Outcomes of Intra- versus Extra-Corporeal Ileocolic Anastomosis after Minimally Invasive Right Colectomy for Cancer: An Observational Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Surgical Technique
2.3. Variables
2.4. Statistical Methods
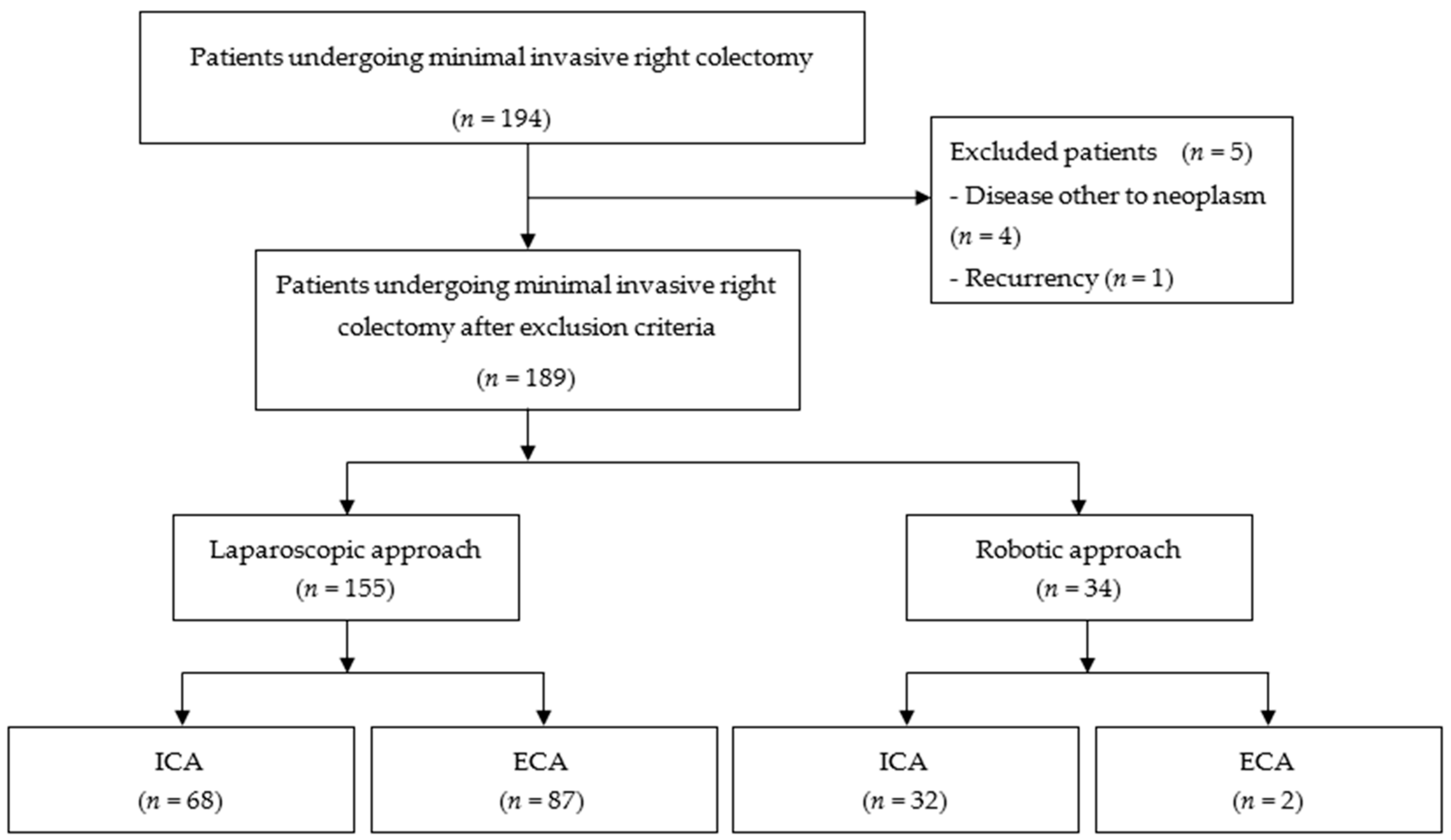
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.-J.; Ciombor, K.K.; Cohen, S.A.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. NCCN Guidelines Insights: Colon Cancer, Version 2.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 359–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellino, G.; Warren, O.; Mills, S.; Rasheed, S.; Tekkis, P.P.; Kontovounisios, C. Comparison of Western and Asian Guidelines Concerning the Management of Colon Cancer. Dis. Colon. Rectum. 2018, 61, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Nordholm-Carstensen, A.; Schnack Rasmussen, M.; Krarup, P.M. Increased leak rates following stapled versus handsewnileocolic anastomosis in patients with right-sided colon cancer: Anationwide cohort study. Dis. Colon. Rectum. 2019, 62, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Biondo, S.; Gálvez, A.; Ramírez, E.; Frago, R.; Kreisler, E. Emergency surgery for obstructing and perforated colon cancer: Patterns of recur-rence and prognostic factors. Tech. Coloproctol. 2019, 23, 1141–1161. [Google Scholar] [CrossRef]
- Hüttner, F.J.; Warschkow, R.; Schmied, B.M.; Diener, M.K.; Tarantino, I.; Ulrich, A. Prognostic impact of anastomotic leakage after elective colon resection for cancer—A propensity score matched analysis of 628 patients. Eur. J. Surg. Oncol. 2018, 44, 456–462. [Google Scholar] [CrossRef]
- Van Rooijen, S.; Jongen, A.C.; Wu, Z.-Q.; Ji, J.-F.; Slooter, G.D.; Roumen, R.M.; Bouvy, N.D. Definition of colorectal anastomotic leakage: A consensus survey among Dutch and Chinese colorectal surgeons. World J. Gastroenterol. 2017, 23, 6172–6180. [Google Scholar] [CrossRef]
- Goto, S.; Hasegawa, S.; Hida, K.; Uozumi, R.; Kanemitsu, Y.; Watanabe, T.; Sugihara, K.; Sakai, Y. Multicenter analysis of impact of anastomotic leakage on long-term oncologic outcomes after curative resection of colon cancer. Surgery 2017, 162, 317–324. [Google Scholar] [CrossRef]
- Bruce, J.; Krukowski, Z.H.; Al-Khairy, G.; Russell, E.M.; Park, K.G.M. Systematic review of the definition and measurement of anastomotic leak after gastrointestinal surgery. Br. J. Surg. 2001, 88, 1157–1168. [Google Scholar] [CrossRef]
- Adams, K.; Papagrigoriadis, S. Little consensus in either definition or diagnosis of a lower gastro-intestinal anastomotic leak amongst colorectal surgeons. Int. J. Color. Dis. 2013, 28, 967–971. [Google Scholar] [CrossRef]
- Kingham, T.P.; Pachter, H.L. Colonic anastomotic leak: Riskfactors, diagnosis, and treatment. J. Am. Coll. Surg. 2009, 208, 269–278. [Google Scholar] [CrossRef]
