1. Introduction
Medial open wedge high tibial osteotomy (MOWHTO) is an established, effective operative treatment for relatively young and active patients with osteoarthritis in the medial compartment of the tibiofemoral joint and varus deformity [
1,
2]. MOWHTO reduces the pressure of the medial compartment in the tibiofemoral joint by realigning the mechanical axis from the medial to the lateral side in the coronal plane [
3,
4]. This procedure has been reported to have good long-term clinical outcomes such as reduced pain and improved knee joint function [
5,
6,
7]. Previous studies on MOWHTO tended to focus mainly on the change of alignment in the coronal plane regarding correction angle and postoperative coronal realignment [
8,
9,
10]. However, MOWHTO is the three-dimensional (3D) surgical procedure. Therefore, the postoperative effect of osteotomy on the proximal tibia should also be considered in the sagittal plane. In addition to correction in the coronal plane, maintaining alignment in the sagittal plane has been reported to be important. The change in the posterior tibial slope in the sagittal plane influences the biomechanics of the knee joint. The increase in posterior tibial slope of the tibiofemoral joint leads to anterior translation of the tibia relative to the femur, thus developing an overload on the anterior cruciate ligament [
11,
12]. An increased posterior tibial slope of the tibiofemoral joint could also cause a redistribution of pressure into the posterior tibia in the anterior cruciate ligament-deficient knee, resulting in degenerative change in articular cartilage [
13] and an increase of vertical vector force onto the patellofemoral joint, which could lead to osteoarthritis of the patellofemoral joint [
14,
15].
Despite efforts to maintain the posterior tibial slope of the tibiofemoral joint after MOWHTO, the posterior tibial slope tends to change after MOWHTO [
12,
16]. Change in posterior tibial slope before and after MOWHTO can be affected by various factors, including the osteotomy opening gap ratio between the anterior and posterior cortex [
17,
18]. Recently, the inclination angle of osteotomy in the sagittal plane has also been reported to affect change in the posterior tibial slope [
19]. However, to the best of our knowledge, there has been no comprehensive study on the effect of the osteotomy inclination angle in the sagittal plane on changes in the posterior tibial slope after MOWHTO, including the correlation between the osteotomy inclination angle and postoperative posterior tibial slope angle. Therefore, the purpose of this study was to investigate the effect of the osteotomy inclination angle in the sagittal plane on the change in posterior tibial slope after MOWHTO by comparing how anterior and posterior inclination affect the posterior tibial slope and assessing the correlation between the osteotomy inclination angle and postoperative posterior tibial slope angle. The measurement of values in this study was performed not only in two-dimensional radiographs, but also in 3D reconstructed images. It was hypothesized that anterior or posterior inclination of osteotomy in the sagittal plane would influence the change in the posterior tibial slope after MOWHTO.
