
Association of Non-Invasive Positive Pressure Ventilation with Short-Term Clinical Outcomes in Patients Hospitalized for Acute Decompensated Heart Failure

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
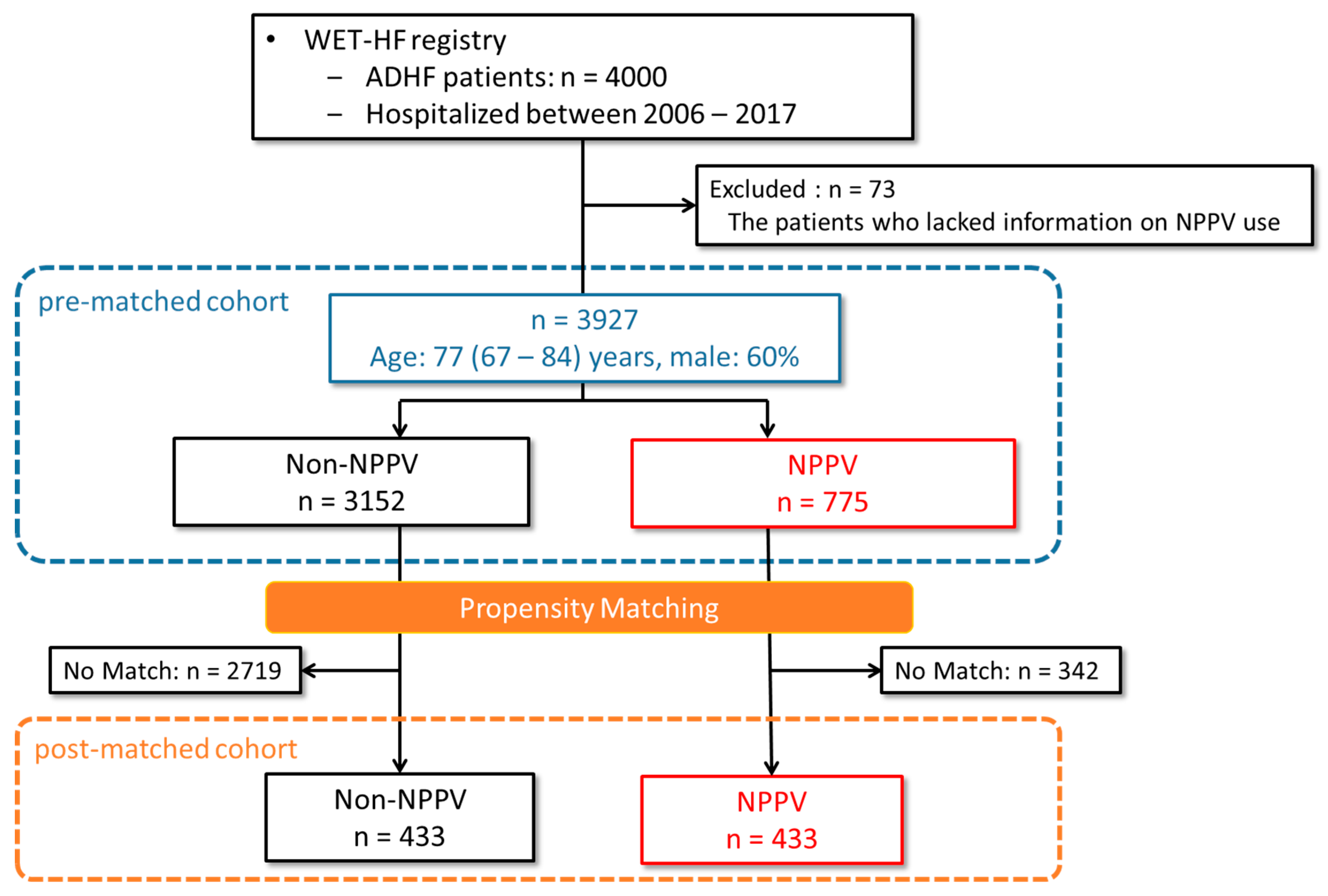
2.1. Study Design
2.2. Endpoint
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Factors Associated with NPPV Use
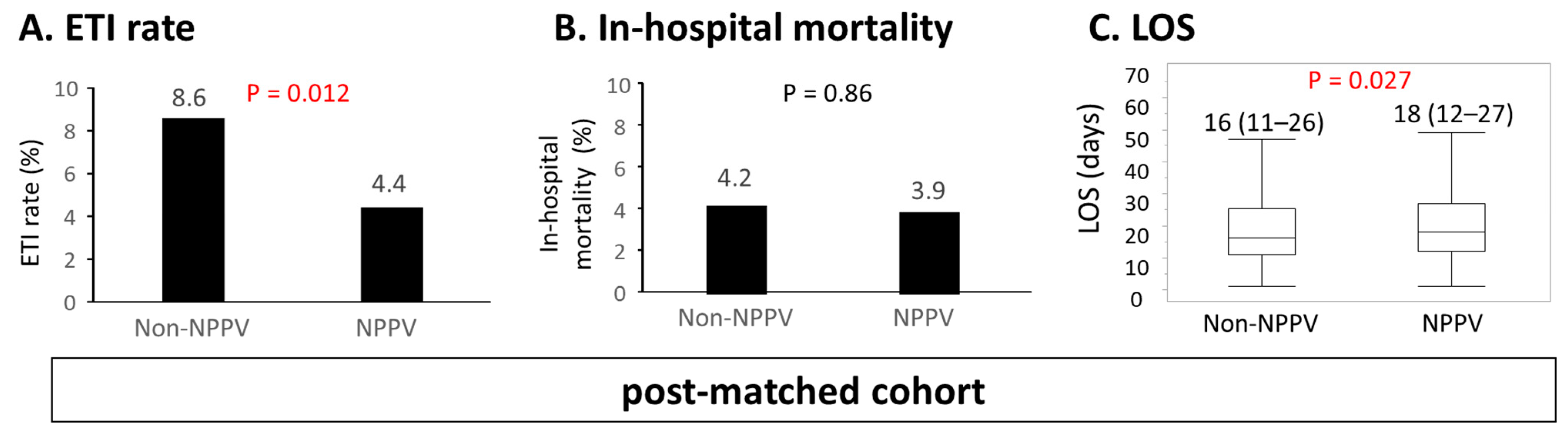
3.3. Findings in the Post-Matched Cohort
3.4. Sensitivity Analysis
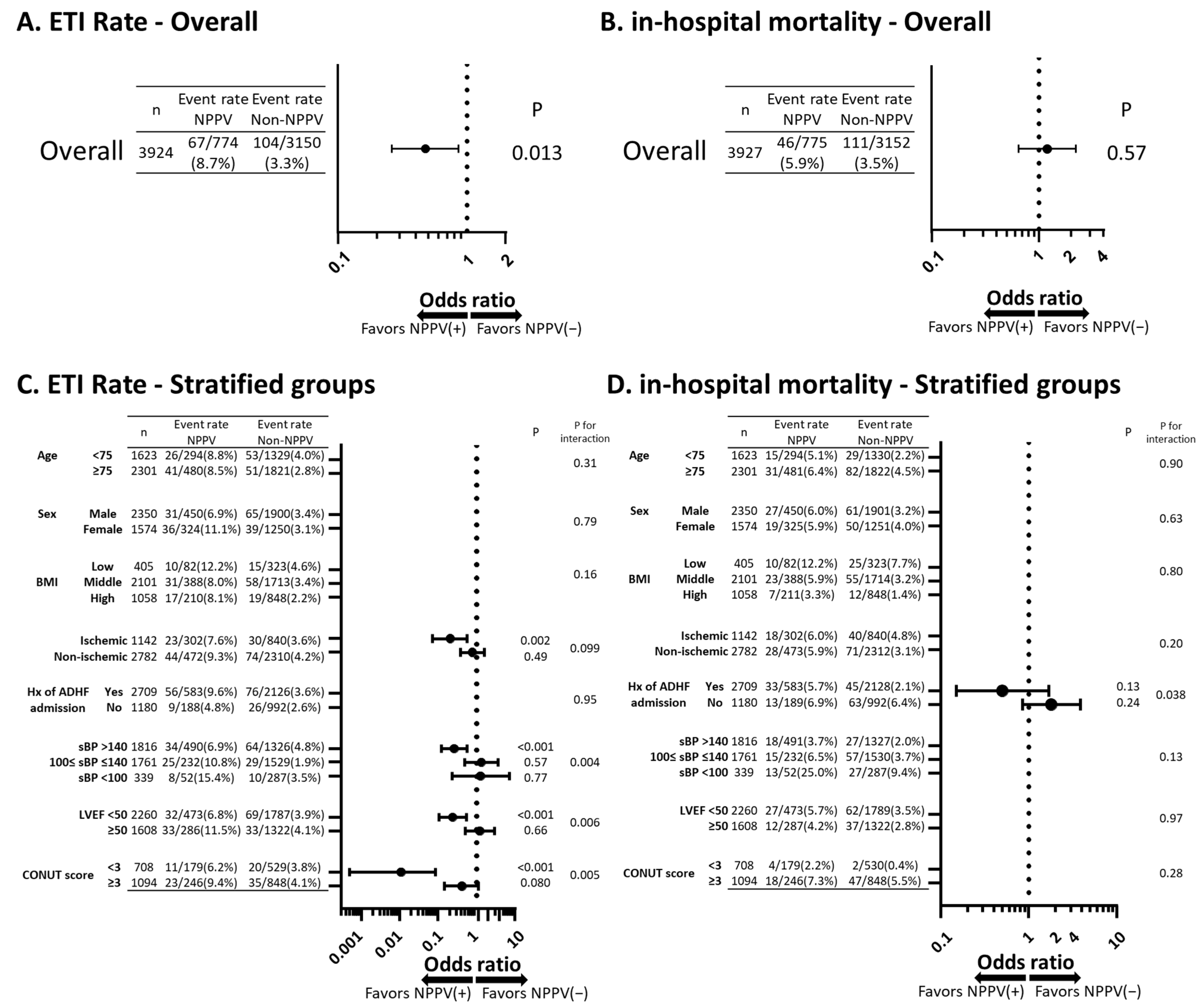
3.5. Stratified Analysis
4. Discussion
4.1. Impact of NPPV Use on ACPE
4.2. The Relationship among Ischemic Etiology, Hypertension, and NPPV Use
4.3. The Subgroups Associated with Longer LOS along with Receiving NPPV
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ponikowski, P.; Anker, S.D.; AlHabib, K.F.; Cowie, M.R.; Force, T.L.; Hu, S.; Jaarsma, T.; Krum, H.; Rastogi, V.; Rohde, L.E.; et al. Heart failure: Preventing disease and death world-wide. ESC Heart Fail. 2014, 1, 4–25. [Google Scholar] [CrossRef] [PubMed]
- Antohi, E.-L.; Ambrosy, A.P.; Collins, S.P.; Ahmed, A.; Iliescu, V.A.; Cotter, G.; Pang, P.S.; Butler, J.; Chioncel, O. Therapeutic Advances in the Management of Acute Decompensated Heart Failure. Am. J. Ther. 2019, 26, e222–e233. [Google Scholar] [CrossRef]
- Brochard, L.; Isabey, D.; Piquet, J.; Amaro, P.; Mancebo, J.; Messadi, A.A.; Brun-Buisson, C.; Rauss, A.; Lemaire, F.; Harf, A. Reversal of acute exacerbations of chronic obstruc-tive lung disease by inspiratory assistance with a face mask. N. Engl. J. Med. 1990, 323, 1523–1530. [Google Scholar] [CrossRef]
- Lin, M.; Yang, Y.F.; Chiang, H.T.; Chang, M.S.; Chiang, B.N.; Cheitlin, M.D. Reappraisal of continuous positive airway pressure ther-apy in acute cardiogenic pulmonary edema. Short-term results and long-term follow-up. Chest 1995, 107, 1379–1386. [Google Scholar] [CrossRef]
- Chadda, K.; Annane, D.; Hart, N.; Gajdos, P.; Raphaël, J.C.; Lofaso, F. Cardiac and respiratory effects of continuous positive airway pressure and noninvasive ventilation in acute cardiac pulmonary edema. Crit. Care Med. 2002, 30, 2457–2461. [Google Scholar] [CrossRef]
- Gray, A.; Goodacre, S.; Newby, D.E.; Masson, M.; Sampson, F.; Nicholl, J. Noninvasive Ventilation in Acute Cardiogenic Pulmonary Edema. N. Engl. J. Med. 2008, 359, 142–151. [Google Scholar] [CrossRef] [Green Version]
