanced fibrosis in a Texas Hispanic community cohort. World J. Hepatol. 2015, 7, 1586–1594. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.; Roman, M.J.; Seward, J.B.; Shanewise, J.S. Recommendations for chamber quantification. Eur. J. Echocardiogr. 2006, 7, 79–108. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsen, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L. Recommendations for the echocardiographic assessment of native valvular regurgitation: An executive summary from the European Association of Cardiovascular Imaging. Eur. Hear. J. Cardiovasc. Imaging 2013, 14, 611–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [Green Version]
- Vijayaraghavan, G.; Sivasankaran, S. Global longitudinal strain: A practical step-by-step approach to longitudinal strain imaging. J. Indian Acad. Echocardiogr. Cardiovasc. Imaging 2020, 4, 22. [Google Scholar] [CrossRef]
- Muraru, D.; Cucchini, U.; Mihăilă, S.; Miglioranza, M.H.; Aruta, P.; Cavalli, G.; Cecchetto, A.; Padayattil-Josè, S.; Peluso, D.; Iliceto, S.; et al. Left Ventricular Myocardial Strain by Three-Dimensional Speckle-Tracking Echocardiography in Healthy Subjects: Reference Values and Analysis of Their Physiologic and Technical Determinants. J. Am. Soc. Echocardiogr. 2014, 27, 858–871.e1. [Google Scholar] [CrossRef]
- Reisner, S.A.; Lysyansky, P.; Agmon, Y.; Mutlak, D.; Lessick, J.; Friedman, Z. Global longitudinal strain: A novel index of left ventricular systolic function. J. Am. Soc. Echocardiogr. 2004, 17, 630–633. [Google Scholar] [CrossRef] [Green Version]
- Lupsor-Platon, M.; Stefanescu, H.; Muresan, D.; Florea, M.; Szasz, M.E.; Maniu, A.; Badea, R. Noninvasive assessment of liver ste-atosis using ultrasound methods. Med. Ultrason. 2014, 16, 236–245. [Google Scholar]
- Joy, D.; Thava, V.R.; Scott, B.B. Diagnosis of fatty liver disease: Is biopsy necessary? Eur. J. Gastroenterol. Hepatol. 2003, 15, 539–543. [Google Scholar] [CrossRef]
- Poynard, T.; Ratziu, V.; Naveau, S.; Thabut, D.; Charlotte, F.; Messous, D.; Capron, D.; Abella, A.; Massard, J.; Ngo, Y.; et al. The diagnostic value of biomarkers (SteatoTest) for the prediction of liver steatosis. Comp. Hepatol. 2005, 4, 10. [Google Scholar] [CrossRef] [Green Version]
- Lassailly, G.; Caiazzo, R.; Hollebecque, A.; Buob, D.; Leteurtre, E.; Arnalsteen, L.; Louvet, A.; Pigeyre, M.; Raverdy, V.; Verkindt, H.; et al. Validation of noninvasive biomarkers (FibroTest, SteatoTest, and NashTest) for prediction of liver injury in patients with morbid obesity. Eur. J. Gastroenterol. Hepatol. 2011, 23, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Bonci, E.; Chiesa, C.; Versacci, P.; Anania, C.; Silvestri, L.; Pacifico, L. Association of Nonalcoholic Fatty Liver Disease with Subclinical Cardiovascular Changes: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2015, 2015, 213737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijarnpreecha, K.; Lou, S.; Panjawatanan, P.; Cheungpasitporn, W.; Pungpapong, S.; Lukens, F.J.; Ungprasert, P. Association between diastolic cardiac dysfunction and nonalcoholic fatty liver disease: A systematic review and meta-analysis. Dig. Liver Dis. 2018, 50, 1166–1175. