
Association of Infliximab and Vedolizumab Trough Levels with Reported Rates of Adverse Events: A Cross-Sectional Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.1.1. Study Outcomes
- occurrence of any adverse events;
- number of adverse events per patient; and
- analysis per specific adverse event (Appendix A).
2.1.2. Definitions
- established diagnosis of Crohn’s disease or ulcerative colitis (based on endoscopy and histology or imaging);
- regular infliximab or vedolizumab treatment at the Sheba Medical Center in light of the above diagnosis;
- patients under maintenance treatment who have completed induction protocol (weeks 0, 2, and 6);
- available clinical, demographic, and clinical data, as well as drug trough levels; and
- age > 18 years.
2.2. Measurement of Vedolizumab Concentrations
2.3. Measurement of Infliximab Concentrations
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Patient Population and Demographics
3.2. Association of Drug Trough Levels with Occurrence of Adverse Events
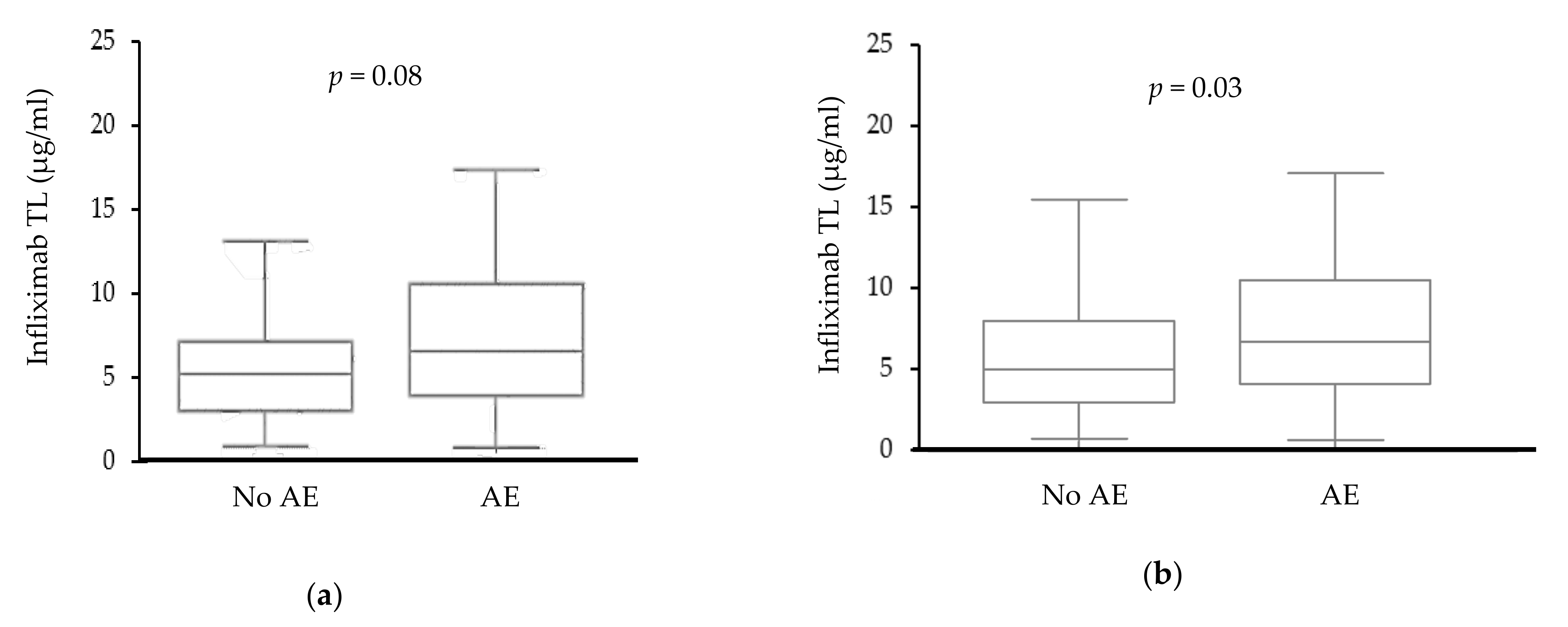
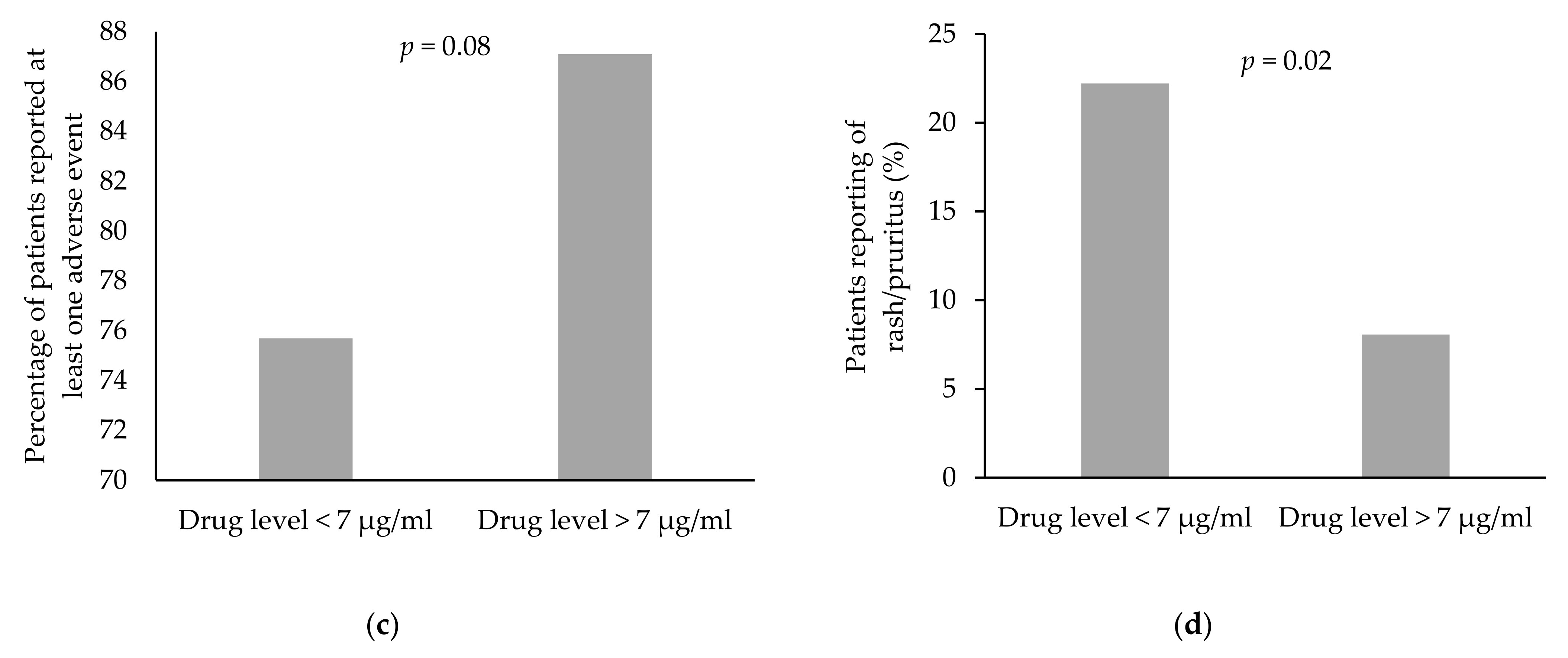
3.2.1. Infliximab
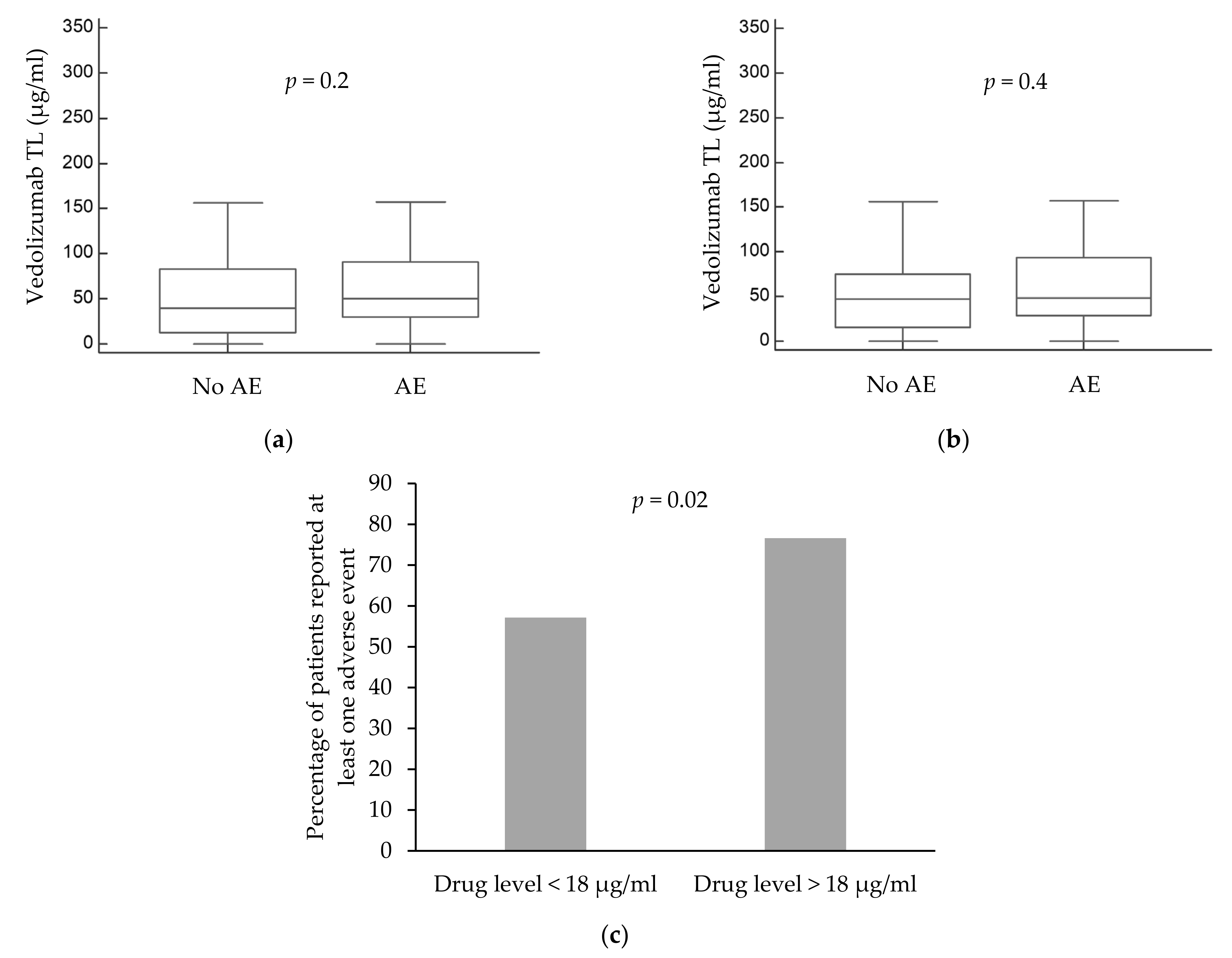
3.2.2. Vedolizumab
3.3. Drug Trough Levels and Serious AEs
3.3.1. Infliximab
3.3.2. Vedolizumab
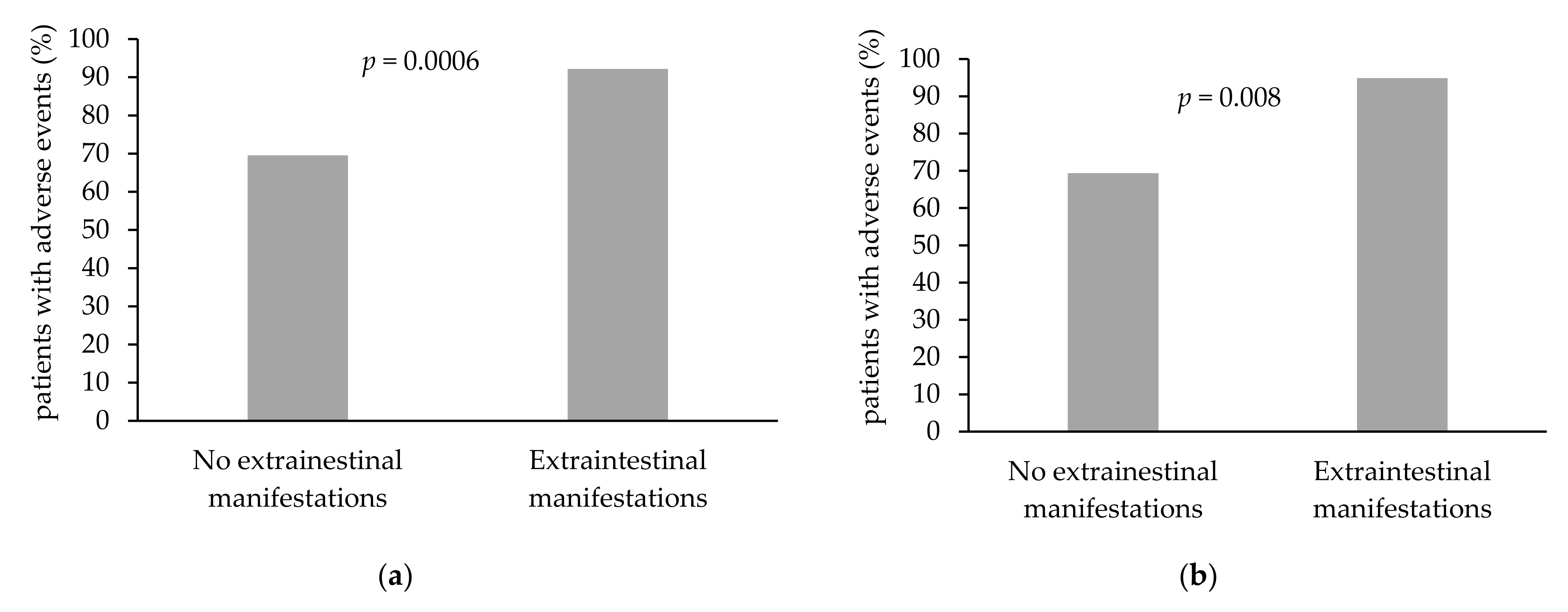
3.4. Association of Patient-Specific Characteristics with the Occurrence of Adverse Events
3.5. Factors Affecting the Occurrence of AE in the General Cohort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Adverse event/symptom | Did you experience: yes/no | Did it cause/resulted in treatment cessation: yes/no | Did you receive treatment for this adverse event, if yes, please elaborate: |
| headache | |||
| dizziness | |||
| abdominal pain | |||
| nausea or vomiting | |||
| fever | |||
| cough | |||
| dyspnea | |||
| sinusitis | |||
| pneumonia | |||
| pharyngitis | |||
| blushing | |||
| increased fatigue | |||
| rash/pruritis | |||
| urinary tract infection | |||
| arthralgia | |||
| arthritis | |||
| peripheral edema | |||
| parasthesia | |||
| bone pain | |||
| myalgia | |||
| muscle weakness | |||
