
Prepregnancy Assessment of Liver Function to Predict Perinatal and Postpregnancy Outcomes in Biliary Atresia Patients with Native Liver

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
3. Results
3.1. Patients
3.2. Maternal Characteristics and Obstetrical Outcomes
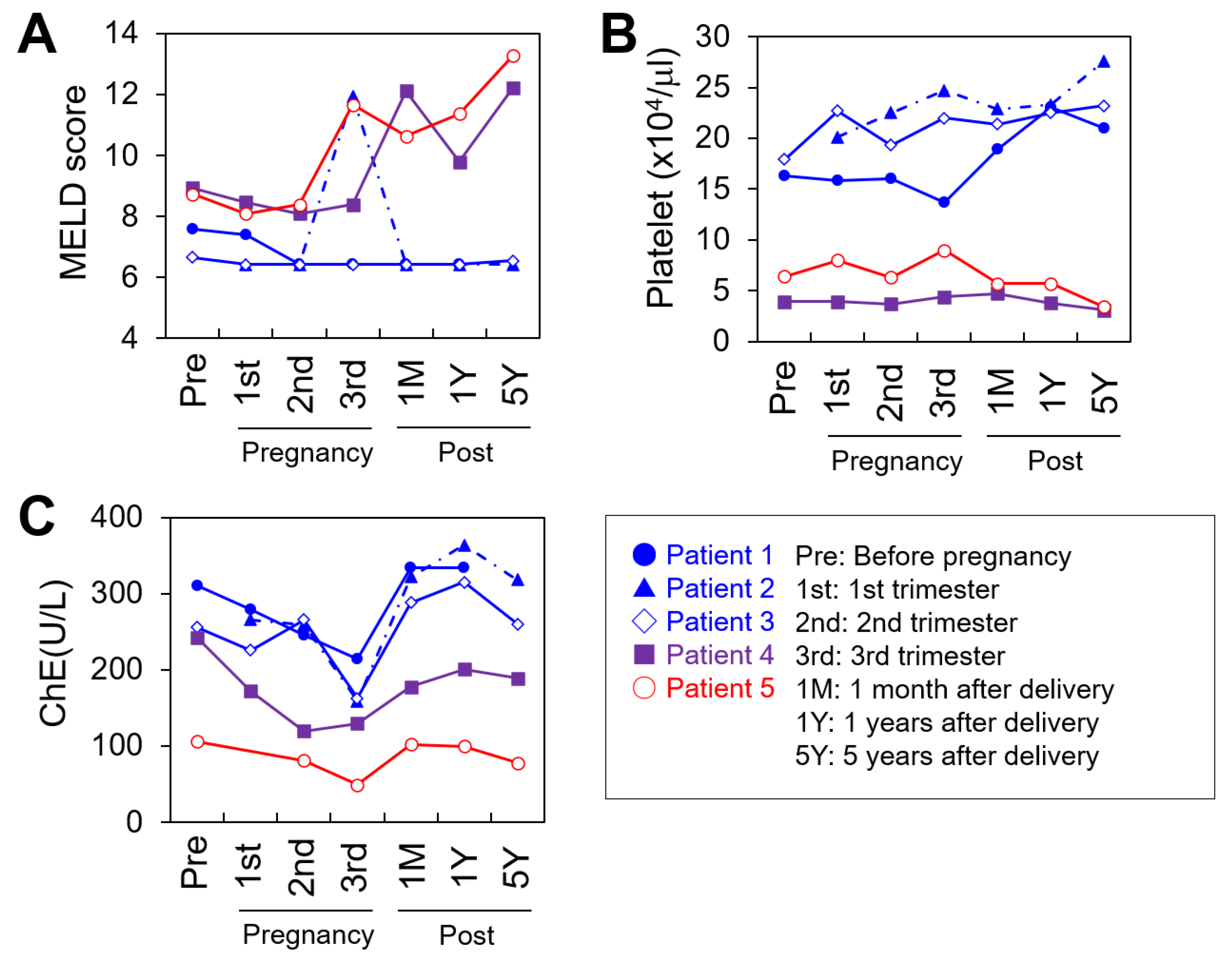
3.3. Maternal Liver Function during the Perinatal Period
3.4. Maternal Prognosis after Delivery
3.5. Individual Clinical Courses in Pregnancy
3.5.1. Patient 1: Favorable Case
3.5.2. Patient 2: Favorable Case
3.5.3. Patient 3: Favorable Case
3.5.4. Patient 4: Borderline Case
3.5.5. Patient 5: Unfavorable Case
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kasai, M.; Kimura, S.; Asakura, Y.; Suzuki, H.; Taira, Y.; Ohashi, E. Surgical treatment of biliary atresia. J. Pediatr. Surg. 1968, 3, 665–675. [Google Scholar]
- Serinet, M.O.; Wildhaber, B.E.; Broué, P.; Lachaux, A.; Sarles, J.; Jacquemin, E.; Gauthier, F.; Chardot, C. Impact of age at Kasai operation on its results in late childhood and adolescence: A rational basis for biliary atresia screening. Pediatrics 2009, 123, 1280–1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nio, M.; Sasaki, H.; Wada, M.; Kazama, T.; Nishi, K.; Tanaka, H. Impact of age at Kasai operation on short- and long-term outcomes of type III biliary atresia at a single institution. J. Pediatr. Surg. 2010, 45, 2361–2363. [Google Scholar] [CrossRef] [PubMed]
- Ng, V.L.; Haber, B.H.; Magee, J.C.; Miethke, A.; Murray, K.F.; Michail, S.; Karpen, S.J.; Kerkar, N.; Molleston, J.P.; Romero, R.; et al. Childhood Liver Disease Research and Education Network (CHiLDREN). Medical status of 219 children with biliary atresia surviving long-term with their native livers: Results from a North American multicenter consortium. J. Pediatr. 2014, 165, 539–546.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadzić, N.; Davenport, M.; Tizzard, S.; Singer, J.; Howard, E.R.; Mieli-Vergani, G. Long-term survival following Kasai portoenterostomy: Is chronic liver disease inevitable? J. Pediatr. Gastroenterol. Nutr. 2003, 37, 430–433. [Google Scholar] [CrossRef] [PubMed]