- Nava, S.; Carbone, G.; DiBattista, N.; Bellone, A.; Baiardi, P.; Cosentini, R.; Marenco, M.; Giostra, F.; Borasi, G.; Groff, P. Noninvasive ventilation in cardiogenic pulmonary edema: A multicenter randomized trial. Am. J. Respir. Crit. Care Med. 2003, 168, 1432–1437. [Google Scholar] [CrossRef] [Green Version]
- Ducros, L.; Logeart, D.; Vicaut, E.; Henry, P.; Plaisance, P.; Collet, J.-P.; Broche, C.; Gueye, P.; Vergne, M.; on behalf of the CPAP collaborative study group; et al. CPAP for acute cardiogenic pulmonary oedema from out-of-hospital to cardiac intensive care unit: A randomised multicentre study. Intensive Care Med. 2011, 37, 1501–1509. [Google Scholar] [CrossRef]
- Frontin, P.; Bounes, V.; Houzé-Cerfon, C.H.; Charpentier, S.; Houzé-Cerfon, V.; Ducassé, J.L. Continuous positive airway pressure for cardiogenic pulmonary edema: A randomized study. Am. J. Emerg. Med. 2011, 29, 775–781. [Google Scholar] [CrossRef]
- Berbenetz, N.; Wang, Y.; Brown, J.; Godfrey, C.; Ahmad, M.; Vital, F.M.; Lambiase, P.; Banerjee, A.; Bakhai, A.; Chong, M. Non-invasive positive pressure ventilation (CPAP or bilevel NPPV) for cardiogenic pulmonary oedema. Cochrane Database Syst. Rev. 2019, 4, CD005351. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, Y.; Kohsaka, S.; Sato, N.; Takano, T.; Kitai, T.; Yoshikawa, T.; Matsue, Y. 9-Year Trend in the Management of Acute Heart Fail-ure in Japan: A Report From the National Consortium of Acute Heart Failure Registries. J. Am. Heart Assoc. 2018, 7, e008687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeda, S.; Nejima, J.; Takano, T.; Nakanishi, K.; Takayama, M.; Sakamoto, A.; Ogawa, R. Effect of Nasal Continuous Positive Airway Pressure on Pulmonary Edema Complicating Acute Myocardial Infarction. Jpn. Circ. J. 1998, 62, 553–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKee, P.A.; Castelli, W.P.; McNamara, P.M.; Kannel, W.B. The Natural History of Congestive Heart Failure: The Framingham Study. N. Engl. J. Med. 1971, 285, 1441–1446. [Google Scholar] [CrossRef]
- Yagawa, M.; Nagatomo, Y.; Izumi, Y.; Mahara, K.; Tomoike, H.; Shiraishi, Y.; Kohno, T.; Mizuno, A.; Goda, A.; Kohsaka, S.; et al. Effect of Obesity on the Prognostic Impact of Atrial Fibrillation in Heart Failure With Preserved Ejection Fraction. Circ. J. 2017, 81, 966–973. [Google Scholar] [CrossRef] [Green Version]
