
Clinical Efficacy of Ruxolitinib in Patients with Myelofibrosis: A Nationwide Population-Based Study in Korea

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
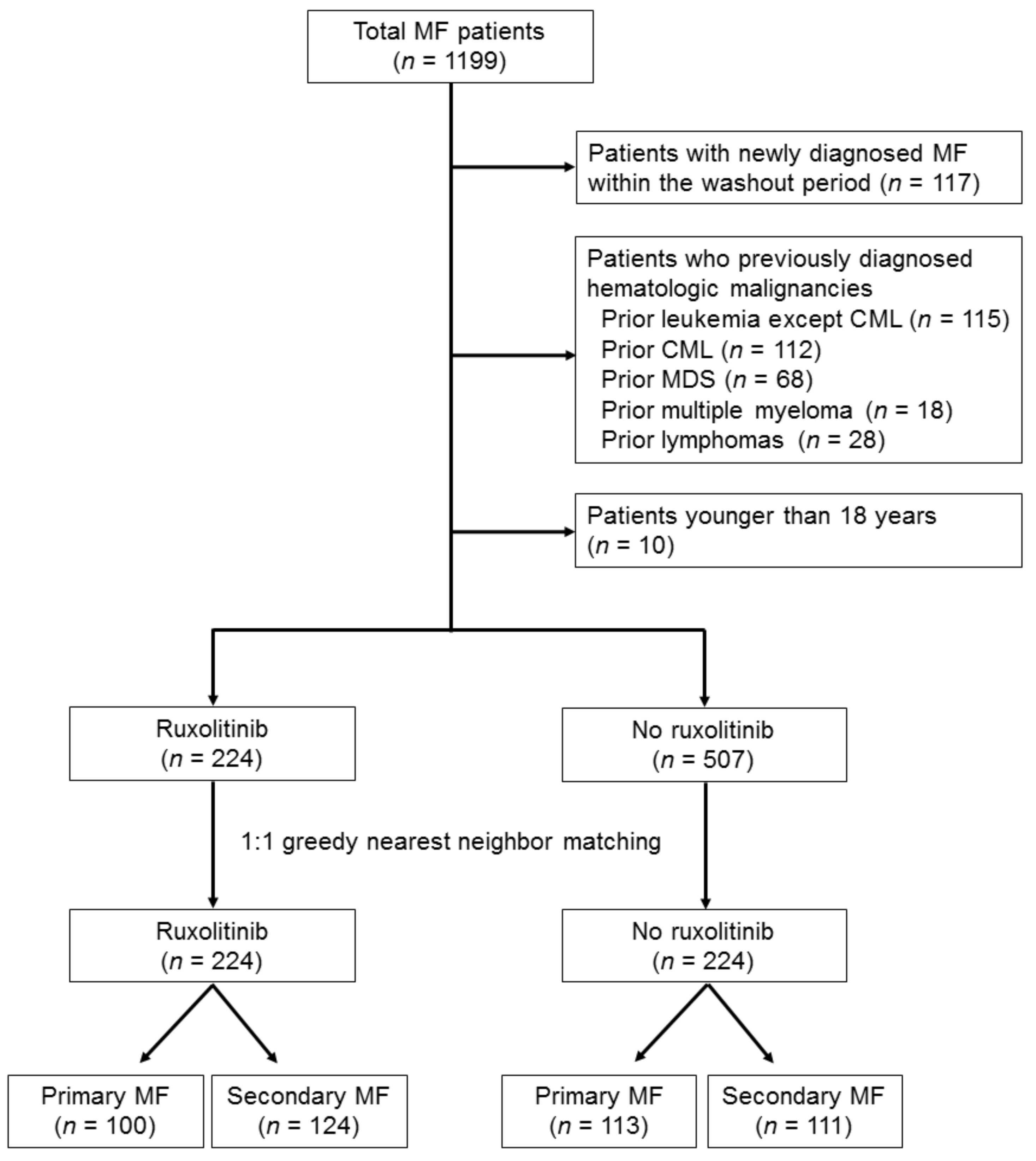
2.2. Patient Selection
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Study Polulation
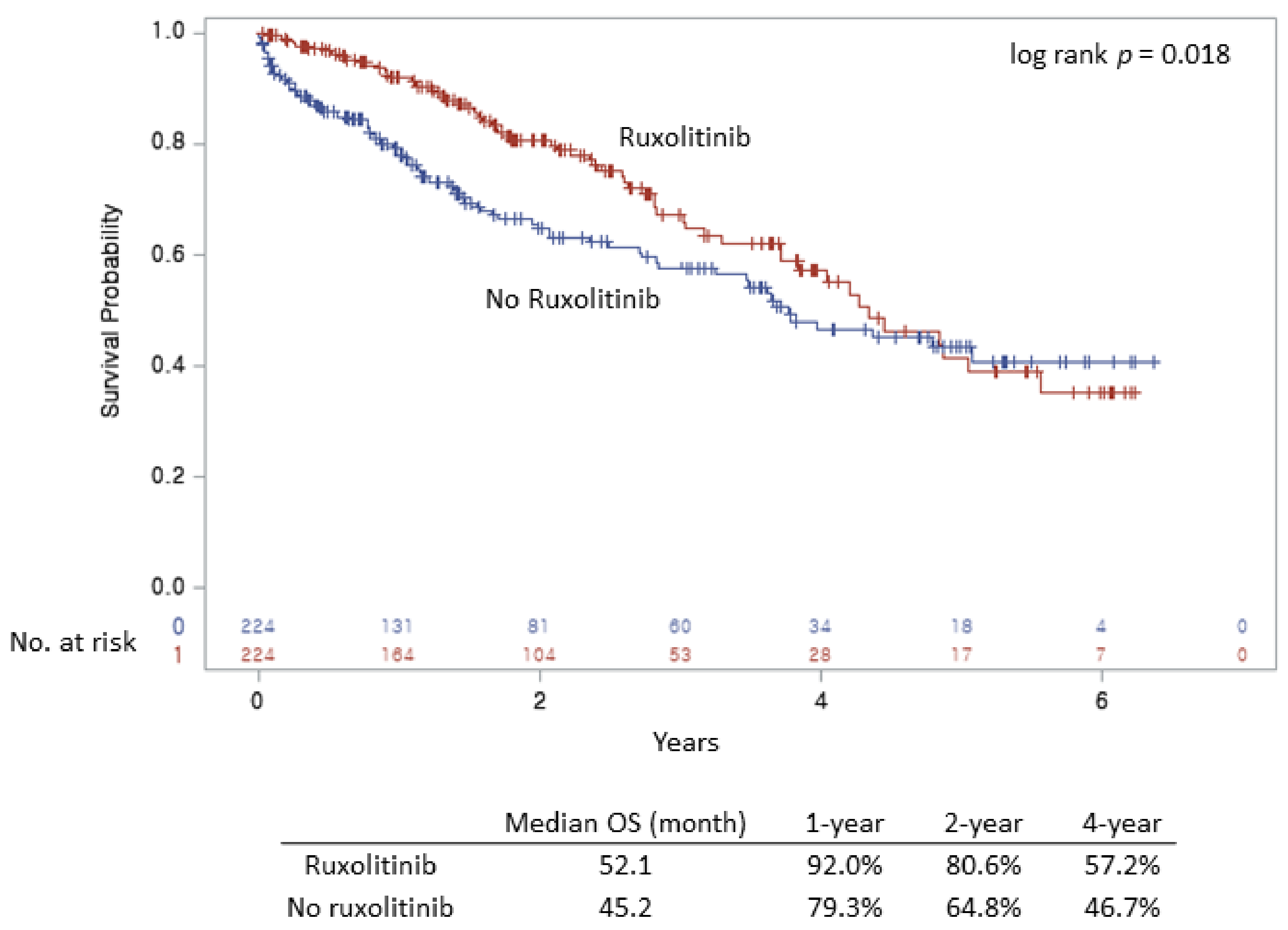
3.2. Clinical Outcomes Based on Ruxolitinib Treatment
3.3. Subgroup Analysis in Patients Treated with Ruxolitinib
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tefferi, A.; Nicolosi, M.; Mudireddy, M.; Lasho, T.L.; Gangat, N.; Begna, K.H.; Hanson, C.A.; Ketterling, R.P.; Pardanani, A. Revised cytogenetic risk stratification in primary myelofibrosis: Analysis based on 1002 informative patients. Leukemia 2018, 32, 1189–1199. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.; Aldoss, I.; Yang, D.; Mokhtari, S.; Khaled, S.; Aribi, A.; Afkhami, M.; Al Malki, M.M.; Cao, T.; Mei, M.; et al. MIPSS70+ v2.0 predicts long-term survival in myelofibrosis after allogeneic HCT with the Flu/Mel conditioning regimen. Blood Adv. 2019, 3, 83–95. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.; Lee, J.-O.; Bang, S.-M. Incidence, Survival and Prevalence Statistics of Classical Myeloproliferative Neoplasm in Korea. J. Korean Med. Sci. 2016, 31, 1579–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mascarenhas, J.; Hoffman, R. Ruxolitinib: The first FDA approved therapy for the treatment of myelofibrosis. Clin. Cancer Res. 2012, 18, 3008–3014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massaro, F.; Molica, M.; Breccia, M. How ruxolitinib modified the outcome in myelofibrosis: Focus on overall survival, allele burden reduction and fibrosis changes. Expert Rev. Hematol. 