1. Introduction
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) constitutes a serious health problem that truncates the life of millions of people and their families around the world [
1,
2,
3]. ME/CFS is a chronic condition characterized by profound fatigue which is exacerbated by physical/mental and emotional activity (also known as PEM; post-exertional malaise), lack of refreshing sleep and dysautonomia, and multiple additional comorbidities [
4]; its diagnosis still solely relies on clinical symptom assessment [
5,
6,
7] after ruling out potential subjacent illness that could explain patient´s symptoms.
Despite a number of studies aimed at evidencing routine clinical parameters that may be useful, at least for the suspicion of an ME/CFS case, few are the differences that have been reported [
8]. For example, Nacul et al. found significantly lower median values of serum creatine kinase (CK) in severely ill patients compared to healthy controls (HCs) and non-severe ME/CFS (median = 54, 101.5, and 84 U/L, respectively) [
9], a finding confirmed by two additional studies [
10,
11]. While CK differences may be derived from patient sedentarism itself, some potential differences, including the levels of alkaline phosphatase, free T4 levels, or eosinophil counts, detected at lower significance (
p < 0.1) in small cohorts (
n = 15/group) [
10] deserve further exploration in larger cohorts, individually or in combination with others.
Blood factors differentially altered in ME/CFS subgroups may constitute valuable tools in the clinic for achieving improved patient treatments, particularly for precision medicine purposes, while they may also serve to minimize patient heterogeneity in research studies. Unveiling the nature of ME/CFS, in fact, might well depend on homogeneous patient subset assessment, boosting the statistical robustness of data.
Therefore, in the current study we aimed at identifying clinical parameters that differentiate ME/CFS case subgroups by themselves or in relation to symptom severity, in a large cohort of female ME/CFS cases (n = 250), with potential therapeutic and/or research purposes.
4. Discussion
As earlier mentioned, the use of standard blood tests to at least support a potential case of ME/CFS (“triage” diagnosis method) and/or differentiate case subgroups for therapeutic and research purposes would provide clear advantages. In fact, it may well constitute the key toward unveiling ME/CFS subgroup etiology and evolution.