| Other |
References
- Lichtenstein, G.R.; Feagan, B.G.; Cohen, R.D.; A Salzberg, B.; Diamond, R.H.; Price, S.; Langholff, W.; Londhe, A.; Sandborn, W.J. Serious infection and mortality in patients with Crohn’s disease: More than 5 years of follow-up in the TREAT™ registry. Am. J. Gastroenterol. 2012, 107, 1409–1422. [Google Scholar] [CrossRef] [Green Version]
- Park, S.C.; Jeen, Y.T. Anti-integrin therapy for inflammatory bowel disease. World J. Gastroenterol. 2018, 24, 1868–1880. [Google Scholar] [CrossRef] [Green Version]
- Sandborn, W.J.; Feagan, B.G.; Rutgeerts, P.; Hanauer, S.; Colombel, J.-F.; Sands, B.E.; Lukas, M.; Fedorak, R.; Lee, S.; Bressler, B.; et al. Vedolizumab as induction and maintenance therapy for Crohn’s disease. N. Engl. J. Med. 2013, 369, 711–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feagan, B.G.; Feagan, B.G.; Rutgeerts, P.; Hanauer, S.; Colombel, J.-F.; Sands, B.E.; Lukas, M.; Fedorak, R.; Lee, S.; Bressler, B.; et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2013, 369, 699–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, R.D.; Bhayat, F.; Blake, A.; Travis, S. The Safety Profile of Vedolizumab in Ulcerative Colitis and Crohn’s Disease: 4 Years of Global Post-marketing Data. J. Crohns. Colitis 2020, 14, 192–204. [Google Scholar] [CrossRef] [PubMed]
- Kopylov, U.; Seidman, E. Predicting durable response or resistance to antitumor necrosis factor therapy in inflammatory bowel disease. Therap. Adv. Gastroenterol. 2016, 9, 513–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoseyni, H.; Xu, Y.; Zhou, H. Therapeutic Drug Monitoring of Biologics for Inflammatory Bowel Disease: An Answer to Optimized Treatment? J. Clin. Pharmacol. 2018, 58, 864–876. [Google Scholar] [CrossRef] [PubMed]
- Greener, T.; Kabakchiev, B.; Steinhart, A.H.; Silverberg, M.S. Higher Infliximab Levels Are Not Associated With an Increase in Adverse Events in Inflammatory Bowel Disease. Inflamm. Bowel. Dis. 2018, 24, 1808–1814. [Google Scholar] [CrossRef]