2017, 10, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Verstovsek, S.; Mesa, R.A.; Gotlib, J.; Levy, R.S.; Gupta, V.; DiPersio, J.F.; Catalano, J.V.; Deininger, M.; Miller, C.; Silver, R.T.; et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N. Engl. J. Med. 2012, 366, 799–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, C.; Kiladjian, J.J.; Al-Ali, H.K.; Gisslinger, H.; Waltzman, R.; Stalbovskaya, V.; McQuitty, M.; Hunter, D.S.; Levy, R.; Knoops, L.; et al. JAK inhibition with ruxolitinib versus best available therapy for myelofibrosis. N. Engl. J. Med. 2012, 366, 787–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verstovsek, S.; Mesa, R.A.; Gotlib, J.; Levy, R.S.; Gupta, V.; DiPersio, J.F.; Catalano, J.V.; Deininger, M.W.; Miller, C.B.; Silver, R.T.; et al. Efficacy, safety, and survival with ruxolitinib in patients with myelofibrosis: Results of a median 3-year follow-up of COMFORT-I. Haematologica 2015, 100, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Cervantes, F.; Vannucchi, A.M.; Kiladjian, J.J.; Al-Ali, H.K.; Sirulnik, A.; Stalbovskaya, V.; McQuitty, M.; Hunter, D.S.; Levy, R.S.; Passamonti, F.; et al. Three-year efficacy, safety, and survival findings from COMFORT-II, a phase 3 study comparing ruxolitinib with best available therapy for myelofibrosis. Blood 2013, 122, 4047–4053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, C.N.; Vannucchi, A.M.; Kiladjian, J.J.; Al-Ali, H.K.; Gisslinger, H.; Knoops, L.; Cervantes, F.; Jones, M.M.; Sun, K.; McQuitty, M.; et al. Long-term findings from COMFORT-II, a phase 3 study of ruxolitinib vs. best available therapy for myelofibrosis. Leukemia 2016, 30, 1701–1707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verstovsek, S.; Gotlib, J.; Mesa, R.A.; Vannucchi, A.M.; Kiladjian, J.J.; Cervantes, F.; Harrison, C.N.; Paquette, R.; Sun, W.; Naim, A.; et al. Long-term survival in patients treated with ruxolitinib for myelofibrosis: COMFORT-I and -II pooled analyses. J. Hematol. Oncol. 2017, 10, 156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervantes, F.; Pereira, A. Does ruxolitinib prolong the survival of patients with myelofibrosis? Blood 2017, 129, 832–837. [Google Scholar] [CrossRef] [PubMed]
