
Analysis of Patient Factors Affecting In Vitro Characteristics of Subacromial Bursal Connective Tissue Progenitor Cells during Rotator Cuff Repair

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Surgical Removal of Subacromial Bursal Tissue
2.3. Subacromial Tissue Processing
2.4. Nucleated Cell Count
2.5. Colony-Forming Units
2.6. Radiographic Analysis
2.7. Statistical Analyses
3. Results
3.1. Subjects
3.2. Correlation between Number of CFUs and Patient Demographics
3.3. Correlation between NCC and Patient Demographics
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oh, L.S.; Wolf, B.R.; Hall, M.P.; Levy, B.A.; Marx, R.G. Indications for rotator cuff repair: A systematic review. Clin. Orthop. Relat. Res. 2007, 455, 52–63. [Google Scholar] [CrossRef] [Green Version]
- Day, M.A.; Westermann, R.W.; Bedard, N.A.; Glass, N.A.; Wolf, B.R. Trends Associated with Open Versus Arthroscopic Rotator Cuff Repair. HSS J. 2019, 15, 133–136. [Google Scholar] [CrossRef]
- Harryman, D.T., 2nd; Mack, L.A.; Wang, K.Y.; Jackins, S.E.; Richardson, M.L.; Matsen, F.A., 3rd. Repairs of the rotator cuff. Correlation of functional results with integrity of the cuff. J. Bone Jt. Surg. 1991, 73, 982–989. [Google Scholar] [CrossRef]
- Galatz, L.M.; Ball, C.M.; Teefey, S.A.; Middleton, W.D.; Yamaguchi, K. The Outcome and Repair Integrity of Completely Arthroscopically Repaired Large and Massive Rotator Cuff Tears. J. Bone Jt. Surg.-Ser. A 2004, 86, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Mather, R.C., III; Koenig, L.; Acevedo, D.; Dall, T.M.; Gallo, P.; Romeo, A.; Tongue, J.; Williams, G.J. The Societal and Economic Value of Rotator Cuff Repair. J. Bone Jt. Surg. Am. 2013, 95, 1993. [Google Scholar] [CrossRef] [Green Version]
- Gerber, C.; Schneeberger, A.; Perren, S.; Nyffeler, R. Experimental rotator cuff repair. A preliminary study. J. Bone Jt. Surg. Am. 1999, 81, 1281–1290. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, D.; Rodeo, S.A. Biological augmentation of rotator cuff tendon repair. Clin. Orthop. Relat. Res. 2008, 466, 622–633. [Google Scholar] [CrossRef] [Green Version]
- Thomopoulos, S.; Genin, G.M.; Galatz, L.M. The development and morphogenesis of the tendon-to-bone insertion-What development can teach us about healing. J. Musculoskelet. Neuronal Interact. 2010, 10, 35–45. [Google Scholar]
- Nourissat, G.; Berenbaum, F.; Duprez, D. Tendon injury: From biology to tendon repair. Nat. Rev. Rheumatol. 2015, 11, 223–233. [Google Scholar] [CrossRef]
- Docheva, D.; Müller, S.A.; Majewski, M.; Evans, C.H. Biologics of Tendon Repair. Adv. Drug Deliv. Rev. 2015, 84, 222–239. [Google Scholar] [CrossRef] [Green Version]
- Carr, J.B.; Rodeo, S.A. The role of biologic agents in the management of common shoulder pathologies: Current state and future directions. J. Shoulder Elb. Surg. 2019, 28, 2041–2052. [Google Scholar] [CrossRef]
- Komura, S.; Satake, T.; Goto, A.; Aoki, H.; Shibata, H.; Ito, K.; Hirakawa, A.; Yamada, Y.; Akiyama, H. Induced pluripotent stem cell-derived tenocyte-like cells promote the regeneration of injured tendons in mice. Sci. Rep. 2020, 10, 3992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodeo, S. Stem Cells 101. Am. J. Sports Med. 2021, 49, 1417–1420. [Google Scholar] [CrossRef] [PubMed]
- Beitzel, K.; Allen, D.; Apostolakos, J.; Russell, R.P.; McCarthy, M.B.; Gallo, G.J.; Cote, M.P.; Mazzocca, A.D. US definitions, current use, and FDA stance on use of platelet-rich plasma in sports medicine. J. Knee Surg. 2015, 28, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Regulatory Considerations for Human Cells, Tissues, and Cellular and Tissue-Based Products: Minimal Manipulation and Homologous Use Guidance for Industry and Food and Drug Administration Staff Contains Nonbinding Recommendations Regulatory Considerations. In Guidance for Industry and Food and Drug Administration Staff; U.S. Department of Health and Human Services: Washington, DC, USA, 2020. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/regulatory-considerations-human-cells-tissues-and-cellular-and-tissue-based-products-minimal (accessed on 8 August 2021).
