
Association of Acute Kidney Injury with the Risk of Dementia: A Meta-Analysis

 ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Search Strategy
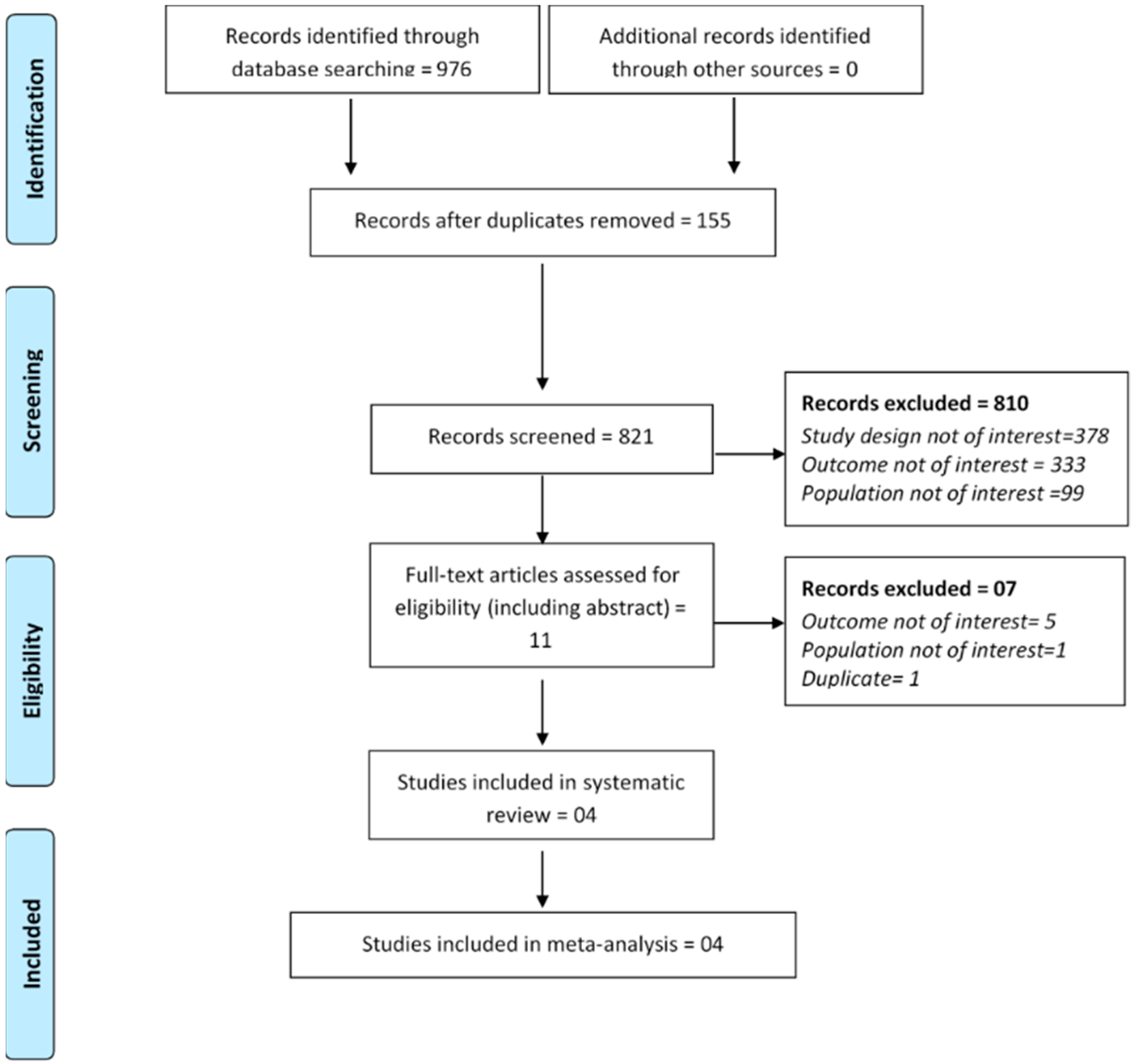
2.3. Study Selection/Inclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment and Certainty of the Evidence
2.6. Statistical Analysis
3. Results
3.1. Studies Characteristics
3.2. Quality Assessment and Certainty of the Evidence
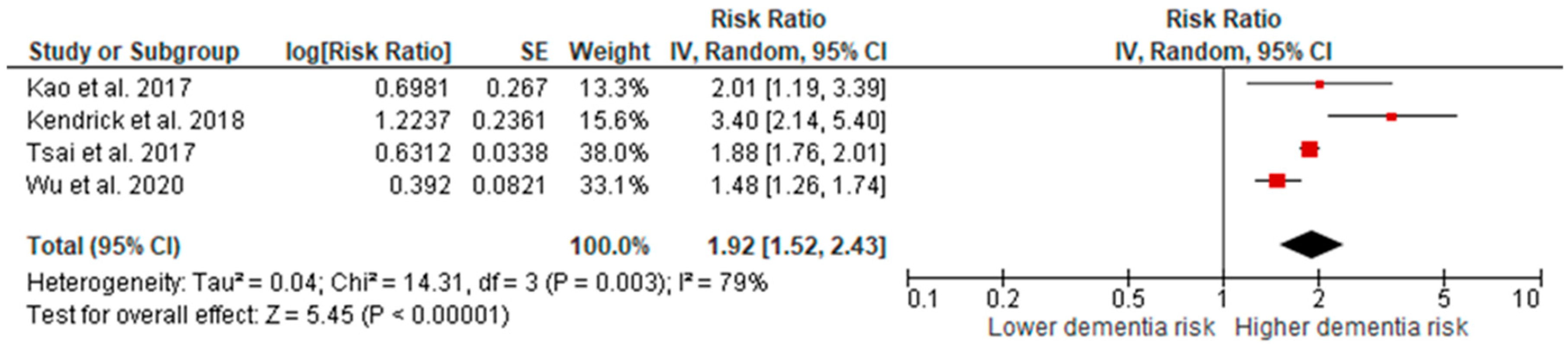
3.3. Meta-Analysis
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conference Presentation
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levey, A.S.; Levin, A.; Kellum, J.A. Definition and classification of kidney diseases. Am. J. Kidney Dis. 2013, 61, 686–688. [Google Scholar] [CrossRef] [PubMed]
- Lameire, N.H.; Bagga, A.; Cruz, D.; De Maeseneer, J.; Endre, Z.; Kellum, J.A.; Liu, K.D.; Mehta, R.L.; Pannu, N.; Biesen, W.V. Acute kidney injury: An increasing global concern. Lancet 2013, 382, 170–179. [Google Scholar] [CrossRef]
- Luyckx, V.A.; Tonelli, M.; Stanifer, J.W. The global burden of kidney disease and the sustainable development goals. Bull. World Health Organ. 2018, 96, 414. [Google Scholar] [CrossRef]
- Hoste, E.A.J.; Kellum, J.A.; Selby, N.M.; Zarbock, A.; Palevsky, P.M.; Bagshaw, S.M.; Goldstein, S.L.; Cerdá, J.; Chawla, L.S. Global epidemiology and outcomes of acute kidney injury. Nat. Rev. Nephrol. 2018, 14, 607–625. [Google Scholar] [CrossRef] [PubMed]
