
Aortic Valve Stenosis and Cardiac Amyloidosis: A Misleading Association

 ,
,
Abstract
:1. Introduction
2. General Features (Epidemiology, Pathophysiology)

{kind=link}
{kind=link}
{kind=link}
| First Author, Study Year | No. of Patients | Population | ATTR (+), n (%) | AL (+), n (%) | Confirmation of Diagnosis | Management of AS | Follow up Duration | Total No. of Deaths (%) | AS-CA Mortality, n (%) |
|---|---|---|---|---|---|---|---|---|---|
| Treibel, 2016 [17] | 146 | Severe AS undergoing SAVR | 6 (4) | 0 | EMB, scintigraphy (DPD) | SAVR (146) | 2.3 yrs (0.02–4.7) | 11 (7.5) | 3 (50) |
| Galat, 2016 [18] | 16 | Concomitant ATTR and moderate or severe AS | 16 (100) | 0 | EMB, scintigraphy (HMDP/DPD) | SAVR (10), TAVR (2), medical management (4) | 33 mos | 7 (44) | |
| Sperry, 2016 [19] | 171 | Group 1: ATTR (144) Group 2: ATTR + AS (27) | 171 (100) | 0 | EMB, scintigraphy (PYP) | SAVR (11) | 6 yrs | 58 (34) | 10 (37) |
| Longhi, 2016 [20] | 43 | Degenerative AS + 1 or more echocardiographic red flags for CA | 5 (12) | 0 | EMB, scintigraphy (DPD) | balloon aortic valvuloplasty | NA | NA | NA |
| Cavalcante, 2017 [21] | 113 | Severe and moderate AS scheduled for CMR | 9 (8) | 0 | CMR-LGE | SAVR (42), TAVR (17) | 18 mos (11–30) | 40 (35) | 5 (56) |
| Castano, 2017 [22] | 151 | Severe AS undergoing TAVR | 24 (16) | 0 | scintigraphy (PYP) | TAVR | 2 yrs | NA | NA |
| Scully, 2018 [23] | 101 | Severe AS undergoing TAVR | 14 (14) | 0 | scintigraphy (DPD) | TAVR | NA | NA | NA |
| Java, 2018 [24] | 16 | Amyloidosis patients undergoing AVR | 5 (31) | 6 (38) | EMB or extracardiac biopsy, scintigraphy (PYP) | TAVR (5) SAVR (11) | 1.9 yrs (1.2–4.8) | 4 (25) | |
| Peskò, 2019 [25] | 55 | Retrospective analysis of consecutive amyloidosis patients | 9 (20) | 44 (80) | CMR-LGE, scintigraphy (PYP) | NA | NA | 9 mos mortality:23 (42) | NA |
| Nitsche, 2020 [26] | 191 | Severe AS undergoing TAVR | 15 (8) | 1 (0.5) | CMR, scintigraphy (DPD), EMB | TAVR | 15.3 ± 7.9 mos | 33 (17) | 3 (19) |
| Scully, 2020 [27] | 200 | Severe symptomatic AS referred for TAVR | 26 (13) | 0 | scintigraphy (DPD) | TAVR (149), SAVR (2), medical management (49) | 19 (10–27) mos | 42 (21) | 6 (23) |
| Nitsche, 2021 [6] | 407 | Severe AS undergoing TAVR | 47 (11) | 1 (0.2) | scintigraphy (DPD), EMB or extracardiac biopsy | TAVR (333), SAVR (10), medical management (65) | 1.7 yrs | 97 (24) | 1 year mortality: 15 (31) |
| Rosenblum, 2021 [28] | 204 | Severe AS undergoing TAVR | 27 (13) | 0 | scintigraphy (PYP) | TAVR | 2.04 yrs | 63 (31) | 9 (33) |
| Faggiano, 2021 (unpublished data) | 50 | Patients with clinically relevant aortic stenosis | 9 (18) | 0 | scintigraphy (DPD) | TAVR, SAVR, medical therapy | NA | NA | NA |
| First Author, Study Year | Age, Years | Male (%) | NYHA I/II/III/IV, (%) | AF (%) | Carpal Tunnel Syndrome, n (%) | Nt-proBNP (ng/dL) |
|---|---|---|---|---|---|---|
| Treibel, 2016 [17] | 77 | 67 | NA | NA | 1 (17) | 259 |
| Galat, 2016 [18] | 79 ± 6 | 81 | III–IV (60) | 56 | 5 (31) | 438 (243–473) |
| Sperry, 2016 [19] | 79.4 ± 6.6 | 71 | III–IV (66.6) | 58.3 | NA | NA |
