
Effects of Dry Needling in Teres Major Muscle in Elite Handball Athletes. A Randomised Controlled Trial

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Approval
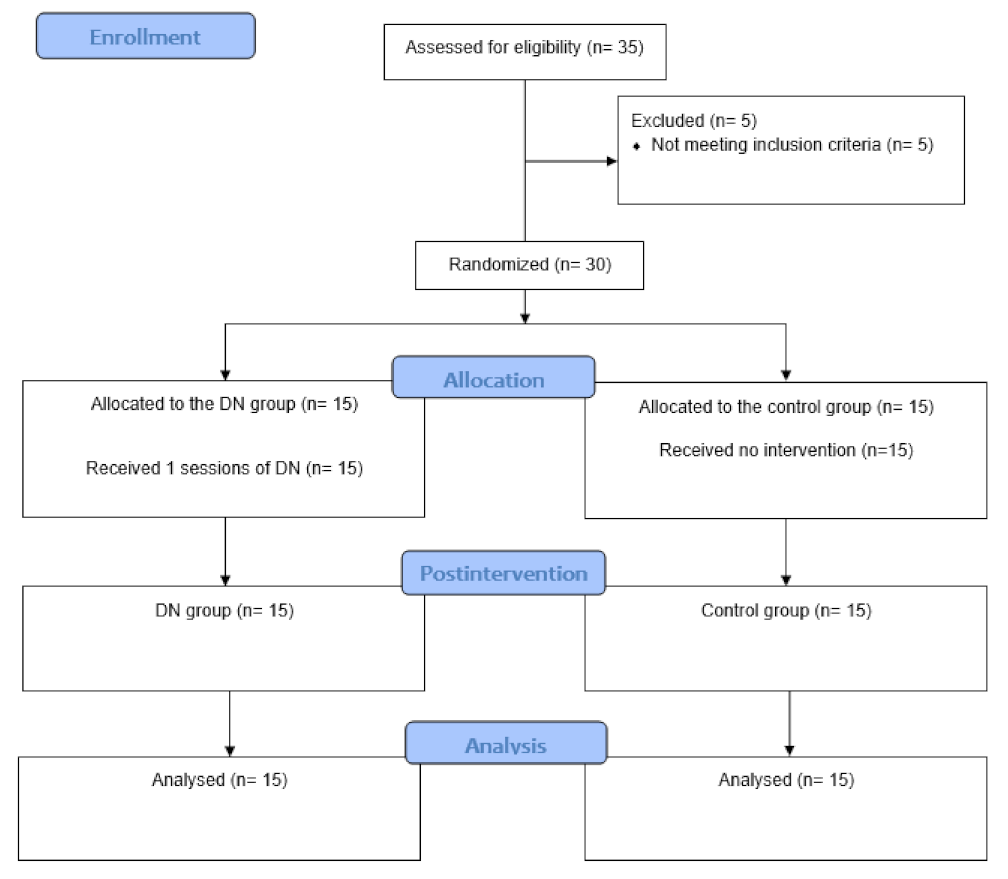
2.2. Sample Size
2.3. Participants
2.4. Randomization and Masking
2.5. Interventions
2.6. Outcomes
2.6.1. Pain Intensity
2.6.2. Passive Range of Motion
2.6.3. Muscle Strength
2.6.4. Extensibility
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sporis, G.; Vuleta, D.; Milanović, D. Fitness profiling in handball: Physical and physiological characteristics of elite players. Coll. Antropol. 2010, 34, 1009–1014. [Google Scholar] [PubMed]
- Kibler, W.B.; Kuhn, J.E.; Wilk, K.; Sciascia, A.; Moore, S.; Laudner, K.; Ellenbecker, T.; Thigpen, C.; Uhl, T. The disabled throwing shoulder: Spectrum of pathology—10-year update. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 141–161. [Google Scholar] [CrossRef] [PubMed]
- Karcher, C.; Buchheit, M. On-Court demands of elite handball, with special reference to playing positions. Sport Med. 2014, 44, 797–814. [Google Scholar] [CrossRef] [PubMed]
- Mohseni-Bandpei, M.A.; Keshavarz, R.; Minoonejhad, H.; Mohsenifar, H.; Shakeri, H. Shoulder Pain in Iranian Elite Athletes: The Prevalence and Risk Factors. J. Manip. Physiol. Ther. 2012, 35, 541–548. [Google Scholar] [CrossRef]
- Myklebust, G.; Hasslan, L.; Bahr, R.; Steffen, K. High prevalence of shoulder pain among elite Norwegian female handball players. Scand. J. Med. Sci. Sport 2013, 23, 288–294. [Google Scholar] [CrossRef]
- Wilk, K.E.; Macrina, L.C.; Fleisig, G.S.; Porterfield, R.; Ii, C.D.S.; Harker, P.; Paparesta, N.; Andrews, J.R. Correlation of Glenohumeral Internal Rotation Deficit and Total Rotational Motion to Shoulder Injuries in Professional Baseball Pitchers. Am. J. Sports Med. 2010, 39, 329–335. [Google Scholar] [CrossRef]
- Burkhart, S.S.; Morgan, C.D.; Kibler, W. The disabled throwing shoulder: Spectrum of pathology part I: Pathoanatomy and biomechanics. Arthrosc. J. Arthrosc. Relat. Surg. 2003, 19, 404–420. [Google Scholar] [CrossRef] [Green Version]
- Ceballos-Laita, L.; Pérez-Manzano, A.; Mingo-Gómez, T.; Hernando-Garijo, I.; Medrano-De-La-Fuente, R.; Estébanez-de-Miguel, E.; Barrio, J.D. Range of motion and muscle function on shoulder joints of young handball athletes. J. Back Musculoskelet. Rehabil. 2021, 1–7. [Google Scholar] [CrossRef]
- Wilk, K.E.; Meister, K.; Andrews, J.R. Current Concepts in the Rehabilitation of the Overhead Throwing Athlete. Am. J. Sports Med. 2002, 30, 136–151. [Google Scholar] [CrossRef]
- Burkhart, S.S.; Morgan, C.D.; Kibler, W.B. The disabled throwing shoulder: Spectrum of Pathology Part II: Evaluation and treatment of SLAP lesions in throwers. Arthrosc. J. Arthrosc. Relat. Surg. 2003, 19, 531–539. [Google Scholar] [CrossRef]
