
Involvement of Cutaneous Sensory Corpuscles in Non-Painful and Painful Diabetic Neuropathy

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
- Clinical history: age, gender, time of evolution of disease, variant of peripheral neuropathy, HbA1c value, presence of proinflammatory and inflammatory factors (c-reactive protein, erythrocyte sedimentation rate), alterations in blood clotting test, ankle-brachial index, Doppler, and nervous conduction studies.
- Physical examination: maintained local sensibility, popliteal artery pulse assessment, skin alterations or deformities and allodynia/hyperalgesia/paresthesia/anesthesia. Sensitivity was focused on the clinical examination if anatomical structures and biochemical channels in study are responsible of this sensation.
- Monofilament testing: to ascertain the presence of sensibility in 4 random points at the affected extremity.
- Plantar discrimination: capacity, which is closely associated with mechanosensory receptors. Alterations in this variable may be related to an increase, decrease, or absence of mechanoreceptor.
- DN4 test to estimate neuropathic pain: Previous studies describe how alterations on these sensory structures may produce extreme effects in the form of a total anesthesia in the studied region, or even an excessive painful response under normally painless stimuli. Data from patients and analytical are summarized in Table 1.
2.2. Material and Treatment of the Tissues
2.3. Histology and Immunohistochemistry
2.4. Quantitative Study
3. Results
3.1. Quantitative Analyses of Cutaneous Sensory Corpuscles: Association between Density and Neuropathy
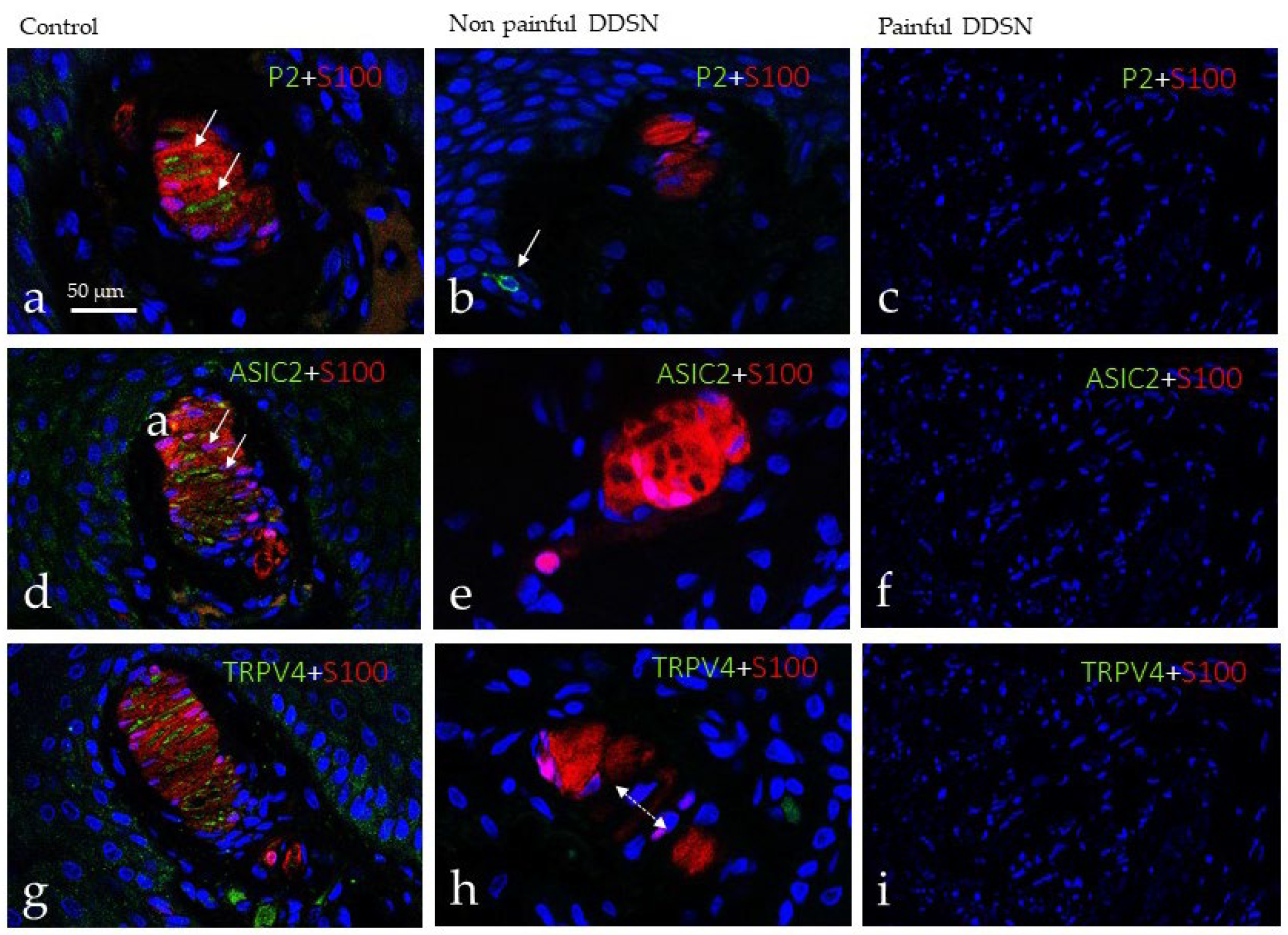
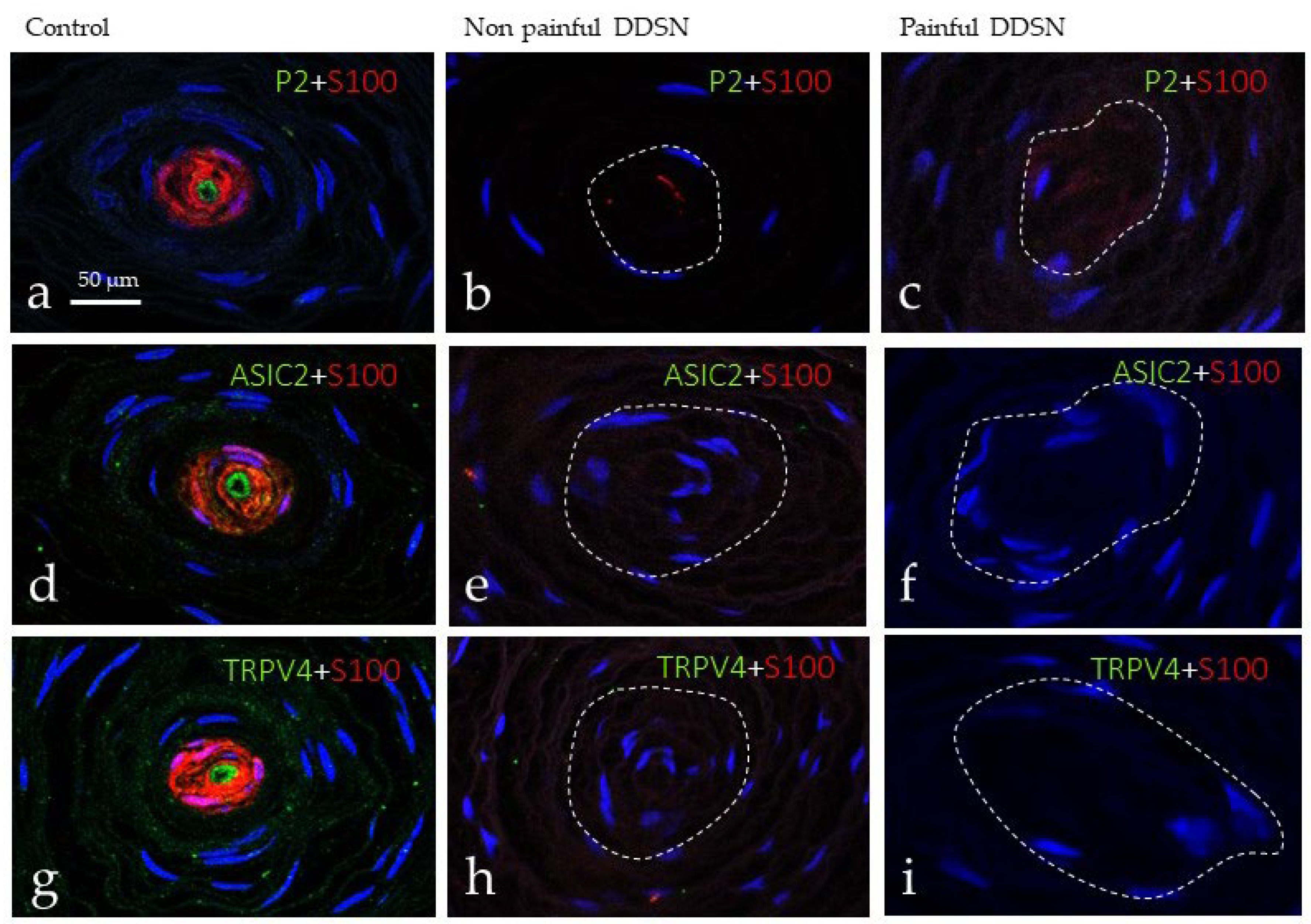
3.2. Immunohistochemical Profile of Meissner and Pacinian Corpuscles
3.3. Immunohistochemical Profile of Merkel Cells
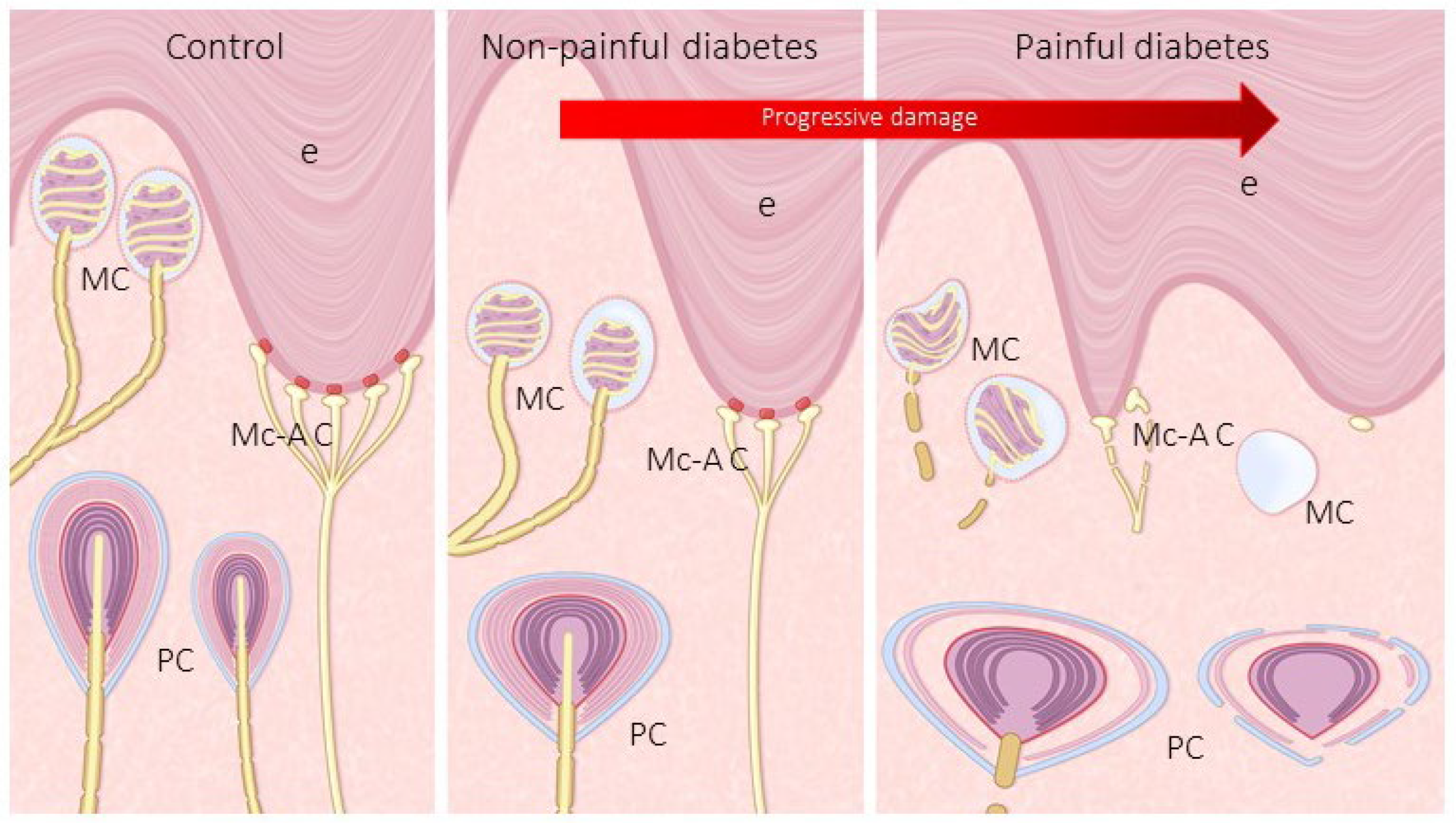
