Evaluation of the Efficacy of Immersive Virtual Reality Therapy as a Method Supporting Pulmonary Rehabilitation: A Randomized Controlled Trial



Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Measures
2.2.1. Perception of Stress Questionnaire
2.2.2. Hospital Anxiety and Depression Scale
2.2.3. Functional Capacity
2.3. Instruments
2.4. Procedure
2.5. Statistical Analysis
3. Results
3.1. Evaluation of Stress Levels
3.2. Evaluation of Depression and Anxiety
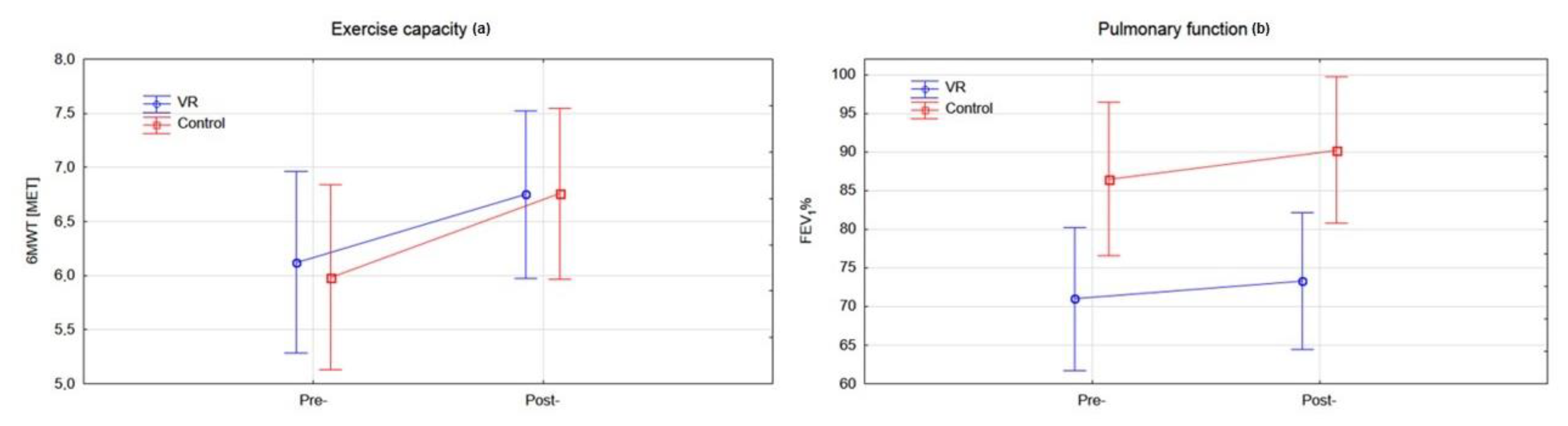
3.3. Evaluation of Functional Capacity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Lopez-Campos, J.L.; Tan, W.; Soriano, J.B. Global burden of COPD. Respirology 2016, 21, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Park, M.A.; Park, M.J.; Jo, Y.S. Clinical characteristics and related risk factors of depression in patients with early COPD. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 1583–1590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matte, D.L.; Pizzichini, M.M.; Hoepers, A.T.; Diaz, A.P.; Karloh, M.; Dias, M.; Pizzichini, E. Prevalence of depression in COPD: A systematic review and meta-analysis of controlled studies. Respir. Med. 2016, 117, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Pollok, J.; van Agteren, J.E.; Esterman, A.J.; Carson-Chahhoud, K.V. Psychological therapies for the treatment of depression in chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2019, 3, CD012347. [Google Scholar] [CrossRef]
- Li, Z.; Liu, S.; Wang, L.; Smith, L. Mind-Body Exercise for Anxiety and Depression in COPD Patients: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 17, 22. [Google Scholar] [CrossRef] [Green Version]
- Panagioti, M.; Scott, C.; Blakemore, A.; Coventry, P.A. Overview of the prevalence, impact, and management of depression and anxiety in chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 1289–1306. [Google Scholar] [CrossRef] [Green Version]
- Tselebis, A.; Pachi, A.; Ilias, I.; Kosmas, E.; Bratis, D.; Moussas, G.; Tzanakis, N. Strategies to improve anxiety and depression in patients with COPD: A mental health perspective. Neuropsychiatr. Dis. Treat. 2016, 12, 297–328. [Google Scholar] [CrossRef] [Green Version]
- Gordon, C.S.; Waller, J.W.; Cook, R.M.; Cavalera, S.L.; Lim, W.T.; Osadnik, C.R. Effect of Pulmonary Rehabilitation on Symptoms of Anxiety and Depression in COPD: A Systematic Review and Meta-Analysis. Chest 2019, 156, 80–91. [Google Scholar] [CrossRef]
- McCarthy, B.; Casey, D.; Devane, D.; Murphy, K.; Murphy, E.; Lacasse, Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2015, CD003793. [Google Scholar] [CrossRef]