- Komuro, J.; Nagatomo, Y.; Mahara, K.; Isobe, M.; Goda, A.; Sujino, Y.; Mizuno, A.; Shiraishi, Y.; Kohno, T.; Kohsaka, S.; et al. Clinical Scenario Classification for Characterization and Outcome Prediction of Acute Decompensated Heart Failure Under Contemporary Phenotyping. Circ. Rep. 2019, 1, 162–170. [Google Scholar] [CrossRef] [Green Version]
- Fukuoka, R.; Kohno, T.; Kohsaka, S.; Shiraishi, Y.; Sawano, M.; Abe, T.; Nagatomo, Y.; Goda, A.; Mizuno, A.; Fukuda, K.; et al. Prediction of sudden cardiac death in Japanese heart failure patients: International validation of the Seattle Proportional Risk Model. Europace 2020, 22, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Narumi, T.; Arimoto, T.; Funayama, A.; Kadowaki, S.; Otaki, Y.; Nishiyama, S.; Takahashi, H.; Shishido, T.; Miyashita, T.; Miyamoto, T.; et al. The prognostic importance of objective nutritional indexes in patients with chronic heart failure. J. Cardiol. 2013, 62, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Akita, K.; Kohno, T.; Kohsaka, S.; Shiraishi, Y.; Nagatomo, Y.; Goda, A.; Mizuno, A.; Sujino, Y.; Fukuda, K.; Yoshikawa, T.; et al. Prognostic Impact of Previous Hospitalization in Acute Heart Failure Patients. Circ. J. 2019, 83, 1261–1268. [Google Scholar] [CrossRef] [Green Version]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for con-trolling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Nava, S.; Hill, N. Non-invasive ventilation in acute respiratory failure. Lancet 2009, 374, 250–259. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart fail-ure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on prac-tice guidelines. Circulation 2013, 128, e240–e327. [Google Scholar] [CrossRef]
- Viera, A.J. Odds Ratios and Risk Ratios: What’s the Difference and Why Does It Matter? South. Med. J. 2008, 101, 730–734. [Google Scholar] [CrossRef] [PubMed]
- Pirracchio, R.; Rigon, M.R.; Mebazaa, A.; Zannad, F.; Alla, F.; Chevret, S. Continuous Positive Airway Pressure (CPAP) May Not Reduce Short-Term Mortality in Cardiogenic Pulmonary Edema: A Propensity-Based Analysis. J. Card. Fail. 2013, 19, 108–116. [Google Scholar] [CrossRef]