| Longhi, 2016 [20] | 84 (79–90) | 80 | III–IV (100) | NA | 3 (60) | NA |
| Cavalcante, 2017 [21] | 88 ± 6 | 89 | III–IV (78) | 67 | NA | NA |
| Castano, 2017 [22] | 86.3 ± 5.7 | 92 | 0/25/75/0 | 41.7 | 4 (16) | 3220 (1092 ± 19,007) |
| Scully, 2018 [23] | 88 ± 6 | 50 | NA | NA | NA | NA |
| Java, 2018 [24] | 76 (71–82) | 69 | 6/50/31/13 | 13 | NA | NA |
| Peskò, 2019 [25] | 69 (68–82) | 60 | III–IV (100) | 20 | NA | NA |
| Nitsche, 2020 [26] | 84 (81–89) | 63 | III–IV (62.5) | 56.3 | NA | 3634 (1241–6323) |
| Scully, 2020 [27] | 88 ± 5 | 62 | NA | 42 | NA | 370 (129–563) |
| Nitsche, 2021 [6] | 87 (84–92) | 65 | NA | 50 | 6 (19) | 486 (141–750) |
| Rosenblum, 2021 [28] | 86 ± 5 | 96 | III–IV (100) | 37 | 6 (22) | NA |
| Faggiano, 2021 (unpublished data) | 85.6 ± 4.3 | 84 | II (44)–III/IV (55) | 77 | 1 (11) | NA |
| First Author, Study Year | LVEF (%) | IVST, mm | LF-LG AS, % | AVA, cm2 | AVAi, cm2/m2 | Mean AV Gradient (mmHg) | LV SV Index mL/m2 | GLS (%) | CMR LGE (+), n (%) |
|---|---|---|---|---|---|---|---|---|---|
| Treibel, 2016 [17] | 67 | 16.7 | NA | NA | 0.4 | NA | NA | −12.6 | 2 (30%) |
| Galat, 2016 [18] | 50 ± 13 | 18 ± 4 | 86 | 0.8 ± 0.25 | NA | 33 ± 23 | 27 ± 7 | −7 ± 0.7 | 12 (100%) |
| Sperry, 2016 [19] | 50 ± 13.9 | 18.6 ± 4.4 | 40.7 | 0.89 ± 0.29 | 0.45 | 21.8 ± 13 | NA | NA | NA |
| Longhi, 2016 [20] | ↓ in 40% | 18 (16–21) | 80 | NA | < 0.6 | NA | NA | NA | NA |
| Cavalcante, 2017 [21] | 43 ± 17 | 18 ± 5 | 78 | NA | 0.4 ± 0.2 | 30 ± 14 | 33 ± 10 | NA | 9 (100%) |
| Castano, 2017 [22] | 47.6 ± 17.6 | 13 ± 0.3 | 37.5 | NA | 0.8 ± 0.16 | 35.2 ± 13.9 | 29.9 ± 10.5 | −12.4 + 5.2 | NA |
| Scully, 2018 [23] | NA | NA | NA | NA | NA | 37 ± 12 | 32 ± 7 | NA | NA |
| Java, 2018 [24] | 60 (59–65) | 13 (11–14) | NA | NA | 0.51 | 46 (36–51) | NA | NA | NA |
| Peskò, 2019 [25] | 59 (51–60) | 17 (13–20) | 60 | NA | NA | NA | 30 | NA | 3 (60) |
| Nitsche, 2020 [26] | 62 (44–70) | 15.5 (13.3–19.8) | 56.3 | 0.6 | NA | 35 (26–48.5) | 27.4 (22.3–33.7) | −13.8 (16.6–10.2) | 4 (25%) |
| Scully, 2020 [27] | 54 ± 14 | 14 ± 3 | 31 | 0.74 ± 0.23 | NA | 37 ± 14 | 34 ± 10 | −15 ± 6 | NA |
| Nitsche, 2021 [6] | 51 (42–64) | 16 (14–19) | 56 | 0.7 | NA | 36 (25–48) | 35.8 (27.4–44) | −13.7 (17.3–10.2) | NA |
| Rosenblum, 2021 [28] | 48 ± 17 | 14 ± 4 | 37 | 0.8 ± 0.15 | NA | 35 ± 13 | 31 ± 11 | NA | NA |
| Faggiano, 2021 (unpublished data) | 42.4 ± 9.9 | 18.3 ± 4.1 | NA | 0.64 ± 0.12 | NA | 33.4 ± 22.5 | NA | NA | NA |
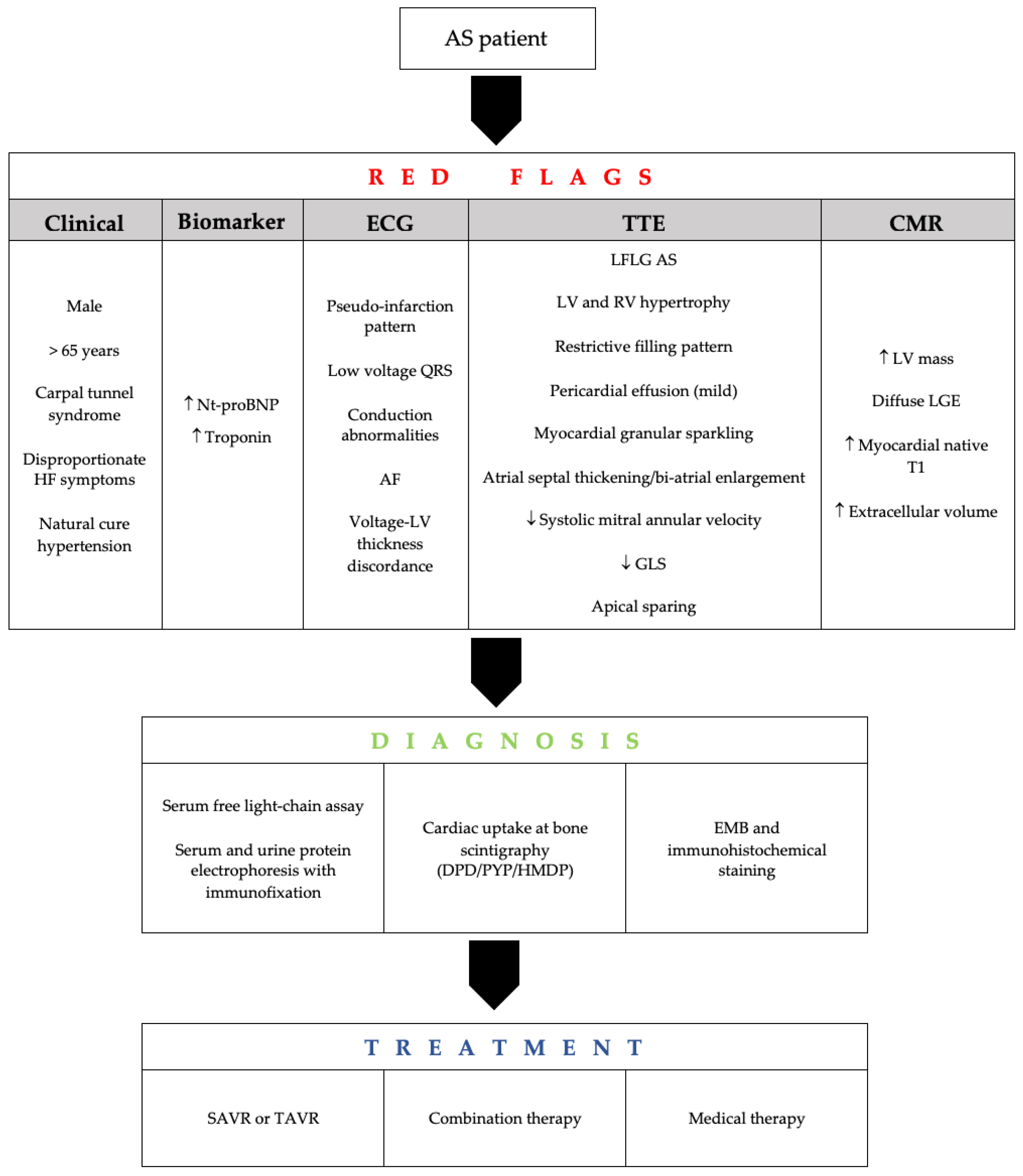
3. Clinical and Imaging Assessment
4. Screening and Predictors
5. Prognosis and Management
6. Conclusions
Funding
Conflicts of Interest
References
- Coffey, S.; Cox, B.; Williams, M.J.A. The prevalence, incidence, progression, and risks of aortic valve sclerosis: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2014, 63, 2852–2861. [Google Scholar] [CrossRef] [Green Version]
- Cornwell, G.G.; Murdoch, W.L.; Kyle, R.A.; Westermark, P.; Pitkänen, P. Frequency and distribution of senile cardiovascular amyloid. A clinicopathologic correlation. Am. J. Med. 1983, 75, 618–623. [Google Scholar] [CrossRef]