- Hirst, N.A.; Tiernan, J.P.; Millner, P.A.; Jayne, D.G. Systematic review of methods to predict and detect anastomotic leakage in colorectal surgery. Color. Dis. 2014, 16, 95–109. [Google Scholar] [CrossRef] [PubMed]
- Marinello, F.G.; Baguena, G.; Lucas, E.; Frasson, M.; Hervás, D.; Flor-Lorente, B.; Esclapez, P.; Espí, A.; García-Granero, E. Anastomotic leakage after colon cancer resection: Does the individual surgeon mat-ter? Colorectal Dis. 2016, 18, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Sciuto, A.; Merola, G.; De Palma, G.D.; Sodo, M.; Pirozzi, F.; Bracale, U. Predictive factors for anastomotic leakage after laparoscopic colorectal surgery. World J. Gastroenterol. 2018, 24, 2247–2260. [Google Scholar] [CrossRef]
- Frasson, M.; ANACO Study Group; Granero-Castro, P.; Rodríguez, J.L.R.; Flor-Lorente, B.; Braithwaite, M.; Martínez, E.M.; Pérez, J.A.Á; Cazador, A.C.; Espí, A.; et al. Risk factors for anastomotic leak and postoperative morbidity and mortality after elective right colectomy for cancer: Results from a prospective, multicentric study of 1102 patients. Int. J. Color. Dis. 2016, 31, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Espín, E.; Vallribera, F.; Kreisler, E.; Biondo, S. Clinical impact of leakage in patients with handsewn vs stapled anastomosis after right hemicolectomy: A retrospective study. Color. Dis. 2020, 22, 1286–1292. [Google Scholar] [CrossRef]
- Stein, S.A.; Bergamaschi, R. Extracorporeal versus intracorporeal ileocolic anastomosis. Tech. Coloproctol. 2013, 17, 35–39. [Google Scholar] [CrossRef]
- Aiolfi, A.; Bona, D.; Guerrazzi, G.; Bonitta, G.; Rausa, E.; Panizzo, V.; Campanelli, G.; Micheletto, G. Intracorporeal Versus Extracorporeal Anastomosis in Laparoscopic Right Colectomy: An Updated Systematic Review and Cumulative Meta-Analysis. J. Laparoendosc. Adv. Surg. Tech. 2020, 30, 402–412. [Google Scholar] [CrossRef]
- Emile, S.H.; Elfeki, H.; Shalaby, M.; Sakr, A.; Bassuni, M.; Christensen, P.; Wexner, S.D. Intracorporeal versus extracorporeal anastomosis in minimally invasive right colectomy: An updated systematic review and meta-analysis. Tech. Coloproctol. 2019, 23, 1023–1035. [Google Scholar] [CrossRef]
- Ricci, C.; Casadei, R.; Alagna, V.; Zani, E.; Taffurelli, G.; Pacilio, C.A.; Minni, F. A critical and comprehensive systematic review and meta-analysis of studies comparing intracorporeal and extracorporeal anastomosis in laparoscopic right hemicolectomy. Langenbeck’s Arch. Surg. 2017, 402, 417–427. [Google Scholar] [CrossRef]
- Chengwu, J.; Jin, C.; Hu, T.; Wei, M.; Wang, Z. Intracorporeal Versus Extracorporeal Anastomosis in Laparoscopic Right Colectomy: A Systematic Review and Meta-Analysis. J. Laparoendosc. Adv. Surg. Tech. 2017, 27, 348–357. [Google Scholar] [CrossRef]