- Schnell, D.; Timsit, J.-F.; Darmon, M.; Vesin, A.; Goldgran-Toledano, D.; Dumenil, A.-S.; Garrouste-Orgeas, M.; Adrie, C.; Bouadma, L.; Planquette, B.; et al. Noninvasive mechanical ventilation in acute respiratory failure: Trends in use and outcomes. Intensive Care Med. 2014, 40, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Miró, Ò.; Martínez, G.; Masip, J.; Gil, V.; Martín-Sánchez, F.J.; Llorens, P.; Herrero-Puente, P.; Sánchez, C.; Richard, F.; Lucas-Invernón, J.; et al. Effects on short term outcome of non-invasive venti-lation use in the emergency department to treat patients with acute heart failure: A propensity score-based analysis of the EAHFE Registry. Eur. J. Intern. Med. 2018, 53, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Leite-Moreira, A.F.; Correia-Pinto, J. Load as an acute determinant of end-diastolic pressure-volume relation. Am. J. Physiol. Circ. Physiol. 2001, 280, H51–H59. [Google Scholar] [CrossRef]
- López, B.; Gonzalez, A.; Varo, N.; Laviades, C.; Querejeta, R.; Díez, J. Biochemical Assessment of Myocardial Fibrosis in Hypertensive Heart Disease. Hypertension 2001, 38, 1222–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, R.; Gandhi, S.K.; Little, W.C. Acute heart failure with preserved systolic function. Crit. Care Med. 2008, 36, S52–S56. [Google Scholar] [CrossRef]
- Mitchell, G.F.; Hwang, S.-J.; Vasan, R.S.; Larson, M.G.; Levy, D.; Benjamin, E.J.; Pencina, M.J.; Hamburg, N.M.; Vita, J.A. Response to Letters Regarding Article, “Arterial Stiffness and Cardiovascular Events: The Framingham Heart Study”. Circulation 2010, 122, 505–511. [Google Scholar] [CrossRef] [Green Version]
- Namba, T.; Masaki, N.; Matsuo, Y.; Sato, A.; Kimura, T.; Horii, S.; Yasuda, R.; Yada, H.; Kawamura, A.; Takaseet, B.; et al. Arterial Stiffness Is Significantly Associated With Left Ven-tricular Diastolic Dysfunction in Patients with Cardiovascular Disease. Int. Heart J. 2016, 57, 729–735. [Google Scholar] [CrossRef] [Green Version]
- Lenique, F.; Habis, M.; Lofaso, F.; Dubois-Randé, J.L.; Harf, A.; Brochard, L. Ventilatory and hemodynamic effects of continuous positive airway pressure in left heart failure. Am. J. Respir. Crit. Care Med. 1997, 155, 500–505. [Google Scholar] [CrossRef]
- Wiesen, J.; Ornstein, M.; Tonelli, A.; Menon, V.; Ashton, R.W. State of the evidence: Mechanical ventilation with PEEP in patients with cardiogenic shock. Heart 2013, 99, 1812–1817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elhabyan, A.K.; Reyes, B.J.; Hallak, O.; Broce, M.; Rosencrance, J.G.; Lucas, B.D.; Fazal, H. Subendocardial ischemia without coronary artery disease: Is elevated left ventricular end