4. Discussion
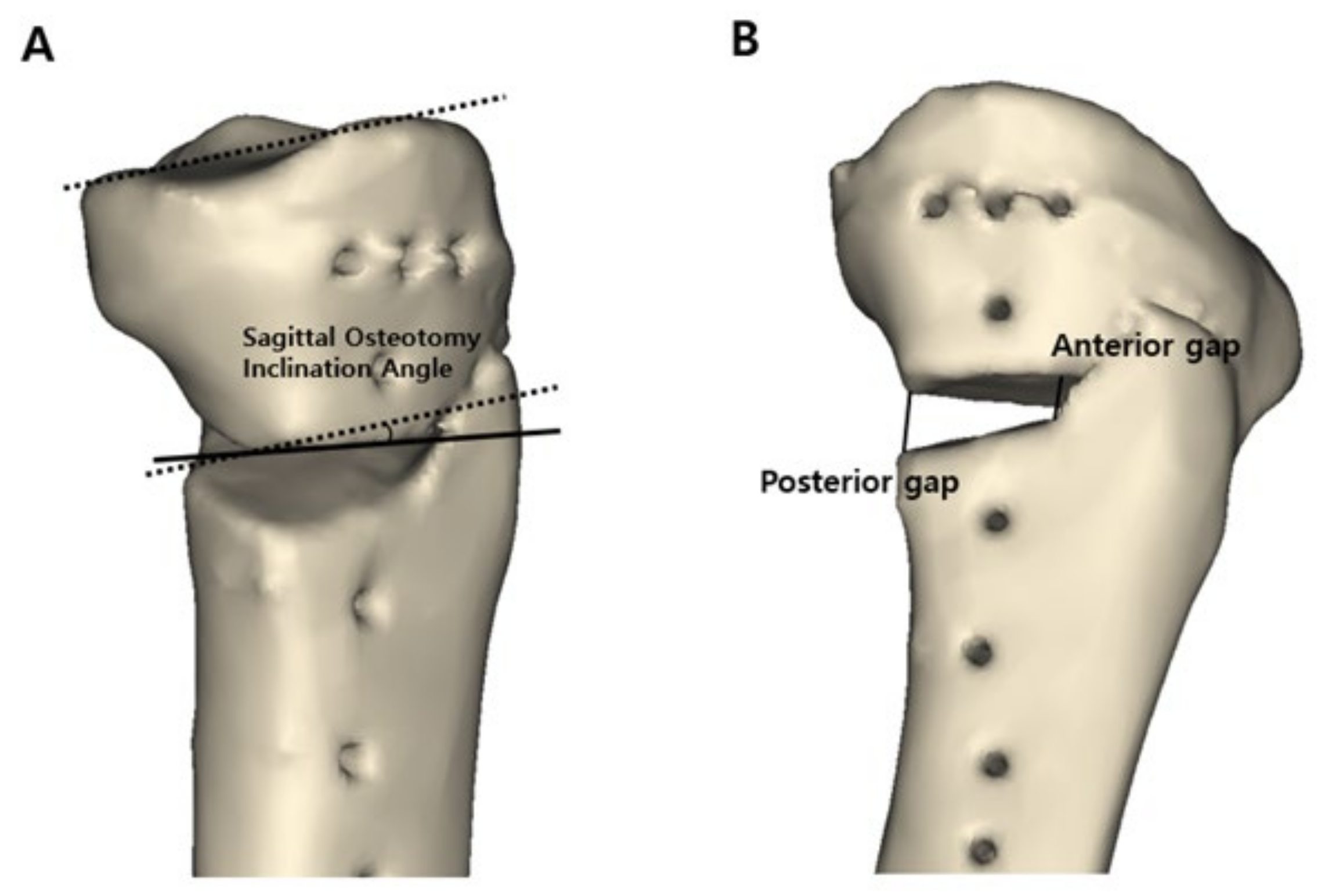
The posterior tibial slope changes after MOWHTO, but little is known about the effect of the osteotomy inclination angle in the sagittal plane on the change in the posterior tibial slope. To investigate this effect, changes in the posterior tibial slope before and after surgery were measured, and the tendency and extent of the change in the posterior tibial slope were assessed by comparing two groups: anterior and posterior osteotomy inclination in the sagittal plane. According to the principal findings of this study, although the mean gap ratio between the anterior and posterior openings was maintained at an appropriate value, approximately 2:3, as recommended in a previous study [