- Rodeo, S.A. Moving Toward Responsible Use of Biologics in Sports Medicine. Am. J. Sports Med. 2018, 46, 1797–1799. [Google Scholar] [CrossRef] [PubMed]
- Dominici, M.; Blanc, K.L.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef]
- Lhee, S.H.; Jo, Y.H.; Kim, B.Y.; Nam, B.M.; Nemeno, J.G.; Lee, S.; Yang, W.; Lee, J.I. Novel supplier of mesenchymal stem cell: Subacromial bursa. In Transplantation Proceedings; Elsevier: Amsterdam, The Netherlands, 2013; Volume 45, pp. 3118–3121. [Google Scholar] [CrossRef]
- Utsunomiya, H.; Uchida, S.; Sekiya, I.; Sakai, A.; Moridera, K.; Nakamura, T. Isolation and characterization of human mesenchymal stem cells derived from shoulder tissues involved in rotator cuff tears. Am. J. Sports Med. 2013, 41, 657–668. [Google Scholar] [CrossRef]
- Song, N.; Armstrong, A.; Li, F.; Ouyang, H.; Niyibizi, C. Multipotent mesenchymal stem cells from human subacromial bursa: Potential for cell based tendon tissue engineering. Tissue Eng. Part A 2014, 20, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Steinert, A.F.; Kunz, M.; Prager, P.; Göbel, S.; Klein-Hitpass, L.; Ebert, R.; Nöth, U.; Jakob, F.; Gohlke, F. Characterization of bursa subacromialis-derived mesenchymal stem cells. Stem Cell Res. Ther. 2015, 6, 114. [Google Scholar] [CrossRef] [Green Version]
- Muschler, G.F.; Midura, R.J. Connective tissue progenitors: Practical concepts for clinical applications. Clin. Orthop. Relat. Res. 2002, 1, 66–80. [Google Scholar] [CrossRef]
- Patterson, T.E.; Boehm, C.; Nakamoto, C.; Rozic, R.; Walker, E.; Piuzzi, N.S.; Muschler, G.F. The Efficiency of Bone Marrow Aspiration for the Harvest of Connective Tissue Progenitors from the Human Iliac Crest. J. Bone Jt. Surg.-Am. Vol. 2017, 99, 1673–1682. [Google Scholar] [CrossRef]
- Morikawa, D.; Johnson, J.D.; Kia, C.; McCarthy, M.B.R.; Macken, C.; Bellas, N.; Baldino, J.B.; Cote, M.P.; Mazzocca, A.D. Examining the Potency of Subacromial Bursal Cells as a Potential Augmentation for Rotator Cuff Healing: An In Vitro Study. Arthrosc.-J. Arthrosc. Relat. Surg. 2019, 35, 2978–2988. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, D.; Muench, L.N.; Baldino, J.B.; Kia, C.; Johnson, J.; Otto, A.; Pauzenberger, L.; Dyrna, F.; McCarthy, M.B.R.; Mazzocca, A.D. Comparison of Preparation Techniques for Isolating Subacromial Bursa-Derived Cells as a Potential Augment for Rotator Cuff Repair. Arthrosc.-J. Arthrosc. Relat. Surg. 2020, 36, 80–85. [Google Scholar] [CrossRef]
- Baldino, J.B.; Muench, L.N.; Kia, C.; Johnson, J.; Morikawa, D.; Tamburini, L.; Landry, A.; Gordon-Hackshaw, L.; Bellas, N.; McCarthy, M.B.; et al. Intraoperative and In Vitro Classification of Subacromial Bursal Tissue. Arthrosc.-J. Arthrosc. Relat. Surg. 2020, 36, 2057–2068. [Google Scholar] [CrossRef]