diastolic pressure the culprit? Curr. Med. Res. Opin. 2004, 20, 773–777. [Google Scholar] [CrossRef]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Bos, C.; Benamouzig, R.; Bruhat, A.; Roux, C.; Mahé, S.; Valensi, P.; Gaudichon, C.; Ferrière, F.; Rautureau, J.; Tomé, D. Short-term protein and energy supplementation activates nitrogen kinetics and accretion in poorly nourished elderly subjects. Am. J. Clin. Nutr. 2000, 71, 1129–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kundi, H.; Wadhera, R.K.; Strom, J.B.; Valsdottir, L.R.; Shen, C.; Kazi, D.S.; Yeh, R.W. Association of Frailty With 30-Day Outcomes for Acute Myocardial Infarction, Heart Failure, and Pneumonia Among Elderly Adults. JAMA Cardiol. 2019, 4, 1084–1091. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p Value | Odds Ratio | 95% CI | p Value | |
| Age | 1.006 | 1.000~1.012 | 0.050 | 0.998 | 0.988~1.008 | 0.74 |
| Sex (female) | 1.097 | 0.935~1.287 | 0.25 | 1.045 | 0.819~1.334 | 0.72 |
| Admission year 2006–2009 | 1 (ref) | - | - | 1 (ref) | - | - |
| 2010–2013 | 5.726 | 3.630~3.033 | <0.001 | 3.660 | 1.962~6.829 | <0.001 |
| 2014–2017 | 7.368 | 4.704~11.542 | <0.001 | 6.389 | 3.466~11.76 | <0.001 |
| Etiology ICM | 1 (ref) | - | - | 1 (ref) | - | - |
| DCM | 0.369 | 0.275~0.494 | <0.001 | 0.461 | 0.300~0.707 | <0.001 |
| VHD | 0.598 | 0.486~0.735 | <0.001 | 0.866 | 0.634~1.183 | 0.37 |
| Prior ADHF admission | 0.695 | 0.581~0.833 | <0.001 | 0.898 | 0.584~0.950 | 0.45 |
| Atrial fibrillation | 0.592 | 0.504~0696 | <0.001 | 0.745 | 0.584~0.950 | 0.018 |
| Home oxygen therapy | 1.684 | 1.139~2.488 | 0.006 | 1.573 | 0.869~2.847 | 0.14 |
| Dialysis | 2.484 | 1.735~3.555 | <0.001 | 1.704 | 0.842~3.449 | 0.14 |
| sBP | 1.016 | 1.014~1.018 | <0.001 | 1.012 | 1.009~1.016 | <0.001 |
| Heart Rate | 1.014 | 1.011~1.016 | <0.001 | 1.009 | 1.005~1.013 | <0.001 |
| SpO2 | 0.911 | 0.899~0.923 | <0.001 | 0.914 | 0.898~0.931 | <0.001 |
| NYHA (IV/II–III) | 2.806 | 2.380~3.308 | <0.001 | 2.292 | 1.806~2.909 | <0.001 |
| Cold extremities | 2.777 | 2.290~3.368 | <0.001 | 2.196 | 1.714~2.814 | <0.001 |
| Rales | 2.589 | 2.172~3.087 | <0.001 | 1.554 | 1.221~1.977 | <0.001 |
| BNP/NT-proBNP quartile 1st | 1 (ref) | - | - | 1 (ref) | - | - |
| 2nd | 1.329 | 1.040~1.700 | 0.023 | 1.215 | 0.864~1.708 | 0.26 |
| 3rd | 1.495 | 1.174~1.904 | 0.001 | 1.175 | 0.789~1.582 | 0.53 |