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pop-Busui, R.; Boulton, A.J.; Feldman, E.L.; Bril, V.; Freeman, R.; Malik, R.A.; Sosenko, J.M.; Ziegler, D. Diabetic Neuropathy: A Position Statement by the American Diabetes Association. Diabetes Care 2017, 40, 136–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tesfaye, S.; Boulton, A.J.; Dyck, P.J.; Freeman, R.; Horowitz, M.; Kempler, P.; Lauria, G.; Malik, R.A.; Spallone, V.; Vinik, A.; et al. Diabetic neuropathies: Update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care 2010, 33, 2285–2293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, T.; Nawroth, P.; Kuner, R. Structure-function relationships in peripheral nerve contributions to diabetic peripheral neuropathy. Pain 2019, 160, S29–S36. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.; Frank, B.; Marshall, A.; Khalil, R.S.; Ponirakis, G.; Petropoulos, I.N.; Cuthbertson, D.J.; Malik, R.A.; Alam, U. Early Detection of Diabetic Peripheral Neuropathy: A Focus on Small Nerve Fibres. Diagnostics 2021, 11, 165. [Google Scholar] [CrossRef]
- Karlsson, P.; Gylfadottir, S.S.; Kristensen, A.G.; Ramirez, J.D.; Cruz, P.; Le, N.; Shillo, P.R.; Tesfaye, S.; Rice, A.S.C.; Tankisi, H.; et al. Axonal swellings are related to type 2 diabetes, but not to distal diabetic sensorimotor polyneuropathy. Diabetologia 2021, 64, 923–931. [Google Scholar] [CrossRef]
- Boulton, A.J.; Armstrong, D.G.; Albert, S.F.; Frykberg, R.G.; Hellman, R.; Kirkman, M.S.; Lavery, L.A.; Lemaster, J.W.; Mills, J.L.; Mueller, M.J.; et al. Comprehensive foot examination and risk assessment: A report of the task force of the foot care interest group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists. Diabetes Care 2008, 31, 1679–1685. [Google Scholar] [CrossRef] [Green Version]
- Papanas, N.; Ziegler, D. New diagnostic tests for diabetic distal symmetric polyneuropathy. J. Diabetes Complicat. 2011, 25, 44–51. [Google Scholar] [CrossRef]
