1. Introduction
Colorectal cancer (CRC) is a significant global health burden, ranking third in cancer-associated mortality among all types of malignancies [
1,
2,
3]. The clinical features and prognosis of CRC are highly heterogeneous in histopathological subtypes [
4,
5,
6,
7]. Signet-ring cell carcinoma (SRCC) is a very rare histopathological subtype of CRC that constitutes approximately 1% of CRC cases [
8,
9]. SRCC is defined as carcinoma with >50% of signet-ring cells, characterized by intracytoplasmic mucin that displaces the nucleus to the periphery [
10,
11,
12]. SRCCs mostly originate from undifferentiated stem cells of the colorectal mucosa and often show poor differentiation, diffuse infiltration, rapid growth, and high metastatic frequency [
13,
14]. SRCCs have an extremely poor prognosis as they are generally detected at an advanced stage and are in an unresectable state [
12,
15,
16,
17,
18]. Despite its rarity, colorectal SRCC is clinically crucial because it is associated with a poor survival outcome.
To date, limited population-based studies on the incidence and survival rates of colorectal SRCCs have been reported, possibly because of its low incidence. All previous studies used Western population databases, generally the Surveillance, Epidemiology, and End Results (SEER) database, which is the largest cancer dataset in the United States [
8,
19,
20,
21]. However, there is a survival disparity between Western and Asian CRC owing to differences in biology and socioeconomic status; hence, investigation of the incidence and survival rates of colorectal SRCC in Asians is necessary [
22]. The present nationwide population-based study analyzed Korea Central Cancer Registry (KCCR) data between 1999 and 2017.
2. Materials and Methods
The Korean National Cancer Incidence Database (KNCIDB), a nationwide population-based database of cancer occurrence, was constructed by the KCCR of the National Cancer Center (Goyang, South Korea) [
23]. We obtained the necessary approval from the KCCR. The KNCIDB classifies cancer according to the International Classification of Diseases for Oncology, third edition (ICD-O-3) [
11]. We used ICD code 8490/3 to retrieve data on SRCC from the KNCIDB. ICD codes C18 and C19–20 were used to define colon cancer and rectal cancer, respectively. These methods are used widely in other studies [
21,
24,
25]. That is, the diagnosis in the Korean National Cancer Registry is based on pathology.
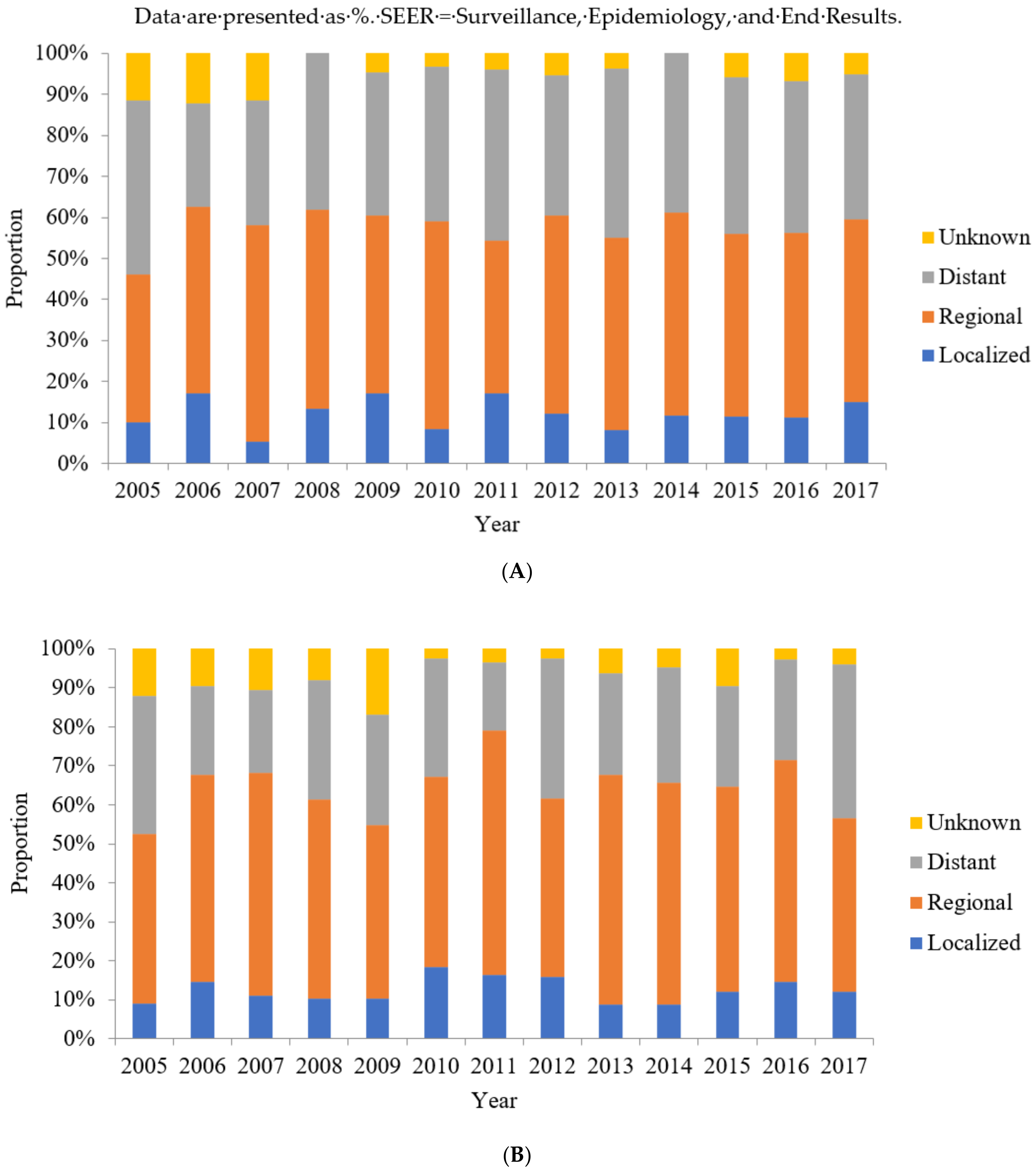