- Seabra, P.; Van Eck, C.F.; Sá, M.; Torres, J. Are professional handball players at risk for developing a glenohumeral internal rotation deficit in their dominant arm? Phys. Sportsmed. 2017, 45, 77–81. [Google Scholar] [PubMed]
- Almeida, G.P.L.; Silveira, P.F.; Rosseto, N.P.; Barbosa, G.; Ejnisman, B.; Cohen, M. Glenohumeral range of motion in handball players with and without throwing-related shoulder pain. J. Shoulder Elb. Surg. 2013, 22, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Tyler, T.F.; Nicholas, S.J.; Lee, S.J.; Mullaney, M.; McHugh, M.P. Correction of posterior shoulder tightness is associated with symptom resolution in patients with internal impingement. Am. J. Sports Med. 2010, 38, 114–119. [Google Scholar] [CrossRef]
- Keller, R.A.; De Giacomo, A.F.; Neumann, J.A.; Limpisvasti, O.; Tibone, J.E. Glenohumeral Internal Rotation Deficit and Risk of Upper Extremity Injury in Overhead Athletes: A Meta-Analysis and Systematic Review. Sports Health 2018, 10, 125–132. [Google Scholar] [CrossRef]
- Manske, R.C.; Meschke, M.; Porter, A.; Smith, B.; Reiman, M. A Randomized Controlled Single-Blinded Comparison of Stretching Versus Stretching and Joint Mobilization for Posterior Shoulder Tightness Measured by Internal Rotation Motion Loss. Sports Health 2009, 2, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Barra-López, M.E.; López-de-Celis, C.; Pérez-Bellmunt, A.; Puyalto-de-Pablo, P.; Sánchez-Fernández, J.J.; Lucha-López, M.O. The supporting role of the teres major muscle, an additional component in glenohumeral stability? An anatomical and radiological study. Med. Hypotheses 2020, 141, 109728. [Google Scholar] [CrossRef]
- Gerwin, R.D. Diagnosis of Myofascial Pain Syndrome. Phys. Med. Rehabil. Clin. 2014, 25, 341–355. [Google Scholar] [CrossRef]
- Simons, D.; Travell, J.G.; Simons, L. Myofascial Pain and Dysfunction: The Trigger Point Manual, 2nd ed; Editorial Panamericana: Madrid, Spain, 2007; Volume 44. [Google Scholar]
- Kietrys, D.M.; Palombaro, K.M.; Azzaretto, E.; Hubler, R.; Schaller, B.; Schlussel, J.M.; Tucker, M. Effectiveness of dry needling for upper-quarter myofascial pain: A systematic review and meta-analysis. J. Orthop. Sports Phys. Ther. 2013, 43, 620–634. [Google Scholar] [CrossRef] [Green Version]
- Dommerholt, J.; Mayoral del Moral, O.; Gröbli, C. Trigger Point Dry Needling. J. Man. Manip. Ther. 2006, 14, 70E–87E. [Google Scholar] [CrossRef]
- Kamali, F.; Sinaei, E.; Morovati, M. Comparison of Upper Trapezius and Infraspinatus Myofascial Trigger Point Therapy by Dry Needling in Overhead Athletes With Unilateral Shoulder Impingement Syndrome. J. Sport Rehabil. 2019, 28, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Santana, M.J.; Gómez-Chiguano, G.F.; Cleland, J.A.; Arias-Buria, J.L.; Fernández-de-las-Peñas, C.; Plaza-Manzano, G. Effects of Trigger Point Dry Needling for Nontraumatic Shoulder Pain of Musculoskeletal Origin: A Systematic Review and Meta-Analysis. Phys. Ther. Rehabil. J. 2020, 101, 216. [Google Scholar]