- Buonocore, M. Unilateral peripheral neuropathic pain: The role of neurodiagnostic skin biopsy. World J. Clin. Cases 2014, 2, 27–31. [Google Scholar] [CrossRef]
- Duchesne, M.; Magy, L.; Richard, L.; Ingrand, P.; Neau, J.P.; Mathis, S.; Vallat, J.M. Simultaneous Quantification of Unmyelinated Nerve Fibers in Sural Nerve and in Skin. J. Neuropathol. Exp. Neurol. 2016, 75, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Roszkowska, A.M.; Licitra, C.; Tumminello, G.; Postorino, E.I.; Colonna, M.R.; Aragona, P. Corneal nerves in diabetes-The role of the in vivo corneal confocal microscopy of the subbasal nerve plexus in the assessment of peripheral small fiber neuropathy. Surv. Ophthalmol. 2020, 6257, 30133–30138. [Google Scholar] [CrossRef]
- Ferdousi, M.; Azmi, S.; Kalteniece, A.; Petropoulos, I.N.; Ponirakis, G.; Asghar, O.; Alam, U.; Marshall, A.; Boulton, A.J.M.; Efron, N.; et al. Greater small nerve fibre damage in the skin and cornea of type 1 diabetic patients with painful compared to painless diabetic neuropathy. Eur. J. Neurol. 2021, 28, 1745–1751. [Google Scholar] [CrossRef]
- Bönhof, G.J.; Strom, A.; Püttgen, S.; Ringel, B.; Brüggemann, J.; Bódis, K.; Müssig, K.; Szendroedi, J.; Roden, M.; Ziegler, D. Patterns of cutaneous nerve fibre loss and regeneration in type 2 diabetes with painful and painless polyneuropathy. Diabetologia 2017, 60, 2495–2503. [Google Scholar] [CrossRef] [Green Version]
- Bierhaus, A.; Haslbeck, K.M.; Humpert, P.M.; Liliensiek, B.; Dehmer, T.; Morcos, M.; Sayed, A.A.; Andrassy, M.; Schiekofer, S.; Schneider, J.G.; et al. Loss of pain perception in diabetes is dependent on a receptor of the immunoglobulin superfamily. J. Clin. Investig. 2004, 114, 1741–1751. [Google Scholar] [CrossRef] [Green Version]