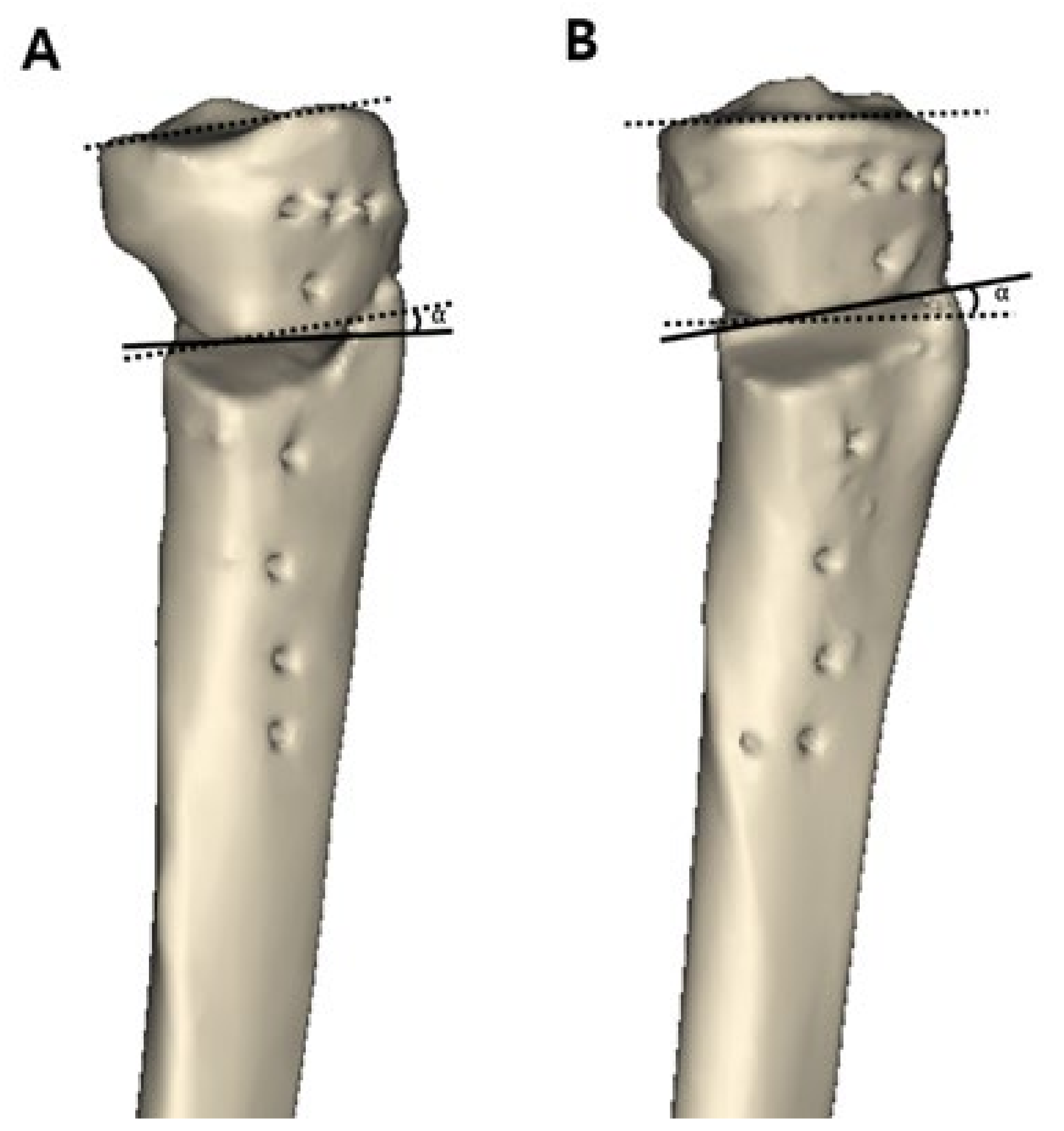
17], there was a significant difference in the posterior tibial slope before and after MOWHTO. In addition, the osteotomy inclination angle in the sagittal plane had a significant effect on the change in the posterior tibial slope. The anterior osteotomy inclination angle with the forward part of the osteotomy plane heading downward with respect to the medial tibial plateau line led to an increase in the postoperative posterior tibial slope. In contrast, the posterior osteotomy inclination angle led to a decrease in the postoperative posterior tibial slope.