- Dyrna, F.; Zakko, P.; Pauzenberger, L.; McCarthy, M.B.; Mazzocca, A.D.; Dyment, N.A. Human Subacromial Bursal Cells Display Superior Engraftment Versus Bone Marrow Stromal Cells in Murine Tendon Repair. Am. J. Sports Med. 2018, 46, 3511–3520. [Google Scholar] [CrossRef]
- Muench, L.N.; Kia, C.; Berthold, D.P.; Uyeki, C.; Otto, A.; Cote, M.P.; McCarthy, M.B.; Beitzel, K.; Arciero, R.A.; Mazzocca, A.D. Preliminary Clinical Outcomes Following Biologic Augmentation of Arthroscopic Rotator Cuff Repair Using Subacromial Bursa, Concentrated Bone Marrow Aspirate, and Platelet-Rich Plasma. Arthrosc. Sport. Med. Rehabil. 2020, 2, e803–e813. [Google Scholar] [CrossRef] [PubMed]
- Dei Giudici, L.; Castricini, R. Local Autologous Stem Cells Application in Rotator Cuff Repairs: “LASCA” Technique. Arthrosc. Tech. 2020, 9, e1571–e1575. [Google Scholar] [CrossRef]
- Freislederer, F.; Dittrich, M.; Scheibel, M. Biological Augmentation With Subacromial Bursa in Arthroscopic Rotator Cuff Repair. Arthrosc. Tech. 2019, 8, e741–e747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carballo, C.B.; Lebaschi, A.; Rodeo, S.A. Cell-based approaches for augmentation of tendon repair. Tech. Shoulder Elb. Surg. 2017, 18, e6–e14. [Google Scholar] [CrossRef]
- Le, B.T.N.; Wu, X.L.; Lam, P.H.; Murrell, G.A.C. Factors predicting rotator cuff retears: An analysis of 1000 consecutive rotator cuff repairs. Am. J. Sports Med. 2014, 42, 1134–1142. [Google Scholar] [CrossRef]
- Ateschrang, A.; Eggensperger, F.; Ahrend, M.D.; Schröter, S.; Stöckle, U.; Kraus, T.M. Obesity causes poorer clinical results and higher re-tear rates in rotator cuff repair. Arch. Orthop. Trauma Surg. 2018, 138, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Zhang, J.; Ruan, D.; Zhao, K.; Chen, X.; Shen, W. Clinical and Structural Outcomes After Rotator Cuff Repair in Patients With Diabetes: A Meta-analysis. Orthop. J. Sport. Med. 2020, 8, 2325967120948499. [Google Scholar] [CrossRef] [PubMed]
- Lobo-Escolar, L.; Ramazzini-Castro, R.; Codina-Grañó, D.; Lobo, E.; Minguell-Monyart, J.; Ardèvol, J. Risk factors for symptomatic retears after arthroscopic repair of full-thickness rotator cuff tears. J. Shoulder Elb. Surg. 2020, 32, 2191–2200. [Google Scholar] [CrossRef]
- Muench, L.N.; Baldino, J.B.; Berthold, D.P.; Kia, C.; Lebaschi, A.; Cote, M.P.; McCarthy, M.B.; Mazzocca, A.D. Subacromial Bursa–Derived Cells Demonstrate High Proliferation Potential Regardless of Patient Demographics and Rotator Cuff Tear Characteristics. Arthrosc.-J. Arthrosc. Relat. Surg. 2020, 36, 2794–2802. [Google Scholar] [CrossRef]
- Morikawa, D.; LeVasseur, M.R.; Luczak, S.B.; Mancini, M.R.; Bellas, N.; McCarthy, M.B.R.; Cote, M.P.; Berthold, D.P.; Muench, L.N.; Mazzocca, A.D. Decreased Colony-Forming Ability of Subacromial Bursa-Derived Cells During Revision Arthroscopic Rotator Cuff Repair. Arthrosc. Sports Med. Rehabil. 2021, 3, e1047–e1054. [Google Scholar] [CrossRef]