- Grams, M.E.; Rabb, H. The distant organ effects of acute kidney injury. Kidney Int. 2012, 81, 942–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortrie, G.; de Geus, H.R.; Betjes, M.G. The aftermath of acute kidney injury: A narrative review of long-term mortality and renal function. Crit. Care 2019, 23, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowson, C.S.; Liao, K.P.; Davis, J.M., III; Solomon, D.H.; Matteson, E.L.; Knutson, K.L.; Hlatky, M.A.; Gabriel, S.E. Rheumatoid arthritis and cardiovascular disease. Am. Heart J. 2013, 166, 622–628.e1. [Google Scholar] [CrossRef] [Green Version]
- Cioffi, G.; Ognibeni, F.; Dalbeni, A.; Giollo, A.; Orsolini, G.; Gatti, D.; Rossini, M.; Viapiana, O. High prevalence of occult heart disease in normotensive patients with rheumatoid arthritis. Clin. Cardiol. 2018, 41, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Ungprasert, P.; Srivali, N.; Kittanamongkolchai, W. Risk of incident atrial fibrillation in patients with rheumatoid arthritis: A systematic review and meta-analysis. Int. J. Rheum. Dis. 2017, 20, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Uzun, S.; Kozumplik, O.; Folnegović-Šmalc, V. Alzheimer’s dementia: Current data review. Coll. Antropol. 2011, 35, 1333–1337. [Google Scholar] [PubMed]
- WHO. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 25 August 2021).