- Marti-Carvajal, A.J.; Anand, V.; Sola, I. Janus kinase-1 and Janus kinase-2 inhibitors for treating myelofibrosis. Cochrane Database Syst. Rev. 2015, CD010298. [Google Scholar] [CrossRef] [PubMed]
- Verstovsek, S.; Mesa, R.A.; Gotlib, J.; Gupta, V.; DiPersio, J.F.; Catalano, J.V.; Deininger, M.W.; Miller, C.B.; Silver, R.T.; Talpaz, M.; et al. Long-term treatment with ruxolitinib for patients with myelofibrosis: 5-year update from the randomized, double-blind, placebo-controlled, phase 3 COMFORT-I trial. J. Hematol. Oncol. 2017, 10, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangle, N.; Cook, J.; Perkins, S.; Teman, C.J.; Bahler, D.; Hickman, K.; Wilson, A.; Prchal, J.; Salama, M.E. Myelofibrotic transformations of polycythemia vera and essential thrombocythemia are morphologically, biologically, and prognostically indistinguishable from primary myelofibrosis. Appl. Immunohistochem. Mol. Morphol. 2014, 22, 663–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masarova, L.; Bose, P.; Daver, N.; Pemmaraju, N.; Newberry, K.J.; Manshouri, T.; Cortes, J.; Kantarjian, H.M.; Verstovsek, S. Patients with post-essential thrombocythemia and post-polycythemia vera differ from patients with primary myelofibrosis. Leuk. Res. 2017, 59, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Gowin, K.; Coakley, M.; Kosiorek, H.; Mesa, R. Discrepancies of applying primary myelofibrosis prognostic scores for patients with post polycythemia vera/essential thrombocytosis myelofibrosis. Haematologica 2016, 101, e405–e406. [Google Scholar] [CrossRef] [Green Version]