- Wiles, L.; Cafarella, P.; Williams, M.T. Exercise training combined with psychological interventions for people with chronic obstructive pulmonary disease. Respirology 2015, 20, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Guell, R.; Resqueti, V.; Sangenis, M.; Morante, F.; Martorell, B.; Casan, P.; Guyatt, G.H. Impact of pulmonary rehabilitation on psychosocial morbidity in patients with severe COPD. Chest 2006, 129, 899–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fodor, L.A.; Cotet, C.D.; Cuijpers, P.; Szamoskozi, S.; David, D.; Cristea, I.A. The effectiveness of virtual reality based interventions for symptoms of anxiety and depression: A meta-analysis. Sci. Rep. 2018, 8, 10323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plopa, M.; Makarowski, R. The Perception of Stress Questionnaire; VIZJA Press&IT: Warsaw, Poland, 2010. [Google Scholar]
- Mihalca, A.M.; Pilecka, W. The factorial structure and validity of the Hospital Anxiety and Depression Scale (HADS) in Polish adolescents. Psychiatr. Pol. 2015, 49, 1071–1088. [Google Scholar] [CrossRef]
- Singh, S.J.; Puhan, M.A.; Andrianopoulos, V.; Hernandes, N.A.; Mitchell, K.E.; Hill, C.J.; Lee, A.L.; Camillo, C.A.; Troosters, T.; Spruit, M.A.; et al. An official systematic review of the European Respiratory Society/American Thoracic Society: Measurement properties of field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1447–1478. [Google Scholar] [CrossRef]
- Geidl, W.; Carl, J.; Cassar, S.; Lehbert, N.; Mino, E.; Wittmann, M.; Wagner, R.; Schultz, K.; Pfeifer, K. Physical Activity and Sedentary Behaviour Patterns in 326 Persons with COPD before Starting a Pulmonary Rehabilitation: A Cluster Analysis. J. Clin. Med. 2019, 8, 1346. [Google Scholar] [CrossRef] [Green Version]
- Viljanen, A. Reference values for spirometric, pulmonary diffusing capacity and body plethysmographic studies. Scand. J. Clin. Investig. 1982, 42, 1–50. [Google Scholar]
- Mazurek, J.; Kiper, P.; Cieslik, B.; Rutkowski, S.; Mehlich, K.; Turolla, A.; Szczepanska-Gieracha, J. Virtual reality in medicine: A brief overview and future research directions. Hum. Mov. 2019, 20, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Rutkowski, S.; Rutkowska, A.; Kiper, P.; Jastrzebski, D.; Racheniuk, H.; Turolla, A.; Szczegielniak, J.; Casaburi, R. Virtual Reality Rehabilitation in Patients with Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial. Int. J. Chronic Obstr. 2020, 15, 117–124. [Google Scholar] [CrossRef] [Green Version]
- Morris, S.B. Estimating effect sizes from pretest-posttest-control group designs. Organ. Res. Methods 2008, 11, 364–386. [Google Scholar] [CrossRef]
- Cohen, D. Statistical Power Analysis for the Behavioral Sciences. Routledge 1988. [Google Scholar] [CrossRef]
- Gaggioli, A.; Pallavicini, F.; Morganti, L.; Serino, S.; Scaratti, C.; Briguglio, M.; Crifaci, G.; Vetrano, N.; Giulintano, A.; Bernava, G.; et al. Experiential virtual scenarios with real-time monitoring (interreality) for the management of psychological stress: A block randomized controlled trial. J. Med. Internet Res. 2014, 16, e167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, T.; Moorhouse, N.; Shi, X.; Amin, M.F. A Virtual Reality-Supported Intervention for Pulmonary Rehabilitation of Patients With Chronic Obstructive Pulmonary Disease: Mixed Methods Study. J. Med. Internet Res. 2020, 22, e14178. [Google Scholar] [CrossRef] [PubMed]