| 4th | 2.128 | 1.686~2.686 | <0.001 | 1.191 | 0.822~1.725 | 0.35 |
| CRP | 13.421 | 6.292~28.703 | 0.075 | 1.075 | 1.042~1.109 | <0.001 |
| eGFR | 0.334 | 0.154~0.713 | 0.005 | 0.999 | 0.993~1.004 | 0.63 |
| LVEF | 0.821 | 0.534~1.263 | 0.37 | 0.997 | 0.993~1.007 | 0.58 |
| Prehospital: β-blocker | 0.751 | 0.639~0.882 | <0.001 | 1.12 | 0.87~1.43 | 0.80 |
| Prehospital: RASi | 1.220 | 1.029~1.447 | 0.021 | 1.387 | 1.100~1.749 | 0.006 |
| Prehospital: MRA | 0.556 | 0.433~0.714 | <0.001 | 0.764 | 0.530~1.099 | 0.14 |
| Prehospital: loop diuretics | 0.632 | 0.537~0.743 | <0.001 | 0.914 | 0.709~1.179 | 0.49 |
| Post-Matched Cohort | ||||
|---|---|---|---|---|
| Non-NPPV (n = 433) | NPPV (n = 433) | p Value | SDM | |
| Year | 0.32 | |||
| 2006–2009 (%) | 20 (5) | 15 (3) | 0.01 | |
| 2010–2013 (%) | 142 (33) | 127 (29) | 0.01 | |
| 2014–2017 (%) | 271 (63) | 291 (67) | 0.01 | |
| Age (years) | 77 (67–84) | 78 (69–84) | 0.40 | 0.06 |
| Female (%) | 183 (42) | 172 (40) | 0.45 | 0.04 |
| BMI | 23.0 (20.5–25.9) | 23.1 (20.3–26.0) | 0.74 | 0.03 |
| Etiology | 0.97 | |||
| DCM (%) | 44 (10) | 41 (9) | 0.02 | |
| ICM (%) | 157 (36) | 156 (36) | 0.01 | |
| VHD (%) | 122 (28) | 121 (28) | 0.01 | |
| HFr/mr/pEF | 0.82 | |||
| HFrEF (%) | 169 (39) | 175 (40) | 0.02 | |
| HFmrEF (%) | 85 (20) | 88 (20) | 0.02 | |
| HFpEF (%) | 179 (41) | 170 (39) | 0.04 | |
| Prior ADHF admission (%) | 116 (27) | 118 (27) | 0.88 | 0.01 |
| Atrial Fibrillation (%) | 179 (41) | 186 (43) | 0.63 | 0.03 |
| Hypertension (%) | 303 (70) | 313 (72) | 0.45 | 0.05 |
| Dyslipidemia (%) | 157 (36) | 196 (45) | 0.008 | 0.18 |
| DM (%) | 152 (35) | 161 (37) | 0.52 | 0.04 |
| Smoking (%) | 190 (44) | 190 (44) | 1 | 0 |
| Dialysis (%) | 17 (4) | 16 (4) | 0.86 | 0.01 |
| COPD (%) | 31 (7) | 17 (4) | 0.037 | 0.14 |
| Stroke/TIA (%) | 63 (15) | 69 (16) | 0.58 | 0.01 |
| Home oxygen therapy (%) | 22 (5) | 20 (5) | 0.75 | 0.02 |
| Pacemaker (%) | 28 (6) | 27 (6) | 0.89 | 0.01 |
| ICD (%) | 11 (3) | 13 (3) | 0.68 | 0.03 |
| CRT (%) | 3 (1) | 4 (1) | 0.70 | 0.03 |
| Clinical Presentation at Admission | ||||
| NYHA II/III/IV | 0.37 | |||
| II (%) | 47 (11) | 60 (14) | 0.09 | |
| III (%) | 105 (24) | 107 (25) | 0.01 | |
| IV (%) | 271 (65) | 266 (61) | 0.07 | |
| sBP (mmHg) | 147 (124–172) | 147 (124–174) | 0.93 | 0 |
| Heart rate (bpm) | 98 (78–118) | 100 (81–120) | 0.12 | 0.07 |
| SpO2 (%) | 95 (90–97) | 94 (89–97) | 0.39 | 0.002 |