- Passamonti, F.; Giorgino, T.; Mora, B.; Guglielmelli, P.; Rumi, E.; Maffioli, M.; Rambaldi, A.; Caramella, M.; Komrokji, R.; Gotlib, J.; et al. A clinical-molecular prognostic model to predict survival in patients with post polycythemia vera and post essential thrombocythemia myelofibrosis. Leukemia 2017, 31, 2726–2731. [Google Scholar] [CrossRef] [PubMed]
- Breccia, M.; Andriani, A.; Montanaro, M.; Abruzzese, E.; Buccisano, F.; Cedrone, M.; Centra, A.; Villiva, N.; Celesti, F.; Trawinska, M.M.; et al. Ruxolitinib in clinical practice for primary and secondary myelofibrosis: An analysis of safety and efficacy of Gruppo Laziale of Ph-negative MPN. Ann. Hematol. 2017, 96, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Tefferi, A. Primary myelofibrosis: 2019 update on diagnosis, risk-stratification and management. Am. J. Hematol. 2018, 93, 1551–1560. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| before Matching (n = 731) | after Matching (n = 426) | |||||
|---|---|---|---|---|---|---|
| No Ruxolitinib (n = 509) | Ruxolitinib (n = 224) | p | No Ruxolitinib (n = 224) | Ruxolitinib (n = 224) | p | |
| Age, years | <0.001 a | 0.192 c | ||||
| Mean (SD) | 60.8 (16.1) | 66.0 (11.1) | 66.9 (12.3) | 66.0 (11.1) | ||
| Median (min, max) | 63.0 (18.0, 92.0) | 68.0 (28.0, 88.0) | 68.5 (25.0, 92.0) | 68.0 (28.0, 88.0) | ||
| Sex, n (%) | 0.889 b | 0.729 d | ||||
| Male | 288 (56.8) | 126 (56.3) | 123 (54.9) | 126 (56.3) | ||
| Female | 219 (43.2) | 98 (43.7) | 101 (45.1) | 98 (43.7) | ||
| Thrombotic complications, n (%) | 0.037 b | 0.670 d | ||||
| Yes | 245 (48.3) | 127 (56.7) | 131 (58.5) | 127 (56.7) | ||
| No | 262 (51.7) | 97 (43.3) | 93 (41.5) | 97 (43.3) | ||
| RBC transfusion dependency, n (%) | 0.208 b | 1.000 d | ||||
| Yes | 121 (23.9) | 44 (19.6) | 44 (19.6) | 44 (19.6) | ||
| No | 386 (76.1) | 180 (80.4) | 180 (80.4) | 180 (80.4) | ||
| PLT transfusion dependency, n (%) | <0.001 b | 1.000 d | ||||
| Yes | 45 (8.9) | 1 (0.5) | 1 (0.5) | 1 (0.5) | ||
| No | 462 (91.1) | 223 (99.5) | 223 (99.5) | 223 (99.5) | ||