- Merlini, G.; Bellotti, V. Molecular mechanisms of amyloidosis. N. Engl. J. Med. 2003, 349, 583–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gertz, M.A.; Dispenzieri, A.; Sher, T. Pathophysiology and treatment of cardiac amyloidosis. Nat. Rev. Cardiol. 2015, 12, 91–102. [Google Scholar] [CrossRef]
- Balciunaite, G.; Rimkus, A.; Zurauskas, E.; Zaremba, T.; Palionis, D.; Valeviciene, N.; Aidietis, A.; Serpytis, P.; Rucinskas, K.; Sogaard, P.; et al. Transthyretin cardiac amyloidosis in aortic stenosis: Prevalence, diagnostic challenges, and clinical implications. Hell J. Cardiol. HJC Hell Kardiol. Ep. 2020, 61, 92–98. [Google Scholar] [CrossRef]
- Nitsche, C.; Scully, P.R.; Patel, K.P.; Kammerlander, A.A.; Koschutnik, M.; Dona, C.; Wollenweber, T.; Ahmed, N.; Thornton, G.D.; Kelion, A.D.; et al. Prevalence and Outcomes of Concomitant Aortic Stenosis and Cardiac Amyloidosis. J. Am. Coll. Cardiol. 2021, 77, 128–139. [Google Scholar] [CrossRef]
- Kittleson, M.M.; Maurer, M.S.; Ambardekar, A.V.; Bullock-Palmer, R.P.; Chang, P.P.; Eisen, H.J.; Nair, A.P.; Nativi-Nicolau, J.; Ruberg, F.L. American Heart Association Heart Failure and Transplantation Committee of the Council on Clinical Cardiology. Cardiac Amyloidosis: Evolving Diagnosis and Management: A Scientific Statement From the American Heart Association. Circulation 2020, 142, e7–e22. [Google Scholar] [CrossRef]
- Ternacle, J.; Krapf, L.; Mohty, D.; Magne, J.; Nguyen, A.; Galat, A.; Gallet, R.; Teiger, E.; Côté, N.; Clavel, M.A.; et al. Aortic Stenosis and Cardiac Amyloidosis: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 2638–2651. [Google Scholar] [CrossRef]
- Gargiulo, P.; Perrone-Filardi, P. Dangerous relationships: Aortic stenosis and transthyretin cardiac amyloidosis. Eur. Heart, J. 2017, 38, 2888–2889. [Google Scholar] [CrossRef]
- Damy, T.; Judge, D.P.; Kristen, A.V.; Berthet, K.; Li, H.; Aarts, J. Cardiac findings and events observed in an open-label clinical trial of tafamidis in patients with non-Val30Met and non-Val122Ile hereditary transthyretin amyloidosis. J. Cardiovasc. Transl. Res. 2015, 8, 117–127. [Google Scholar] [CrossRef] [Green Version]
- Falk, R.H.; Alexander, K.M.; Liao, R.; Dorbala, S. AL (Light-Chain) Cardiac Amyloidosis: A Review of Diagnosis and Therapy. J. Am. Coll. Cardiol. 2016, 68, 1323–1341. [Google Scholar] [CrossRef] [PubMed]
- Dweck, M.R.; Boon, N.A.; Newby, D.E. Calcific aortic stenosis: A disease of the valve and the myocardium. J. Am. Coll. Cardiol. 2012, 60, 1854–1863. [Google Scholar] [CrossRef] [Green Version]
- Joseph, J.; Naqvi, S.Y.; Giri, J.; Goldberg, S. Aortic Stenosis: Pathophysiology, Diagnosis, and Therapy. Am. J. Med. 2017, 130, 253–263. [Google Scholar] [CrossRef]
- Zhao, L.; Buxbaum, J.N.; Reixach, N. Age-related oxidative modifications of transthyretin modulate its amyloidogenicity. Biochemistry 2013, 52, 1913–1926. [Google Scholar] [CrossRef] [Green Version]
- Henderson, B.C.; Tyagi, N.; Ovechkin, A.; Kartha, G.K.; Moshal, K.S.; Tyagi, S.C. Oxidative remodeling in pressure overload induced chronic heart failure. Eur. J. Heart Fail. 2007, 9, 450–457. [Google Scholar] [CrossRef]