- Zippenfennig, C.; Drechsel, T.J.; Monteiro, R.L.; Sacco, I.C.N.; Milani, T.L. The Mechanoreceptor’s Role in Plantar Skin Changes in Individuals with Diabetes Mellitus. J. Clin. Med. 2021, 10, 2537. [Google Scholar] [CrossRef]
- Drechsel, T.J.; Monteiro, R.L.; Zippenfennig, C.; Ferreira, J.S.S.P.; Milani, T.L.; Sacco, I.C.N. Low and High Frequency Vibration Perception Thresholds Can Improve the Diagnosis of Diabetic Neuropathy. J. Clin. Med. 2021, 10, 3073. [Google Scholar] [CrossRef]
- Cobo, R.; García-Piqueras, J.; Cobo, J.; Vega, J.A. The Human Cutaneous Sensory Corpuscles: An Update. J. Clin. Med. 2021, 10, 227. [Google Scholar] [CrossRef]
- García-Suarez, O.; García-Mesa, Y.; García-Piqueras, J.; Salvo, G.; Cobo, J.L.; Alba, E.; Cobo, R.; Feito, J.; Vega, J.A. The Cutaneous Biopsy for the Diagnosis of Peripheral Neuropathies: Meissner’s Corpuscles and Merkel’s Cells. In Desmystifying Polyneuropathy. Recent Adavances and New Directions; Bozzetto-Ambrosi, P., Ed.; IntechOpen: London, UK, 2019; pp. 267–278. [Google Scholar]
- Nolano, M.; Tozza, S.; Caporaso, G.; Provitera, V. Contribution of Skin Biopsy in Peripheral Neuropathies. Brain Sci. 2020, 10, 989. [Google Scholar] [CrossRef]
- Ras, V.R.; Nava, P.B. Age-related changes of neurites in Meissner corpuscles of diabetic mice. Exp. Neurol. 1986, 91, 488–501. [Google Scholar] [CrossRef]
- Paré, M.; Albrecht, P.J.; Noto, C.J.; Bodkin, N.L.; Pittenger, G.L.; Schreyer, D.J.; Tigno, X.T.; Hansen, B.C.; Rice, F.L. Differential hypertrophy and atrophy among all types of cutaneous innervation in the glabrous skin of the monkey hand during aging and naturally occurring type 2 diabetes. J. Comp. Neurol. 2007, 501, 543–567. [Google Scholar] [CrossRef]
- Peltier, A.C.; Myers, M.I.; Artibee, K.J.; Hamilton, A.D.; Yan, Q.; Guo, J.; Shi, Y.; Wang, L.; Li, J. Evaluation of dermal myelinated nerve fibers in diabetes mellitus. J. Peripher. Nerv. Syst. 2013, 18, 162–167. [Google Scholar] [CrossRef] [Green Version]
