
Spirometry Examination of Adolescents with Thoracic Idiopathic Scoliosis: Is Correction for Height Loss Useful?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Radiological Examination
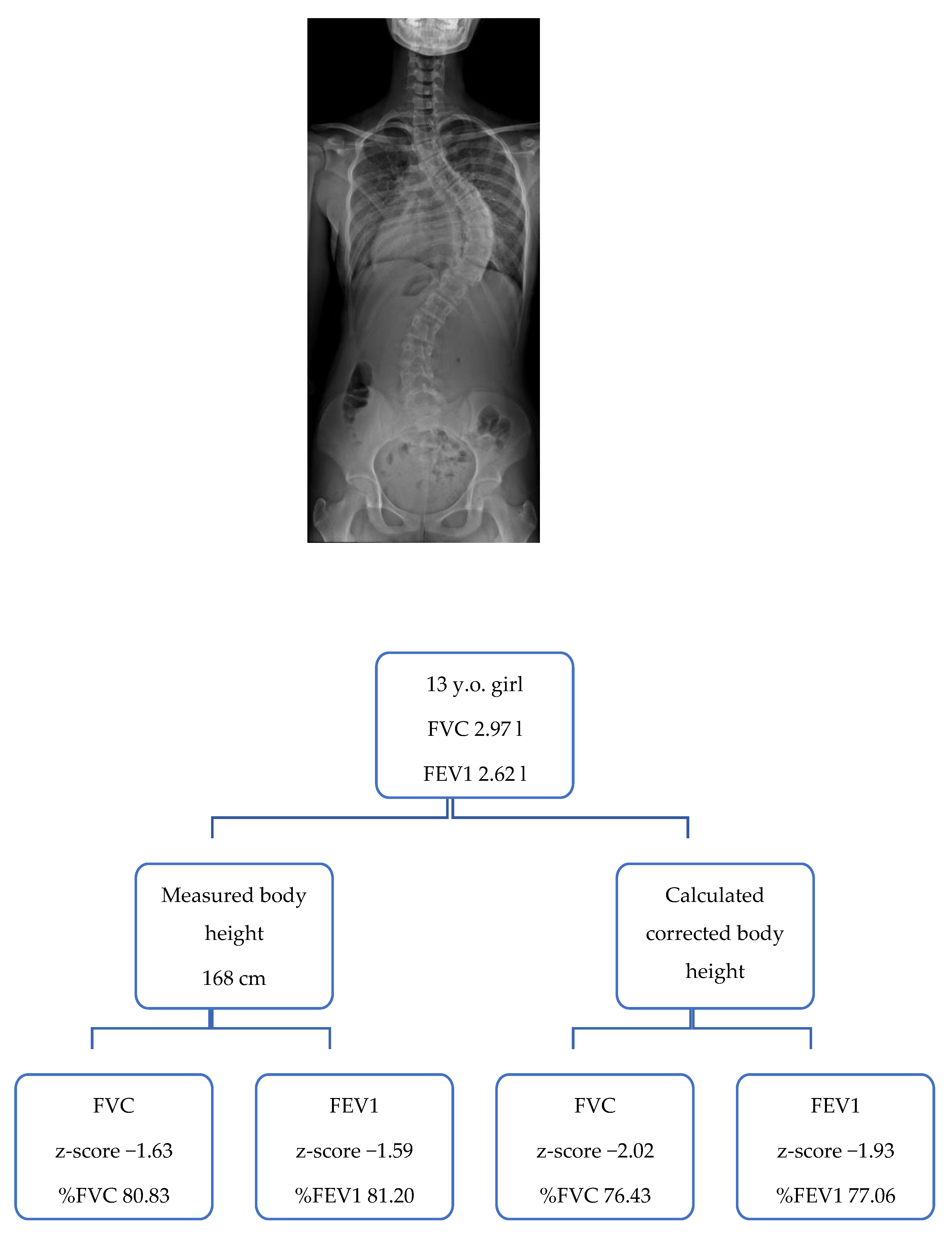
2.3. Corrected Body Height Calculation
2.4. Pulmonary Testing
2.5. Statistical Analysis
3. Results
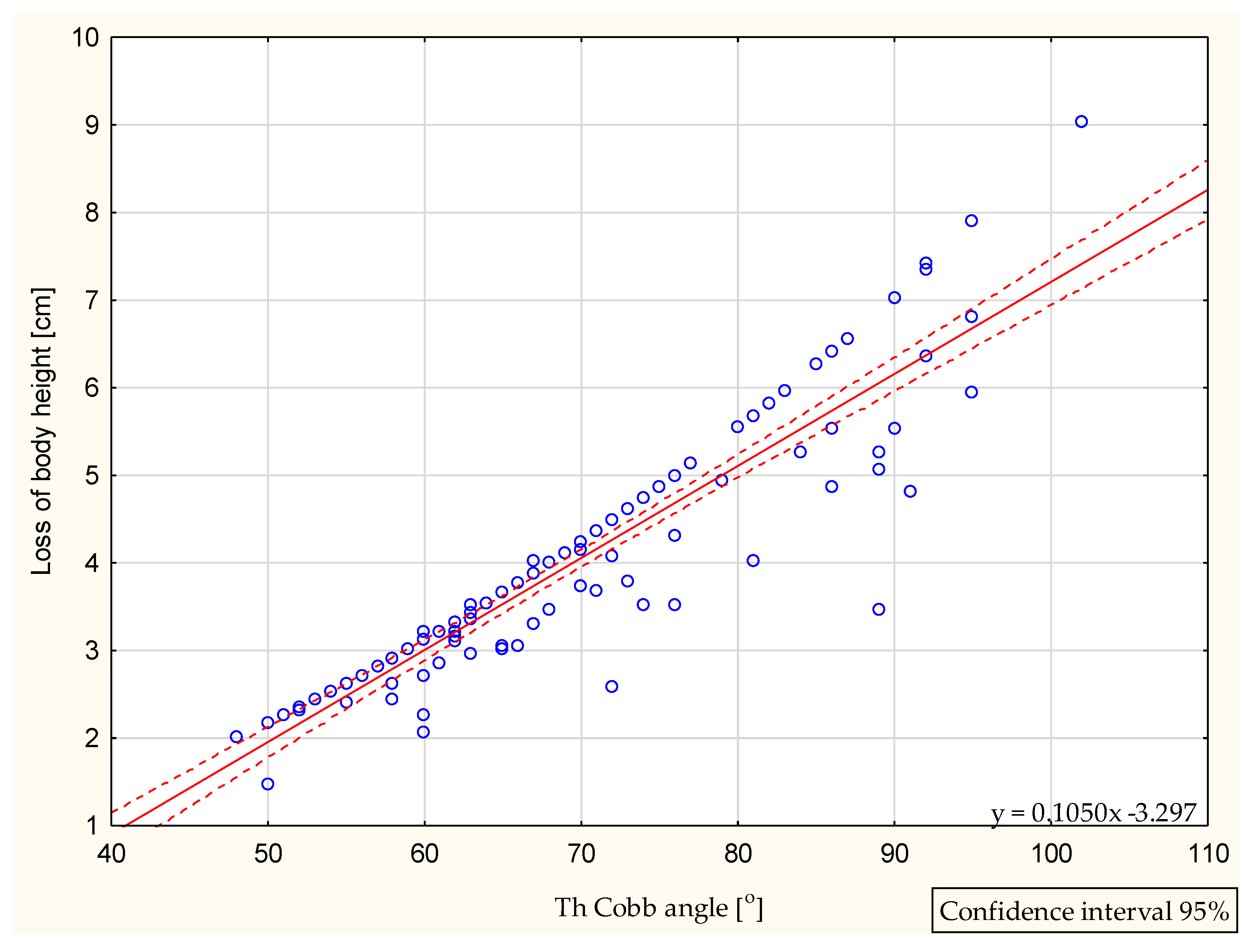
3.1. Cobb Angle Analysis
3.2. Measured versus Corrected Body Height
3.3. Predicted Pulmonary Parameters Calculated for the Measured versus the Corrected Body Height
3.4. Pulmonary Parameters Values Registered at Spirometry Examination
3.5. Comparison of the Pulmonary Parameters in Subgroup I versus Subgroup II
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Subgroup I | Subgroup II | |||||
|---|---|---|---|---|---|---|
| Parameter | FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p-Value | FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p-Value |
| Predicted value (L) | 3.83 ± 0.6 | 4.00 ± 0.6 | p < 0.01 * | 3.82 ± 0.6 | 4.13 ± 0.7 | p < 0.01 * |
| LLN (L) | 3.09 ± 0.5 | 3.23 ± 0.5 | p < 0.01 * | 3.08 ± 0.5 | 3.34 ± 0.6 | p < 0.01 * |
| ULN (L) | 4.59 ± 0.7 | 4.80 ± 0.7 | p < 0.01 * | 4.57 ± 0.7 | 4.95 ± 0.8 | p < 0.01 * |
| FEV1m Measured Body Height | FEV1c Corrected Body Height | FEV1m vs. FEV1c p-Value | FEV1m Measured Body Height | FEV1c Corrected Body Height | FEV1m vs. FEV1c p-Value | |
| Predicted value (L) | 3.36 ± 0.6 | 3.50 ± 0.5 | p < 0.01 * | 3.34 ± 0.5 | 3.59 ± 0.5 | p < 0.01 * |
| LLN (L) | 2.70 ± 0.4 | 2.82 ± 0.5 | p < 0.01 * | 2.69 ± 0.4 | 2.89 ± 0.4 | p < 0.01 * |
| ULN (L) | 4.00 ± 0.7 | 4.17 ± 0.6 | p < 0.01 * | 3.98 ± 0.6 | 4.28 ± 0.6 | p < 0.01 * |
| Subgroup I | Subgroup II | |||||
|---|---|---|---|---|---|---|
| Parameter | FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p-Value | FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p-Value |
| Predicted value (L) | 3.88 ± 0.6 | 4.05 ± 0.6 | p < 0.01 * | 3.74 ± 0.5 | 4.06 ± 0.6 | p < 0.01 * |
| LLN (L) | 3.13 ± 0.5 | 3.27 ± 0.5 | p < 0.01 * | 3.02 ± 0.4 | 3.27 ± 0.5 | p < 0.01 * |
| ULN (L) | 4.65 ± 0.7 | 4.86 ± 0.7 | p < 0.01 * | 4.49 ± 0.6 | 4.87 ± 0.7 | p < 0.01 * |
| FEV1m Measured Body Height | FEV1c Corrected Body Height | FEV1m vs. FEV1c p-Value | FEV1m Measured Body Height | FEV1c Corrected Body Height | FEV1m vs. FEV1c p-Value | |