- Nichols, E.; Szoeke, C.E.I.; Vollset, S.E.; Abbasi, N.; Abd-Allah, F.; Abdela, J.; Aichour, M.T.E.; Akinyemi, R.O.; Alahdab, F.; Asgedom, S.W. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 88–106. [Google Scholar] [CrossRef] [Green Version]
- Duggan, S.; Blackman, T.; Martyr, A.; Van Schaik, P. The impact of early dementia on outdoor life: Ashrinking world’? Dementia 2008, 7, 191–204. [Google Scholar] [CrossRef] [Green Version]
- Norton, S.; Matthews, F.E.; Barnes, D.E.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: An analysis of population-based data. Lancet Neurol. 2014, 13, 788–794. [Google Scholar] [CrossRef] [Green Version]
- Plassman, B.L.; Williams, J.W., Jr.; Burke, J.R.; Holsinger, T.; Benjamin, S. Systematic review: Factors associated with risk for and possible prevention of cognitive decline in later life. Ann. Intern. Med. 2010, 153, 182–193. [Google Scholar] [CrossRef] [Green Version]
- Schiffrin, E.L.; Lipman, M.L.; Mann, J.F. Chronic kidney disease: Effects on the cardiovascular system. Circulation 2007, 116, 85–97. [Google Scholar] [CrossRef] [Green Version]
- Tamura, M.K.; Yaffe, K. Dementia and cognitive impairment in ESRD: Diagnostic and therapeutic strategies. Kidney Int. 2011, 79, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etgen, T.; Chonchol, M.; Förstl, H.; Sander, D. Chronic kidney disease and cognitive impairment: A systematic review and meta-analysis. Am. J. Nephrol. 2012, 35, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Bugnicourt, J.-M.; Godefroy, O.; Chillon, J.-M.; Choukroun, G.; Massy, Z.A. Cognitive disorders and dementia in CKD: The neglected kidney-brain axis. J. Am. Soc. Nephrol. 2013, 24, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Kalaria, R.N.; Maestre, G.E.; Arizaga, R.; Friedland, R.P.; Galasko, D.; Hall, K.; Luchsinger, J.A.; Ogunniyi, A.; Perry, E.K.; Potocnik, F. Alzheimer’s disease and vascular dementia in developing countries: Prevalence, management, and risk factors. Lancet Neurol. 2008, 7, 812–826. [Google Scholar] [CrossRef] [Green Version]
- Deckers, K.; Camerino, I.; van Boxtel, M.P.; Verhey, F.R.; Irving, K.; Brayne, C.; Kivipelto, M.; Starr, J.M.; Yaffe, K.; de Leeuw, P.W. Dementia risk in renal dysfunction: A systematic review and meta-analysis of prospective studies. Neurology 2017, 88, 198–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.; Liang, Y.; Chigurupati, S.; Lathia, J.D.; Pletnikov, M.; Sun, Z.; Crow, M.; Ross, C.A.; Mattson, M.P.; Rabb, H. Acute kidney injury leads to inflammation and functional changes in the brain. J. Am. Soc. Nephrol. 2008, 19, 1360–1370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, S.K.; Molitoris, B.A. Renal endothelial injury and microvascular dysfunction in acute kidney injury. Semin. Nephrol. 2015, 35, 96–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kendrick, J.; Holmen, J.; Srinivas, T.; You, Z.; Chonchol, M.; Jovanovich, A. Acute kidney injury is associated with an increased risk of dementia. Kidney Int. Rep. 2019, 4, 1491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, H.-H.; Yen, R.-F.; Lin, C.-L.; Kao, C.-H. Increased risk of dementia in patients hospitalized with acute kidney injury: A nationwide population-based cohort study. PLoS ONE 2017, 12, e0171671. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.; Singh, A.; Antony, B.S.E.; Kulgarova, J.; Licenik, R.; Klugar, M. Association of acute kidney injury with the risk of dementia: A meta-analysis protocol. medRxiv 2021. [Google Scholar] [CrossRef]
- Hussain, S.; Singh, A.; Zameer, S.; Jamali, M.C.; Baxi, H.; Rahman, S.O.; Alam, M.; Altamish, M.; Singh, A.K.; Anil, D.; et al. No association between proton pump inhibitor use and risk of dementia: Evidence from a meta-analysis. J. Gastroenterol. Hepatol. 2020, 35, 19–28. [Google Scholar] [CrossRef] [PubMed]
- GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, F.; Sun, L.; Kaptoge, S. Association of beta-2-microglobulin and cardiovascular events and mortality: A systematic review and meta-analysis. Atherosclerosis 2021, 320, 70–78. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, A.; Hussain, S.; Najmi, A.K. Number of studies, heterogeneity, generalisability, and the choice of method for meta-analysis. J. Neurol. Sci. 2017, 381, 347. [Google Scholar] [CrossRef] [PubMed]
- GRADEpro GDT: GRADEpro Guideline Development Tool [Software]. McMaster University; Evidence Prime, Inc.: Hamilton, ON, Canada, 2020; Available online: https://gradepro.org (accessed on 25 August 2021).