| Prior hydroxyurea treatment, n (%) | <0.001 b | 0.251 d | ||||
| Yes | 131 (25.8) | 110 (49.1) | 105 (46.9) | 110 (49.1) | ||
| No | 376 (74.2) | 114 (50.9) | 119 (53.1) | 114 (50.9) | ||
| Unmatched | Propensity Score Matched | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | No. of Events | HR | 95% CI | p | p for Interaction | n | No. of Events | HR | 95% CI | p | p for Interaction | |
| Overall | ||||||||||||
| No ruxolitinib | 507 | 165 | 1.00 | 224 | 83 | 1.00 | ||||||
| Ruxolitinib | 224 | 63 | 0.75 | 0.56–1.01 | 0.058 | 224 | 63 | 0.67 | 0.49–0.93 | 0.017 | ||
| 0.881 | 0.104 | |||||||||||
| Primary MF | ||||||||||||
| No ruxolitinib | 291 | 99 | 1.00 | 113 | 52 | 1.00 | ||||||
| Ruxolitinib | 100 | 32 | 0.78 | 0.54–1.14 | 0.198 | 100 | 32 | 0.53 | 0.35–0.81 | 0.003 | ||
| Secondary MF | ||||||||||||
| No ruxolitinib | 216 | 66 | 1.00 | 111 | 31 | 1.00 | ||||||
| Ruxolitinib | 124 | 31 | 0.75 | 0.50–1.12 | 0.169 | 124 | 31 | 0.91 | 0.55–1.52 | 0.729 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, B.-H.; Moon, H.; Chae, J.-E.; Kang, K.-W.; Kim, B.-S.; Lee, J.; Park, Y. Clinical Efficacy of Ruxolitinib in Patients with Myelofibrosis: A Nationwide Population-Based Study in Korea. J. Clin. Med. 2021, 10, 4774. https://doi.org/10.3390/jcm10204774
Lee B-H, Moon H, Chae J-E, Kang K-W, Kim B-S, Lee J, Park Y. Clinical Efficacy of Ruxolitinib in Patients with Myelofibrosis: A Nationwide Population-Based Study in Korea. Journal of Clinical Medicine. 2021; 10(20):4774. https://doi.org/10.3390/jcm10204774
Chicago/Turabian StyleLee, Byung-Hyun, Hyemi Moon, Jae-Eun Chae, Ka-Won Kang, Byung-Soo Kim, Juneyoung Lee, and Yong Park. 2021. "Clinical Efficacy of Ruxolitinib in Patients with Myelofibrosis: A Nationwide Population-Based Study in Korea" Journal of Clinical Medicine 10, no. 20: 4774. https://doi.org/10.3390/jcm10204774