| Predicted value (L) | 3.40 ± 0.5 | 3.54 ± 0.5 | p < 0.01 * | 3.29 ± 0.4 | 3.55 ± 0.5 | p < 0.01 * |
| LLN (L) | 2.73 ± 0.4 | 2.85 ± 0.4 | p < 0.01 * | 2.65 ± 0.4 | 2.86 ± 0.4 | p < 0.01 * |
| ULN (L) | 4.05 ± 0.6 | 4.21 ± 0.6 | p < 0.01 * | 3.91 ± 0.5 | 4.22 ± 0.6 | p < 0.01 * |
| Subgroup I | Subgroup II | |||||
|---|---|---|---|---|---|---|
| Parameter | FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p-Value | FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p -Value |
| Predicted value (L) | 3.75 ± 0.7 | 3.91 ± 0.7 | p < 0.01 * | 3.92 ± 0.7 | 4.22 ± 0.8 | p < 0.01 * |
| LLN (L) | 3.02 ± 0.5 | 3.15 ± 0.6 | p < 0.01 * | 3.17 ± 0.6 | 3.41 ± 0.6 | p < 0.01 * |
| ULN (L) | 4.50 ± 0.8 | 4.69 ± 0.8 | p < 0.01 * | 4.68 ± 0.8 | 5.04 ± 0.9 | p < 0.01 * |
| FEV1m Measured Body Height | Fev1c Corrected Body Height | FEV1m vs. FEV1c p-Value | FEV1m Measured Body Height | FEV1c Corrected Body Height | FEV1m vs. FEV1c p-Value | |
| Predicted value (L) | 3.30 ± 0.5 | 3.43 ± 0.6 | p < 0.01 * | 3.40 ± 0.6 | 3.64 ± 0.6 | p < 0.01 * |
| LLN (L) | 2.66 ± 0.4 | 2.76 ± 0.4 | p < 0.01 * | 2.73 ± 0.5 | 2.92 ± 0.5 | p < 0.01 * |
| ULN (L) | 3.92 ± 0.6 | 4.09 ± 0.7 | p < 0.01 * | 4.05 ± 0.7 | 4.34 ± 0.7 | p < 0.01 * |
| Subgroup I | Subgroup II | |||||
|---|---|---|---|---|---|---|
| Parameter | FVC 3.07 ± 0.7 L | FVC 2.85 ± 0.8 L | ||||
| FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p−Value | FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p−Value | |
| z-score | −1.69 ± 1.4 | −1.98 ± 1.3 | p < 0.01 * | −2.18 ± 1.6 | −2.67 ± 1.4 | p < 0.01 * |
| %FVC | 80.30 ± 16.0 | 76.89 ± 15.4 | p < 0.01 * | 74.87 ± 17.8 | 69.31 ± 16.8 | p < 0.01 * |
| FEV1 2.67 ± 0.7 L | FEV1 2.41 ± 0.6 L | |||||
| FEV1m Measured Body Height | FEV1c Corrected Body Height | FEV1m vs. FEV1c p-Value | FEV1m Measured Body Height | FEV1c Corrected Body Height | FEV1m vs. FEV1c p-Value | |
| z-score | −1.66 ± 1.8 | −1.92 ± 1.5 | p < 0.01 * | −2.26 ± 1.5 | −2.67 ± 1.4 | p < 0.01 * |
| %FEV1 | 79.90 ± 22.1 | 76.81 ± 17.7 | p < 0.01 * | 72.61 ± 18.9 | 67.56 ± 17.7 | p < 0.01 * |
| Subgroup I | Subgroup II | |||||
|---|---|---|---|---|---|---|
| Parameter | FVC 3.07 ± 0.8 L | FVC 2.95 ± 0.7 L | ||||
| Fvcm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p-Value | FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p-Value | |