- Kristen, A.V.; Schnabel, P.A.; Winter, B.; Helmke, B.M.; Longerich, T.; Hardt, S.; Koch, A.; Sack, F.U.; Katus, H.A.; Linke, R.P.; et al. High prevalence of amyloid in 150 surgically removed heart valves--a comparison of histological and clinical data reveals a correlation to atheroinflammatory conditions. Cardiovasc. Pathol. Off. J. Soc. Cardiovasc. Pathol. 2010, 19, 228–235. [Google Scholar] [CrossRef]
- Treibel, T.A.; Fontana, M.; Gilbertson, J.A.; Castelletti, S.; White, S.K.; Scully, P.R.; Roberts, N.; Hutt, D.F.; Rowczenio, D.M.; Whelan, C.J.; et al. Occult Transthyretin Cardiac Amyloid in Severe Calcific Aortic Stenosis: Prevalence and Prognosis in Patients Undergoing Surgical Aortic Valve Replacement. Circ. Cardiovasc. Imaging 2016, 9, e005066. [Google Scholar] [CrossRef] [Green Version]
- Galat, A.; Guellich, A.; Bodez, D.; Slama, M.; Dijos, M.; Zeitoun, D.M.; Milleron, O.; Attias, D.; Dubois-Randé, J.L.; Mohty, D.; et al. Aortic stenosis and transthyretin cardiac amyloidosis: The chicken or the egg? Eur. Heart J. 2016, 37, 3525–3531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperry, B.W.; Jones, B.M.; Vranian, M.N.; Hanna, M.; Jaber, W.A. Recognizing Transthyretin Cardiac Amyloidosis in Patients with Aortic Stenosis: Impact on Prognosis. JACC Cardiovasc. Imaging 2016, 9, 904–906. [Google Scholar] [CrossRef] [PubMed]
- Longhi, S.; Lorenzini, M.; Gagliardi, C.; Milandri, A.; Marzocchi, A.; Marrozzini, C.; Saia, F.; Ortolani, P.; Biagini, E.; Guidalotti, P.L.; et al. Coexistence of Degenerative Aortic Stenosis and Wild-Type Transthyretin-Related Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2016, 9, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Cavalcante, J.L.; Rijal, S.; Abdelkarim, I.; Althouse, A.D.; Sharbaugh, M.S.; Fridman, Y.; Soman, P.; Forman, D.E.; Schindler, J.T.; Gleason, T.G.; et al. Cardiac amyloidosis is prevalent in older patients with aortic stenosis and carries worse prognosis. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 2017, 19, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castaño, A.; Narotsky, D.L.; Hamid, N.; Khalique, O.K.; Morgenstern, R.; DeLuca, A.; Rubin, J.; Chiuzan, C.; Nazif, T.; Vahl, T.; et al. Unveiling transthyretin cardiac amyloidosis and its predictors among elderly patients with severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur. Heart J. 2017, 38, 2879–2887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scully, P.R.; Moon, J.C.; Treibel, T.A. Cardiac amyloidosis in aortic stenosis: The tip of the iceberg. J. Thorac. Cardiovasc. Surg. 2018, 156, 965–966. [Google Scholar] [CrossRef] [Green Version]
- Java, A.P.; Greason, K.L.; Dispenzieri, A.; Grogan, M.; King, K.S.; Maleszewski, J.J.; Daly, R.C.; Eleid, M.F.; Pochettino, A.; Schaff, H.V. Aortic valve replacement in patients with amyloidosis. J. Thorac. Cardiovasc. Surg. 2018, 156, 98–103. [Google Scholar] [CrossRef]
