
Perceptions of Patients and Their Families Regarding Limitation of Therapeutic Effort in the Intensive Care Unit

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Type of Study and Setting
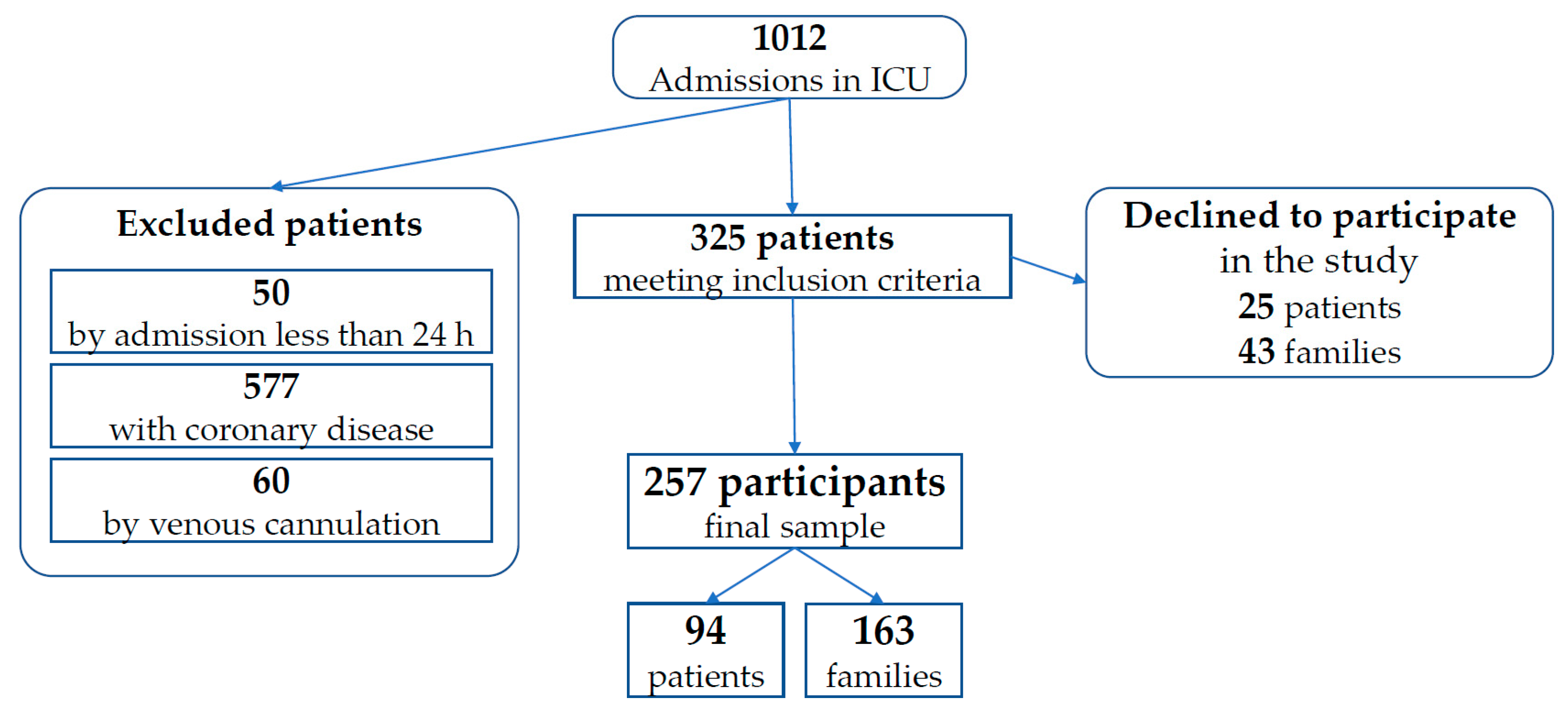
2.2. Study Population and Sample Size
2.3. Inclusion and Exclusion Criteria
2.4. Measurement Instruments and Variables
2.5. Procedures
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Patients/Family Characteristics
3.2. Clinical Profile
3.3. Responses to the Questionnaire
4. Discussion
4.1. Main Findings of the Study
4.2. Context of the Findings within the Current Literature
4.3. Limitations of the Study
4.4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stokes, H.; Vanderspank-Wright, B.; Fothergill Bourbonnais, F.; Wright, D.K. Meaningful experiences and end-of-life care in the intensive care unit: A qualitative study. Intensive Crit. Care Nurs. 2019, 53, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Borsellino, P. Limitation of the therapeutic effort: Ethical and legal justification for withholding and/or withdrawing life sustaining treatments. Multidiscip. Respir. Med. 2015, 10, 5. [Google Scholar] [CrossRef] [Green Version]
- Sprung, C.L.; Cohen, S.L.; Sjokvist, P.; Baras, M.; Bulow, H.H.; Hovilehto, S.; Ledoux, D.; Lippert, A.; Maia, P.; Phelan, D.; et al. End-of-life practices in European intensive care units: The ethicus study. JAMA 2003, 290, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Hinkle, L.J.; Bosslet, G.T.; Torke, A.M. Factors associated with family satisfaction with end-of-life care in the ICU: A systematic review. Chest 2015, 147, 82–93. [Google Scholar] [CrossRef]
- Efstathiou, N.; Walker, W. Intensive care nurses’ experiences of providing end-of-life care after treatment withdrawal: A qualitative study. J. Clin. Nurs. 2014, 23, 3188–3196. [Google Scholar] [CrossRef] [Green Version]
- Chalfin, D.B.; Trzeciak, S.; Likourezos, A.; Baumann, B.M.; Dellinger, R.P.; FCCM for the DELAY-ED Study Group. Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit. Care Med. 2007, 35, 1477–1483. [Google Scholar] [CrossRef]
- Manalo, M.F. End-of-life decisions about withholding or withdrawing therapy: Medical, ethical, and religio-cultural considerations. Palliat. Care 2013, 7, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Velarde-Garcia, J.F.; Luengo-Gonzalez, R.; Gonzalez-Hervias, R.; Cardenete-Reyes, C.; Alvarez-Embarba, B.; Palacios-Cena, D. Limitation of therapeutic effort experienced by intensive care nurses. Nurs. Ethics 2018, 25, 867–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varkey, B. Principles of clinical ethics and their application to practice. Med. Princ. Pr. 2021, 30, 17–28. [Google Scholar] [CrossRef]