- Michener, L.A.; Snyder, A.R.; Leggin, B.G. Responsiveness of the Numeric Pain Rating Scale in Patients With Shoulder Pain and the Effect of Surgical Status. J. Sport Rehabil. 2011, 20, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Bron, C.; Franssen, J.; Wensing, M.; Oostendorp, R.A. Interrater Reliability of Palpation of Myofascial Trigger Points in Three Shoulder Muscles. J. Man. Manip. Ther. 2007, 15, 203–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, C.; Torigoe, Y. Electrophysiological characteristics of localized twitch responses in responsive taut bands of rabbit skeletal muscle fibers. J. Musculoskelet. Pain. 1994, 2, 17–43. [Google Scholar] [CrossRef]
- Hong, C.-Z.; Torigoe, Y.; Yu, J. The Localized Twitch Responses in Responsive Taut Bands of Rabbit Skeletal Muscle Fibers Are Related to the Reflexes at Spinal Cord Level. J. Musculoskelet. Pain 1995, 3, 15–33. [Google Scholar] [CrossRef]
- Ceballos-Laita, L.; Jiménez-del-Barrio, S.; Marín-Zurdo, J.; Moreno-Calvo, A.; Marín-Boné, J.; Albarova-Corral, M.I.; Estébanez-de-Miguel, E. Effectiveness of Dry Needling Therapy on Pain, Hip Muscle Strength and Physical Function in Patients With Hip Osteoarthritis: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2021, 102, 959–966. [Google Scholar] [CrossRef]
- Jensen, M.P.; Turner, J.A.; Romano, J.M.; Fisher, L.D. Comparative reliability and validity of chronic pain intensity measures. Pain 1999, 83, 157–162. [Google Scholar] [CrossRef]
- Fieseler, G.; Jungermann, P.; Koke, A.; Irlenbusch, L.; Delank, K.S.; Schwesig, R. Range of motion and isometric strength of shoulder joints of team handball athletes duringthe playing season, part II: Changes after midseason. J. Shoulder Elb. Surg. 2015, 24, 391–398. [Google Scholar] [CrossRef]
- Fieseler, G.; Jungermann, P.; Koke, A.; Irlenbusch, L.; Delank, K.S.; Schwesig, R. Glenohumeral range of motion (ROM) and isometric strength of professional team handball athletes, part III: Changes over the playing season. Arch. Orthop. Trauma Surg. 2015, 135, 1691–1700. [Google Scholar] [CrossRef]
- Romero-Franco, N.; Fernández-Domínguez, J.C.; Montaño-Munuera, J.A.; Romero-Franco, J.; Jiménez-Reyes, P. Validity and reliability of a low-cost dynamometer to assess maximal isometric strength of upper limb: Low cost dynamometry and isometric strength of upper limb. J. Sports Sci. 2019, 37, 1787–1793. [Google Scholar] [CrossRef]
- Tyler, T.F.; Roy, T.; Nicholas, S.J.; Gleim, G.W.; Davies, G.J.; Wilk, K.E.; Ellenbecker, T. Reliability and Validity of a New Method of Measuring Posterior Shoulder Tightness. J. Orthop. Sports Phys. Ther. 1999, 29, 262–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyler, T.F.; Nicholas, S.J.; Roy, T.; Gleim, G.W. Quantification of posterior capsule tightness and motion loss in patients with shoulder impingement. Am. J. Sports Med. 2000, 28, 668–673. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Hillsdale, N.J., Ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1988. [Google Scholar]