- Peskó, G.; Jenei, Z.; Varga, G.; Apor, A.; Vágó, H.; Czibor, S.; Prohászka, Z.; Masszi, T.; Pozsonyi, Z. Coexistence of aortic valve stenosis and cardiac amyloidosis: Echocardiographic and clinical significance. Cardiovasc. Ultrasound 2019, 17, 32. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, C.; Aschauer, S.; Kammerlander, A.A.; Schneider, M.; Poschner, T.; Duca, F.; Binder, C.; Koschutnik, M.; Stiftinger, J.; Goliasch, G.; et al. Light-chain and transthyretin cardiac amyloidosis in severe aortic stenosis: Prevalence, screening possibilities, and outcome. Eur. J. Heart Fail. 2020, 22, 1852–1862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scully, P.R.; Patel, K.P.; A Treibel, T.; Thornton, G.D.; Hughes, R.K.; Chadalavada, S.; Katsoulis, M.; Hartman, N.; Fontana, M.; Pugliese, F.; et al. Prevalence and outcome of dual aortic stenosis and cardiac amyloid pathology in patients referred for transcatheter aortic valve implantation. Eur. Heart J. 2020, 41, 2759–2767. [Google Scholar] [CrossRef] [Green Version]
- Rosenblum, H.; Masri, A.; Narotsky, D.L.; Goldsmith, J.; Hamid, N.; Hahn, R.T.; Kodali, S.; Vahl, T.; Nazif, T.; Khalique, O.K.; et al. Unveiling outcomes in coexisting severe aortic stenosis and transthyretin cardiac amyloidosis. Eur. J. Heart Fail. 2021, 23, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Sperry, B.W.; Reyes, B.A.; Ikram, A.; Donnelly, J.; Phelan, D.; Jaber, W.A.; Shapiro, D.; Evans, P.J.; Maschke, S.; Kilpatrick, S.E.; et al. Tenosynovial and Cardiac Amyloidosis in Patients Undergoing Carpal Tunnel Release. J. Am. Coll. Cardiol. 2018, 72, 2040–2050. [Google Scholar] [CrossRef]
- Fosbøl, E.; Rørth, R.; Leicht, B.P.; Schou, M.; Maurer, M.S.; Kristensen, S.L.; Kober, L.; Gustafsson, F. Association of Carpal Tunnel Syndrome with Amyloidosis, Heart Failure, and Adverse Cardiovascular Outcomes. J. Am. Coll. Cardiol. 2019, 74, 15–23. [Google Scholar] [CrossRef]
- Yanagisawa, A.; Ueda, M.; Sueyoshi, T.; Okada, T.; Fujimoto, T.; Ogi, Y.; Kitagawa, K.; Tasaki, M.; Misumi, Y.; Oshima, T.; et al. Amyloid deposits derived from transthyretin in the ligamentum flavum as related to lumbar spinal canal stenosis. Mod. Pathol. 2015, 28, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bequignon, E.; Guellich, A.; Bartier, S.; Raynal, M.; Prulière-Escabasse, V.; Canoui-Poitrine, F.; Coste, A.; Damy, T. How your ears can tell what is hidden in your heart: Wild-type transthyretin amyloidosis as potential cause of sensorineural hearing loss inelderly-AmyloDEAFNESS pilot study. Amyloid. Int. J. Exp. Clin. Investig. Off. J. Int. Soc. Amyloidosis 2017, 24, 96–100. [Google Scholar] [CrossRef]
- Ruberg, F.L.; Grogan, M.; Hanna, M.; Kelly, J.W.; Maurer, M.S. Transthyretin Amyloid Cardiomyopathy: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 2872–2891. [Google Scholar] [CrossRef]
- Arvanitis, M.; Simon, S.; Chan, G.; Fine, D.; Beardsley, P.; LaValley, M.; Jacobson, D.; Koch, C.; Berk, J.L.; Connors, L.; et al. Retinol binding protein 4 (RBP4) concentration identifies V122I transthyretin cardiac amyloidosis. Amyloid. Int. J. Exp. Clin. Investig. Off. J. Int. Soc. Amyloidosis 2017, 24 (Suppl. 1), 120–121. [Google Scholar] [CrossRef] [PubMed]