- Creigh, P.D.; McDermott, M.P.; Sowden, J.E.; Ferguson, M.; Herrmann, D.N. In-vivo reflectance confocal microscopy of Meissner’s corpuscles in diabetic distal symmetric polyneuropathy. J. Neurol. Sci. 2017, 378, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Cobo, R.; García-Piqueras, J.; García-Mesa, Y.; Feito, J.; García-Suárez, O.; Vega, J.A. Peripheral Mechanobiology of Touch-Studies on Vertebrate Cutaneous Sensory Corpuscles. Int. J. Mol. Sci. 2020, 21, 6221. [Google Scholar] [CrossRef] [PubMed]
- Llombart, B.; Monteagudo, C.; López-Guerrero, J.A.; Carda, C.; Jorda, E.; Sanmartín, O.; Almenar, S.; Molina, I.; Martín, J.M.; Llombart-Bosch, A. Clinicopathological and immunohistochemical analysis of 20 cases of Merkel cell carcinoma in search of prognostic markers. Histopathology 2005, 46, 622–634. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, M.; Agnarsdóttir, M.; Edqvist, P.H.; Coter, A.; Ponten, F. SATB2 is expressed in Merkel cell carcinoma. Arch. Dermatol. Res. 2016, 308, 449–454. [Google Scholar] [CrossRef]
- García-Mesa, Y.; García-Piqueras, J.; García, B.; Feito, J.; Cabo, R.; Cobo, J.; Vega, J.A.; García-Suárez, O. Merkel cells and Meissner’s corpuscles in human digital skin display Piezo2 immunoreactivity. J. Anat. 2017, 231, 978–989. [Google Scholar] [CrossRef] [Green Version]
- Alleman, C.J.; Westerhout, K.Y.; Hensen, M.; Chambers, C.; Stoker, M.; Long, S.; van Nooten, F.E. Humanistic and economic burden of painful diabetic peripheral neuropathy in Europe: A review of the literature. Diabetes Res. Clin. Pract. 2015, 109, 215–225. [Google Scholar] [CrossRef] [Green Version]
- Vinik, A.I.; Vinik, E.J.; Colberg, S.R.; Morrison, S. Falls risk in older adults with type 2 diabetes. Clin. Geriatr. Med. 2015, 31, 89–99. [Google Scholar] [CrossRef]