- Shimaoka, S.; Ohi, R.; Saeki, M.; Miyano, T.; Tanaka, K.; Shiraki, K.; Nio, M. Japanese Biliary Atresia Society. Problems during and after pregnancy of former biliary atresia patients treated successfully by the Kasai procedure. J. Pediatr. Surg. 2001, 36, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Ando, H.; Inomata, Y.; Iwanaka, T.; Kuroda, T.; Nio, M.; Matsui, A.; Yoshida, M. Japanese Biliary Atresia Society. Clinical practice guidelines for biliary atresia in Japan: A secondary publication of the abbreviated version translated into English. J. Hepatobiliary Pancreat Sci. 2021, 28, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, T.; Saeki, M.; Morikawa, N.; Fuchimoto, Y. Biliary atresia and pregnancy: Puberty may be an important point for predicting the outcome. J. Pediatr. Surg. 2005, 40, 1852–1855. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Nio, M.; Hayashi, Y.; Ishii, T.; Sano, N.; Ohi, R. Problems during and after pregnancy in female patients with biliary atresia. J. Pediatr. Surg. 2007, 42, 1329–1332. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, O.E.; Crosby, D.; Byrne, B.; Regan, C. Pregnancy complicated by portal hypertension secondary to biliary atresia. Case Rep. Obstet. Gynecol. 2013, 2013, 421386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samyn, M.; Davenport, M.; Jain, V.; Hadzic, N.; Joshi, D.; Heneghan, M.; Dhawan, A.; Heaton, N. Young People with Biliary Atresia Requiring Liver Transplantation: A Distinct Population Requiring Specialist Care. Transplantation 2019, 103, e99–e107. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, T.; Saeki, M.; Morikawa, N.; Watanabe, K. Management of adult biliary atresia patients: Should hard work and pregnancy be discouraged? J. Pediatr. Surg. 2007, 42, 2106–2109. [Google Scholar] [CrossRef] [PubMed]
- Samyn, M. Transitional care of biliary atresia. Semin. Pediatr. Surg. 2020, 29, 150948. [Google Scholar] [CrossRef] [PubMed]
- Westbrook, R.H.; Yeoman, A.D.; O’Grady, J.G.; Harrison, P.M.; Devlin, J.; Heneghan, M.A. Model for end-stage liver disease score predicts outcome in cirrhotic patients during pregnancy. Clin. Gastroenterol. Hepatol. 2011, 9, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.R.; Biggins, S.W.; Kremers, W.K.; Wiesner, R.H.; Kamath, P.S.; Benson, J.T.; Edwards, E.; Therneau, T.M. Hyponatremia and mortality among patients on the liver-transplant waiting list. N. Engl. J. Med. 2008, 359, 1018–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pathak, B.; Sheibani, L.; Lee, R.H. Cholestasis of pregnancy. Obstet Gynecol. Clin. N. Am. 2010, 37, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Surti, B.; Saab, S. Pregnancy and cirrhosis. Liver Transpl. 2008, 14, 1081–1091. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient | Maternal Age | Nulli-Parity | Mode of Delivery | GA at Delivery (Weeks/Days) | BW | Changes in BA Complication during the Perinatal Period | ||