Although clustering methods based on case symptoms have been useful in identifying autonomic phenotypes in CFS [
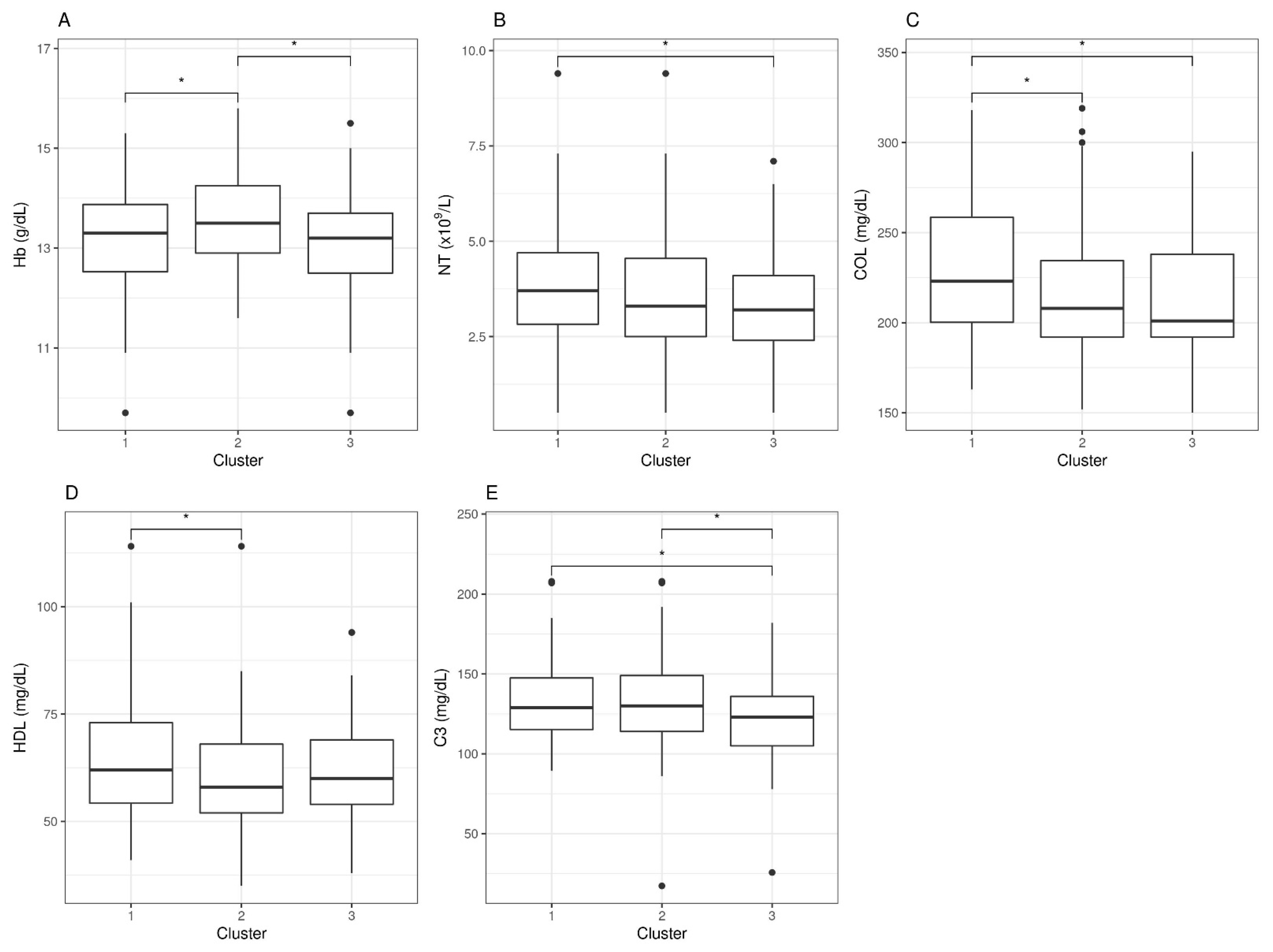
25], they failed at detecting robust blood correlations between symptoms and individual blood parameters in our cohort (
Figure 2). The approach did, however, show potential for differentiating cases with severe, moderate, or mild affection as defined by the five symptom scores used for clustering (
Table 2 and
Table 3). The physiological significance of the findings, including the increased levels of C3 in severe and moderate with respect to mildly affected cases or the increased neutrophil count in severe ME/CFS by itself or in combination with LDL and cholesterol, as well as their involvement in symptom development or maintenance, remains to be elucidated.
Nevertheless, the presence of a large proportion of ME/CFS (42.8% or 107/250) cases with increased expression of C1q, for the first time, may importantly set the basis for future ME/CFS subtyping.
C1q acts as the first component in the classical complement pathway. The complement system is a central part of innate immunity with two important functions: serving as a defense system against invading pathogens and for the clearing of dead cells or debris [
26,
27]. C1q recognizes PAMPs (pathogen-associated molecular patterns), including LPS (lipopolysaccharide) and bacterial porins [
28], in addition to recognizing molecules such as phosphatidylserine and dsDNA exposed on the surface of dying cells [
29,
30].
Thus, the detected increased levels of C1q and other complement components in a subgroup of ME/CFS cases may indicate a state of active efferocytosis toward fighting a subjacent infection or while clearing damaged tissue. Moreover, cases with chronic activation of the complement pathway may, for this reason, become particularly sensitive to PEM [
4,
5,
6,
7], a possibility that may be worth exploring.
It is well documented that, both inefficient and overstimulation of the complement system can be detrimental for the host, being associated with increased susceptibility to infections, autoimmunity, chronic inflammation, and thrombotic microangiopathy, among others [
24,
26,
27,
31]. Some of these processes have been associated with ME/CFS [
32,
33]. We, however, only found a few cases of positive self-antigen immunity across the 10-test run applied to the 250 participating cases (
Supplementary Table S1).