A total of 10,780 patients who were diagnosed with colorectal SRCC between 1999 and 2017 were identified in the KNCIDB, which included data on patient age and sex and the SEER summary stages of the tumor. The SEER summary stages, which are used to categorize tumor stage in the KNCIDB, include localized, regional, distant, and unknown stages.
The crude incidence rate was defined as the total number of newly diagnosed cases in a year divided by the mid-year population in South Korea [
26]. The age-standardized incidence rate, the weighted average of the age-specific rates, was calculated using Segi’s world standard population [
26,
27]. The relative survival rate (RSR) was defined as the ratio of the observed survival rate to the expected survival rate. The expected survival rate, defined as the expected mortality of the general population of the same age and sex, was calculated using the Ederer II method [
26,
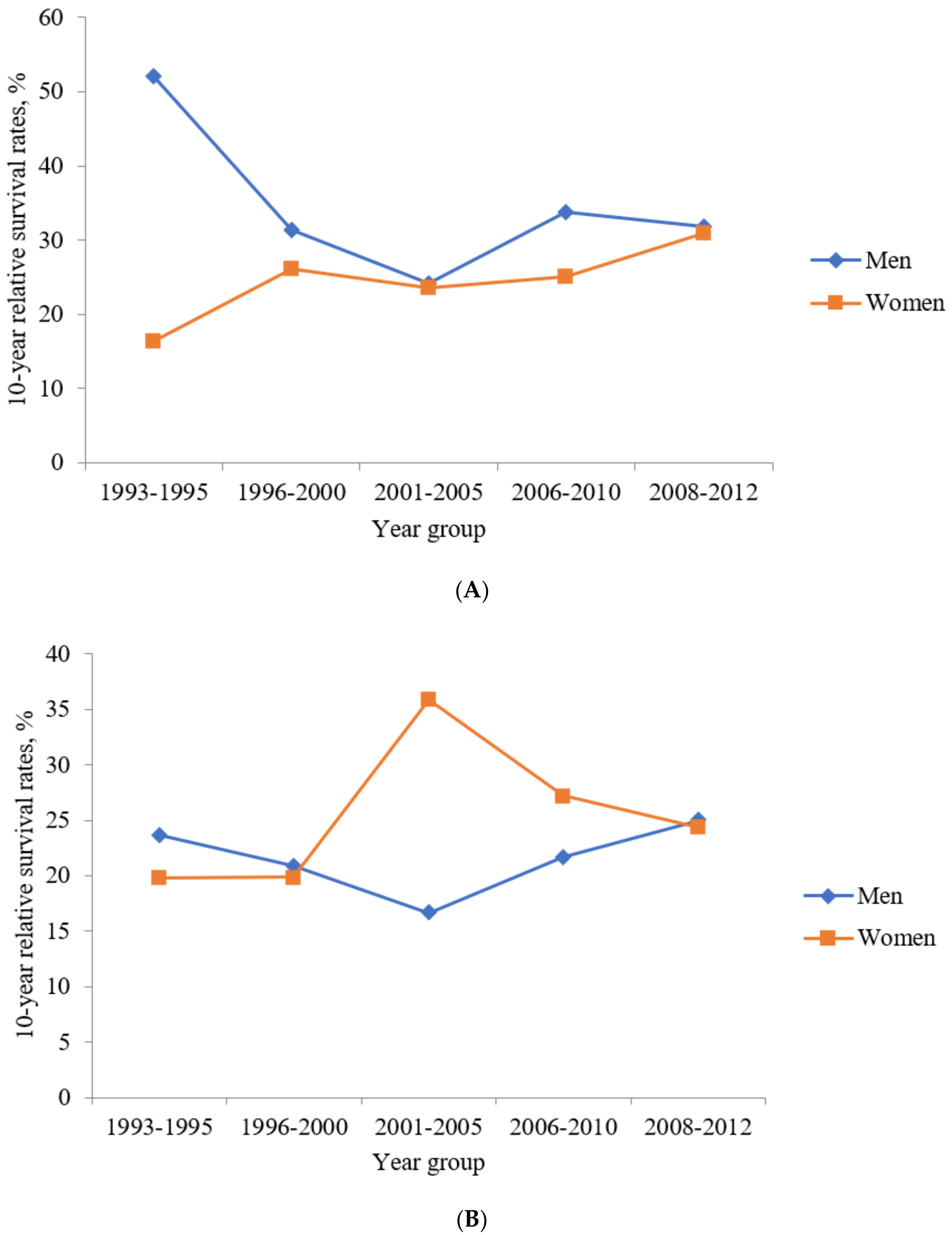
28]. The 5-year RSR was calculated for the following periods: 1993–1995, 1996–2000, 2001–2005, 2006–2010, 2011–2015, and 2013–2017. The 10-year RSR was calculated for the following periods: 1993–1995, 1996–2000, 2001–2005, 2006–2010, and 2008–2012. SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA) was used for statistical analysis.
Ethics Statement
This study was approved by the Institutional Review Board of Wonju Severance Christian Hospital (CR319145), which waived the requirement for informed consent from the patients.