- Ward, M.G.; Sparrow, M.P.; Roblin, X. Therapeutic drug monitoring of vedolizumab in inflammatory bowel disease: Current data and future directions. Therap. Adv. Gastroenterol. 2018, 11, 17562848–18772786. [Google Scholar] [CrossRef]
- Dreesen, E.; Verstockt, B.; Bian, S.; de Bruyn, M.; Compernolle, G.; Tops, S.; Noman, M.; Van Assche, G.; Ferrante, M.; Gils, A.; et al. Evidence to Support Monitoring of Vedolizumab Trough Concentrations in Patients With Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2018, 16, 1937–1946.e8. [Google Scholar] [CrossRef]
- Ungar, B.; Kopylov, U.; Yavzori, M.; Fudim, E.; Picard, O.; Lahat, A.; Coscas, D.; Waterman, M.; Haj-Natour, O.; Orbach-Zingboim, N.; et al. Association of Vedolizumab Level, Anti-Drug Antibodies, and α4β7 Occupancy With Response in Patients With Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2018, 16, 697–705.e7. [Google Scholar] [CrossRef] [Green Version]
- Ben-Horin, S.; Yavzori, M.; Katz, L.; Kopylov, U.; Picard, O.; Fudim, E.; Coscas, D.; Bar-Meir, S.; Goldstein, I.; Chowers, Y. The immunogenic part of infliximab is the F(ab’)2, but measuring antibodies to the intact infliximab molecule is more clinically useful. Gut 2011, 60, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Pouillon, L.; Ferrante, M.; Van Assche, G.; Rutgeerts, P.; Noman, M.; Sabino, J.; Casteele, N.V.; Gils, A.; Vermeire, S. Mucosal Healing and Long-term Outcomes of Patients With Inflammatory Bowel Diseases Receiving Clinic-Based vs. Trough Concentration-Based Dosing of Infliximab. Clin. Gastroenterol. Hepatol. 2018, 16, 1276–1283.e1. [Google Scholar] [CrossRef] [PubMed]
- Guidi, L.; Pugliese, D.; Tonucci, T.P.; Bertani, L.; Costa, F.; Privitera, G.; Tolusso, B.; Di Mario, C.; Albano, E.; Tapete, G.; et al. Early vedolizumab trough levels predict treatment persistence over the first year in inflammatory bowel disease. United Eur. Gastroenterol. J. 2019, 7, 1189–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pouillon, L.; Vermeire, S.; Bossuyt, P. Vedolizumab trough level monitoring in inflammatory bowel disease: A state-of-the-art overview. BMC Med. 2019, 17, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanauer, S.B. Review article: Safety of infliximab in clinical trials. Aliment. Pharmacol. Ther. 1999, 13 (Suppl. S4), 16–22. [Google Scholar] [CrossRef]