- Calvo-Lobo, C.; Pacheco-da-Costa, S.; Martínez-Martínez, J.; Rodríguez-Sanz, D.; Cuesta-Álvaro, P.; López-López, D. Dry Needling on the Infraspinatus Latent and Active Myofascial Trigger Points in Older Adults With Nonspecific Shoulder Pain. J. Geriatr. Phys. Ther. 2018, 41, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, J.P.; Danoff, J.V.; Desai, M.J.; Parikh, S.; Nakamura, L.Y.; Phillips, T.M.; Gerber, L.H. Biochemicals Associated With Pain and Inflammation are Elevated in Sites Near to and Remote From Active Myofascial Trigger Points. Arch. Phys. Med. Rehabil. 2008, 89, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.-L.; Yang, S.-A.; Yang, C.-C.; Chou, L.-W. Dry Needling at Myofascial Trigger Spots of Rabbit Skeletal Muscles Modulates the Biochemicals Associated with Pain, Inflammation, and Hypoxia. Evid.-Based Complement. Altern. Med. 2012, 2012, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Cerezo-Téllez, E.; Torres-Lacomba, M.; Fuentes-Gallardo, I.; Perez-Muñoz, M.; Mayoral-del-Moral, O.; Lluch-Girbés, E.; Prieto-Valiente, L.; Falla, D. Effectiveness of dry needling for chronic non-specific neck pain. Pain 2016, 157, 1905–1917. [Google Scholar] [CrossRef] [Green Version]
- Mansfield, C.; Vanetten, L.; Willy, R.; Di Stasi, S.; Robert, M.; Briggs, M. The effects of needling therapies on muscle force production. A systematic review and Meta-Analysis. J. Orthop. Sports Phys. Ther. 2018, 49, 154–170. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Outcomes | DN Group | Control Group | p-Value |
|---|---|---|---|
| Age (years) | 22.47 (3.04) | 22.31 (4.37) | U = 106.50; p = 0.591 |
| Height (cm) | 182.20 (9.21) | 186.25 (6.99) | F = 1.91; p = 0.177 |
| Weight (Kg) | 80.33 (10.80) | 85.56 (11.52) | F = 1.69; p = 0.203 |
| BMI (Kg/cm2) | 24.17 (2.57) | 24.64 (2.80) | F = 0.22; p = 0.637 |
| NPRS | 3.96 (2.20) | 3.56 (2.84) | U = 101.00; p = 0.894 |
| IR ROM (°) | 22.00 (6.49) | 25.78 (5.65) | F = 3.00; p = 0.109 |
| ER ROM (°) | 95.60 (10.54) | 98.03 (6.21) | F = 0.62; p = 0.437 |
| GIRD (°) | −25.63 (8.9) | −25.46 (8.13) | F = 0.01; p = 0.958 |
| ERG (°) | 8.43 (7.68) | 5.40 (12.42) | F = 0.65; p = 0.425 |
| IR strength (Kg) | 13.06 (1.96) | 13.93 (2.99) | F = 0.88; p = 0.353 |
| ER strength (Kg) | 16.52 (3.98) | 16.25 (3.58) | F = 0.03; p = 0.844 |
| Extensibility (°) | −14.43 (6.73) | −13.34 (4.76) | F = 0.27; p = 0.605 |
| Outcomes | Baseline Mean (SD) | Postintervention Mean (SD) | Within-Group Changes | Effect Size | Between-Groups p-Values | Effect Size |
|---|---|---|---|---|---|---|
| Pain intensity | ||||||