4. Discussion
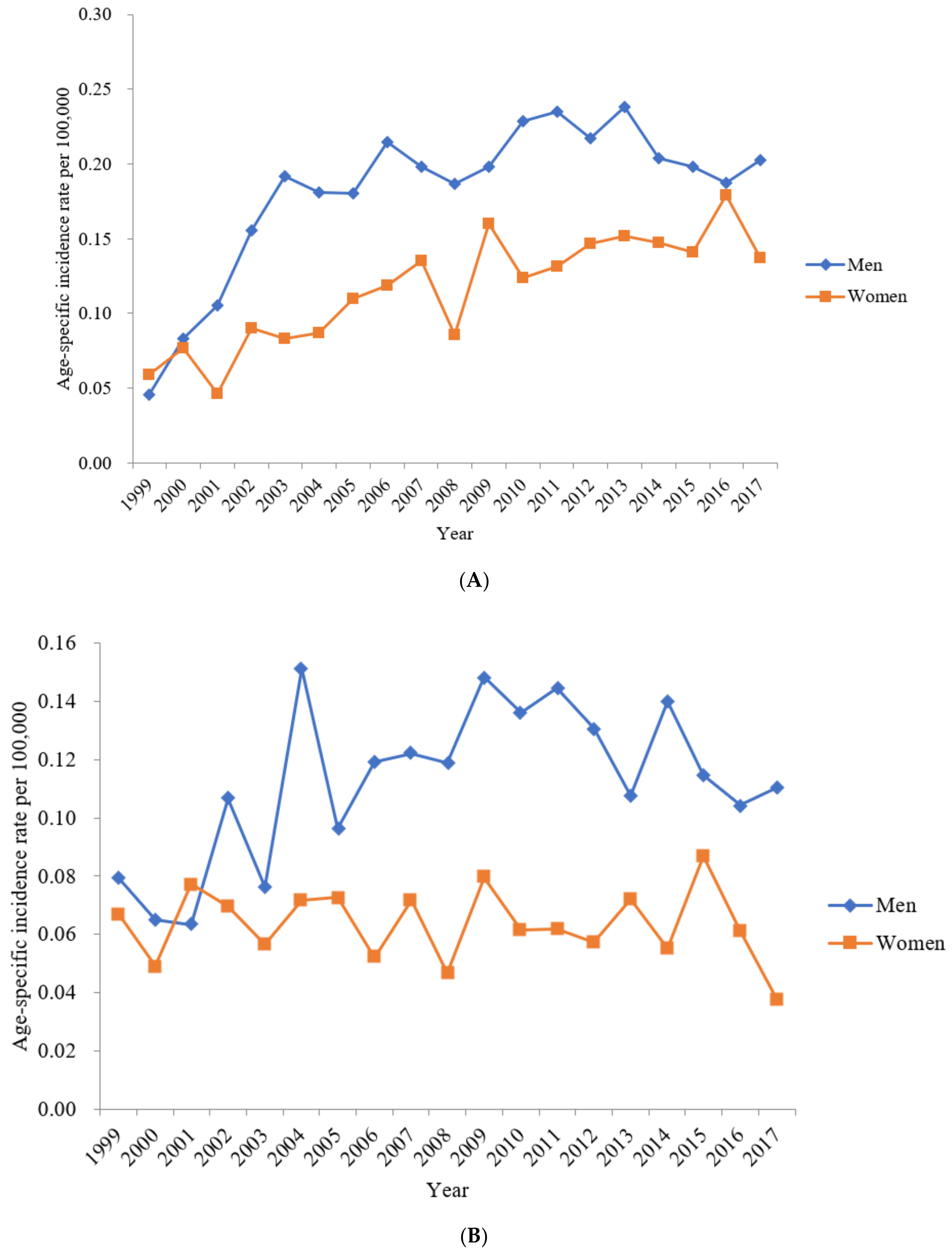
Our study evaluated the nationwide incidence and survival rates of colorectal SRCCs in South Korea, the incidence of which was extremely low. In 2017, only 168 individuals of the 51.4 million population in South Korea were diagnosed with colorectal SRCC. In addition, the results of our study revealed that the age-standardized incidence rate of colon SRCC has gradually increased, while that of rectum SRCC has remained stable, from 1999 to 2017.
A population-based study conducted in the United States reported that 4740 and 936 patients were diagnosed with colon SRCC and rectum SRCC between 2000 and 2014, respectively, with the highest age-adjusted incidence rates of 0.41 and 0.075 per 100,000 individuals, respectively, for colon SRCC and rectum SRCC [
19]. In our study, the highest age-standardized incidence rates during 2000–2014 were 0.19 per 100,000 individuals for colon SRCC and 0.10 per 100,000 individuals for rectum SRCC. The age-adjusted incidence rates for colon SRCC in the United States gradually decreased from 2000 to 2014, while those in South Korea have gradually increased [
19]. We must be careful when comparing and interpreting these incidences. This is because the definitions of terms used in the studies are different. In addition, it should be kept in mind that Korea cannot be directly compared to the multiethnic United States because it is relatively monoethnic.