- Allaix, M.E.; Degiuli, M.; Bonino, M.A.; Arezzo, A.; Mistrangelo, M.; Passera, R.; Morino, M. Intracorporeal or Extracorporeal Ileocolic Anastomosis After Laparoscopic Right Colectomy. Ann. Surg. 2019, 270, 762–767. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Re-porting of Observational Studies in Epidemiology (STROBE)statement: Guidelines for reporting observational studies. Lancet 2007, 143, 573–577. [Google Scholar]
- Slankamenac, K.; Graf, R.; Barkun, J.; Puhan, M.A.; Clavien, P.-A. The comprehensive complication index: A novel continuous scale to measure surgical morbidity. Ann. Surg. 2013, 258, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahbari, N.N.; Weitz, J.; Hohenberger, W.; Heald, R.J.; Moran, B.; Ulrich, A.; Holm, T.; Wong, W.D.; Tiret, E.; Moriya, Y.; et al. Definition and grading of anastomotic leakage following anterior resection of the rectum: A proposal by the International Study Group of Rectal Cancer. Surgery 2010, 147, 339–351. [Google Scholar] [CrossRef] [PubMed]
- DeSouza, A.; Domajnko, B.; Park, J.; Marecik, S.; Prasad, L.; Abcarian, H. Incisional hernia, midline versus low transverse incision: What is the ideal incision for specimen extraction and hand-assisted laparoscopy? Surg. Endosc. 2010, 25, 1031–1036. [Google Scholar] [CrossRef]
- Lee, L.; Abou-Khalil, M.; Liberman, S.; Boutros, M.; Fried, G.M.; Feldman, L.S. Incidence of incisional hernia in the specimen extraction site for laparoscopic colo-rectal surgery: Systematic review and meta-analysis. Surg. Endosc. 2017, 31, 5083–5093. [Google Scholar] [CrossRef]
- Pujol, M.; Limón, E.; Gonzalez, J.L.-C.; Sallés, M.; Bella, F.; Gudiol, F. Surveillance of surgical site infections in elective colorectal surgery. Results of the VINCat Program (2007–2010). Enferm. Infecc. Microbiol. Clín. 2012, 30, 20–25. [Google Scholar] [CrossRef]
- Espín, E.; Solís-Peña, A.; Pellino, G.; Kreisler, E.; Fraccalvieri, D.; Muinelo-Lorenzo, M.; Maseda-Díaz, O.; García-González, J.M.; Santamaría-Olabarrieta, M.; Codina-Cazador, A.; et al. Preoperative oral antibiotics and surgical-site infections in colon surgery (ORALEV): A multicentre, single-blind, pragmatic, randomised controlled trial. Lancet Gastroenterol. Hepatol. 2020, 5, 729–738. [Google Scholar] [CrossRef]
- Badia, J.M.; Rubio-Pérez, I.; López-Menéndez, J.; Diez, C.; Al-Raies Bolaños, B.; Ocaña-Guaita, J.; Meijome, X.M.; Chamorro-Pons, M.; Calderón-Nájera, R.; Ortega-Pérez, G.; et al. The persistent breach between evidence and practice in the prevention of surgical site infection. Qualitative study. Int. J. Surg. 2020, 82, 231–239. [Google Scholar] [CrossRef]
- GlobalSurg Collaborative. Surgical site infection after gastrointestinal surgery in children: An international, multicentre, prospective cohort study. BMJ Glob. Health. 2020, 5, e003429. [Google Scholar] [CrossRef] [PubMed]