- Stamatiades, G.A.; Ioannou, P.; Petrikkos, G.; Tsioutis, C. Fungal infections in patients with inflammatory bowel disease: A systematic review. Mycoses 2018, 61, 366–376. [Google Scholar] [CrossRef] [PubMed]
- Inflammatory Bowel Disease Group, Chinese Society of Gastroenterology, Chinese Medical Association. Evidence-based consensus on opportunistic infections in inflammatory bowel disease (republication). Intest. Res. 2018, 16, 178–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hastings, R.; Ding, T.; Butt, S.; Gadsby, K.; Zhang, W.; Moots, R.J.; Deighton, C. Neutropenia in patients receiving anti-tumor necrosis factor therapy. Arthritis. Care Res. 2010, 62, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Salar, A.; Bessa, X.; Muñiz, E.; Monfort, D.; Besses, C.; Andreu, M. Infliximab and adalimumab-induced thrombocytopenia in a woman with colonic Crohn’s disease. Gut 2007, 56, 1169–1170. [Google Scholar] [CrossRef] [Green Version]
- Bessissow, T.; Renard, M.; Hoffman, I.; Vermeire, S.; Rutgeerts, P.; Van Assche, G. Review article: Non-malignant haematological complications of anti-tumour necrosis factor alpha therapy. Aliment. Pharmacol. Ther. 2012, 36, 312–323. [Google Scholar] [CrossRef]
- Vermeire, S.; Noman, M.; Van Assche, G.; Baert, F.; Van Steen, K.; Esters, N.; Joossens, S.; Bossuyt, X.; Rutgeerts, P. Autoimmunity associated with anti-tumor necrosis factor alpha treatment in Crohn’s disease: A prospective cohort study. Gastroenterology 2003, 125, 32–39. [Google Scholar] [CrossRef]
- Mariette, X.; Tubach, F.; Bagheri, H.; Bardet, M.; Berthelot, J.-M.; Gaudin, P.; Heresbach, D.; Martin, A.; Schaeverbeke, T.; Salmon, D.; et al. Lymphoma in patients treated with anti-TNF: Results of the 3-year prospective French RATIO registry. Ann. Rheum. Dis. 2010, 69, 400–408. [Google Scholar] [CrossRef]
- Rosen, T.; Martinelli, P. Erythema nodosum associated with infliximab therapy. Dermatol. Online J. 2008, 14, 3. [Google Scholar] [PubMed]