- Page, K. The four principles: Can they be measured and do they predict ethical decision making? BMC Med. Ethics 2012, 13, 10. [Google Scholar] [CrossRef] [Green Version]
- Baena Alvarez, C. Limitation of therapeutic effort: When less is more. Colomb. Med. 2015, 46, 1–2. [Google Scholar] [CrossRef]
- Weisbord, S.D.; Fried, L.F.; Arnold, R.M.; Fine, M.J.; Levenson, D.J.; Peterson, R.A.; Switzer, G.E. Prevalence, severity, and importance of physical and emotional symptoms in chronic hemodialysis patients. J. Am. Soc. Nephrol. 2005, 16, 2487–2494. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Veldhuyzen Van Zanten, S.J.; Feeny, D.H.; Patrick, D.L. Measuring quality of life in clinical trials: A taxonomy and review. CMAJ 1989, 140, 1441–1448. [Google Scholar]
- Mitchell, H.; Noble, S.; Finlay, I.; Nelson, A. Defining the palliative care patient: Its challenges and implications for service delivery. BMJ Support Palliat. Care 2013, 3, 46–52. [Google Scholar] [CrossRef]
- Groebe, B.; Rietz, C.; Voltz, R.; Strupp, J. How to talk about attitudes toward the end of life: A qualitative study. Am. J. Hosp. Palliat. Care 2019, 36, 697–704. [Google Scholar] [CrossRef]
- Billings, J.A. The need for safeguards in advance care planning. J. Gen. Intern. Med. 2012, 27, 595–600. [Google Scholar] [CrossRef] [Green Version]
- Sprung, C.L.; Truog, R.D.; Curtis, J.R.; Joynt, G.M.; Baras, M.; Michalsen, A.; Briegel, J.; Kesecioglu, J.; Efferen, L.; De Robertis, E.; et al. Seeking worldwide professional consensus on the principles of end-of-life care for the critically ill. The consensus for worldwide end-of-life practice for patients in intensive care units (WELPICUS) study. Am. J. Respir. Crit. Care Med. 2014, 190, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Dunphy, E.J.; Conlon, S.C.; O’Brien, S.A.; Loughrey, E.; O’Shea, B.J. End-of-life planning with frail patients attending general practice: An exploratory prospective cross-sectional study. Br. J. Gen. Pr. 2016, 66, e661–e666. [Google Scholar] [CrossRef] [Green Version]
- CNDH. Convenio Para La Protección de Los Derechos Humanos y a Dignidad Del Ser Humano Con Respecto a Las Aplicaciones De La Biología y La Medicina; Cuadernos de Bioética: Madrid, Spain, 1997. [Google Scholar]
- Ley 41/2002, De 14 De Noviembre, Básica Reguladora De La Autonomía Del Paciente y De Derechos y Obligaciones en Materia de Información y Documentación Clínica. Jefatura del Estado. Boletín Oficial de Estado número 274, de 15 de noviembre de 2002. Available online: https://www.boe.es/buscar/pdf/2002/BOE-A-2002-22188-consolidado.pdf (accessed on 15 October 2021).