- González-López, E.; Gagliardi, C.; Dominguez, F.; Quarta, C.C.; Moral, F.J.D.H.-D.; Milandri, A.; Salas, C.; Cinelli, M.; Cobo-Marcos, M.; Lorenzini, M.; et al. Clinical characteristics of wild-type transthyretin cardiac amyloidosis: Disproving myths. Eur. Heart J. 2017, 38, 1895–1904. [Google Scholar] [CrossRef] [PubMed]
- Rapezzi, C.; Merlini, G.; Quarta, C.C.; Riva, L.; Longhi, S.; Leone, O.; Salvi, F.; Ciliberti, P.; Pastorelli, F.; Biagini, E.; et al. Systemic cardiac amyloidoses: Disease profiles and clinical courses of the 3 main types. Circulation 2009, 120, 1203–1212. [Google Scholar] [CrossRef] [Green Version]
- Maurer, M.S.; Elliott, P.; Comenzo, R.; Semigran, M.; Rapezzi, C. Addressing Common Questions Encountered in the Diagnosis and Management of Cardiac Amyloidosis. Circulation 2017, 135, 1357–1377. [Google Scholar] [CrossRef] [Green Version]
- Rapezzi, C.; Lorenzini, M.; Longhi, S.; Milandri, A.; Gagliardi, C.; Bartolomei, I.; Salvi, F.; Maurer, M.S. Cardiac amyloidosis: The great pretender. Heart Fail. Rev. 2015, 20, 117–124. [Google Scholar] [CrossRef]
- Damy, T.; Maurer, M.S.; Rapezzi, C.; Planté-Bordeneuve, V.; Karayal, O.N.; Mundayat, R.; Suhr, O.B.; Kristen, A.V. Clinical, ECG and echocardiographic clues to the diagnosis of TTR-related cardiomyopathy. Open Heart 2016, 3, e000289. [Google Scholar] [CrossRef] [Green Version]
- Dungu, J.N.; Anderson, L.J.; Whelan, C.J.; Hawkins, P.N. Cardiac transthyretin amyloidosis. Heart Br. Card. Soc. 2012, 98, 1546–1554. [Google Scholar] [CrossRef]
- Martinez-Naharro, A.; Treibel, T.; Abdel-Gadir, A.; Bulluck, H.; Zumbo, G.; Knight, D.S.; Kotecha, T.; Francis, R.; Hutt, D.F.; Rezk, T.; et al. Magnetic Resonance in Transthyretin Cardiac Amyloidosis. J. Am. Coll. Cardiol. 2017, 70, 466–477. [Google Scholar] [CrossRef]
- Boldrini, M.; Cappelli, F.; Chacko, L.; Restrepo-Cordoba, M.A.; Sainz, A.L.; Giannoni, A.; Aimo, A.; Baggiano, A.; Martinez-Naharro, A.; Whelan, C.; et al. Multiparametric Echocardiography Scores for the Diagnosis of Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2020, 13, 909–920. [Google Scholar] [CrossRef]
- Yingchoncharoen, T.; Agarwal, S.; Popović, Z.B.; Marwick, T.H. Normal ranges of left ventricular strain: A meta-analysis. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2013, 26, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Porciani, M.C.; Lilli, A.; Perfetto, F.; Cappelli, F.; Rao, C.M.; Del Pace, S.; Ciaccheri, M.; Castelli, G.; Tarquini, R.; Romagnani, L.; et al. Tissue Doppler and strain imaging: A new tool for early detection of cardiac amyloidosis. Amyloid. Int. J. Exp. Clin. Investig. Off. J. Int. Soc. Amyloidosis 2009, 16, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Koyama, J.; Ray-Sequin, P.A.; Falk, R.H. Longitudinal myocardial function assessed by tissue velocity, strain, and strain rate tissue Doppler echocardiography in patients with AL (primary) cardiac amyloidosis. Circulation 2003, 107, 2446–2452. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M.; Banypersad, S.M.; Treibel, T.; Maestrini, V.; Sado, D.M.; White, S.K.; Pica, S.; Castelletti, S.; Piechnik, S.K.; Robson, M.D.; et al. Native T1 mapping in transthyretin amyloidosis. JACC Cardiovasc. Imaging 2014, 7, 157–165. [Google Scholar] [CrossRef] [Green Version]