- Iborra, M.; Beltrán, B.; Bastida, G.; Aguas, M.; Nos, P. Infliximab and adalimumab-induced psoriasis in Crohn’s disease: A paradoxical side effect. J. Crohns. Colitis 2011, 5, 157–161. [Google Scholar] [CrossRef] [Green Version]
- Deepak, P.; Stobaugh, D.J.; Sherid, M.; Sifuentes, H.; Ehrenpreis, E.D. Neurological events with tumour necrosis factor alpha inhibitors reported to the Food and Drug Administration Adverse Event Reporting System. Aliment. Pharmacol. Ther. 2013, 38, 388–396. [Google Scholar] [CrossRef]
- Seror, R.; Richez, C.; Sordet, C.; Rist, S.; Gossec, L.; Direz, G.; Houvenagel, E.; Berthelot, J.-M.; Pagnoux, C.; Dernis, E.; et al. Pattern of demyelination occurring during anti-TNF-α therapy: A French national survey. Rheumatology 2013, 52, 868–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, E.S.; Packer, M.; Lo, K.H.; Fasanmade, A.A.; Willerson, J.T. Randomized, double-blind, placebo-controlled, pilot trial of infliximab, a chimeric monoclonal antibody to tumor necrosis factor-alpha, in patients with moderate-to-severe heart failure: Results of the anti-TNF Therapy Against Congestive Heart Failure (ATTACH) trial. Circulation 2003, 107, 3133–3140. [Google Scholar]
- Sote, Y.; Green, S.; Maddison, P. Complete heart block after infliximab therapy. Rheumatology 2008, 47, 227–228. [Google Scholar] [CrossRef] [Green Version]
- Prinz, J.C. Autoimmune-like syndromes during TNF blockade: Does infection have a role? Nat. Rev. Rheumatol. 2011, 7, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, S.; Dignass, A.; Peyrin-Biroulet, L.; Hather, G.; DeMuth, D.; Mosli, M.; Curtis, R.; Khalid, J.M.; Loftus, E. Systematic review with meta-analysis: Real-world effectiveness and safety of vedolizumab in patients with inflammatory bowel disease. J. Gastroenterol. 2018, 53, 1048–1064. [Google Scholar] [CrossRef] [Green Version]
- Narula, N.; Peerani, F.; Meserve, J.; Kochhar, G.; Chaudrey, K.; Hartke, J.; Chilukuri, P.; Koliani-Pace, K.; Winters, A.; Katta, L.; et al. Vedolizumab for Ulcerative Colitis: Treatment Outcomes from the VICTORY Consortium. Am. J. Gastroenterol. 2018, 113, 1345. [Google Scholar] [CrossRef]