| z-score | −1.54 ± 1.3 | −1.84 ± 1.2 | p < 0.01 * | −2.30 ± 1.7 | −2.80 ± 1.6 | p < 0.01 * |
| %FVC | 82.01 ± 14.6 | 78.49 ± 14.0 | p < 0.01 * | 73.41 ± 19.4 | 67.73 ± 18.2 | p < 0.01 * |
| FEV1 2.66 ± 0.7 L | FEV1 2.62 ± 0.6 L | |||||
| FEV1m Measured Body Height | FEV1c Corrected Body Height | FEV1m vs. FEV1c p-Value | FEV1m Measured Body Height | FEV1c Corrected Body Height | FEV1m vs. FEV1c p-Value | |
| z-score | −1.51 ± 1.6 | −1.78 ± 1.2 | p < 0.01 * | −2.48 ± 1.5 | −2.89 ± 1.4 | p < 0.01 * |
| %FEV1 | 81.79 ± 19.3 | 78.51 ± 18.5 | p < 0.01 * | 70.02 ± 18.6 | 64.93 ± 17.6 | p < 0.01 * |
| Subgroup I | Subgroup II | |||||
|---|---|---|---|---|---|---|
| Parameter | FVC 3.07 ± 0.7 L | FVC 2.78 ± 0.7 L | ||||
| FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p-Value | FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p-Value | |
| z-score | −1.96 ± 1.5 | −2.23 ± 1.5 | p < 0.01 * | −2.05 ± 1.4 | −2.5 ± 1.4 | p < 0.01 * |
| %FVC | 77.23 ± 18.2 | 74.02 ± 17.5 | p < 0.01 * | 76.5 ± 16.3 | 71.09 ± 15.3 | p < 0.01 * |
| FEV1 2.59 ± 0.6 L | FEV1 2.32 ± 0.6 L | |||||
| Fev1m Measured Body Height | Fev1c Corrected Body Height | FEV1m vs. FEV1c p-Value | FEV1m Measured Body Height | FEV1c Corrected body height | FEV1m vs. FEV1c p-value | |
| z-score | −1.94 ± 1.4 | −2.18 ± 1.3 | p < 0.01 * | −2.02 ± 1.6 | −2.43 ± 1.5 | p < 0.01 * |
| %FEV1 | 76.77 ± 16.8 | 73.76 ± 16.1 | p < 0.01 * | 75.5 ± 19.3 | 70.49 ± 18.0 | p < 0.01 * |
Appendix B

References
- Weinstein, S.L. Natural history. Spine 1999, 24, 2592–2600. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.L.; Zavala, D.C.; Ponseti, I.V. Idiopathic scoliosis: Long-term follow-up and prognosis in untreated patients. J. Bone Jt. Surg. Am. 1981, 63, 702–712. [Google Scholar] [CrossRef] [Green Version]
- Johnston, C.E.; Richards, B.S.; Sucato, D.J.; Bridwell, K.H.; Lenke, L.G.; Erickson, M.; Spinal Deformity Study Group. Correlation of preoperative deformity magnitude and pulmonary function tests in adolescent idiopathic scoliosis. Spine 2011, 36, 1096–1102. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C.; Viviani, G.R.; Kirkley, A.; Killian, K.J. Factors determining pulmonary function in adolescent idiopathic thoracic scoliosis. Am. Rev. Respir. Dis. 1993, 148, 288–294. [Google Scholar] [CrossRef]