|---|---|---|---|---|---|---|---|---|
| Prepregnancy | during Pregnancy | Postpartum | ||||||
| 1 | 30 | Yes | VD | 39 w 4 d | 2980 g | None | None | None |
| 2 | 32 | Yes | VD | 36 w 6 d | 2578 g | Cholangitis | Recurrence of cholangitis | Recurrence of cholangitis |
| 3 | 39 | No | VD | 36 w 5 d | 2690 g | Cholangitis | Recurrence of cholangitis | Recurrence of cholangitis |
| 4 | 40 | No | CS | 37 w 3 d | 2590 g | Cholangitis GE varices Thrombocytopenia | Recurrence of cholangitis Exacerbation of GE varices Thrombocytopenia | Recurrence of cholangitis Exacerbation of GE varices Thrombocytopenia Liver dysfunction |
| 5 | 34 | Yes | CS | 30 w 0 d | 842 g | GE varices Thrombocytopenia Ascites | Rupture of GE varices Hepatic encephalopathy Thrombocytopenia Ascites Liver dysfunction | Exacerbation of GE varices Hepatic encephalopathy Thrombocytopenia Ascites Liver dysfunction |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takahashi, N.; Ochiai, D.; Yamada, Y.; Tamagawa, M.; Kanamori, H.; Kato, M.; Ikenoue, S.; Kasuga, Y.; Kuroda, T.; Tanaka, M. Prepregnancy Assessment of Liver Function to Predict Perinatal and Postpregnancy Outcomes in Biliary Atresia Patients with Native Liver. J. Clin. Med. 2021, 10, 3956. https://doi.org/10.3390/jcm10173956
Takahashi N, Ochiai D, Yamada Y, Tamagawa M, Kanamori H, Kato M, Ikenoue S, Kasuga Y, Kuroda T, Tanaka M. Prepregnancy Assessment of Liver Function to Predict Perinatal and Postpregnancy Outcomes in Biliary Atresia Patients with Native Liver. Journal of Clinical Medicine. 2021; 10(17):3956. https://doi.org/10.3390/jcm10173956
Chicago/Turabian StyleTakahashi, Nobuhiro, Daigo Ochiai, Yohei Yamada, Masumi Tamagawa, Hiroki Kanamori, Mototoshi Kato, Satoru Ikenoue, Yoshifumi Kasuga, Tatsuo Kuroda, and Mamoru Tanaka. 2021. "Prepregnancy Assessment of Liver Function to Predict Perinatal and Postpregnancy Outcomes in Biliary Atresia Patients with Native Liver" Journal of Clinical Medicine 10, no. 17: 3956. https://doi.org/10.3390/jcm10173956