- Real Decreto 124/2007, de 2 de Febrero, Por el Que se Regula el Registro Nacional de Instrucciones Previas y el Correspondiente Fichero Automatizado de Datos de Carácter Personal. Ministerio de Sanidad y Consumo. Boletín Oficial de Estado número 40, de 15 de febrero de 2007. Available online: https://www.boe.es/buscar/pdf/2007/BOE-A-2007-3160-consolidado.pdf (accessed on 15 October 2021).
- Decreto 15/2006, de 21 de Febrero, del Registro de Voluntades Anticipadas de Castilla-La Mancha. (DOCM 42 de 24-02-2006). Available online: http://www.juansiso.es/REPERTORIO/C%20Mancha/CASTILLA%20LA%20MANCHA.%20Decreto%2015-2006%20de%20Voluntades%20Anticipadas.pdf (accessed on 15 October 2021).
- Baliza, F.; Bousso, R.; Spineli, V.; Silva, L.; Poles, K. Palliative care in the home: Perceptions of nurses in the Family Health Strategy. Acta Paul. Enferm. 2012, 25, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Ip, M.; Gilligan, T.; Koenig, B.; Raffin, T.A. Ethical decision-making in critical care in Hong Kong. Crit. Care Med. 1998, 26, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Nebot, C.; Ortega, B.; Mira, J.J.; Ortiz, L. [Dying with dignity. A study of living wills]. Gac. Sanit. 2010, 24, 437–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chochinov, H.M.; Hack, T.; Hassard, T.; Kristjanson, L.J.; McClement, S.; Harlos, M. Dignity in the terminally ill: A cross-sectional, cohort study. Lancet 2002, 360, 2026–2030. [Google Scholar] [CrossRef]
- Fried, T.R.; Van Ness, P.H.; Byers, A.L.; Towle, V.R.; O’Leary, J.R.; Dubin, J.A. Changes in preferences for life-sustaining treatment among older persons with advanced illness. J. Gen. Intern. Med. 2007, 22, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Barrio, I.; Simón, P.; Pascau, M.J. Role of the nurse in advance planning:beyond prior instructions or advance directives. Enfermería Clínica 2004, 14, 235–241. [Google Scholar] [CrossRef]
- Yildiz Celtek, N.; Suren, M.; Demir, O.; Okan, I. Karnofsky performance scale validity and reliability of Turkish palliative cancer patients. Turk. J. Med. Sci. 2019, 49, 894–898. [Google Scholar] [CrossRef]
- Bernaola-Sagardui, I. Validation of the Barthel index in the Spanish population. Enferm Clin. 2018, 28, 210–211. [Google Scholar] [CrossRef]
- Fernandez, R.R.; Cruz, J.J.; Mata, G.V. Validation of a quality of life questionnaire for critically ill patients. Intensive Care Med. 1996, 22, 1034–1042. [Google Scholar] [CrossRef]
- Russell, N. End-of-life care in hospital. Intern. Med. J. 2019, 49, 1056. [Google Scholar] [CrossRef] [PubMed]
- Campbell, L. Opinion piece: Honouring the wishes of a dying patient: From intensive care to home with palliative care. Contemp. Nurse 2013, 45, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Gonella, S.; Basso, I.; De Marinis, M.G.; Campagna, S.; Di Giulio, P. Good end-of-life care in nursing home according to the family carers’ perspective: A systematic review of qualitative findings. Palliat. Med. 2019, 33, 589–606. [Google Scholar] [CrossRef]