| PND (%) | 193 (45) | 222 (52) | 0.029 | 0.15 |
| Orthopnea (%) | 252 (59) | 272 (66) | 0.056 | 0.13 |
| Rales (%) | 305 (70) | 297 (69) | 0.55 | 0.04 |
| Sound III (%) | 194 (45) | 212 (50) | 0.23 | 0.08 |
| JVD (%) | 217 (52) | 213 (52) | 0.91 | 0.01 |
| Edema (%) | 287 (66) | 271 (63) | 0.32 | 0.07 |
| Cold extremities (%) | 150 (35) | 145 (33) | 0.72 | 0.02 |
| Laboratory Data | ||||
| BNP/NT-pBNP quartile | 0.92 | |||
| 1st | 78 (18) | 85 (20) | 0.04 | |
| 2nd | 104 (24) | 104 (24) | 0.001 | |
| 3rd | 123 (28) | 123 (28) | 0.01 | |
| 4th | 128 (30) | 121 (28) | 0.04 | |
| BNP (pg/mL) | 889 (447–1419) | 871 (432–1575) | 0.97 | 0.08 |
| NT-proBNP (pg/mL) | 4884 (2577–10,017) | 4485 (2356–9239) | 0.70 | 0.09 |
| Hemoglobin (g/dL) | 12.0 (10.4–13.8) | 11.9 (10.5–13.7) | 0.54 | 0.07 |
| BUN (mg/dL) | 22.6 (17.8–32.7) | 22.0 (16.9–33.8) | 0.93 | 0.04 |
| eGFR (mL/min/1.73 m2) | 46.5 (32.9–61.0) | 48.6 (30.4–63.0) | 0.57 | 0.05 |
| UA (mg/dL) | 6.7 (5.6–8.2) | 6.4 (5.2–7.9) | 0.043 | 0.14 |
| Na (mEq/L) | 140 (137–142) | 140 (137–142) | 0.55 | 0.1 |
| CRP (mg/dL) | 0.7 (0.2–2.4) | 0.6 (0.2–2.5) | 0.58 | 0.03 |
| Echocardiography | ||||
| LVDd (mm) | 52 (45–59) | 52 (46–58) | 0.97 | 0.003 |
| LVEF (%) | 45 (32–57) | 44 (31–58) | 0.87 | 0.01 |
| LAD (mm) | 43 (38–49) | 43 (38–48) | 0.36 | 0.04 |
| E/e’ | 18.3 (13.2–27.5) | 19.2 (13.9–26.6) | 0.47 | 0.08 |
| TRPG (mmHg) | 29 (22–37) | 29 (23–38) | 0.45 | 0.03 |
| Pre-hospital treatment | ||||
| ACE-I/ARB (%) | 203 (47) | 208 (48) | 0.73 | 0.02 |
| β-blocker (%) | 187 (43) | 182 (42) | 0.73 | 0.02 |
| MRA (%) | 62 (14) | 48 (11) | 0.15 | 0.097 |
| Loop diuretic(po.) (%) | 170 (39) | 171 (39) | 0.94 | 0.004 |
| Thiazide (%) | 16 (4) | 20 (5) | 0.49 | 0.05 |
| In-hospital treatment | ||||
| Loop diuretics (iv.) (%) | 313 (72) | 343 (79) | 0.017 | 0.03 |
| Nitrates (%) | 129 (39) | 197 (46) | <0.001 | 0.3 |
| Carperitide (%) | 210 (49) | 241 (56) | 0.032 | 0.15 |
| PDE-III (%) | 14 (3) | 11 (3) | 0.55 | 0.04 |
| Catecholamine(%) | 61 (14) | 102 (24) | <0.001 | 0.24 |
| IABP (%) | 18 (4) | 12 (3) | 0.27 | 0.08 |
| n (NPPV/Non-NPPV) | LOS (NPPV/Non-NPPV) | p for Interaction | β | SEM | t-Value | p Value | ||
|---|---|---|---|---|---|---|---|---|
| Overall | 775/3152 | 14 (10–27)/14 (10–23) | NA | 1.527 | 0.715 | 2.14 | 0.032 | |
| Stratified groups | ||||||||
| Age | <75 | 294/1330 | 15 (10–26)/15 (10–23) | 0.21 | ||||