- Newton, P.O.; Faro, F.D.; Gollogly, S.; Betz, R.R.; Lenke, L.G.; Lowe, T.G. Results of preoperative pulmonary function testing of adolescents with idiopathic scoliosis. A study of six hundred and thirty-one patients. J. Bone Jt. Surg. Am. 2005, 87, 1937–1946. [Google Scholar] [CrossRef]
- Kotani, T.; Minami, S.; Takahashi, K.; Isobe, K.; Nakata, Y.; Takaso, M.; Inoue, M.; Maruta, T.; Akazawa, T.; Ueda, T.; et al. An analysis of chest wall and diaphragm motions in patients with idiopathic scoliosis using dynamic breathing MRI. Spine 2004, 29, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Bjure, J.; Grimby, G.; Nachemson, A. Correction of body height in predicting spirometric values in scoliotic patients. Scand. J. Clin. Lab. Investig. 1968, 21, 191–192. [Google Scholar] [CrossRef]
- Kono, K.; Asazuma, T.; Suzuki, N.; Ono, T. Body height correction in scoliosis patients for pulmonary function test. J. Orthop. Surg. 2000, 8, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Ylikoski, M. Height of girls with adolescent idiopathic scoliosis. Eur. Spine J. 2003, 12, 288–291. [Google Scholar] [CrossRef] [Green Version]
- Stokes, I.A. Stature and growth compensation for spinal curvature. Stud. Health Technol. Inform. 2008, 140, 48–51. [Google Scholar]
- Tyrakowski, M.; Kotwicki, T.; Czubak, J.; Siemionow, K. Calculation of corrected body height in idiopathic scoliosis: Comparison of four methods. Eur. Spine J 2014, 23, 1244–1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cobb, J.R. Outline for the study of scoliosis. Instr. Course Lect. 1948, 5, 261–275. [Google Scholar]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.J.; Lenke, L.G.; Bridwell, K.H.; Kim, K.L.; Steger-May, K. Pulmonary function in adolescent idiopathic scoliosis relative to the surgical procedure. J. Bone Jt. Surg. Am. 2005, 87, 1534–1541. [Google Scholar]
- Kim, Y.J.; Lenke, L.G.; Bridwell, K.H.; Cheh, G.; Whorton, J.; Sides, B. Prospective pulmonary function comparison following posterior segmental spinal instrumentation and fusion of adolescent idiopathic scoliosis: Is there a relationship between major thoracic curve correction and pulmonary function test improvement? Spine 2007, 32, 2685–2693. [Google Scholar] [CrossRef] [PubMed]