- Kirchhoff, K.T.; Anumandla, P.R.; Foth, K.T.; Lues, S.N.; Gilbertson-White, S.H. Documentation on withdrawal of life support in adult patients in the intensive care unit. Am. J. Crit. Care 2004, 13, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Krug, K.; Miksch, A.; Peters-Klimm, F.; Engeser, P.; Szecsenyi, J. Correlation between patient quality of life in palliative care and burden of their family caregivers: A prospective observational cohort study. BMC Palliat. Care 2016, 15, 4. [Google Scholar] [CrossRef] [Green Version]
- Guidet, B.; Flaatten, H.; Boumendil, A.; Morandi, A.; Andersen, F.H.; Artigas, A.; Bertolini, G.; Cecconi, M.; Christensen, S.; Faraldi, L.; et al. Withholding or withdrawing of life-sustaining therapy in older adults (>/= 80 years) admitted to the intensive care unit. Intensive Care Med. 2018, 44, 1027–1038. [Google Scholar] [CrossRef]
- Schubart, J.R.; Levi, B.H.; Dellasega, C.; Whitehead, M.; Green, M.J. Factors that affect decisions to receive (or not receive) life-sustaining treatment in advance care planning. J. Psychosoc. Nurs Ment. Health Serv. 2014, 52, 38–44. [Google Scholar] [CrossRef]
- Tillyard, A.R. Ethics review: ’Living wills’ and intensive care—An overview of the American experience. Crit. Care 2007, 11, 219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Michaels, J.; Meeker, M.A. Family outcomes and perceptions of end-of-life care in the intensive care unit: A mixed-methods review. J. Palliat. Care 2020, 35, 143–153. [Google Scholar] [CrossRef]
- Molina, J.; Perez, M.; Herreros, B.; Martin, M.D.; Velasco, M. [Knowledge and attitude regarding previous instructions for the patients of a public hospital of Madrid]. Rev. Clin. Esp. 2011, 211, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Silveira, M.J.; Kim, S.Y.; Langa, K.M. Advance directives and outcomes of surrogate decision making before death. N. Engl. J. Med. 2010, 362, 1211–1218. [Google Scholar] [CrossRef] [Green Version]
- Ahluwalia, S.C.; Chuang, F.L.; Antonio, A.L.; Malin, J.L.; Lorenz, K.A.; Walling, A.M. Documentation and discussion of preferences for care among patients with advanced cancer. J. Oncol. Pr. 2011, 7, 361–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAdam, J.L.; Stotts, N.A.; Padilla, G.; Puntillo, K. Attitudes of critically ill Filipino patients and their families toward advance directives. Am. J. Crit. Care 2005, 14, 17–25. [Google Scholar] [CrossRef]