- Austin, B.A.; Tang, W.W.; Rodriguez, E.R.; Tan, C.; Flamm, S.D.; Taylor, D.O.; Starling, R.C.; Desai, M.Y. Delayed hyper-enhancement magnetic resonance imaging provides incremental diagnostic and prognostic utility in suspected cardiac amyloidosis. JACC Cardiovasc. Imaging 2009, 2, 1369–1377. [Google Scholar] [CrossRef] [Green Version]
- Syed, I.S.; Glockner, J.F.; Feng, D.; Araoz, P.A.; Martinez, M.W.; Edwards, W.D.; Gertz, M.A.; Dispenzieri, A.; Oh, J.K.; Bellavia, D.; et al. Role of cardiac magnetic resonance imaging in the detection of cardiac amyloidosis. JACC Cardiovasc. Imaging 2010, 3, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Naharro, A.; Kotecha, T.; Norrington, K.; Boldrini, M.; Rezk, T.; Quarta, C.C.; Treibel, T.; Whelan, C.J.; Knight, D.S.; Kellman, P.; et al. Native T1 and Extracellular Volume in Transthyretin Amyloidosis. JACC Cardiovasc. Imaging 2019, 12, 810–819. [Google Scholar] [CrossRef] [PubMed]
- Knight, D.S.; Zumbo, G.; Barcella, W.; Steeden, J.A.; Muthurangu, V.; Martinez-Naharro, A.; Treibel, T.; Abdel-Gadir, A.; Bulluck, H.; Kotecha, T.; et al. Cardiac Structural and Functional Consequences of Amyloid Deposition by Cardiac Magnetic Resonance and Echocardiography and Their Prognostic Roles. JACC Cardiovasc. Imaging. 2019, 12, 823–833. [Google Scholar] [CrossRef]
- Maurer, M.S.; Bokhari, S.; Damy, T.; Dorbala, S.; Drachman, B.M.; Fontana, M.; Grogan, M.; Kristen, A.V.; Lousada, I.; Nativi-Nicolau, J.; et al. Expert Consensus Recommendations for the Suspicion and Diagnosis of Transthyretin Cardiac Amyloidosis. Circ. Heart Fail. 2019, 12, e006075. [Google Scholar] [CrossRef] [PubMed]
- Gillmore, J.D.; Maurer, M.S.; Falk, R.H.; Merlini, G.; Damy, T.; Dispenzieri, A.; Wechalekar, A.D.; Berk, J.L.; Quarta, C.C.; Grogan, M.; et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation 2016, 133, 2404–2412. [Google Scholar] [CrossRef]
- Perugini, E.; Guidalotti, P.L.; Salvi, F.; Cooke, R.M.; Pettinato, C.; Riva, L.; Leone, O.; Farsad, M.; Ciliberti, P.; Reggiani, M.L.B.; et al. Noninvasive etiologic diagnosis of cardiac amyloidosis using 99mTc-3,3-diphosphono-1,2-propanodicarboxylic acid scintigraphy. J. Am. Coll. Cardiol. 2005, 46, 1076–1084. [Google Scholar] [CrossRef] [Green Version]
- Hutt, D.F.; Quigley, A.-M.; Page, J.; Hall, M.L.; Burniston, M.; Gopaul, D.; Lane, T.; Whelan, C.J.; Lachmann, H.; Gillmore, J.D.; et al. Utility and limitations of 3,3-diphosphono-1,2-propanodicarboxylic acid scintigraphy in systemic amyloidosis. Eur. Heart J. Cardiovasc. Imaging. 2014, 15, 1289–1298. [Google Scholar] [CrossRef]
- Dorbala, S.; Cuddy, S.; Falk, R.H. How to Image Cardiac Amyloidosis: A Practical Approach. JACC Cardiovasc. Imaging 2020, 13, 1368–1383. [Google Scholar] [CrossRef]
- Carroll, J.D.; Gaasch, W.H.; McAdam, K.P. Amyloid cardiomyopathy: Characterization by a distinctive voltage/mass relation. Am. J. Cardiol. 1982, 49, 9–13. [Google Scholar] [CrossRef]