| ≥75 | 481/1822 | 18 (11–27)/14 (9–22) | ||||||
| sex | Male | 450/1901 | 16 (10–26)/14 (10–23) | 0.69 | ||||
| Female | 325/1251 | 19 (11–29)/14 (9–22) | ||||||
| BMI | Low | 82/323 | 16 (9–28)/15 (9–28) | 0.73 | ||||
| Middle | 388/1714 | 17 (11–27)/14 (10–22) | ||||||
| High | 211/848 | 17 (10–26)/14 (9–21) | ||||||
| Etiology | Ischemic | 302/840 | 17 (10–26)/15 (10–23) | 0.008 | 0.069 | 1.217 | 0.06 | 0.96 |
| Non-ischemic | 473/2312 | 17 (11–27)/14 (9–22) | 2.375 | 0.88 | 2.69 | 0.007 | ||
| Hx of ADHF admission | Yes | 189/992 | 16 (9–26)/14 (10–24) | 0.084 | 1.404 | 1.646 | 0.85 | 0.39 |
| No | 583/2128 | 17 (11–27)/14 (9–22) | 1.524 | 0.754 | 2.02 | 0.044 | ||
| sBP | ≥140 | 491/1327 | 16 (10–24)/14 (9–21) | 0.062 | 1.362 | 0.901 | 1.51 | 0.13 |
| 100≤ <140 | 232/1530 | 19 (12–31)/14 (10–23) | 0.548 | 1.25 | 0.44 | 0.66 | ||
| <100 | 52/287 | 25 (12–40)/17 (10–31) | 7.077 | 2.338 | 3.03 | 0.003 | ||
| LVEF | <50 | 473/1789 | 17 (10–27)/15 (10–24) | 0.50 | ||||
| ≥50 | 287/1322 | 18 (11–27)/13 (9–21) | ||||||
| CONUT score | ≤3 | 179/530 | 14 (9–26)/13 (9–21) | 0.044 | 0.523 | 0.919 | 0.57 | 0.57 |
| >3 | 248/848 | 20 (12–35) /16 (10–27) | 4.044 | 1.306 | 3.1 | 0.002 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yukino, M.; Nagatomo, Y.; Goda, A.; Kohno, T.; Takei, M.; Nishihata, Y.; Saji, M.; Toyosaki, Y.; Nakano, S.; Ikegami, Y.; et al. Association of Non-Invasive Positive Pressure Ventilation with Short-Term Clinical Outcomes in Patients Hospitalized for Acute Decompensated Heart Failure. J. Clin. Med. 2021, 10, 5092. https://doi.org/10.3390/jcm10215092
Yukino M, Nagatomo Y, Goda A, Kohno T, Takei M, Nishihata Y, Saji M, Toyosaki Y, Nakano S, Ikegami Y, et al. Association of Non-Invasive Positive Pressure Ventilation with Short-Term Clinical Outcomes in Patients Hospitalized for Acute Decompensated Heart Failure. Journal of Clinical Medicine. 2021; 10(21):5092. https://doi.org/10.3390/jcm10215092
Chicago/Turabian StyleYukino, Midori, Yuji Nagatomo, Ayumi Goda, Takashi Kohno, Makoto Takei, Yosuke Nishihata, Mike Saji, Yuichi Toyosaki, Shintaro Nakano, Yukinori Ikegami, and et al. 2021. "Association of Non-Invasive Positive Pressure Ventilation with Short-Term Clinical Outcomes in Patients Hospitalized for Acute Decompensated Heart Failure" Journal of Clinical Medicine 10, no. 21: 5092. https://doi.org/10.3390/jcm10215092