Previous studies have noted that the posterior tibial slope changes after MOWHTO [
12,
18]. A recent meta-analysis also reported that posterior tibial slope increased by 2.02° after MOWTHO [
16]. Maintaining the posterior tibial slope before and after surgery is important to avoid unpredictable adverse effects. An increase in the posterior tibial slope could cause anterior translation of the tibia and increase the load on the anterior cruciate ligament [
11,
12]. An increased posterior tibial slope could also cause a redistribution of pressure into the posterior tibia in the anterior cruciate ligament-deficient knee, causing degenerative changes in articular cartilage [
13] and an increase of vertical vector force onto the patellofemoral joint, which could lead to osteoarthritis of the patellofemoral joint [
14,
15]. In addition to the knee joint, it has been reported that the tibial slope also has important biomechanical implications on the ankle joint [
31]. For these reasons, it is important to maintain the posterior tibial slope after MOWHTO, but there are practical difficulties in maintaining the posterior tibial slope during surgery because the proximal tibia is triangular, and osteotomy is performed from the anteromedial aspect without seeing the overall shape of the tibia. To avoid changes in the posterior tibial slope after MOWHTO, maintaining a constant ratio of the osteotomy opening gap between the anterior and posterior cortices has been emphasized [
17,
18]. Noyes et al. [
18] reported that to maintain the original posterior tibial slope, the anterior gap should be one half of the posterior gap, and Song et al. [
17] demonstrated that the normal posterior tibial slope can be unchanged if the anterior opening gap is approximately 67% of the posterior opening gap. To maintain the opening gap ratio, various factors leading to postoperative changes in the posterior tibial slope should be considered during surgery, such as incomplete posterior osteotomy, posterolateral hinge position, and an anteriorly placed plate affecting the gap ratio between the anterior and posterior cortices [