- Park, J.H.; Oh, K.S.; Kim, T.M.; Kim, J.; Yoon, J.P.; Kim, J.Y.; Chung, S.W. Effect of Smoking on Healing Failure After Rotator Cuff Repair. Am. J. Sports Med. 2018, 46, 2960–2968. [Google Scholar] [CrossRef]
- Garcia, G.H.; Liu, J.N.; Wong, A.; Cordasco, F.; Dines, D.M.; Dines, J.S.; Gulotta, L.V.; Warren, R. Hyperlipidemia increases the risk of retear after arthroscopic rotator cuff repair. J. Shoulder Elb. Surg. 2017, 26, 2086–2090. [Google Scholar] [CrossRef]
- Shin, S.J.; Kook, S.H.; Rao, N.; Seo, M.J. Clinical Outcomes of Modified Mason-Allen Single-Row Repair for Bursal-Sided Partial-Thickness Rotator Cuff Tears: Comparison with the Double-Row Suture-Bridge Technique. Am. J. Sports Med. 2015, 43, 1976–1982. [Google Scholar] [CrossRef]
- O’Donnell, E.A.; Fu, M.C.; White, A.E.; Taylor, S.A.; Dines, J.S.; Dines, D.M.; Warren, R.F.; Gulotta, L.V. The Effect of Patient Characteristics and Comorbidities on the Rate of Revision Rotator Cuff Repair. Arthrosc.-J. Arthrosc. Relat. Surg. 2020, 36, 2380–2388. [Google Scholar] [CrossRef]
- Mazzocca, A.D.; McCarthy, M.B.R.; Chowaniec, D.M.; Cote, M.P.; Arciero, R.A.; Drissi, H. Rapid isolation of human stem cells (connective tissue progenitor cells) from the proximal humerus during arthroscopic rotator cuff surgery. Am. J. Sports Med. 2010, 38, 1438–1447. [Google Scholar] [CrossRef]
- Beitzel, K.; McCarthy, M.B.R.; Cote, M.P.; Durant, T.J.S.; Chowaniec, D.M.; Solovyova, O.; Russell, R.P.; Arciero, R.A.; Mazzocca, A.D. Comparison of mesenchymal stem cells (osteoprogenitors) harvested from proximal humerus and distal femur during arthroscopic surgery. Arthrosc.-J. Arthrosc. Relat. Surg. 2013, 29, 301–308. [Google Scholar] [CrossRef]
- Voss, A.; McCarthy, M.B.; Singh, H.; Beitzel, K.; DiVenere, J.; Cote, M.P.; Hoberman, A.R.; Nowak, M.; Imhoff, A.B.; Mazzocca, A.D. The Influence of Trocar Fenestration and Volume on Connective Tissue Progenitor Cells (Stem Cells) in Arthroscopic Bone Marrow Aspiration from the Proximal Humerus. Arthrosc.-J. Arthrosc. Relat. Surg. 2017, 33, 1167–1174.e. [Google Scholar] [CrossRef] [PubMed]
- McElvany, M.D.; McGoldrick, E.; Gee, A.O.; Neradilek, M.B.; Matsen, F.A. Rotator cuff repair: Published evidence on factors associated with repair integrity and clinical outcome. Am. J. Sports Med. 2015, 43, 491–500. [Google Scholar] [CrossRef]
- Saccomanno, M.F.; Sircana, G.; Cazzato, G.; Donati, F.; Randelli, P.; Milano, G. Prognostic factors influencing the outcome of rotator cuff repair: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3809–3819. [Google Scholar] [CrossRef]
- Djahangiri, A.; Cozzolino, A.; Zanetti, M.; Helmy, N.; Rufibach, K.; Jost, B.; Gerber, C. Outcome of single-tendon rotator cuff repair in patients aged older than 65 years. J. Shoulder Elb. Surg. 2013, 22, 45–51. [Google Scholar] [CrossRef]