- Vedantam, R.; Lenke, L.G.; Bridwell, K.H.; Haas, J.; Linville, D.A. A prospective evaluation of pulmonary function in patients with adolescent idiopathic scoliosis relative to the surgical approach used for spinal arthrodesis. Spine 2000, 25, 82–90. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.M.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: The global lung function 2012 equations. Eur. Res. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef]
- Tsiligiannis, T.; Grivas, T. Pulmonary function in children with idiopathic scoliosis. Scoliosis 2012, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- McMaster, M.J.; Glasby, M.A.; Singh, H.; Cunningham, S. Lung function in congenital kyphosis and kyphoscoliosis. J. Spinal Disord. Tech. 2007, 20, 203–208. [Google Scholar] [CrossRef]
- American Thoracic Society. Lung function testing: Selection of reference values and interpretative strategies. Am. Rev. Respir. Dis. 1991, 144, 1202–1218. [Google Scholar] [CrossRef]
- Borowitz, D.; Armstrong, D.; Cerny, F. Relief of central airways obstruction following spinal release in a patient with idiopathic scoliosis. Pediatr. Pulmonol. 2001, 31, 86–88. [Google Scholar] [CrossRef]
- Bartlett, W.; Garrido, E.; Wallis, C.; Tucker, S.K.; Noordeen, H. Lordoscoliosis and large intrathoracic airway obstruction. Spine 2009, 34, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Hepper, N.G.; Black, L.F.; Fowler, W.S. Relationships of lung volume to height and arm span in normal subjects and in patients with spinal deformity. Am. Rev. Respir. Dis. 1965, 91, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Crapo, R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. General considerations for lung function testing. Eur. Respir. J. 2005, 26, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golshan, M.; Crapo, R.O.; Jensen, R.L.; Golshan, R. Arm span as an independent predictor of pulmonary function parameters: Validation and reference values. Respirology 2007, 12, 361–366. [Google Scholar] [CrossRef]
- Johnson, B.E.; Westgate, H.D. Methods of predicting vital capacity in patients with thoracic scoliosis. J. Bone Jt. Surg. Am. 1970, 52, 1433–1439. [Google Scholar] [CrossRef]
- Linderholm, H.; Lindgren, U. Prediction of spirometric values in patients with scoliosis. Acta Orthop. Scand. 1978, 49, 469–474. [Google Scholar] [CrossRef]