- Kao, C.-C.; Wu, C.-H.; Lai, C.-F.; Huang, T.-M.; Chen, H.-H.; Wu, V.-C.; Chen, L.; Wu, M.-S.; Wu, K.-D.; The NSARF Group. Long-term risk of dementia following acute kidney injury: A population-based study. Tzu-Chi Med. J. 2017, 29, 201. [Google Scholar]
- Wu, Y. Dementia as an independent risk factor for acute kidney injury in elderly patients: A propensity-score matching study. Nephrology 2020, 25, 24. [Google Scholar]
- See, E.J.; Jayasinghe, K.; Glassford, N.; Bailey, M.; Johnson, D.W.; Polkinghorne, K.R.; Toussaint, N.D.; Bellomo, R. Long-term risk of adverse outcomes after acute kidney injury: A systematic review and meta-analysis of cohort studies using consensus definitions of exposure. Kidney Int. 2019, 95, 160–172. [Google Scholar] [CrossRef]
- Bedford, M.; Farmer, C.; Levin, A.; Ali, T.; Stevens, P. Acute kidney injury and CKD: Chicken or egg? Am. J. Kidney Dis. 2012, 59, 485–491. [Google Scholar] [CrossRef]
- CKD increases risk of acute kidney injury during hospitalization. Nat. Clin. Pract. Nephrol. 2008, 4, 408. Available online: https://www.nature.com/articles/ncpneph0850#citeas (accessed on 25 August 2021). [CrossRef]
- Chen, T.-B.; Yiao, S.-Y.; Sun, Y.; Lee, H.-J.; Yang, S.-C.; Chiu, M.-J.; Chen, T.-F.; Lin, K.-N.; Tang, L.-Y.; Lin, C.-C. Comorbidity and dementia: A nationwide survey in Taiwan. PLoS ONE 2017, 12, e0175475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, R.; Booth, A.; Rockwood, K.; Peters, J.; D’Este, C.; Anstey, K.J. Combining modifiable risk factors and risk of dementia: A systematic review and meta-analysis. BMJ Open 2019, 9, e022846. [Google Scholar] [CrossRef]
- Bunn, F.; Burn, A.-M.; Goodman, C.; Rait, G.; Norton, S.; Robinson, L.; Schoeman, J.; Brayne, C. Comorbidity and dementia: A scoping review of the literature. BMC Med. 2014, 12, 1–15. [Google Scholar] [CrossRef]
- Zijlstra, L.E.; Trompet, S.; Mooijaart, S.P.; van Buren, M.; Sattar, N.; Stott, D.J.; Jukema, J.W. The association of kidney function and cognitive decline in older patients at risk of cardiovascular disease: A longitudinal data analysis. BMC Nephrol. 2020, 21, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Yaffe, K.; Ackerson, L.; Tamura, M.K.; Le Blanc, P.; Kusek, J.W.; Sehgal, A.R.; Cohen, D.; Anderson, C.; Appel, L.; DeSalvo, K. Chronic kidney disease and cognitive function in older adults: Findings from the chronic renal insufficiency cohort cognitive study. J. Am. Geriatr. Soc. 2010, 58, 338–345. [Google Scholar] [CrossRef] [Green Version]
- Hailpern, S.M.; Melamed, M.L.; Cohen, H.W.; Hostetter, T.H. Moderate chronic kidney disease and cognitive function in adults 20 to 59 years of age: Third National Health and Nutrition Examination Survey (NHANES III). J. Am. Soc. Nephrol. 2007, 18, 2205–2213. [Google Scholar] [CrossRef] [Green Version]
- Hiramatsu, R.; Iwagami, M.; Nitsch, D. Association between chronic kidney disease and incident diagnosis of dementia in England: A cohort study in Clinical Practice Research Datalink. BMJ Open 2020, 10, e033811. [Google Scholar] [CrossRef]
- Fleegal-DeMotta, M.A.; Doghu, S.; Banks, W.A. Angiotensin II modulates BBB permeability via activation of the AT(1) receptor in brain endothelial cells. J. Cereb. Blood Flow Metab. 2009, 29, 640–647. [Google Scholar] [CrossRef] [Green Version]