- Zimmerman, A.; Bai, L.; Ginty, D.D. The gentle touch receptors of mammalian skin. Science 2014, 346, 950–954. [Google Scholar] [CrossRef] [Green Version]
- Shillo, P.; Sloan, G.; Greig, M.; Hunt, L.; Selvarajah, D.; Elliott, J.; Gandhi, R.; Wilkinson, I.D.; Tesfaye, S. Painful and Painless Diabetic Neuropathies: What Is the Difference? Curr. Diabetes Rep. 2019, 19, 32. [Google Scholar] [CrossRef] [Green Version]
- Rosenberger, D.C.; Blechschmidt, V.; Timmerman, H.; Wolff, A.; Treede, R.D. Challenges of neuropathic pain: Focus on diabetic neuropathy. J. Neural. Transm. 2020, 127, 589–624. [Google Scholar] [CrossRef] [Green Version]
- Mizisin, A.P. Mechanisms of diabetic neuropathy: Schwann cells. Handb. Clin. Neurol. 2014, 126, 401–428. [Google Scholar] [CrossRef]
- Sima, A.A.; Zhang, W. Mechanisms of diabetic neuropathy: Axon dysfunction. Handb. Clin. Neurol. 2014, 26, 429–442. [Google Scholar] [CrossRef]
- Themistocleous, A.C.; Ramirez, J.D.; Shillo, P.R.; Lees, J.G.; Selvarajah, D.; Orengo, C.; Tesfaye, S.; Rice, A.S.; Bennett, D.L. The Pain in Neuropathy Study (PiNS): A cross-sectional observational study determining the somatosensory phenotype of painful and painless diabetic neuropathy. Pain 2016, 157, 1132–1145. [Google Scholar] [CrossRef] [Green Version]
- Lauria, G.; Merkies, I.S.; Faber, C.G. Small fiber neuropathy. Curr. Opin. Neurol. 2012, 25, 542–549. [Google Scholar] [CrossRef]
- Andersen, S.T.; Witte, D.R.; Andersen, H.; Bjerg, L.; Bruun, N.H.; Jørgensen, M.E.; Finnerup, N.B.; Lauritzen, T.; Jensen, T.S.; Tankisi, H.; et al. Risk-Factor Trajectories Preceding Diabetic Polyneuropathy: ADDITION-Denmark. Diabetes Care 2018, 41, 1955–1962. [Google Scholar] [CrossRef] [Green Version]
- Jensen, T.S.; Baron, R.; Haanpää, M.; Kalso, E.; Loeser, J.D.; Rice, A.S.; Treede, R.D. A new definition of neuropathic pain. Pain 2011, 152, 2204–2205. [Google Scholar] [CrossRef]