- Salinger, T.; Hu, K.; Liu, D.; Herrmann, S.; Lorenz, K.; Ertl, G.; Nordbeck, P. Cardiac amyloidosis mimicking severe aortic valve stenosis—A case report demonstrating diagnostic pitfalls and role of dobutamine stress echocardiography. BMC Cardiovasc. Disord. 2017, 17, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salinger, T.; Hu, K.; Liu, D.; Herrmann, S.; Lorenz, K.; Ertl, G.; Nordbeck, P. Impact of aortic valve calcification, as measured by MDCT, on survival in patients with aortic stenosis: Results of an international registry study. J. Am. Coll. Cardiol. 2014, 64, 1202–1213. [Google Scholar] [CrossRef] [Green Version]
- Monticelli, F.C.; Kunz, S.N.; Keller, T.; Bleiziffer, S. Cardiac amyloidosis as a potential risk factor for transapical transcatheter aortic valve implantation. J. Card. Surg. 2014, 29, 623–624. [Google Scholar] [CrossRef]
- Fitzmaurice, G.J.; Wishart, V.; Graham, A.N.J. An unexpected mortality following cardiac surgery: A post-mortem diagnosis of cardiac amyloidosis. Gen. Thorac. Cardiovasc. Surg. 2013, 61, 417–421. [Google Scholar] [CrossRef]
- Kotani, N.; Hashimoto, H.; Muraoka, M.; Kabara, S.; Okawa, H.; Matsuki, A. Fatal perioperative myocardial infarction in four patients with cardiac amyloidosis. Anesthesiology 2000, 92, 873–875. [Google Scholar] [CrossRef] [PubMed]
- Moreno, R.; Dobarro, D.; De Sa, E.L.; Prieto, M.; Morales, C.; Orbe, L.C.; Moreno-Gomez, I.; Filgueiras, D.; Sanchez-Recalde, A.; Galeote, G.; et al. Cause of complete atrioventricular block after percutaneous aortic valve implantation: Insights from a necropsy study. Circulation 2009, 120, e29–e30. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 27, ehab368. [Google Scholar] [CrossRef] [PubMed]



| Fibril Protein | Precursor Protein | Target Organs |
|---|---|---|
| ATTR | Transthyretin (wild-type or variant) | Wild type: heart, carpal tunnel syndrome (bilateral), ligaments, lumbar spinal stenosis Variant (variable): heart, PNS, ANS, ligaments, lumbar spinal stenosis, leptomeningeal, eye, gastrointestinal tract |
| AL | Monoclonal immunoglobulin light chain | Heart, PNS (no CNS), ANS, liver, lung, gastrointestinal tract, soft tissues (tongue), kidney, myopathy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonelli, A.; Paris, S.; Nardi, M.; Henein, M.Y.; Agricola, E.; Troise, G.; Faggiano, P. Aortic Valve Stenosis and Cardiac Amyloidosis: A Misleading Association. J. Clin. Med. 2021, 10, 4234. https://doi.org/10.3390/jcm10184234
Bonelli A, Paris S, Nardi M, Henein MY, Agricola E, Troise G, Faggiano P. Aortic Valve Stenosis and Cardiac Amyloidosis: A Misleading Association. Journal of Clinical Medicine. 2021; 10(18):4234. https://doi.org/10.3390/jcm10184234
Chicago/Turabian StyleBonelli, Andrea, Sara Paris, Matilde Nardi, Michael Y. Henein, Eustachio Agricola, Giovanni Troise, and Pompilio Faggiano. 2021. "Aortic Valve Stenosis and Cardiac Amyloidosis: A Misleading Association" Journal of Clinical Medicine 10, no. 18: 4234. https://doi.org/10.3390/jcm10184234