- Zeissig, S.; Rosati, E.; Dowds, C.M.; Aden, K.; Bethge, J.; Schulte, B.; Pan, W.H.; Mishra, N.; Zuhayra, M.; Marx, M.; et al. Vedolizumab is associated with changes in innate rather than adaptive immunity in patients with inflammatory bowel disease. Gut 2019, 68, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, N.K.; Azizov, A.; Halder, S.; Xenodemetropoulos, T.; Armstrong, D.; Tse, F.; Marshall, J.; Narula, N. Higher vedolizumab serum levels do not increase the risk of adverse events in patients with inflammatory bowel disease. Scand. J. Gastroenterol. 2020, 55, 800–805. [Google Scholar] [CrossRef]
- Bodini, G.; Demarzo, M.G.; Saracco, M.; Coppo, C.; De Maria, C.; Baldissarro, I.; Savarino, E.; Savarino, V.; Giannini, E.G. High anti-TNF alfa drugs trough levels are not associated with the occurrence of adverse events in patients with inflammatory bowel disease. Scand. J. Gastroenterol. 2019, 54, 1220–1225. [Google Scholar] [CrossRef] [PubMed]
- Lie, M.R.; Kreijne, J.E.; van der Woude, C.J. Sex Is Associated with Adalimumab Side Effects and Drug Survival in Patients with Crohn’s Disease. Inflamm. Bowel. Dis. 2017, 23, 75–81. [Google Scholar] [CrossRef] [Green Version]
- Greuter, T.; Manser, C.; Pittet, V.; Vavricka, S.R.; Biedermann, L. Gender Differences in Inflammatory Bowel Disease. Digestion 2020, 101 (Suppl. 1), 98–104. [Google Scholar] [CrossRef]
- Hauser, G.; Tkalcic, M.; Stimac, D.; Milić, S.; Sincić, B.M. Gender related differences in quality of life and affective status in patients with inflammatory bowel disease. Coll. Antropol. 2011, 35 (Suppl. 2), 203–207. [Google Scholar] [PubMed]
- Saraiva, S.; Cortez-Pinto, J.; Barosa, R.; Castela, J.; Moleiro, J.; Rosa, I.; da Siva, J.P.; Dias Pereira, A. Evaluation of fatigue in inflammatory bowel disease—a useful tool in daily practice. Scand. J. Gastroenterol. 2019, 54, 465–470. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Infliximab N(%) | Vedolizumab N(%) | |
|---|---|---|---|
| Age (years, IQR) | 31, 26–41 | 40, 31–57 | |
| Gender (female) a | 60 (48%) | 36 (51%) | |