| DN group | 3.96 (2.20) | 0.65 (0.71) | −3.30 (2.02, 4.59) p < 0.001 | 2.0 | F = 21.72; p < 0.001 | 1.3 |
| Control group | 3.56 (2.84) | 3.06 (2.50) | −0.50 (−0,05, 1.05) p = 0.072 | 0.1 | ||
| IR ROM (°) | ||||||
| DN group | 22.00 (6.49) | 45.26 (6.54) | 23.26 (−28.12, −18.40) p < 0.001 | 3.5 | F = 102.70; p < 0.001 | 3.0 |
| Control group | 25.78 (5.65) | 26.40 (5.82) | 0.62 (−1.53, 0.28) p = 0.164 | 0.1 | ||
| ER ROM (°) | ||||||
| DN group | 95.60 (10.54) | 89.06 (11.07) | −6.53 (−0.41, 13.48) p = 0.063 | 0.6 | F = 5.57; p = 0.025 | 1.0 |
| Control group | 98.03 (6.21) | 99.12 (6.75) | 1.09 (−2.69, 0.50) p = 0.166 | 0.1 | ||
| GIRD (°) | ||||||
| DN group | −25.63 (8.9) | −2.50 (9.03) | 23.13 (−27.96, −18.30) p < 0.001 | 2.5 | F = 80.50; p < 0.001 | 2.6 |
| Control group | −25.46 (8.13) | −26.21 (8.75) | −0.75 (−2.40, 3.90) p = 0.619 | 0.1 | ||
| ERG (°) | ||||||
| DN group | 8.43 (7.68) | 1.90 (13.11) | −6.53 (−0.41, 13.48) p = 0.063 | 0.6 | F = 5.57; p = 0.025 | 0.3 |
| Control group | 5.40 (12.42) | 6.50 (12.44) | 1.09 (−2.69, 0.50) p = 0.166 | 0.1 | ||
| IR Strength (Kg) | ||||||
| DN group | 13.06 (1.96) | 13.51 (2.69) | 0.44 (−1.53, 0.63) p = 0.392 | 0.1 | F = 0.11; p = 0.773 | 0.2 |
| Control group | 13.93 (2.99) | 14.18 (2.80) | 0.25 (−0.78, 0.27) p = 0.321 | 0.1 | ||
| ER Strength (Kg) | ||||||
| DN group | 16.52 (3.98) | 17.27 (4.35) | 0.75 (−1.85, 0.35) p = 0.165 | 0.1 | F = 0.02; p = 0.884 | 0.1 |
| Control group | 16.25 (3.58) | 16.88 (4.34) | 0.63 (−1.99, 0.73) p = 0.339 | 0.1 | ||
| Extensibility (°) | ||||||
| DN group | −14.43 (6.73) | −0.8 (3.78) | 13.63 (−17.19, −10.07) p < 0.001 | 2.5 | F = 53.32; p < 0.001 | 2.9 |
| Control group | −13.34 (4.76) | −15.96 (6.34) | −2.62 (−0.55, 5.80) p = 0.099 | 0.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceballos-Laita, L.; Medrano-de-la-Fuente, R.; Estébanez-De-Miguel, E.; Moreno-Cerviño, J.; Mingo-Gómez, M.T.; Hernando-Garijo, I.; Jiménez-del-Barrio, S. Effects of Dry Needling in Teres Major Muscle in Elite Handball Athletes. A Randomised Controlled Trial. J. Clin. Med. 2021, 10, 4260. https://doi.org/10.3390/jcm10184260
Ceballos-Laita L, Medrano-de-la-Fuente R, Estébanez-De-Miguel E, Moreno-Cerviño J, Mingo-Gómez MT, Hernando-Garijo I, Jiménez-del-Barrio S. Effects of Dry Needling in Teres Major Muscle in Elite Handball Athletes. A Randomised Controlled Trial. Journal of Clinical Medicine. 2021; 10(18):4260. https://doi.org/10.3390/jcm10184260
Chicago/Turabian StyleCeballos-Laita, Luis, Ricardo Medrano-de-la-Fuente, Elena Estébanez-De-Miguel, Jorge Moreno-Cerviño, María Teresa Mingo-Gómez, Ignacio Hernando-Garijo, and Sandra Jiménez-del-Barrio. 2021. "Effects of Dry Needling in Teres Major Muscle in Elite Handball Athletes. A Randomised Controlled Trial" Journal of Clinical Medicine 10, no. 18: 4260. https://doi.org/10.3390/jcm10184260