The National Cancer Institute’s SEER database from 1975–2016 showed that SRCC comprised 1.0% of all cases of colorectal cancer [
24]. Other studies reported that SRCC consist of 0.1–2.6% of CRC [
18,
29]. In our study, SRCC comprised 0.59% (168 patients) of all colorectal cancer (28,111 patients) in 2017, and our results fall within this range.
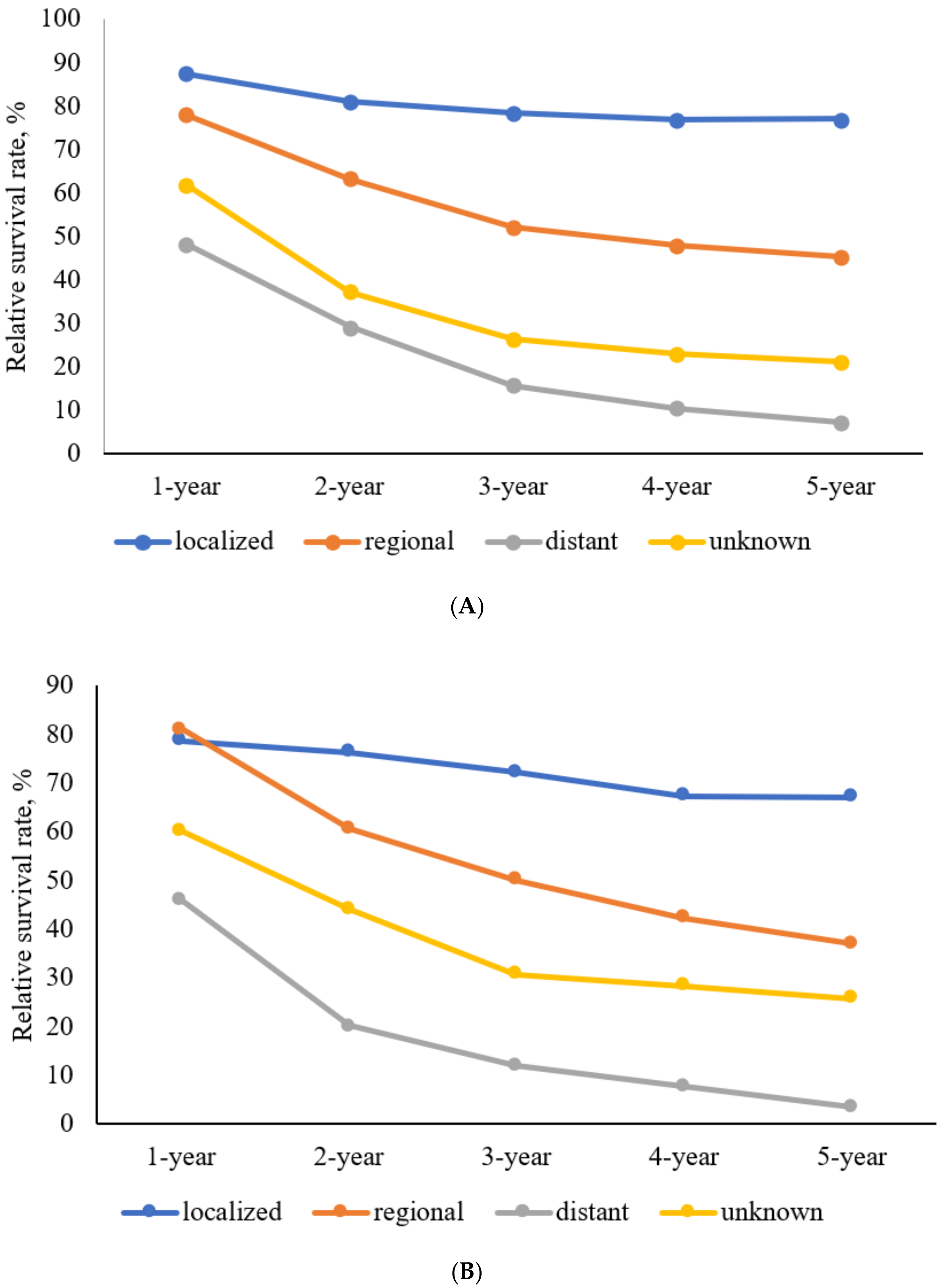
Colorectal SRCC is associated with a poor prognosis as it is generally diagnosed at an advanced stage [
12,
15,
16,
17,
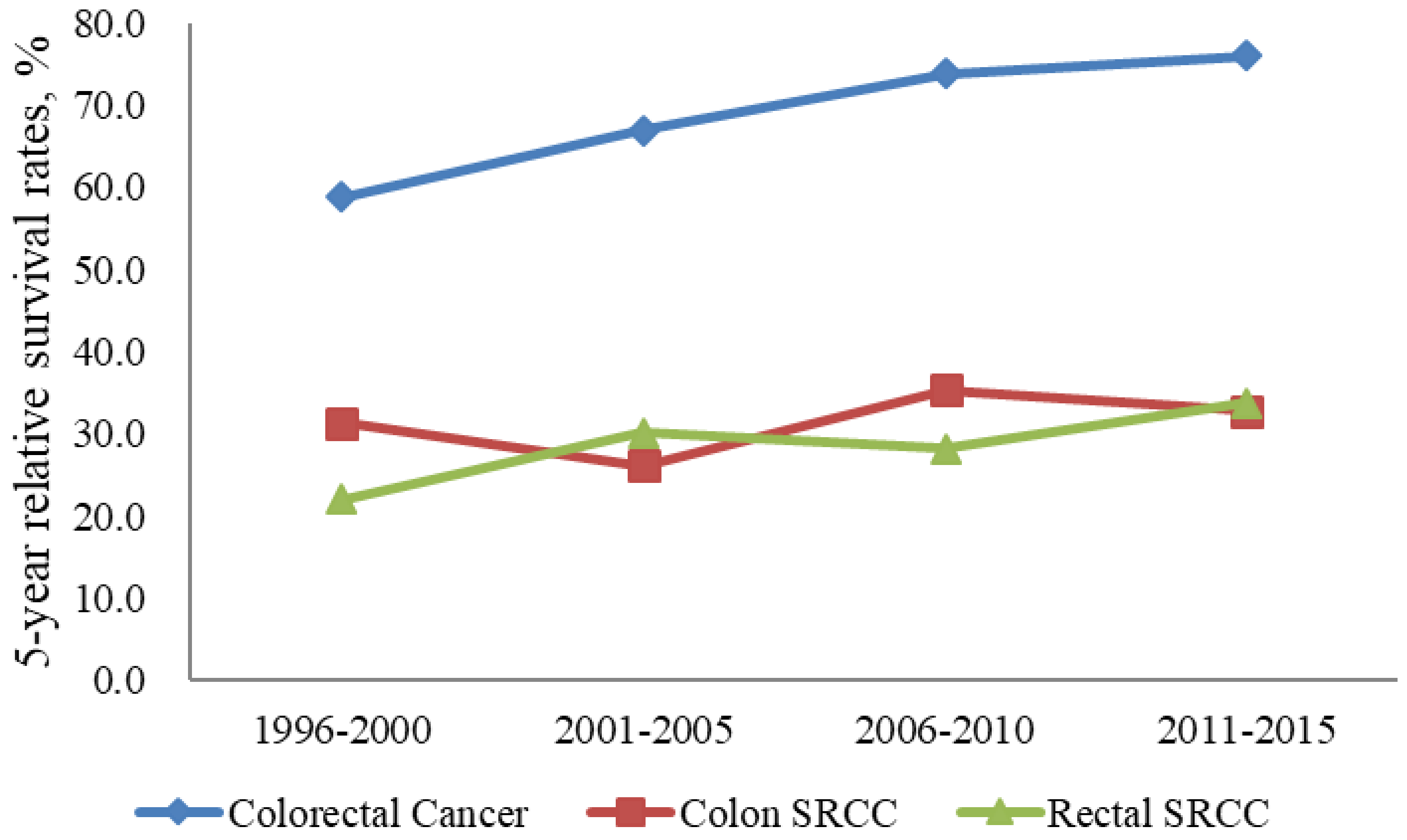
18]. In our study, the proportions of cases with distant metastasis were the second largest among colon SRCC and rectum SRCC cases. The 5-year RSRs of patients in South Korea with colon SRCC and rectum SRCC were 33.0% and 29.4%, respectively, between 1993 and 2017. In the United States, the 5-year RSRs of patients with colon SRCC and rectum SRCC were 28.6% and 21.1%, respectively, between 1992 and 2000 [
8]. In our study, the 5-year RSR of colon SRCC was higher than that of rectum SRCC, consistent with the findings of other studies [
8,
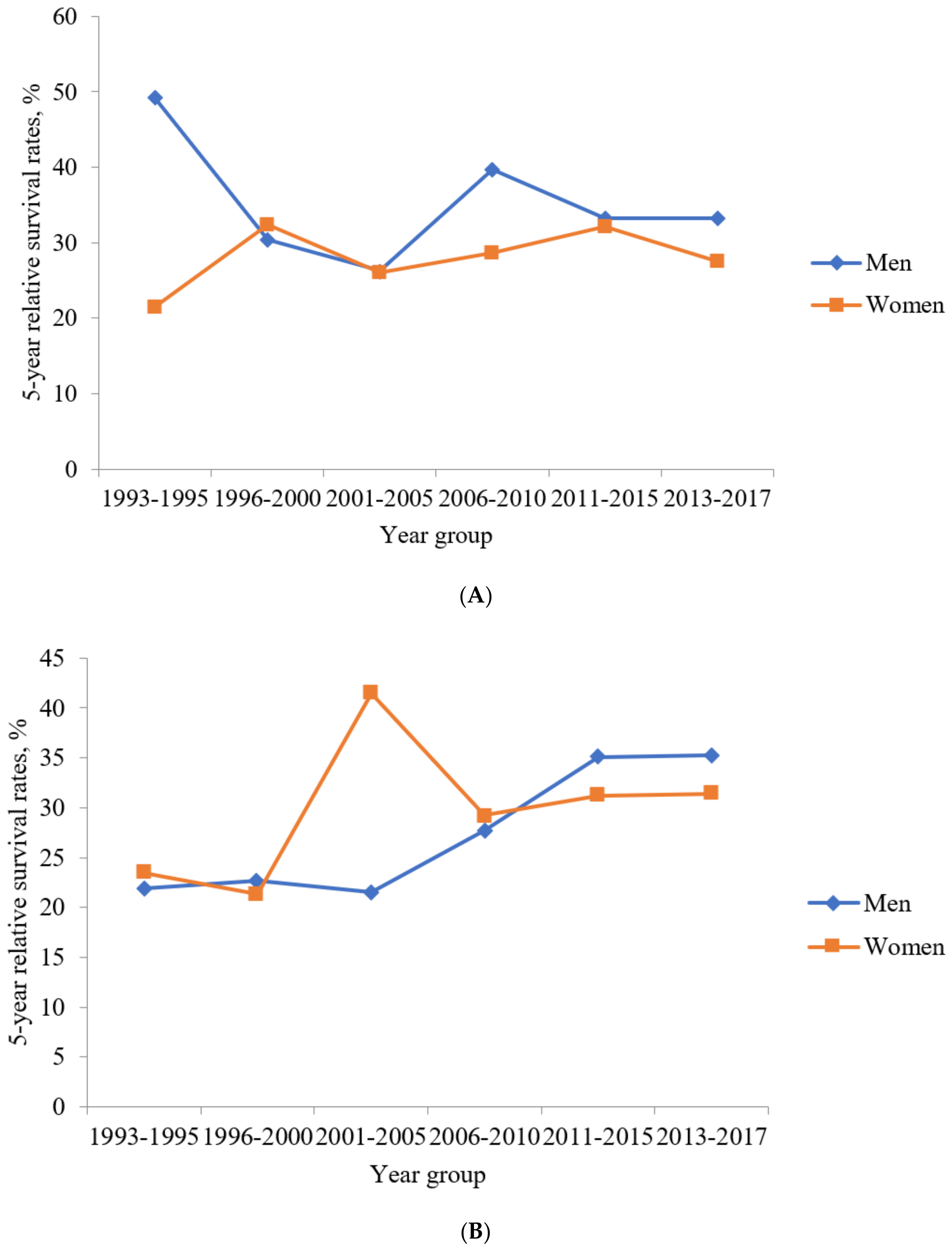