| Extraintestinal manifestations a | 57 (46%) | 33 (46%) | |
| Smoking a | 22 (18%) | 11 (15%) | |
| Previous surgery a | 27 (22%) | 17 (24%) | |
| Concomitant immunomodulator therapy a | 25 (20%) | 5 (7%) | |
| Concomitant methotrexate therapy a | 1 (1%) | 1 (1%) | |
| Concomitant corticosteroid therapy a | 9 (7%) | 7 (10%) | |
| Previous anti-TNF therapy a | 53 (4%) | 46 (65%) | |
| IBD type (UC) a | 27 (22%) | 37 (52%) | |
| CD—disease location b | Ileal | 52 (54%) | 15 (44%) |
| Colonic | 14 (14%) | 6 (18%) | |
| Ileocolonic | 30 (31%) | 13 (38%) | |
| Upper GI tract * | 1 (1%) | - | |
| CD—disease behavior b | Non-stricturing and non-penetrating | 38 (39%) | 16 (47%) |
| Stricturing | 30 (31%) | 11 (32%) | |
| Penetrating | 29 (30%) | 7 (21%) | |
| UC—disease location c | Extensive colitis | 17 (63%) | 21 (57%) |
| Left-sided colitis | 10 (37%) | 15 (41%) | |
| Proctitis | 0 (0%) | 1 (3%) | |
| Disease duration (years, IQR) | 8, 4–15 | 9, 4–18 | |
| Median trough level, µg/mL (IQR) | 5.3 μg/mL (3.1–9.1) | 47.9 μg/mL (28.2–87.2) | |
| Parameter | Infliximab | Vedolizumab | |||||||
|---|---|---|---|---|---|---|---|---|---|
| With AE N(%)/median | Without AE N(%)/median | OR (CI)/IQR | p-value | With AE N(%)/median | Without AE N(%)/median | OR (CI)/IQR | p-value | ||
| Age | 30 | 33 | 25–41; 28–41 | 0.4 | 47 | 38 | 31–61; 51–46 | 0.3 | |
| Disease duration | 8 | 6 | 5–15; 4–16 | 0.7 | 9 | 6 | 5–18; 3–16 | 0.4 | |
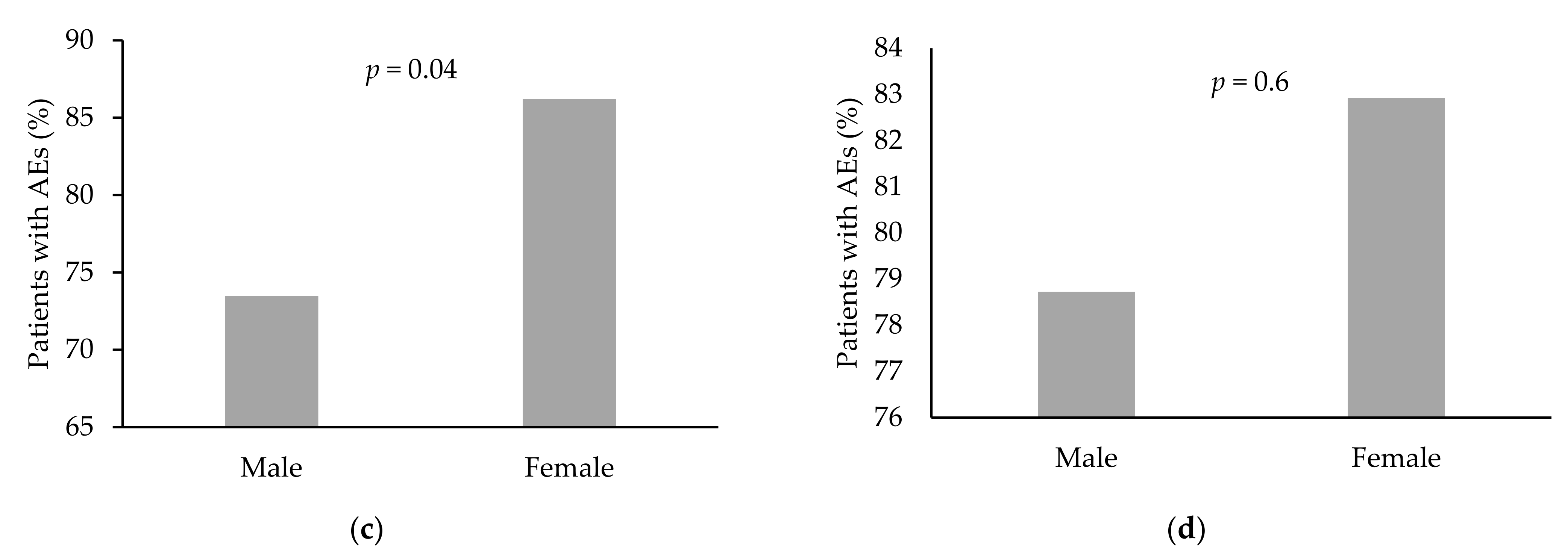
| Gender | Female | 75/86 (87.2%) | 11/86 (12.7%) | 2.2 (1.0–4.9) | 0.04 | 34/41 (82.9%) | 7/41 (17.1%) | 1.3 (0.4–3.8) | 0.6 |
| Male | 61/83 (73.5%) | 22/83 (26.5%) | 37/47 (78.7%) | 10/47 (21.3%) | |||||
| Extraintestinal manifestations | Yes | 71/77 (92.2%) | 6/77 (7.8%) | 5.1 (2.0–13.3) | 0.0006 | 37/39 (94.9%) | 2/39 (5.1%) | 8.1 (1.7–38.3) | 0.008 |
| No | 64/92 (69.6%) | 28/92 (30.4%) | 34/49 (69.4%) | 15/49 (30.6%) | |||||
| Smoking | Yes | 24/29 (82.8%) | 5/29 (17.2%) | 1.2 (0.4–3.5) | 0.7 | 13/14 (92.9%) | 1/14 (7.1%) | 0.2 (0.0–2.3) | 0.2 |
| No | 111/140 (79.3%) | 29/140 (20.7%) | 58/74 (78.4%) | 16/74 (21.6%) | |||||