- Bernardo-Castro, S.; Sousa, J.A.; Brás, A.; Cecília, C.; Rodrigues, B.; Almendra, L.; Machado, C.; Santo, G.; Silva, F.; Ferreira, L. Pathophysiology of Blood–Brain Barrier Permeability Throughout the Different Stages of Ischemic Stroke and Its Implication on Hemorrhagic Transformation and Recovery. Front. Neurol. 2020, 11, 1605. [Google Scholar] [CrossRef] [PubMed]
- Malek, M. Brain consequences of acute kidney injury: Focusing on the hippocampus. Kidney Res. Clin. Pract. 2018, 37, 315. [Google Scholar] [CrossRef] [Green Version]
- Nongnuch, A.; Panorchan, K.; Davenport, A. Brain–kidney crosstalk. Crit. Care 2014, 18, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nie, S.; Feng, Z.; Tang, L.; Wang, X.; He, Y.; Fang, J.; Li, S.; Yang, Y.; Mao, H.; Jiao, J. Risk factor analysis for AKI including laboratory indicators: A Nationwide multicenter study of hospitalized patients. Kidney Blood Press. Res. 2017, 42, 761–773. [Google Scholar] [CrossRef] [PubMed]
- Mogi, M.; Horiuchi, M. Clinical interaction between brain and kidney in small vessel disease. Cardiol. Res. Pract. 2011, 2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutton, T.A.; Fisher, C.J.; Molitoris, B.A. Microvascular endothelial injury and dysfunction during ischemic acute renal failure. Kidney Int. 2002, 62, 1539–1549. [Google Scholar] [CrossRef] [Green Version]
- Kuźma, E.; Lourida, I.; Moore, S.F.; Levine, D.A.; Ukoumunne, O.C.; Llewellyn, D.J. Stroke and dementia risk: A systematic review and meta-analysis. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2018, 14, 1416–1426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chertow, G.M.; Lazarus, J.M.; Paganini, E.P.; Allgren, R.L.; Lafayette, R.A.; Sayegh, M.H. Predictors of mortality and the provision of dialysis in patients with acute tubular necrosis. The Auriculin Anaritide Acute Renal Failure Study Group. J. Am. Soc. Nephrol. 1998, 9, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Taudorf, L.; Nørgaard, A.; Brodaty, H.; Laursen, T.M.; Waldemar, G. Dementia increases mortality beyond effects of comorbid conditions: A national registry-based cohort study. Eur. J. Neurol. 2021, 28, 2174–2184. [Google Scholar] [CrossRef] [PubMed]
- Taudorf, L.; Nørgaard, A.; Waldemar, G.; Laursen, T.M. Mortality in Dementia from 1996 to 2015: A National Registry-Based Cohort Study. J. Alzheimer’s Dis. 2021, 79, 289–300. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year, and Country | Study Design | Database Used | Study Duration | Follow-Up Period | Cohort Size | AKI Patients | Non-AKI Patients | Mean Age (Years) | Female (%) | Assessment of AKI | Assessment of Outcomes (Dementia) | Number of Dementia Cases in AKI/Non-AKI Group | Unadjusted Hazard Ratio/Risk Ratio | Adjusted Hazard/Risk Ratio/Odds Ratio | Study Adjusted for |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kao et al. 2017; Taiwan [36] | Cohort | Longitudinal Health Insurance Database | 1999–2008 | NR | 3445 | 689 | 2756 | 63.33 ± 16.19 | 41.90% | Procedure code | ICD-9-CM codes (290.X, 290.XX, 294.X, 294.XX, 331.X) | 44/67 | NR | 2.01 (95% CI: 1.19–3.39) | Adjusted for baseline co-morbidities, acute organ dysfunction, and the propensity score |
| Kendrick et al. 2019, USA [24] | Cohort | Intermountain Healthcare | 1999–2009 | 5.8 years | 2082 | 1041 | 1041 | 61 ± 16 | NR | ICD-9 codes and KDIGO guidelines | ICD-9 codes (290 to 290.4 and 331) | 73/24 | NR | 3.4 (95% CI: 2.14–5.40); composite outcome of dementia or death: 1.60 (1.40, 1.84) | Propensity matched |