- Tashjian, R.Z.; Hollins, A.M.; Kim, H.M.; Teefey, S.A.; Middleton, W.D.; Steger-May, K.; Galatz, L.M.; Yamaguchi, K. Factors affecting healing rates after arthroscopic double-row rotator cuff repair. Am. J. Sports Med. 2010, 38, 2435–2442. [Google Scholar] [CrossRef]
- Balyk, R.; Luciak-Corea, C.; Otto, D.; Baysal, D.; Beaupre, L. Do outcomes differ after rotator cuff repair for patients receiving workers’ compensation? Clin. Orthop. Relat. Res. 2008, 466, 3025–3033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallon, W.J.; Misamore, G.; Snead, D.S.; Denton, P. The impact of preoperative smoking habits on the results of rotator cuff repair. J. Shoulder Elb. Surg. 2004, 13, 129–132. [Google Scholar] [CrossRef]
- Miyatake, K.; Takeda, Y.; Fujii, K.; Suzue, N.; Kawasaki, Y.; Omichi, Y.; Yokoyama, K. Comparable clinical and structural outcomes after arthroscopic rotator cuff repair in diabetic and non-diabetic patients. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3810–3817. [Google Scholar] [CrossRef]
- Cho, N.S.; Moon, S.C.; Jeon, J.W.; Rhee, Y.G. The influence of diabetes mellitus on clinical and structural outcomes after arthroscopic rotator cuff repair. Am. J. Sports Med. 2015, 43, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Clement, N.D.; Hallett, A.; MacDonald, D.; Howie, C.; McBirnie, J. Does diabetes affect outcome after arthroscopic repair of the rotator cuff? J. Bone Jt. Surg.-Ser. B 2010, 92, 1112–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, A.L.; Shapiro, J.A.; Ahn, A.K.; Zuckerman, J.D.; Cuomo, F. Rotator cuff repair in patients with type I diabetes mellitus. J. Shoulder Elb. Surg. 2003, 12, 416–421. [Google Scholar] [CrossRef]
- Kessler, K.E.; Robbins, C.B.; Bedi, A.; Carpenter, J.E.; Gagnier, J.J.; Miller, B.S. Does Increased Body Mass Index Influence Outcomes After Rotator Cuff Repair? Arthrosc.-J. Arthrosc. Relat. Surg. 2018, 34, 754–761. [Google Scholar] [CrossRef]
- Warrender, W.J.; Brown, O.L.; Abboud, J.A. Outcomes of arthroscopic rotator cuff repairs in obese patients. J. Shoulder Elb. Surg. 2011, 20, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Luo, M.; Pan, J.; Liang, G.; Feng, W.; Zeng, L.; Yang, W.; Liu, J. Risk Factors Affecting Rotator Cuff Retear After Arthroscopic Repair: A meta-analysis and systematic review. J. Shoulder Elb. Surg. 2021, in press. [Google Scholar] [CrossRef]


{kind=link}
| Number of Colony Forming Units | ||||||||
|---|---|---|---|---|---|---|---|---|
| Bursa over Rotator Cuff Tendon | Bursa over Rotator Cuff Muscle | |||||||
| 103 Cells/Well | 104 Cells/Well | 103 Cells/Well | 104 Cells/Well | |||||
| rho | p-Value | rho | p-Value | rho | p-Value | rho | p-Value | |
| Age | −0.179 | 0.522 | −0.319 | 0.246 | −0.036 | 0.899 | −0.013 | 0.965 |
| Sex (Female) | 0.000 | 1.000 | −0.062 | 0.827 | −0.031 | 0.913 | 0.186 | 0.508 |