- Del Valle, M.E.; Cabal, A.; Alvarez-Mendez, J.C.; Calzada, B.; Haro, J.J.; Collier, W.; Vega, J.A. Effect of denervation on lamellar cells of Meissner-like sensory corpuscles of the rat. An immunohistochemical study. Cell Mol. Biol. 1993, 39, 801–807. [Google Scholar]
- Márquez, J.; Pérez-Pérez, M.; Naves, F.J.; Vega, J.A. Effect of spinal cord and peripheral nerve injury on human cutaneous sensory corpuscles. An immunohistochemical study. J. Peripher. Nerv. Syst. 1997, 2, 49–59. [Google Scholar]
- Albuerne, M.; López, S.; Naves, F.J.; Martínez-Almagro, A.; Represa, J.; Vega, J.A. S100alpha and S100beta proteins in human cutaneous sensory corpuscles: Effects of nerve and spinal cord injury. Anat. Rec. 1998, 251, 351–359. [Google Scholar] [CrossRef]
- Tan, A.M. Dendritic spine dysgenesis in neuropathic pain. Prog. Mol. Biol. Transl. Sci. 2015, 131, 385–408. [Google Scholar] [CrossRef]
- Tsuda, M. Microglia in the spinal cord and neuropathic pain. J. Diabetes Investig. 2016, 7, 17–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | NP DDSP | P DDSP | |
|---|---|---|---|
| Age | 62 ± 8.2 s.d. | 60 ± 10.3 | 70 ± 12.4 |
| Gender | mixed | mixed | mixed |
| Evolution (years) | 11 ± 9.4 | 21 ± 6.5 | |
| HBA1C | n.r. (<5.7%) | 6.5 ± 0.5 | 7.6 ± 5.17 |
| C-reactive protein | n.r. (<10 mg/L) | 16 ± 18.75 | 39.5 ± 25.14 |
| GSS | n.r. (0–29 mm/h) | 40.5 ± 58.68 | 129 ± 76.37 |
| Prothrombin rate (%) | n.r. (70–100%) | 74.8 ± 40.38 | 88.6 ± 50.46 |
| Fibrinogen | n.r. (200–400 mg/dL) | 526.5 ± 376.7 | 935 ± 198.15 |
| Ankle-brachial index | n.r. (0.9–1.3 mmHg) | 0.79 ± 0.1 | not valuable |
| Echo-Doppler | n.r. (permeable) | permeable popliteal art. | distal obstruction |
| Sensitivity | n.r. (100%) | Yes (100%) | Yes (50%) |
| Discriminative capacity | n.r. (<1 cm) | 5.5 cm ± 2.17 | 8 cm ± 3.09 |
| Foot pulses | n.r. (100%) | Yes (33%) | Yes (25%) |
| Skin deformity | n.r. (normal skin) | Yes (50%) | Yes (25%) |