- Kumar, A.; Aronow, W.S.; Alexa, M.; Gothwal, R.; Jesmajian, S.; Bhushan, B.; Gaba, P.; Catevenis, J. Prevalence of use of advance directives, health care proxy, legal guardian, and living will in 512 patients hospitalized in a cardiac care unit/intensive care unit in 2 community hospitals. Arch. Med. Sci. 2010, 6, 188–191. [Google Scholar] [CrossRef]
- Solsona, J.F.; Sucarrats, A.; Maull, E.; Barbat, C.; Garcia, S.; Villares, S. [Taking decisions at the end of life. A survey of the attitude of critically ill patients against death]. Med. Clin. 2003, 120, 335–336. [Google Scholar] [CrossRef]
- Ortiz-Goncalves, B.; Albarran Juan, E.; Labajo Gonzalez, E.; Santiago-Saez, A.; Perea-Perez, B. [End-of-life decisions: Results of the expert-validated questionnaire]. Gac. Sanit. 2018, 32, 333–338. [Google Scholar] [CrossRef]
- Sharma, R.K.; Hughes, M.T.; Nolan, M.T.; Tudor, C.; Kub, J.; Terry, P.B.; Sulmasy, D.P. Family understanding of seriously-ill patient preferences for family involvement in healthcare decision making. J. Gen. Intern. Med. 2011, 26, 881–886. [Google Scholar] [CrossRef] [Green Version]
- Shalowitz, D.I.; Garrett-Mayer, E.; Wendler, D. The accuracy of surrogate decision makers: A systematic review. Arch. Intern. Med. 2006, 166, 493–497. [Google Scholar] [CrossRef]
- Tanuseputro, P.; Wodchis, W.P.; Fowler, R.; Walker, P.; Bai, Y.Q.; Bronskill, S.E.; Manuel, D. The health care cost of dying: A population-based retrospective cohort study of the last year of life in Ontario, Canada. PLoS ONE 2015, 10, e0121759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro-Jiménez, G.; Blanco-Portillo, A.; Pérez-Figueras, M.; Pérez-Fernández, E.; García-Caballero, R.; Velasco-Arribas, M. Evolution of the opinion of relatives on the limitation of therapeutic effort in elderly patients. Med. Int. Méx. 2021, 37, 45–55. [Google Scholar] [CrossRef]
- Wakefield, C.E.; Watts, K.J.; Homewood, J.; Meiser, B.; Siminoff, L.A. Attitudes toward organ donation and donor behavior: A review of the international literature. Prog. Transpl. 2010, 20, 380–391. [Google Scholar] [CrossRef]
- De Groot, J.; van Hoek, M.; Hoedemaekers, C.; Hoitsma, A.; Smeets, W.; Vernooij-Dassen, M.; van Leeuwen, E. Decision making on organ donation: The dilemmas of relatives of potential brain dead donors. BMC Med. Ethics 2015, 16, 64. [Google Scholar] [CrossRef] [Green Version]
- Hulme, W.; Allen, J.; Manara, A.R.; Murphy, P.G.; Gardiner, D.; Poppitt, E. Factors influencing the family consent rate for organ donation in the UK. Anaesthesia 2016, 71, 1053–1063. [Google Scholar] [CrossRef] [PubMed]
- Hinders, D. Advance directives: Limitations to completion. Am. J. Hosp. Palliat. Care 2012, 29, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Decker, I.M.; Reed, P.G. Developmental and contextual correlates of elders’ anticipated end-of-life treatment decisions. Death Stud. 2005, 29, 827–846. [Google Scholar] [CrossRef] [PubMed]