- Shi, B.; Mao, S.; Xu, L.; Sun, X.; Liu, Z.; Cheng, J.C.Y.; Zhu, Z.; Qiu, Y. Accurate prediction of height loss in adolescent idiopathic scoliosis: Cobb angle alone is insufficient. Eur. Spine J. 2016, 25, 3341–3346. [Google Scholar] [CrossRef]
- Gardner, A.; Price, A.; Berryman, F.; Pynsent, P. The use of growth standards and corrective formulae to calculate the height loss caused by idiopathic scoliosis. Scoliosis Spinal Disord. 2016, 26, 6. [Google Scholar] [CrossRef] [Green Version]
- Politarczyk, K.; Stępniak, Ł.; Kozinoga, M.; Czaprowski, D.; Kotwicki, T. Loss of the body height due to severe thoracic curvature does impact pulmonary testing results in adolescents with idiopathic scoliosis. Stud. Health Technol. Inform. 2021, 280, 231–234. [Google Scholar]
- Politarczyk, K.; Janusz, P.; Stępniak, Ł.; Kozinoga, M.; Kotwicki, T. Relationship between radiological parameters and preoperative pulmonary function in adolescents with idiopathic scoliosis—Preliminary study. Issue Rehabil. Orthop. Neurophysiol. Sport Promot. 2019, 28, 7–14. [Google Scholar]
- Bates, D.V.; Christie, R.V. Respiratory Function in Disease; Saunders: Philadelphia, PA, USA, 1964; p. 9. [Google Scholar]
- Quanjer, P.H.; Tammeling, G.J.; Cotes, J.E.; Pedersen, O.F.; Peslin, R.; Yernault, J.C. Lung volumes and forced ventilatory flows. Eur. Respir. J. 1993, 6, 5–40. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; van der Grinten, C.P.M.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef] [PubMed]

| Thoracic Cobb Angle Range [°] | Measured Body Height [cm] | Calculated Height Loss [cm] (Stokes) | Calculated Corrected Body Height [cm] | Measured versus Corrected Body Height | |
|---|---|---|---|---|---|
| Lenke 1 and 3 types | |||||
| Subgroup I and II N = 120 | 48–102 | 164.9 ± 7.9 (145.0–185.0) | 3.9 ± 1.4 (1.5–9.0) | 168.8 ± 8.0 (151.3–188.5) | p < 0.01 * |
| Subgroup I N = 84 | 48–74 | 164.9 ± 7.9 (148.0–184.0) | 3.1 ± 0.7 (1.5–4.7) | 168.0 ± 7.8 (151.2–187.5) | p = 0.01 * |
| Subgroup II N = 36 | 75–102 | 165.0 ± 8.1 (145.0–185.0) | 5.7 ± 1.2 (3.5–9.0) | 170.7 ± 8.2 (151.3–188.5) | p = 0.004 * |
| Lenke 1 type | |||||
| Subgroup I and II N = 73 | 48–102 | 165.1 ± 7.7 (145–184) | 3.9 ± 1.4 (2.0–9.0) | 169.0 ± 7.7 (151.2–188.0) | p < 0.01 * |
| Subgroup I N = 54 | 48–74 | 165.5 7 ± 9 (151.0–184.0) | 3.2 ± 0.7 (2.0–4.7) | 168.6 ± 7.8 (153.3–187.2) | p < 0.01 * |