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Huang, J.; Wang, M.; Kumar, R.; Liu, Y.; Liu, S.; Wu, Y.; Wang, X.; Zhu, Y. Comparison of MAFLD and NAFLD diagnostic criteria in real world. Liver Int. 2020, 40, 2082–2089. [Google Scholar] [CrossRef]
- Kitzman, D.W. Normal Age-Related Changes in the Heart: Relevance to Echocardiography in the Elderly. Am. J. Geriatr. Cardiol. 2000, 9, 311–320. [Google Scholar] [CrossRef]
- Singh, M.; Sethi, A.; Mishra, A.K.; Subrayappa, N.K.; Stapleton, D.D.; Pellikka, P.A. Echocardiographic Imaging Challenges in Obesity: Guideline Recommendations and Limitations of Adjusting to Body Size. J. Am. Heart Assoc. 2020, 9, e014609. [Google Scholar] [CrossRef]
- Norvik, J.V.; Schirmer, H.; Ytrehus, K.; Jenssen, T.G.; Zykova, S.N.; Eggen, A.E.; Eriksen, B.O.; Solbu, M.D. Low adiponectin is associated with diastolic dysfunction in women: A cross-sectional study from the Tromsø Study. BMC Cardiovasc. Disord. 2017, 17, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puchałowicz, K.; Kłoda, K.; Dziedziejko, V.; Rać, M.; Wojtarowicz, A.; Chlubek, D.; Safranow, K. Association of Adiponectin, Leptin and Resistin Plasma Concentrations with Echocardiographic Parameters in Patients with Coronary Artery Disease. Diagnostics 2021, 11, 1774. [Google Scholar] [CrossRef]
- Francisco, C.; Neves, J.S.; Falcão-Pires, I.; Leite-Moreira, A. Can Adiponectin Help us to Target Diastolic Dysfunction? Cardiovasc. Drugs Ther. 2016, 30, 635–644. [Google Scholar] [CrossRef]
- Engeli, S.; Feldpausch, M.; Gorzelniak, K.; Hartwig, F.; Heintze, U.; Janke, J.; Möhlig, M.; Pfeiffer, A.F.; Luft, F.C.; Sharma, A.M. Association Between Adiponectin and Mediators of Inflammation in Obese Women. Diabetes 2003, 52, 942–947. [Google Scholar] [CrossRef] [Green Version]
- Akoumianakis, I.; Antoniades, C. The interplay between adipose tissue and the cardiovascular system: Is fat always bad? Cardiovasc. Res. 2017, 113, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Oh, A.; Okazaki, R.; Sam, F.; Valero-Munoz, M. Heart Failure With Preserved Ejection Fraction and Adipose Tissue: A Story of Two Tales. Front. Cardiovasc. Med. 2019, 6, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tengiz, I.; Turk, U.O.; Alioglu, E.; Kirilmaz, B.; Tamer, G.S.; Tuzun, N.; Ercan, E. The relationship between adiponectin, NT-pro-BNP and left ventricular ejection fraction in non-cachectic patients with systolic heart failure: An observational study. Anadolu Kardiyol. Dergisi/Anatol. J. Cardiol. 2013, 13, 221–226. [Google Scholar] [CrossRef]