| Pain test | not pain | not pain | electric shock |
| Monofilament test | n.r. (100%) | Positive (50%) | Positive (100%) |
| Antigen (Clone) | Origin | Dilution | Supplier |
|---|---|---|---|
| Axonal markers | |||
| NSE (BBS/NC/IV-H14) | Mouse | 1:100 | Dako, Glostrup, Denmark |
| NFP (NF-H-RNF402) | Mouse | 1:200 | Santa Cruz Biotechnology, CA, USA |
| Schwann-related cells | |||
| S100P | Rabbit | 1:5000 | Dako, Glostrup, Denmark |
| S100P (4C4.9) | Mouse | 1:1000 | Thermo Scientific, Freemont, CA, USA |
| Merkel cells | |||
| ChrA (DAK-A3) | Mouse | Prediluted | Dako, Glostrup, Denmark |
| CK20 (ks 20.8-IS777) | Mouse | Prediluted | Dako, Glostrup, Denmark |
| Ion channels | |||
| ASIC 2 | Rabbit | 1:200 | Lifespan Biosciences, Seatle, WA, USA |
| TRPV4 | Rabbit | 1:200 | Abcamn, Cambridge, UK |
| PIEZO2 | Rabbit | 1:500 | Sigma-Aldrich, Madrid, Spain |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Mesa, Y.; Feito, J.; González-Gay, M.; Martínez, I.; García-Piqueras, J.; Martín-Cruces, J.; Viña, E.; Cobo, T.; García-Suárez, O. Involvement of Cutaneous Sensory Corpuscles in Non-Painful and Painful Diabetic Neuropathy. J. Clin. Med. 2021, 10, 4609. https://doi.org/10.3390/jcm10194609
García-Mesa Y, Feito J, González-Gay M, Martínez I, García-Piqueras J, Martín-Cruces J, Viña E, Cobo T, García-Suárez O. Involvement of Cutaneous Sensory Corpuscles in Non-Painful and Painful Diabetic Neuropathy. Journal of Clinical Medicine. 2021; 10(19):4609. https://doi.org/10.3390/jcm10194609
Chicago/Turabian StyleGarcía-Mesa, Yolanda, Jorge Feito, Mario González-Gay, Irene Martínez, Jorge García-Piqueras, José Martín-Cruces, Eliseo Viña, Teresa Cobo, and Olivia García-Suárez. 2021. "Involvement of Cutaneous Sensory Corpuscles in Non-Painful and Painful Diabetic Neuropathy" Journal of Clinical Medicine 10, no. 19: 4609. https://doi.org/10.3390/jcm10194609