26,
32,
33,
34]. However, the results of this study showed that, although the mean opening gap ratio was maintained at an appropriate value, approximately 2:3 [
17], the posterior tibial slope could change after MOWHTO. According to the comparison of posterior tibial slopes before and after surgery measured with 3D reconstructed models for all patients, there was a significant increase in the posterior tibial slope after surgery (preoperative value = 9.4 ± 2.9°, postoperative value = 9.9 ± 3.2°,
p = 0.001). Consequently, it is necessary to identify additional factors affecting the change in the posterior tibial slope after MOWHTO.
According to the results of this study, another factor affecting the change in the posterior tibial slope was the inclination angle of osteotomy in the sagittal plane. Few studies have dealt with the osteotomy inclination angle in relation to the posterior tibial slope [
19,
35]. A previous study recommended an osteotomy line parallel to the joint line to avoid inadvertent alteration of the posterior tibial slope [
35]. Lee et al. [
19] investigated the inclination angle of osteotomy in the sagittal plane and noted that only 12.9% of cases were conducted parallel to the medial joint line and 87.1% of osteotomy lines were anteriorly inclined. Anterior inclination of osteotomy in the sagittal plane was reported to increase the posterior tibial slope. In addition to these previous studies, our study comprehensively assessed how anterior or posterior inclination of the sagittal osteotomy line affects the change in the posterior tibial slope after MOWHTO, and the correlation between the osteotomy inclination angle and postoperative posterior tibial slope angle. In our study, 72.5% of patients had anteriorly inclined osteotomy, while 27.5% of patients had posteriorly inclined osteotomy. Similar to a previous study [