| Tsai et al. 2017; Taiwan [25] | Cohort | Taiwan’s National Health Insurance Research Database | 2000–2011 | 12 years | 415576 | 207788 | 207788 | 68.13 ± 16.08 | 39.20% | (ICD-9-CM Code 584 | ICD9-CM Codes 290, 294.1, 331.0 | 3265/4806 | NR | 1.88 (95% CI: 1.76–2.01) | Study adjusted for age, sex, and several co-morbidities (diabetes, hypertension, hyperlipidemia, head injury, depression, stroke, chronic obstructive pulmonary disease, coronary artery disease, congestive heart failure, atrial fibrillation, cancer, liver disease, chronic infection/inflammation, autoimmune disease, malnutrition |
| Wu et al. 2020 * [37] | Case–control | NR | NR | NA | 8108 | 2231 | 5877 | NR | NR | KDIGO guidelines | NR | NR | NR | 1.48 (95% CI: 1.26–1.74) | Adjusted for estimated glomerular filtration rate, age, albumin level, hypertension, myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, chronic lung disease, connective tissue disease, moderate/severe renal disease, tumor, and anemia |
| Cohort Studies | Selection | Comparability | Outcome | ||||||
| Study Author | Representation of the Exposed Cohort | Selection of the Non-Exposed Cohort | Ascertainment of Exposure | Demonstration that Outcome of Interest Was Not Present at the Start of the Study | Comparability of Cohorts on the Basis of Design or Analysis | Assessment of Outcome | Was Follow-Up Long Enough for Outcomes to Occur | Accuracy of Follow-Up of Cohorts | Overall Score |
| Kao, 2017, Taiwan [36] | ✓ | ✓ | ✓ | ✓ | ✓✓ | ✓ | ✗ | ✓ | High (8) |
| Kendrick, 2019, USA [24] | ✓ | ✓ | ✓ | ✓ | ✓✓ | ✓ | ✓ | ✓ | High (9) |
| Tsai, 2017, Taiwan [25] | ✓ | ✓ | ✓ | ✓ | ✓✓ | ✓ | ✓ | ✓ | High (9) |
| Case-Control Study | Selection | Comparability | Outcome | ||||||
| Study author | Is the case definition adequate | Representativeness of the Cases | Selection of Controls | Definition of Controls | Comparability of Cases and Controls on the Basis of the Design or Analysis | Ascertainment of Exposure | Same method of ascertainment for cases and controls | Non-Response Rate | Overall Score |
| Wu, 2020, China [37] | ✓ | ✗ | ✓ | ✓ | ✓✓ | ✗ | ✗ | ✓ | Medium (6) |
| Certainty Assessment | №. of Patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | AKI and Dementia Risk | Placebo | Relative (95% CI) | Absolute (95% CI) | ||
| Dementia Risk | ||||||||||||
| 4 | observational studies | not serious | serious a | not serious | not serious | none | 3382/211749 (1.6%) | 4897/217462 (2.3%) | RR 1.92 (1.52 to 2.43) | 21 more per 1000 (from 12 more to 32 more) | ⨁ ◯ ◯ ◯ VERY LOW | High importance |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussain, S.; Singh, A.; Antony, B.; Claure-Del Granado, R.; Klugarová, J.; Líčeník, R.; Klugar, M. Association of Acute Kidney Injury with the Risk of Dementia: A Meta-Analysis. J. Clin. Med. 2021, 10, 4390. https://doi.org/10.3390/jcm10194390
Hussain S, Singh A, Antony B, Claure-Del Granado R, Klugarová J, Líčeník R, Klugar M. Association of Acute Kidney Injury with the Risk of Dementia: A Meta-Analysis. Journal of Clinical Medicine. 2021; 10(19):4390. https://doi.org/10.3390/jcm10194390
Chicago/Turabian StyleHussain, Salman, Ambrish Singh, Benny Antony, Rolando Claure-Del Granado, Jitka Klugarová, Radim Líčeník, and Miloslav Klugar. 2021. "Association of Acute Kidney Injury with the Risk of Dementia: A Meta-Analysis" Journal of Clinical Medicine 10, no. 19: 4390. https://doi.org/10.3390/jcm10194390