20]. However, although the survival rate is poor, the survival rate is increasing compared to the past (
Figure 6). This is the same phenomenon as the increase in colorectal cancer survival rate in South Korea.
Because SRCC of colorectal cancer is so rare, therapeutic guidelines remain undetermined due to a lack of large randomized controlled trials. To date, surgery is considered as the most important option of treatment [
21]. One population-based study showed that adjuvant chemotherapy was beneficial in stage III SRCC patients [
4]. In metastatic colorectal SRCC, one study reported a better survival of chemotherapy in patients [
30], but other studies reported poor response of chemotherapy in colorectal SRCC [
31,
32]. In SRCC of rectal cancer, neoadjuvant chemoradiotherapy could give rise to good therapeutic response [
33]. Further prospective randomized controlled trials are necessary to make the optimal therapeutic strategies.
There is a disparity in the incidence and survival rates of colorectal SRCCs between men and women. In our study, men had higher age-standardized incidence rates of both colon and rectal SRCCs compared to those in women. In addition, colon SRCC showed a trend of higher 5- and 10-year RSRs in men than in women, contrary to the findings of other studies reporting a lower hazard ratio of death in women than in men [
8,
19]. Further, some studies showed no significant difference in the hazard ratios of death between women and men [
20,
21]. There are research papers that report that hormone or genetic differences cause these results [
24]. However, different countries report different results. Although several studies revealed gender differences, the results did not show a common trend. One study of Surveillance, Epidemiology, and End Results (SEER) database from 2004 until 2015 showed that among qualified postoperative patients, there were more men than women [
34]. One study showed that, in SEER database between 2004 and 2015, numbers of male were 1677 (51.16%) and those of female was 1601 (48.84%) [
21]. In SEER 1975–2016, numbers of male were 2276 (49.6%), and those of female were 2310 (50.4%) [
35].
Our nationwide study included a large number of patients with colorectal SRCC (n = 10,780). This made it possible to comprehensively investigate the trends in the incidence and long-term survival outcomes of patients with colorectal SRCCs in South Korea. In addition, we analyzed all C18 (colon) and C19-20 (rectum) cases. Despite these strengths, our study has some limitations. First, data on clinical information, comorbidities, family history, and molecular genetic profiles were not available. Second, data on treatment modalities, including chemotherapy or radiotherapy, were not available. Lastly, data on several factors affecting survival that may have provided further insights, such as the distant metastasis site, progression-free survival, and recurrence-free survival, were not available.
In conclusion, although the incidence of colorectal SRCC is extremely low in South Korea, it has been increasing in recent decades. The prognosis is extremely poor overall, and especially so in advanced stages of colorectal SRCC. Hence, clinicians should be aware of the differential diagnosis of SRCCs in colorectal cancer cases. As the KNCIDB does not include clinical information, further population-based studies are needed to thoroughly investigate the survival rates of colorectal SRCCs in Asian populations.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}