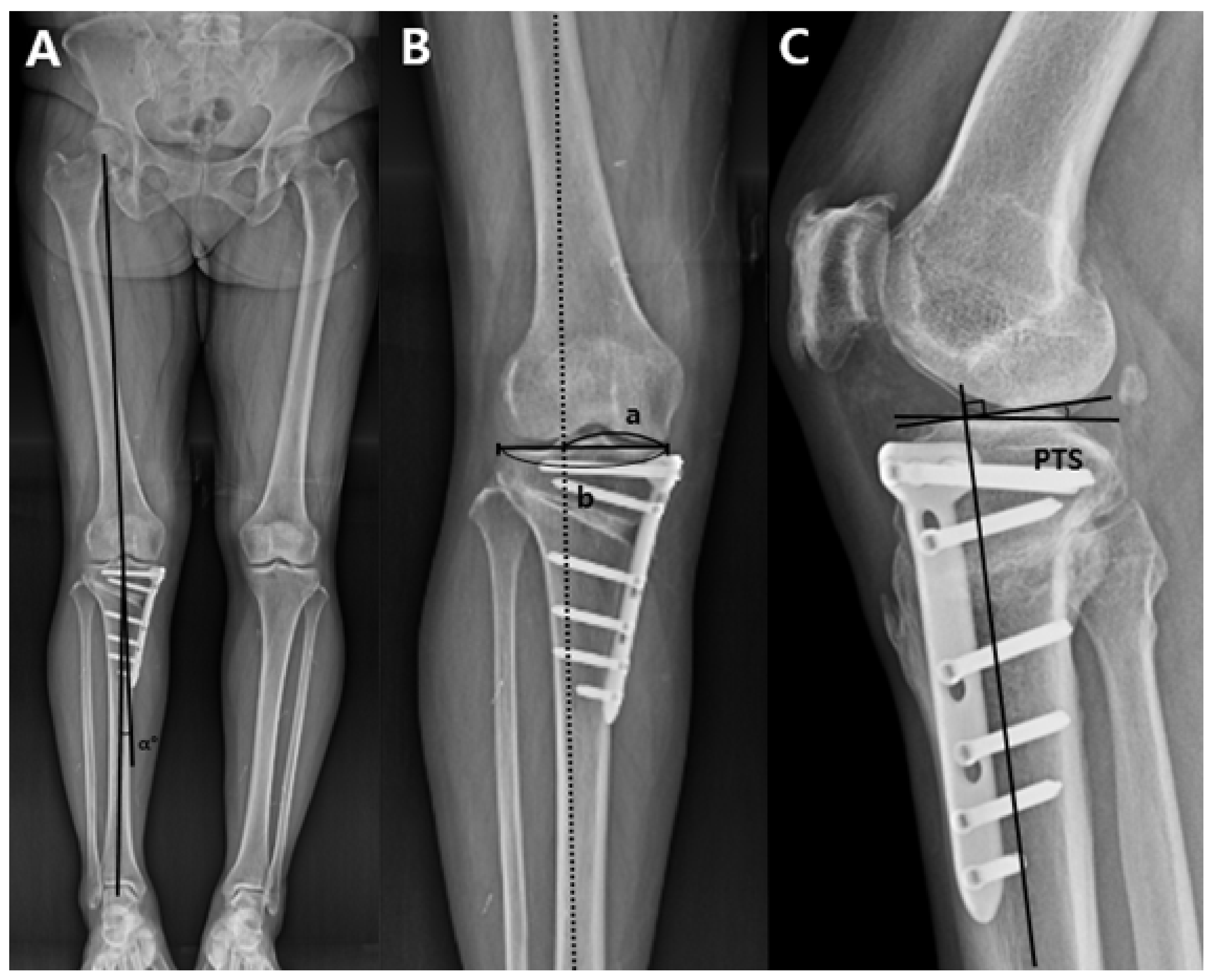
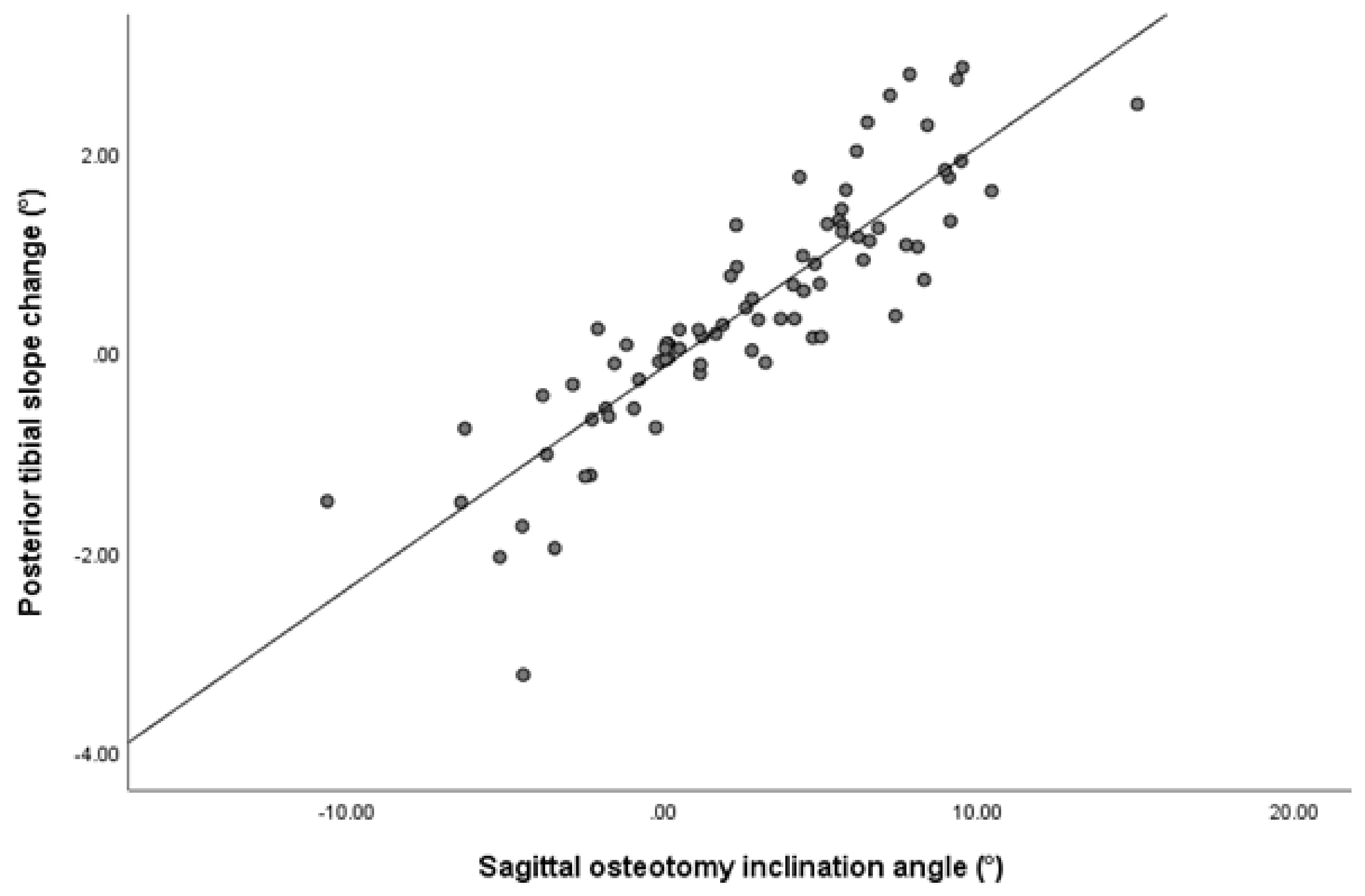
19], the majority of osteotomy lines in the sagittal plane were anteriorly inclined. According to the data measured with 3D reconstructed models, the preoperative posterior tibial slope was 9.7 ± 2.9° and postoperative posterior tibial slope was 10.7 ± 3.0° in group A. The preoperative posterior tibial slope was 8.7 ± 2.7° and the postoperative posterior tibial slope was 7.7 ± 2.7° in group P. The mean osteotomy inclination angle in the sagittal plane was 4.9 ± 3.2 in group A and −3.1 ± 2.5 in group P. Although there was no significant difference in the osteotomy opening gap ratio between the groups, the postoperative posterior tibial slope changed in different direction depending on the difference in the inclination angle in sagittal plane. When the osteotomy line was inclined anteriorly with respect to the medial tibial plateau line, the postoperative posterior tibial slope tended to increase. In contrast, when the osteotomy line was inclined posteriorly, the postoperative posterior tibial slope tended to decrease. Both the Pearson correlation (r = 0.875,
p < 0.001) and multiple regression analyses (β coefficient = 0.216,
p < 0.001) also showed a significant association between the osteotomy inclination angle in the sagittal plane and change in posterior tibial slope. Accordingly, to avoid inadvertent effects on the kinematics of the knee joint, close attention needs to be paid to maintaining the sagittal osteotomy line parallel to the medial joint line during MOWHTO. In addition, in cases where the treatment effect is expected by intentionally adjusting the posterior tibial slope, such as for osteoarthritis with anteroposterior instability, the posterior tibial slope could be controlled by varying the inclination angle of the osteotomy in the sagittal plane [
12].