- Sprung, C.L.; Ricou, B.; Hartog, C.S.; Maia, P.; Mentzelopoulos, S.D.; Weiss, M.; Levin, P.D.; Galarza, L.; de la Guardia, V.; Schefold, J.C.; et al. Changes in end-of-life practices in european intensive care units from 1999 to 2016. JAMA 2019, 322, 1692–1704. [Google Scholar] [CrossRef] [PubMed]
- McCormack, R.; Clifford, M.; Conroy, M. Attitudes of UK doctors towards euthanasia and physician-assisted suicide: A systematic literature review. Palliat. Med. 2012, 26, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Yun, Y.H.; Han, K.H.; Park, S.; Park, B.W.; Cho, C.H.; Kim, S.; Lee, D.H.; Lee, S.N.; Lee, E.S.; Kang, J.H.; et al. Attitudes of cancer patients, family caregivers, oncologists and members of the general public toward critical interventions at the end of life of terminally ill patients. CMAJ 2011, 183, E673–E679. [Google Scholar] [CrossRef] [Green Version]
- Li, L.L.; Cheong, K.Y.; Yaw, L.K.; Liu, E.H. The accuracy of surrogate decisions in intensive care scenarios. Anaesth. Intensive Care 2007, 35, 46–51. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total | Family | Patient | ||||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | p-Value χ2 | ||
| GENDER | Men | 133 | 51.8 | 66 | 40.5 | 67 | 71.3 | 0.001 |
| Women | 124 | 48.2 | 97 | 59.5 | 27 | 28.7 | ||
| AGE (years) | 45.6 + 11.7 | 59.6 + 13.4 | ||||||
| EDUCATION LEVEL | No education | 25 | 9.7 | 2 | 1.2 | 23 | 24.5 | 0.001 |
| Primary level | 102 | 39.7 | 63 | 38.7 | 39 | 41.5 | ||
| Secondary level | 78 | 30.4 | 57 | 35.0 | 21 | 22.3 | ||
| University level | 52 | 20.2 | 41 | 25.2 | 11 | 11.7 | ||
| RELIGION | Non-practicing Catholic | 140 | 54.5 | 87 | 53.4 | 53 | 56.4 | 0.457 |
| Practicing Catholic | 75 | 29.2 | 50 | 30.7 | 25 | 26.6 | ||
| No religion | 37 | 14.4 | 24 | 14.7 | 13 | 13.8 | ||
| Orthodox | 2 | 0.8 | 1 | 0.6 | 1 | 1.1 | ||
| Evangelist | 2 | 0.8 | 0 | 0.0 | 2 | 2.1 | ||
| Muslim | 1 | 0.4 | 1 | 0.6 | 0 | 0.0 | ||
| n | % | ||
|---|---|---|---|
| MEDICAL PATHOLOGY | Cardiovascular | 98 | 38.1 |
| Respiratory | 63 | 24.5 | |
| Neurological | 28 | 10.9 | |
| Sepsis | 15 | 5.8 | |
| Gastrointestinal | 11 | 4.3 | |
| Renal | 5 | 1.9 | |
| Traffic accident | 4 | 1.6 | |
| Traumatology | 2 | 0.8 | |
| Neoplasia | 1 | 0.4 | |
| Heatstroke | 1 | 0.4 | |
| Self-harm | 1 | 0.4 | |
| Metabolic acidosis | 1 | 0.4 | |
| SURGICAL PATHOLOGY | Gastrointestinal surgery | 8 | 3.1 |
| Traumatology | 6 | 2.3 | |
| Neurosurgery | 5 | 1.9 | |
| Urology | 3 | 1.2 | |
| Vascular surgery | 2 | 0.8 | |
| Gynecological surgery | 2 | 0.8 | |