| Previous surgery | Yes | 32/37 (86.5%) | 5/37 (13.5%) | 1.8 (0.6–5.0) | 0.3 | 19/21 (90.5%) | 2/21 (9.5%) | 2.7 (0.5–13.1) | 0.2 |
| No | 103/132 (78%) | 29/132 (22%) | 52/67 (77.6%) | 15/67 (22.4%) | |||||
| Concomitant immunomodulator therapy (Methotrexate/Azathioprine/purinethol) | Yes | 26/36 (72.2%) | 10/36 (27.8%) | 0.6 (0.2–1.3) | 0.2 | 9/10 (90%) | 1/10 (10%) | 2.3 (0.2–19.7) | 0.4 |
| No | 109/133 (82%) | 24/133 (18%) | 62/78 (79.5%) | 16/78 (20.5%) | |||||
| Concomitant corticosteroid therapy | Yes | 9/11 (81.8%) | 2/11 (18.2%) | 1.1 (0.2–5.5) | 0.9 | 7/8 (87.5%) | 1/8 (12.5%) | 1.7 (0.2–15.2) | 0.6 |
| No | 126/158 (79.7%) | 32/158 (20.3%) | 64/80 (80%) | 16/80 (20%) | |||||
| Previous anti-TNF therapy | Yes | 61/72 (84.7%) | 11/72 (15.3%) | 1.7 (0.7–3.8) | 0.2 | 48/57 (84.2%) | 9/57 (15.8%) | 1.8 (0.6–5.4) | 0.3 |
| No | 74/97 (76.3%) | 23/97 (23.7%) | 23/31 (74.2%) | 8/31 (25.8% | |||||
| IBD type | CD | 109/137 (79.6%) | 28/137 (20.4%) | 1.1 (0.4–2.9) | 0.8 | 35/41 (85.4%) | 6/41 (14.6%) | 0.5 (0.1–1.6) | 0.3 |
| UC | 26/32 (81.2%) | 6/32 (18.8%) | 36/47 (76.6%) | 11/47 (23.4%) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veisman, I.; Barzilay, O.; Bruckmayer, L.; Haj-Natour, O.; Kopylov, U.; Eliakim, R.; Ben-Horin, S.; Ungar, B. Association of Infliximab and Vedolizumab Trough Levels with Reported Rates of Adverse Events: A Cross-Sectional Study. J. Clin. Med. 2021, 10, 4265. https://doi.org/10.3390/jcm10184265
Veisman I, Barzilay O, Bruckmayer L, Haj-Natour O, Kopylov U, Eliakim R, Ben-Horin S, Ungar B. Association of Infliximab and Vedolizumab Trough Levels with Reported Rates of Adverse Events: A Cross-Sectional Study. Journal of Clinical Medicine. 2021; 10(18):4265. https://doi.org/10.3390/jcm10184265
Chicago/Turabian StyleVeisman, Ido, Oranit Barzilay, Liora Bruckmayer, Ola Haj-Natour, Uri Kopylov, Rami Eliakim, Shomron Ben-Horin, and Bella Ungar. 2021. "Association of Infliximab and Vedolizumab Trough Levels with Reported Rates of Adverse Events: A Cross-Sectional Study" Journal of Clinical Medicine 10, no. 18: 4265. https://doi.org/10.3390/jcm10184265