- Kalakouti, E.; Simillis, C.; Pellino, G.; Mughal, N.; Warren, O.; Mills, S.; Tan, E.; Kontovounisios, C.; Tekkis, P.P. Characteristics of Surgical Site Infection Following Colorectal Surgery in a Tertiary Center: Extended-spectrum β-Lactamase-producing Bacteria Culprits in Disease. Wounds 2017, 30, 108–113. [Google Scholar] [PubMed]
- GlobalSurg Collaborative. Surgical site infection after gastrointestinal surgery in high-income, middle-income, and low-income countries: A prospective, international, multicentre cohort study. Lancet Infect. Dis. 2018, 18, 516–525. [Google Scholar] [CrossRef] [Green Version]
- Basany, E.E.; Pellino, G. Almirante B. Preoperative oral antibiotics in colon surgery-Authors’ reply. Lancet Gastroenterol. Hepatol. 2020, 5, 802–803. [Google Scholar] [CrossRef]
- Shapiro, R.; Keler, U.; Segev, L.; Sarna, S.; Hatib, K.; Hazzan, D. Laparoscopic right hemicolectomy with intracorporeal anastomosis: Short- and long-term benefits in comparison with extracorporeal anastomosis. Surg. Endosc. 2015, 30, 3823–3829. [Google Scholar] [CrossRef]
- Jamali, F.R.; Soweid, A.M.; Dimassi, H.; Bailey, C.; Leroy, J.; Marescaux, J. Evaluating the Degree of Difficulty of Laparoscopic Colorectal Surgery. Arch. Surg. 2008, 143, 762–767. [Google Scholar] [CrossRef] [Green Version]
- Scotton, G.; Contardo, T.; Zerbinati, A.; Tosato, S.M.; Orsini, C.; Morpurgo, E. From Laparoscopic Right Colectomy with Extracorporeal Anastomosis to Robot-Assisted Intracorporeal Anastomosis to Totally Robotic Right Colectomy for Cancer: The Evolution of Robotic Multiquadrant Abdominal Surgery. J. Laparoendosc. Adv. Surg. Tech. 2018, 28, 1216–1222. [Google Scholar] [CrossRef]
- Spinoglio, G.; Bianchi, P.P.; Marano, A.; Priora, F.; Lenti, L.M.; Ravazzoni, F.; Petz, W.; Borin, S.; Ribero, D.; Formisano, G.; et al. Robotic Versus Laparoscopic Right Colectomy with Complete Mesocolic Excision for the Treatment of Colon Cancer: Perioperative Outcomes and 5-Year Survival in a Consecutive Series of 202 Patients. Ann. Surg. Oncol. 2018, 25, 3580–3586. [Google Scholar] [CrossRef]


{kind=link}
| Type of Anastomosis | ||||
|---|---|---|---|---|
| All (189) | IA (102) | EA (87) | p | |
| Gender, male, n (%) | 93 (49.2) | 51 (50) | 42 (48,3) | 0.66 |
| Age, years, median (range) | 77 (37–93) | 77 (37–92) | 76 (49–93) | 0.7 |
| ASA classification, n (%) | 0.65 | |||
| I | 10 | 6 | 4 | |
| II | 103 | 57 | 46 | |
| III | 72 | 38 | 34 | |
| IV | 4 | 1 | 3 | |
| POSSUM physiological score, median (range) | 18 (11–32) | 16 (12–30) | 18 (11–32) | 0.81 |
| Surgical approach, n (%) | <0.001 | |||
| Laparoscopy | 155 | 68 (43.9) | 87 (56.1) | |
| Robotic surgery | 34 | 32 (94.1) | 2 (5.9) | |
| Type of Anastomosis | ||||
|---|---|---|---|---|
| All (n = 189) | IA (n = 102) | EA (n = 87) | p | |