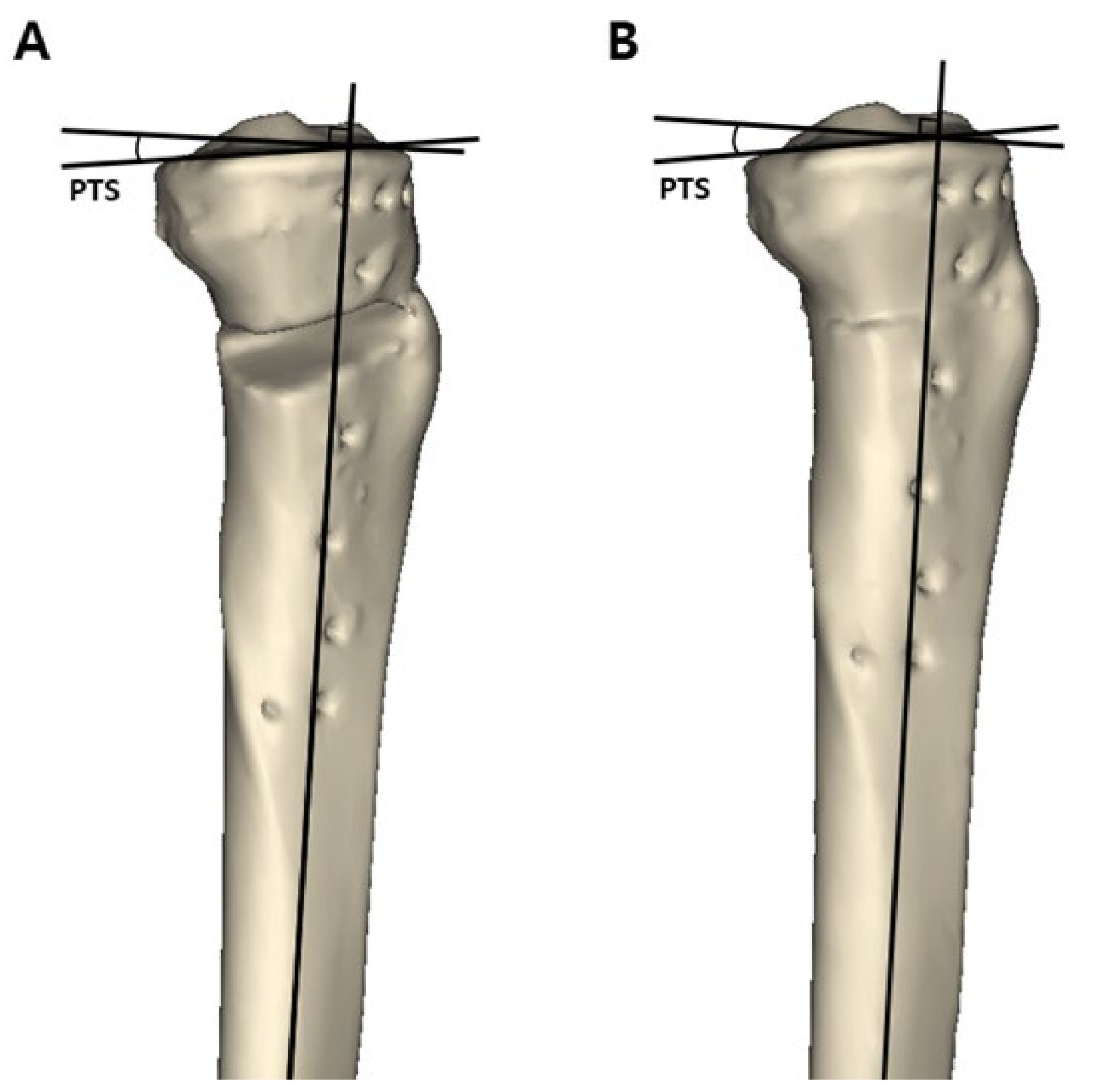
Another notable finding in this study was that measurements with 3D reconstructed models were more reliable than measurement with plain radiographs. When measured with plain radiographs, the intraclass correlation coefficients for interobserver reliability were 0.748 (95% CI, 0.607~0.838) for the preoperative posterior tibial slope and 0.759 (95% CI, 0.625~0.846) for the postoperative posterior tibial slope. However, when measured with 3D reconstructed models, the intraclass correlation coefficients for interobserver reliability were 0.928 (95% CI, 0.888~0.954) for the preoperative posterior tibial slope and 0.937 (95% CI, 0.902~0.960) for the postoperative posterior tibial slope. In comparing the preoperative and postoperative posterior tibial slopes in group P, measured values with plain radiographs did not differ significantly, but measured values with 3D reconstructed models differed significantly. There is still no established method for measuring the posterior tibial slope. A more reliable and generally agreeable method uses the medial tibial plateau line and anatomical axis of the proximal tibial shaft or tibial cortex line [
36]. However, the measurement method using plain radiographs has disadvantages such as poor reproducibility due to the difficulties in obtaining true lateral images of the tibia caused by rotation and distinguishing between the medial and lateral tibial plateau because they overlap [
37]. For these reasons, CT scans and magnetic resonance imaging have been recently used for measurement of the posterior tibial slope. In this study, measurements were performed with 3D reconstructed models using the method presented in previous studies [
25,
26]. The results of our study also demonstrated that measurements with 3D reconstructed models obtain more consistent values with higher interobserver reliability.
This study had several limitations. Firstly, this study was based on retrospectively collected data. In order to obtain a more solid conclusion, a prospective study design by means of a cadaver study or finite elements is needed. Secondly, a preoperative CT scan was not performed. The preoperative 3D tibia model was reconstructed by digitally removing the osteotomy gap from the postoperative 3D tibia model using a lateral hinge as a rotation axis. Although the preoperative 3D tibia model was restored as close to the actual preoperative tibia as possible, there could be a difference with the actual preoperative tibia. Thirdly, the number of patients in each study group was different. The majority of osteotomies in the sagittal plane were anteriorly inclined. Therefore, the number of patients in group A was larger than in group P. The relatively small number of patients could decrease statistical power. However, the calculated statistical power was 99.2%. Thus, the small number of patients in group P was not considered a serious problem. Fourthly, there was a statistically significant difference between the preoperative and postoperative posterior tibial slopes in all patients and in each group. There was also a statistically significant difference in postoperative posterior tibial slopes between the groups. However, as with the minimal clinically important difference, it has not been revealed how much the difference in posterior tibial slope actually affects the clinical outcomes. Accordingly, to determine the clinical effect of the change in posterior tibial slope on functional outcomes, a more in-depth study with long-term clinical follow-up results is needed.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