- Coventry, P.A.; Bower, P.; Keyworth, C.; Kenning, C.; Knopp, J.; Garrett, C.; Hind, D.; Malpass, A.; Dickens, C. The effect of complex interventions on depression and anxiety in chronic obstructive pulmonary disease: Systematic review and meta-analysis. PLoS ONE 2013, 8, e60532. [Google Scholar] [CrossRef] [PubMed]
- Moreno, A.; Wall, K.J.; Thangavelu, K.; Craven, L.; Ward, E.; Dissanayaka, N.N. A systematic review of the use of virtual reality and its effects on cognition in individuals with neurocognitive disorders. Alzheimers Dement. (N. Y.) 2019, 5, 834–850. [Google Scholar] [CrossRef]
- Won, A.S.; Bailey, J.; Bailenson, J.; Tataru, C.; Yoon, I.A.; Golianu, B. Immersive Virtual Reality for Pediatric Pain. Children 2017, 4, 52. [Google Scholar] [CrossRef] [Green Version]
- Tennant, M.; Youssef, G.J.; McGillivray, J.; Clark, T.J.; McMillan, L.; McCarthy, M.C. Exploring the use of Immersive Virtual Reality to enhance Psychological Well-Being in Pediatric Oncology: A pilot randomized controlled trial. Eur. J. Oncol. Nurs. 2020, 48, 101804. [Google Scholar] [CrossRef]
- Spruit, M.A.; Holland, A.E.; Singh, S.J.; Tonia, T.; Wilson, K.C.; Troosters, T. COVID-19: Interim Guidance on Rehabilitation in the Hospital and Post-Hospital Phase from a European Respiratory Society and American Thoracic Society-coordinated International Task Force. Eur. Respir. J. 2020. [Google Scholar] [CrossRef]
- Zandifar, A.; Badrfam, R.; Yazdani, S.; Arzaghi, S.M.; Rahimi, F.; Ghasemi, S.; Khamisabadi, S.; Mohammadian Khonsari, N.; Qorbani, M. Prevalence and severity of depression, anxiety, stress and perceived stress in hospitalized patients with COVID-19. J. Diabetes Metab. Disord. 2020, 1–8. [Google Scholar] [CrossRef]
- Taquet, M.; Luciano, S.; Geddes, J.R.; Harrison, P.J. Bidirectional associations between COVID-19 and psychiatric disorder: Retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry 2020. [Google Scholar] [CrossRef]
- Paz, C.; Mascialino, G.; Adana-Diaz, L.; Rodriguez-Lorenzana, A.; Simbana-Rivera, K.; Gomez-Barreno, L.; Troya, M.; Paez, M.I.; Cardenas, J.; Gerstner, R.M.; et al. Anxiety and depression in patients with confirmed and suspected COVID-19 in Ecuador. Psychiatry Clin. Neurosci. 2020, 74, 554–555. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | VR Group | Control Group | p |
|---|---|---|---|
| Age (years), mean (SD) | 64.4 (5.7) | 67.6 (9.4) | 0.156 |
| Female, n (%) | 21 (84%) | 20 (80%) | 0.719 |
| Body mass (kg), mean (SD) | 77.3 (13.5) | 73.8 (13.5) | 0.355 |
| Body high (cm), mean (SD) | 162.3 (7.1) | 164.1 (8.7) | 0.436 |
| BMI, mean (SD) | 29.7 (5.3) | 27.4 (3.8) | 0.078 |
| Time of tobacco consumption (years), mean (SD) | 13.0 (17.0) | 10.8 (13.0) | 0.619 |
| FEV1 pred., mean (SD) | 71.0 (23.7) | 86.5 (21.1) | 0.047 |
| 6MWT (MET), mean (SD) | 6.12 (1.97) | 5.98 (1.84) | 0.617 |
| Highest educational level, n (%) | p* | ||
| High school | 5 (20%) | 4 (16%) | 0.677 |
| College | 14 (56%) | 14 (56%) | |