- Oztürk, M.; Dursunoğlu, D.; Göksoy, H.; Rota, S.; Gür, S. Evaluation of serum adiponectin levels in patients with heart failure and relationship with functional capacity. Turk Kardiyol. Dern. Ars. Turk Kardiyol. Dern. Yayin Organidir 2009, 37, 384–390. [Google Scholar]
- Frankel, D.S.; Vasan, R.S.; D’Agostino, R.B.; Benjamin, E.; Levy, D.; Wang, T.; Meigs, J.B. Resistin, Adiponectin, and Risk of Heart Failure: The Framingham Offspring Study. J. Am. Coll. Cardiol. 2009, 53, 754–762. [Google Scholar] [CrossRef] [Green Version]
- Kistorp, C.; Faber, J.; Galatius, S.; Gustafsson, F.; Frystyk, J.; Flyvbjerg, A.; Hildebrandt, P. Plasma Adiponectin, Body Mass Index, and Mortality in Patients With Chronic Heart Failure. Circulation 2005, 112, 1756–1762. [Google Scholar] [CrossRef] [Green Version]
- George, J.; Patal, S.; Wexler, D.; Sharabi, Y.; Peleg, E.; Kamari, Y.; Grossman, E.; Sheps, D.; Keren, G.; Roth, A. Circulating adiponectin concentrations in patients with congestive heart failure. Heart 2006, 92, 1420–1424. [Google Scholar] [CrossRef] [Green Version]
- Tamura, T.; Furukawa, Y.; Taniguchi, R.; Sato, Y.; Ono, K.; Horiuchi, H.; Nakagawa, Y.; Kita, T.; Kimura, T. Serum Adiponectin Level as an Independent Predictor of Mortality in Patients With Congestive Heart Failure. Circ. J. 2007, 71, 623–630. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, K.; Wilson, R.M.; Essick, E.E.; Duffen, J.L.; Scherer, P.E.; Ouchi, N.; Sam, F. Effects of Adiponectin on Calcium-Handling Proteins in Heart Failure With Preserved Ejection Fraction. Circ. Heart Fail. 2014, 7, 976–985. [Google Scholar] [CrossRef] [Green Version]
- Zheng, M.; Lu, N.; Ren, M.; Chen, H. Visfatin associated with major adverse cardiovascular events in patients with acute myocardial infarction. BMC Cardiovasc. Disord. 2020, 20, 271. [Google Scholar] [CrossRef] [PubMed]
- Ismaiel, A.; Popa, S.-L.; Dumitrascu, D.L. Acute Coronary Syndromes and Nonalcoholic Fatty Liver Disease: “Un Affaire de Coeur”. Can. J. Gastroenterol. Hepatol. 2020, 2020, 8825615. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Total (n = 80) | Control (n = 40) | MAFLD (n = 40) | p-Value |
|---|---|---|---|---|
| Age (years), median (IQR) | 46 (30–57) | 30 (27–42) | 53.5 (48.75–59) | <0.001 |
| Gender (male), n (%) | 36/80 (45) | 22 (55) | 22 (55) | 1 |
| BMI, median (IQR) | 26.4 (22.32–31.24) | 22.29 (20.17–24.89) | 30.78 (28.1–34.7) | <0.001 |
| Waist circumference (cm), median (IQR) | 96.5 (81.75–105.25) | 82.5 (72–91.5) | 104.5 (100–111) | <0.001 |
| Metabolic syndrome, n (%) | 33/80 (41.25) | 2 (5) | 31 (77.5) | <0.001 |
| Diabetic, n (%) | 16/80 (20) | 0 (0) | 16 (40) | <0.001 |
| Impaired fasting glucose, n (%) | 5/80 (6.25) | 2 (5) | 3 (7.5) | 1 |
| Hypertensive, n (%) | 39/80 (48.75) | 7 (17.5) | 32 (80) | <0.001 |
| SBP-mean (mmHg), median (IQR) | 124.5 (116.38–137.25) | 120.75 (112.5–126) | 132.75 (122.38–147.88) | <0.001 |
| DBP-mean (mmHg), median (IQR) | 79 (74–84) | 75.75 (71.25–79.12) | 83 (78.38–89) | <0.001 |