| Height (cm) | 0.097 | 0.732 | 0.138 | 0.624 | 0.116 | 0.680 | −0.091 | 0.746 |
| Weight (kg) | −0.000 | 1.000 | −0.173 | 0.537 | 0.136 | 0.629 | −0.127 | 0.652 |
| BMI (kg/m2) | −0.189 | 0.499 | −0.368 | 0.177 | −0.129 | 0.648 | −0.161 | 0.567 |
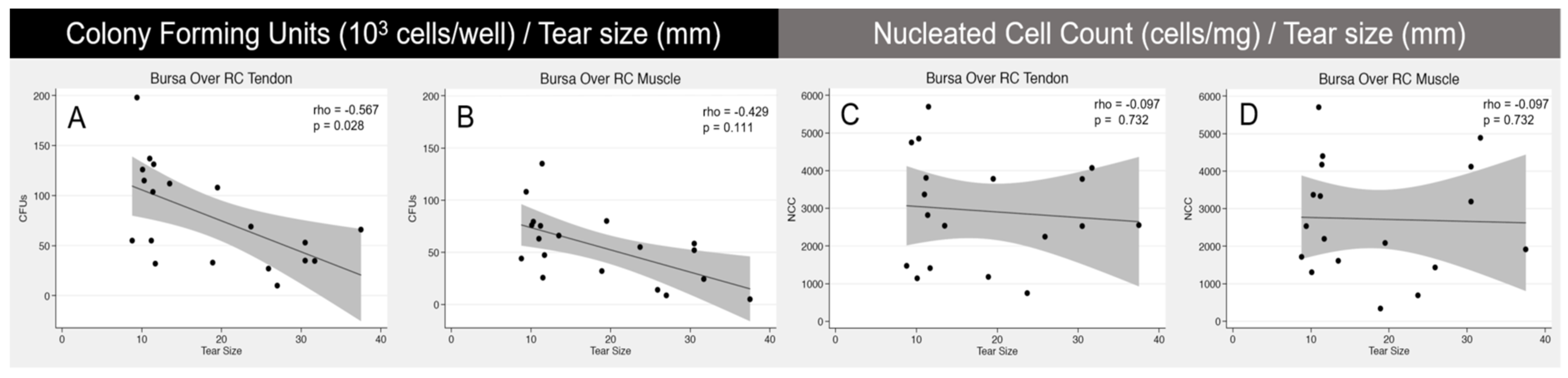
| Tear size (mm) | −0.567 | 0.028 * | −0.645 | 0.009 * | −0.429 | 0.111 | −0.434 | 0.106 |
| Smoking (Non, Former, Current) | −0.147 | 0.602 | −0.137 | 0.627 | 0.221 | 0.429 | −0.018 | 0.950 |
| Brinkman Index (Ciggarettes/d × y) | 0.113 | 0.690 | 0.105 | 0.709 | 0.270 | 0.331 | 0.094 | 0.739 |
| Diabetes mellitus (Yes) | −0.232 | 0.407 | −0.077 | 0.785 | −0.424 | 0.115 | 0.039 | 0.891 |
| Thyroid disease (Yes) | −0.347 | 0.205 | −0.424 | 0.115 | −0.193 | 0.491 | −0.270 | 0.330 |
| Hypertension (Yes) | 0.196 | 0.483 | 0.196 | 0.483 | 0.223 | 0.411 | 0.196 | 0.483 |
| Nucleated Cell Count per Milligram | ||||
|---|---|---|---|---|
| Bursa Over RC Tendon | Bursa over RC Muscle | |||
| rho | p-Value | rho | p-Value | |
| Age | 0.165 | 0.557 | −0.040 | 0.889 |
| Sex (Female) | 0.000 | 1.000 | 0.000 | 1.000 |
| Height (cm) | −0.091 | 0.746 | −0.138 | 0.624 |
| Weight (kg) | −0.363 | 0.184 | −0.038 | 0.894 |
| BMI (kg/m2) | −0.361 | 0.187 | −0.057 | 0.840 |
| Tear size (mm) | −0.097 | 0.732 | −0.097 | 0.732 |
| Smoking (Non, Former, Current) | −0.445 | 0.096 | −0.078 | 0.782 |
| Brinkman Index (Ciggarettes/d × y) | −0.299 | 0.280 | 0.028 | 0.922 |
| Diabetes mellitus (Yes) | 0.039 | 0.891 | 0.077 | 0.785 |
| Thyroid disease (Yes) | −0.039 | 0.891 | −0.270 | 0.330 |
| Hypertension (Yes) | −0.229 | 0.411 | −0.295 | 0.2865 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morikawa, D.; Hawthorne, B.C.; McCarthy, M.B.R.; Bellas, N.; Johnson, J.D.; Trudeau, M.T.; Murphy, K.V.; Mancini, M.R.; LeVasseur, M.R.; Cote, M.P.; et al. Analysis of Patient Factors Affecting In Vitro Characteristics of Subacromial Bursal Connective Tissue Progenitor Cells during Rotator Cuff Repair. J. Clin. Med. 2021, 10, 4006. https://doi.org/10.3390/jcm10174006
Morikawa D, Hawthorne BC, McCarthy MBR, Bellas N, Johnson JD, Trudeau MT, Murphy KV, Mancini MR, LeVasseur MR, Cote MP, et al. Analysis of Patient Factors Affecting In Vitro Characteristics of Subacromial Bursal Connective Tissue Progenitor Cells during Rotator Cuff Repair. Journal of Clinical Medicine. 2021; 10(17):4006. https://doi.org/10.3390/jcm10174006
Chicago/Turabian StyleMorikawa, Daichi, Benjamin C. Hawthorne, Mary Beth R. McCarthy, Nicholas Bellas, Jeremiah D. Johnson, Maxwell T. Trudeau, Kyle V. Murphy, Michael R. Mancini, Matthew R. LeVasseur, Mark P. Cote, and et al. 2021. "Analysis of Patient Factors Affecting In Vitro Characteristics of Subacromial Bursal Connective Tissue Progenitor Cells during Rotator Cuff Repair" Journal of Clinical Medicine 10, no. 17: 4006. https://doi.org/10.3390/jcm10174006