| University | 6 (24%) | 7 (28%) | |
| Material status, n(%) | |||
| Married/cohabiting | 12 (48%) | 14 (56%) | 0.794 |
| Divorced/widowed | 13 (52%) | 9 (36%) | |
| Single | 0 | 2 (8%) | |
| Employment status, n (%) | |||
| Professionally active | 5 (20%) | 5 (20%) | 0.803 |
| Retired | 20 (80%) | 20 (80%) | |
| Subjective health status judgement, n (%) | |||
| Good | 3 (12%) | 7 (28%) | 0.344 |
| Neutral | 18 (72%) | 14 (56%) | |
| Bad | 4 (16%) | 4 (16%) | |
| Voluntary physical activity, n (%) | |||
| Often | 13 (52%) | 15 (60%) | 0.507 |
| Occasionally | 11 (44%) | 10 (40%) | |
| None | 1 (4%) | 0 |
| Variable | VR Group | Control Group | Effect Size | ||||
|---|---|---|---|---|---|---|---|
| Pre | Post | p | Pre | Post | p | ||
| Emotional tension | 24.68 (6.12) | 21.24 (6.03) | 0.0003 | 22.44 (5.77) | 21.28 (5.99) | 0.1998 | −0.377 |
| External stress | 19.24 (6.65) | 17.12 (5.21) | 0.0092 | 16.40 (4.71) | 16.76 (4.77) | 0.6470 | −0.424 |
| Intrapsychic stress | 20.48 (5.85) | 19.96 (5.78) | 0.6356 | 17.52 (6.47) | 17.76 (6.39) | 0.8267 | −0.121 |
| PSQ Total score | 64.40 (15.88) | 58.32 (15.29) | 0.0069 | 56.36 (14.91) | 55.80 (14.19) | 0.7961 | −0.353 |
| HADS-D mean (SD) | 7.96 (2.76) | 6.04 (3.21) | 0.0001 | 6.64 (2.80) | 7.08 (3.56) | 0.4515 | −0.836 |
| HADS-A mean (SD) | 10.36 (3.63) | 8.24 (3.50) | 0.0009 | 8.52 (3.22) | 8.60 (2.87) | 0.8941 | 0.631 |
| HADS Total score | 18.32 (4.90) | 13.24 (4.05) | 0.0001 | 15.16 (4.47) | 15.68 (5.29) | 0.6119 | −1.175 |
| 6MWT [MET], mean (SD) | 6.12 (2.12) | 6.75 (2.24) | 0.0018 | 5.98 (1.84) | 6.76 (1.28) | 0.0002 | −0.074 |
| FEV1 [%], mean (SD) | 71.00 (23.66) | 73.25 (23.24) | 0.1893 | 86.48 (21.13) | 90.24 (19.36) | 0.0429 | −0.066 |
| Determinant | Multiple Regression Model for Exercise Time R2 = 0.12, p < 0.00289 | |
|---|---|---|
| Standardized Beta Coefficient | p-Value | |
| 6MWT | −1.62 | <0.043 |
| FEV1 | −0.17 | <0.010 |
| Determinant | Multiple Regression Model for Exercise Time R2 = 0.06, p < 0.019 | |
|---|---|---|
| Standardized Beta Coefficient | p-Value | |
| FEV1 | −2.44 | <0.0189 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rutkowski, S.; Szczegielniak, J.; Szczepańska-Gieracha, J. Evaluation of the Efficacy of Immersive Virtual Reality Therapy as a Method Supporting Pulmonary Rehabilitation: A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 352. https://doi.org/10.3390/jcm10020352
Rutkowski S, Szczegielniak J, Szczepańska-Gieracha J. Evaluation of the Efficacy of Immersive Virtual Reality Therapy as a Method Supporting Pulmonary Rehabilitation: A Randomized Controlled Trial. Journal of Clinical Medicine. 2021; 10(2):352. https://doi.org/10.3390/jcm10020352
Chicago/Turabian StyleRutkowski, Sebastian, Jan Szczegielniak, and Joanna Szczepańska-Gieracha. 2021. "Evaluation of the Efficacy of Immersive Virtual Reality Therapy as a Method Supporting Pulmonary Rehabilitation: A Randomized Controlled Trial" Journal of Clinical Medicine 10, no. 2: 352. https://doi.org/10.3390/jcm10020352