| MAP-mean (mmHg), median (IQR) | 93.92 (89–101.88) | 90.67 (84.42–94) | 98.92 (92.79–108.62) | <0.001 |
| Pulse pressure-mean (mmHg), median (IQR) | 45.5 (41.38–52) | 44.75 (40–49) | 49.25 (42.38–58.5) | 0.023 |
| Pulse-mean (bpm), median (IQR) | 77.5 (70.88–84.5) | 79.5 (73.38–83.75) | 76.75 (68–84.5) | 0.366 |
| Smoking history, n (%) | 0.963 | |||
| Smoker: | 16/80 (20) | 8 (20) | 8 (20) | |
| Never smoked: | 45/80 (56.25) | 22 (55) | 23 (57.5) | |
| Ex-smoker: | 19/80 (23.75) | 10 (25) | 9 (22.5) | |
| LDL (mg/dL), median (IQR) | 118 (90.5–158.5) | 112.5 (84–140.75) | 127 (99.75–166) | 0.083 |
| HDL (mg/dL), median (IQR) | 48 (42.75–59.25) | 54.5 (46.75–63) | 44 (37.75–49.75) | <0.001 |
| Triglycerides (mg/dL), median (IQR) | 112 (79.5–154) | 82.5 (69–103.5) | 147.5 (115–184.5) | <0.001 |
| Total cholesterol (mg/dL), median (IQR) | 187.5 (151.75–219.25) | 184 (152–215.25) | 196 (146–230.25) | 0.441 |
| Fasting blood sugar (FBS) (mg/dL), median (IQR) | 91 (86–100.25) | 87 (82.75–91.25) | 98 (89.5–123.75) | <0.001 |
| Adiponectin (μg/mL), mean (SD) | 10.92 (1.92) | 11.28 (1.57) | 10.56 (2.18) | 0.097 |
| Visfatin (ng/L), median (IQR) | 16.91 (11.46–23.25) | 14.94 (10.6–22.27) | 18.18 (12.74–23.72) | 0.26 |
| Characteristic | Total (n = 80) | Control (n = 40) | MAFLD (n = 40) | p-Value |
|---|---|---|---|---|
| CIMT-right (mm), median (IQR) | 9 (7–10) | 7 (6–9) | 9.5 (8–11) | <0.001 |
| CIMT-left (mm), median (IQR) | 8.5 (7–10) | 7 (6–8.25) | 10 (8.75–11) | <0.001 |
| CIMT-mean (mm), median (IQR) | 8.5 (7–10) | 7.25 (6.5–8.62) | 9.75 (8.5–11) | <0.001 |
| Left atrial diameter (mm), median (IQR) | 31 (27–34) | 29 (26–31) | 34 (31–36.25) | <0.001 |
| Left ventricular diameter (mm), median (IQR) | 44 (39.75–48) | 42 (38.75–44.25) | 45 (43–49) | 0.002 |
| Right ventricular diameter (mm), median (IQR) | 23 (21–25.25) | 22 (20.75–24) | 25 (22–27) | 0.003 |
| LVPWT (mm), median (IQR) | 10 (8–10) | 8 (8–9) | 10 (10–11) | <0.001 |
| Interventricular septal wall thickness (mm), median (IQR) | 9 (8–10) | 8.5 (8–9) | 10 (9.75–11.25) | <0.001 |
| Interatrial septal wall thickness (mm), median (IQR) | 6 (5–7) | 5 (5–7) | 6 (6–7) | 0.018 |
| LVEDV (mL), median (IQR) | 95 (78.5–114.25) | 84 (73.75–104) | 103 (92–121.75) | <0.001 |
| LVESV (mL), median (IQR) | 45 (36.75–56.75) | 39 (32–47) | 53.5 (43.75–62.75) | <0.001 |
| Ejection fraction (EF) (%), median (IQR) | 50 (46–56.25) | 52.5 (48–57.5) | 48.5 (45.75–52.5) | 0.011 |
| Stroke volume (mL), median (IQR) | 51 (39–57) | 44 (36.75–55.95) | 53 (46.75–57.25) | 0.027 |
| Cardiac output, median (IQR) | 3.52 (2.88–4.32) | 3.22 (2.69–4.01) | 3.79 (3.05–5.13) | 0.029 |
| Early diastolic peak velocity (E (m/s)), median (IQR) | 0.74 (0.62–0.86) | 0.8 (0.71–0.95) | 0.66 (0.58–0.78) | <0.001 |
| Late diastolic peak velocity (A (m/s)), median (IQR) | 0.51 (0.43–0.73) | 0.48 (0.42–0.57) | 0.71 (0.5–0.79) | <0.001 |