| Otorhinolaryngology | 1 | 0.4 | |
| TOTAL | 257 | 100 |
| RESPONDENTS | PAEEC SCALE SCORE | Total | ||||
|---|---|---|---|---|---|---|
| 0–2 Points | 3–7 Points | >8 Points | ||||
| Family | 75 (46%) | 51 (31.3%) | 37 (22.7%) | 163 (100%) | ||
| Patient | 69 (73.4%) | 15 (16%) | 10 (10.6%) | 94 (100%) | ||
| p Value χ2 | ||||||||
|---|---|---|---|---|---|---|---|---|
| Total | Family | Patient | ||||||
| N | % | N | % | N | % | |||
| Willingness to be a donor | No | 168/257 | 65.4 | 132/163 | 81.0 | 36/94 | 38.3 | <0.0001 |
| Yes | 89/257 | 34.6 | 31/163 | 19.0 | 58/94 | 61.7 | ||
| Formalized donor status | No | 75/87 | 86.2 | 24/31 | 77.4 | 51/56 | 91.1 | 0.077 |
| Yes | 12/87 | 13.8 | 7/31 | 22.6 | 5/56 | 8.9 | ||
| Healthcare proxy | No | 233/256 | 91.0 | 148/162 | 91.4 | 85/94 | 90.4 | 0.801 |
| Yes | 23/256 | 9.0 | 14/162 | 8.6% | 9/94 | 9.6 | ||
| Advanced Healthcare Directive | No | 253/257 | 98.4 | 160/163 | 98.2 | 93/94 | 98.9 | 0.628 |
| Yes | 4/257 | 1.6 | 3/163 | 1.8 | 1/94 | 1.1 | ||
| Legal Will | No | 154/257 | 59.9 | 89/163 | 54.6 | 65/94 | 69.1 | 0.022 |
| Yes | 103/257 | 40.1 | 74/163 | 45.4 | 29/94 | 30.9 | ||
| QUESTIONNAIRE RESPONDENTS | WOULD NOT ACCEPT | WOULD ACCEPT | p-Value χ2 |
|---|---|---|---|
| Family | 57/163 (34.9%) | 106/163 (65.0%) | 0.227 |
| Patient | 40/94 (42.5%) | 54/94 (57.4%) | |
| Total | 97/257 (37.7%) | 160/257 (62.2%) |
| PAEEC SCALE SCORE * (Points) | DECISION TO LIMIT TREATMENT | p-Value U Mann–Whitney | |
|---|---|---|---|
| Would Not Accept | Would Accept | ||
| 0–2 | 58 (40.3%) | 86 (59.7%) | 0.5001 |
| 3–7 | 21 (31.8%) | 45 (68.2%) | |
| ≥8 | 18 (38.3%) | 29 (61.7%) | |
| TOTAL | 97 (37.7%) | 160 (62.3%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz Camargo, J.C.; Hernández-Martínez, A.; Rodríguez-Almagro, J.; Parra-Fernández, M.L.; Prado-Laguna, M.d.C.; Martín, M. Perceptions of Patients and Their Families Regarding Limitation of Therapeutic Effort in the Intensive Care Unit. J. Clin. Med. 2021, 10, 4900. https://doi.org/10.3390/jcm10214900
Muñoz Camargo JC, Hernández-Martínez A, Rodríguez-Almagro J, Parra-Fernández ML, Prado-Laguna MdC, Martín M. Perceptions of Patients and Their Families Regarding Limitation of Therapeutic Effort in the Intensive Care Unit. Journal of Clinical Medicine. 2021; 10(21):4900. https://doi.org/10.3390/jcm10214900
Chicago/Turabian StyleMuñoz Camargo, Juan Carlos, Antonio Hernández-Martínez, Julián Rodríguez-Almagro, María Laura Parra-Fernández, María del Carmen Prado-Laguna, and Mairena Martín. 2021. "Perceptions of Patients and Their Families Regarding Limitation of Therapeutic Effort in the Intensive Care Unit" Journal of Clinical Medicine 10, no. 21: 4900. https://doi.org/10.3390/jcm10214900