The observation that, among the many blood parameters measured, those known to be related to C1q function, i.e., C1 inhibitors C3 and C4 showed significant differences between groups (
Table 6) further supports a functional problem of the complement system in this subgroup of cases, perhaps with consequences in the process of coagulation. A prospective follow-up of coagulopathies in this subgroup of patients, thus, appears pertinent.
More recently, Benavente et al. showed that C1q acts as a ligand that can directly bind a series of receptors previously unidentified as partners of this molecule, including the following proteins: CD44, GPR62, BAI1, c-MET, and ADCY5, which trigger activation of downstream signaling pathways [
34,
35] and, thus, affect different aspects of neuroepithelial stem-cell biology. The finding by these authors that C1q is elevated upon nerve injury [
34] and the emerging connections of C1q with neurodegenerative disease [
36,
37] open up the exciting possibility that increased levels of C1q may underlie ME/CFS cognitive problems [
4,
5,
6,
7]. C1q alters prion disease progression, regulates neuron pruning, and modulates the process of phagocytosis by microglia while responding to amyloid plaque formation [
38,
39,
40]. Unfortunately, no specific instruments for detailed cognitive assessment of the participants or neuroimaging tools were used in this study.
Lastly, the fact that the two strata presenting normal vs. increased levels of C1q showed differences in pain may indicate a direct involvement of C1q in case symptoms. It may be relevant to include a more detailed assessment of this symptom by using pain-focused questionnaires, such as the FIQ (Fibromyalgia Impact Questionnaire) and/or others [
41,
42,
43], in future studies of C1q’s role in ME/CFS. Although the failure of questionnaires other than the SF-36 to detect symptom-related differences with C1q levels (
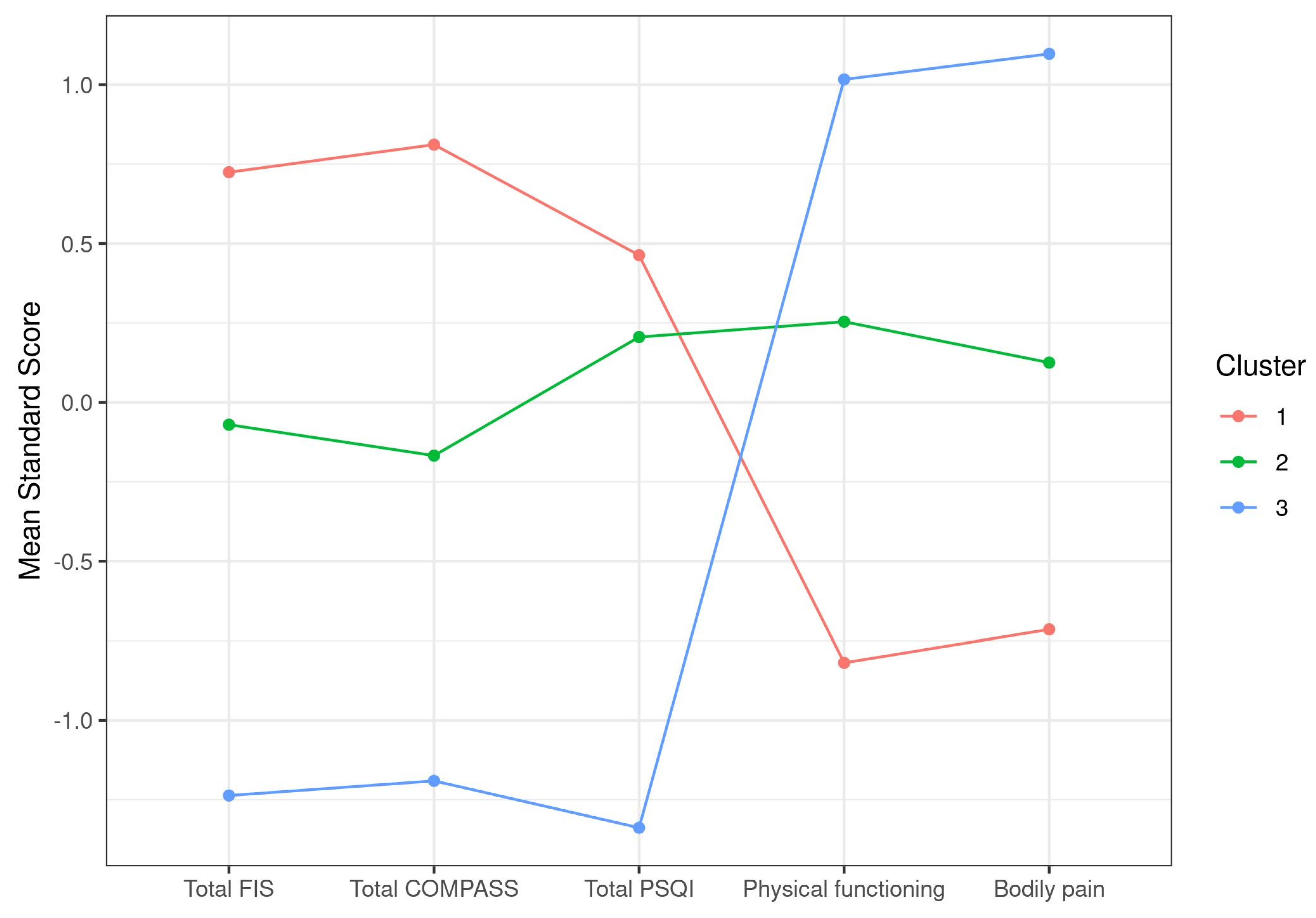
Table 5) lead to us presuming no major involvement of C1q in this aspect of the disease, it seems curious that the plotting of the two clusters showed opposite trends in all five symptoms selected by the k-means screening method to set symptom-based clusters of the cohort (
Figure 1 and
Figure 3).
Moreover, within the 94 cases in the “severe” group (cluster 1) of our symptom-based cluster analysis (