| Early diastolic velocity (e′ (m/s)), median (IQR) | 0.13 (0.11–0.17) | 0.17 (0.14–0.2) | 0.11 (0.09–0.13) | <0.001 |
| Late diastolic velocity (a′ (m/s)), median (IQR) | 0.1 (0.07–0.14) | 0.1 (0.07–0.13) | 0.1 (0.08–0.16) | 0.265 |
| E/A ratio, median (IQR) | 1.4 (0.98–1.8) | 1.72 (1.32–1.98) | 1.05 (0.76–1.42) | <0.001 |
| e′/a′ ratio, median (IQR) | 1.46 (0.81–2.13) | 1.67 (1.41–2.36) | 0.93 (0.7–1.58) | <0.001 |
| E/e′ ratio, median (IQR) | 5.38 (4.43–6.67) | 5.05 (4.04–5.62) | 5.96 (4.98–7.37) | 0.004 |
| Dependent Variable | Predictor | B Unadjusted | (95% CI) | p-Value | R2 | B Adjusted | (95% CI) | p-Value | B-Adjusted Sandwich | (95% CI) | p-Value | B-Adjusted Quantile | (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| E/A ratio | Adiponectin (μg/mL) | 0.069 | (0.0049–0.1331) | 0.035 | 0.056 | 0.0455 | (−0.0148–0.1059) | 0.137 | 0.0455 | (−0.0191–0.1102) | 0.172 | 0.04 | (−0.4–0.7) | 0.189 |
| LVPWT | Adiponectin (μg/mL) | −0.15 | (−0.31–0.01) | 0.06 | 0.045 | −0.02 | (−0.15–0.11) | 0.751 | −0.02 | (−0.16–0.12) | 0.765 | −0.03 | (−0.19–0.09) | 0.62 |
| Visfatin (ng/L) | 0.0002 | (−0.017–0.0173) | 0.984 | 0 | 0 | (−0.0125–0.0125) | 0.999 | 0 | (−0.0136–0.0136) | 0.999 | −0.0085 | (−0.0293–0.0101) | 0.263 | |
| LVEF | Adiponectin (μg/mL) | −0.52 | (−1.31–0.28) | 0.203 | 0.021 | −1.03 | (−1.92–−0.13) | 0.026 | −1.03 | (−1.83–−0.22) | 0.015 | −1.39 | (−1.97–−0.60) | 0.011 |
| CIMT (mean) | Visfatin (ng/L) | −0.0031 | (−0.0283–0.0221) | 0.809 | 0.001 | −0.002 | (−0.0234–0.0194) | 0.852 | −0.002 | (−0.0203–0.0163) | 0.831 | −0.0028 | (−0.0364–0.0141) | 0.870 |
| Interventricular septal wall thickness | Visfatin (ng/L) | −0.0012 | (−0.0228–0.0204) | 0.909 | 0 | −0.0024 | (−0.0186–0.0138) | 0.766 | −0.0024 | (−0.0163–0.0115) | 0.732 | 0.0013 | (−0.0216–0.0096) | 0.875 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ismaiel, A.; Spinu, M.; Budisan, L.; Leucuta, D.-C.; Popa, S.-L.; Chis, B.A.; Berindan-Neagoe, I.; Olinic, D.M.; Dumitrascu, D.L. Relationship between Adipokines and Cardiovascular Ultrasound Parameters in Metabolic-Dysfunction-Associated Fatty Liver Disease. J. Clin. Med. 2021, 10, 5194. https://doi.org/10.3390/jcm10215194
Ismaiel A, Spinu M, Budisan L, Leucuta D-C, Popa S-L, Chis BA, Berindan-Neagoe I, Olinic DM, Dumitrascu DL. Relationship between Adipokines and Cardiovascular Ultrasound Parameters in Metabolic-Dysfunction-Associated Fatty Liver Disease. Journal of Clinical Medicine. 2021; 10(21):5194. https://doi.org/10.3390/jcm10215194
Chicago/Turabian StyleIsmaiel, Abdulrahman, Mihail Spinu, Livia Budisan, Daniel-Corneliu Leucuta, Stefan-Lucian Popa, Bogdan Augustin Chis, Ioana Berindan-Neagoe, Dan Mircea Olinic, and Dan L. Dumitrascu. 2021. "Relationship between Adipokines and Cardiovascular Ultrasound Parameters in Metabolic-Dysfunction-Associated Fatty Liver Disease" Journal of Clinical Medicine 10, no. 21: 5194. https://doi.org/10.3390/jcm10215194