| Subgroup II N = 19 | 75–102 | 163.9 ± 7.2 (145.0–182.0) | 5.9 ± 1.0 (4.8–9.0) | 169.9 ± 7.2 (151.2–188.0) | p < 0.01 * |
| Lenke 3 type | |||||
| Subgroup I and II N = 47 | 50–95 | 164.7 ± 8.3 (148.0–185.0) | 3.9 ± 1.4 (1.5–7.9) | 168.6 ± 8.6 (151.5–188.5) | p < 0.01 * |
| Subgroup I N = 30 | 50–74 | 163.8 ± 7.8 (148.0–184.0) | 3.1 ± 0.6 (1.46–4.1) | 166.9 ± 7.8 (151.5–187.5) | p < 0.01 * |
| Subgroup II N = 17 | 76–95 | 166.3 ± 9.0 (149.0–185) | 5.3 ± 1.2 (3.5–7.9) | 171.6 ± 9.3 (152.5–189.6) | p < 0.01 * |
| Parameter | FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p-Value |
|---|---|---|---|
| Predicted value [L] | 3.83 ± 0.6 | 4.04 ± 0.7 | p < 0.01 * |
| LLN [L] | 3.09 ± 0.5 | 3.26 ± 0.5 | p < 0.01 * |
| ULN [L] | 4.59 ± 0.7 | 4.84 ± 0.8 | p < 0.01 * |
| FEV1m Measured Body Height | FEV1c Corrected Body Height | FEV1m vs. FEV1c p-Value | |
| Predicted value [L] | 3.36 ± 0.51 | 3.53 ± 0.53 | p < 0.01 * |
| LLN [L] | 2.70 ± 0.41 | 2.84 ± 0.42 | p < 0.01 * |
| ULN [L] | 4.00 ± 0.6 | 4.20 ± 0.6 | p < 0.01 * |
| Parameter | FVC 3.00 ± 0.8 L | ||
|---|---|---|---|
| FVCm Measured Body Height | FVCc Corrected Body Height | FVCm vs. FVCc p-Value | |
| z-score | −1.83 ± 1.4 | −2.19 ± 1.4 | p < 0.01 * |
| %FVC | 78.67 ± 16.7 | 74.62 ± 16.1 | p < 0.01 * |
| FEV1 2.59 ± 0.7 L | |||
| FEV1m Measured Body Height | FEV1c Corrected Body Height | FEV1m vs. FEV1c p-Value | |
| z-score | −1.84 ± 1.6 | −2.15 ± 1.5 | p < 0.01 * |
| %FEV1 | 77.78 ± 18.7 | 74.03 ± 18.2 | p < 0.01 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Politarczyk, K.; Kozinoga, M.; Stępniak, Ł.; Panieński, P.; Kotwicki, T. Spirometry Examination of Adolescents with Thoracic Idiopathic Scoliosis: Is Correction for Height Loss Useful? J. Clin. Med. 2021, 10, 4877. https://doi.org/10.3390/jcm10214877
Politarczyk K, Kozinoga M, Stępniak Ł, Panieński P, Kotwicki T. Spirometry Examination of Adolescents with Thoracic Idiopathic Scoliosis: Is Correction for Height Loss Useful? Journal of Clinical Medicine. 2021; 10(21):4877. https://doi.org/10.3390/jcm10214877
Chicago/Turabian StylePolitarczyk, Katarzyna, Mateusz Kozinoga, Łukasz Stępniak, Paweł Panieński, and Tomasz Kotwicki. 2021. "Spirometry Examination of Adolescents with Thoracic Idiopathic Scoliosis: Is Correction for Height Loss Useful?" Journal of Clinical Medicine 10, no. 21: 4877. https://doi.org/10.3390/jcm10214877