Table 2), about 39% (37/94) presented increased C1q levels while 61% (57/94) showed normal levels; within the 107 cases of the “moderate” group (cluster 2), 35% (37/107) had increased C1q and 65% (70/107) normal C1q levels; within the 49 cases of the “mild” group (cluster 3), 33% (16/49) showed increased C1q levels and 67% (33/49) had C1q levels within normal reference values. This indicates a rough 1:2 overall ratio of cases with increased C1q levels in the “mild” group, with a slight increase in this ratio in the “moderate” and an even higher ratio (1:1.5) in the “severe” cluster, suggesting an increased prevalence of high C1q levels with case disease severity, despite the lack of significant correlations between individual symptom scores and C1q levels. A correlation of C1q levels with the chronicity status of cases could not be established either.
Additional blood parameters that showed abnormal values in a large proportion of individuals in our cohort, such as vitamin D deficiency, LDL levels, cholesterol, C3 levels, or platelet mean value, may provide relevant information for treatment options, an aspect not well understood at present, which requires further monitoring in the future.
It should be mentioned that, although different reference values have been established for vitamin D deficiency, for example, the recommendations from the 2011 US Institute of Medicine (IOM) reported a minimal concentration of 52 nmol/L, while the US Endocrine Society guidelines stated a minimal concentration of 78 nmol/L [
44,
45], the applied range in this study was right below the lowest range (50 nmol/L,
Supplementary Table S1), and yet a large proportion of cases (>60%) showed vitamin D deficiency (
Table 4).
Additional Limitations
Although the cohort under study included a considerable number of subjects (n = 250), the external validity of the data remains limited to females. Random selection of participants can lead to more representative results population wise; however, subject heterogeneity translates into enhanced variability, compromising the establishment of robust differences, perhaps relevant to the diagnosis of ME/CFS. The lack of additional relevant differences across ME/CFS cases cannot be ruled out by the laborious, yet discrete analysis here performed.


 ,
, 




{kind=link}
{kind=link}
{kind=link}