| Global morbidity, n (%) | 59 (31.2) | 24 (23.5) | 35 (40.2) | 0.014 |
| Mortality, n (%) | 6 (3.2) | 4 (3.9) | 2 (2.3) | 0.53 |
| Medical complications, n (%) | 19 (10) | 6 (5.9) | 13 (14.9) | 0.039 |
| Cardiac complications | 6 (3.2) | 3 (2.9) | 3 (3.5) | |
| Anaemia | 9 (4.8) | 1 (1) | 8 (9.2) | |
| Respiratory complications | 4 (2.1) | 2 (2) | 2 (2.3) | |
| Global surgical complications, n (%) | 42 (22.2) | 18 (17.8) | 24 (27.6) | 0.1 |
| Surgical Site Infection | 9 (4.8) | 3 (2.9) | 6 (6.9) | 0.31 |
| Anastomotic leakage, n (%) | 19 (10) | 10 (9.8) | 9 (10.3) | 0.55 |
| Non-infectious surgical wound complications, n (%) | 4 (2.1) | 0 | 4 (4.6) | 0.029 |
| Evisceration | 3 (1.6) | 0 | 3 (3.4) | |
| Haematoma | 2 (1) | 0 | 2 (2.2) | |
| Postoperative ileus, n (%) | 29 (15.3) | 11 (10.8) | 18 (20.7) | 0.06 |
| Postoperative ileus, n (%) | 29 (15.3) | 11 (10.8) | 18 (20.7) | 0.06 |
| Need for reoperation, n (%) | 11 (5.8) | 8 (7.8) | 3 (3.5) | 0.14 |
| Surgical Complications | Overall Complications | |||
|---|---|---|---|---|
| Variable | OR (95% CI) | p | OR (95% CI) | p |
| POSSUM physiological score | 1.08 (0.93–1.25) | 0.315 | 1.24 (1.02–1.49) | 0.033 |
| Drain placement at surgery | 0.666 | 0.679 | ||
| No | Ref. | Ref. | ||
| Yes | 1.29 (0.4–4.15) | 1.44 (0.26–7.97) | ||
| ASA | 0.219 | 0.121 | ||
| ASA I | Ref. | Ref. | ||
| ASA II | 0.29 (0.06–1.44) | 0.32 (0.03–3.51) | ||
| ASA III | 0.56 (0.12–2.65) | 1.27 (0.13–12.2) | ||
| ASA IV | 3.1 (0.18–52.6) | 3.19 (0.14–70.78) | ||
| Blood transfusion | 0.001 | 0.083 | ||
| No | Ref. | Ref. | ||
| Yes | 12.14 (2.89–50.91) | 4.02 (0.83–19.38) | ||
| Anastomosis: technique | 0.187 | 0.201 | ||
| Hand-sewn | Ref. | Ref. | ||
| Stapled | 1.87 (0.74–4.75) | 2.16 (0.66–7.04) | ||
| Anastomosis: type | 0.040 | 0.040 | ||
| Intra-corporeal | Ref. | Ref. | ||
| Extra-corporeal | 3.71 (1.06–12.91) | 3.58 (1.06–12.12) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vallribera, F.; Kraft, M.; Pera, M.; Vidal, L.; Espín-Basany, E. Outcomes of Intra- versus Extra-Corporeal Ileocolic Anastomosis after Minimally Invasive Right Colectomy for Cancer: An Observational Study. J. Clin. Med. 2021, 10, 307. https://doi.org/10.3390/jcm10020307
Vallribera F, Kraft M, Pera M, Vidal L, Espín-Basany E. Outcomes of Intra- versus Extra-Corporeal Ileocolic Anastomosis after Minimally Invasive Right Colectomy for Cancer: An Observational Study. Journal of Clinical Medicine. 2021; 10(2):307. https://doi.org/10.3390/jcm10020307
Chicago/Turabian StyleVallribera, Francesc, Miquel Kraft, Meritxell Pera, Laura Vidal, and Eloy Espín-Basany. 2021. "Outcomes of Intra- versus Extra-Corporeal Ileocolic Anastomosis after Minimally Invasive Right Colectomy for Cancer: An Observational Study" Journal of Clinical Medicine 10, no. 2: 307. https://doi.org/10.3390/jcm10020307