
Targeted Temperature Management after Cardiac Arrest: A Systematic Review and Meta-Analysis with Trial Sequential Analysis


 ,
,
Abstract
:1. Introduction
2. Methods
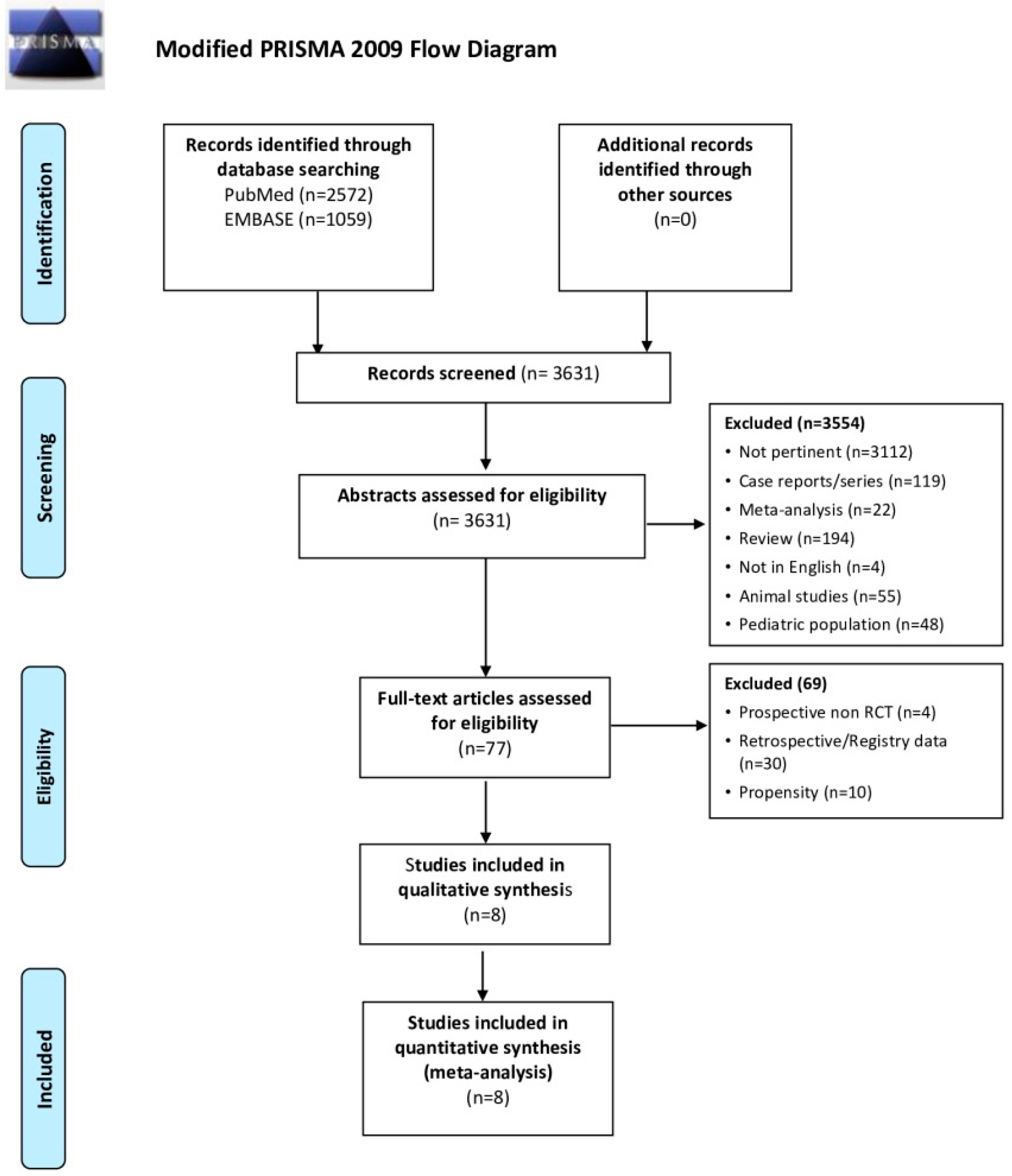
2.1. Search Strategy and Criteria
2.2. Groups and Endpoints
2.3. Quality Assessment and GRADE of Evidence
2.4. Statistical Analysis
3. Results
3.1. Survival
3.2. Neurological Outcome
3.3. Adverse Events
3.4. Grade of Evidence
3.5. Trial Sequential Analysis
3.6. Assessing Risk of Bias and Publication Bias
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Nolan, J.P.; Sandroni, C.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.; et al. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines 2021: Post-resuscitation care. Resuscitation 2021, 161, 220–269. [Google Scholar] [CrossRef]
- Nielsen, N.; Wetterslev, J.; Cronberg, T.; Erlinge, D.; Gasche, Y.; Hassager, C.; Horn, J.; Hovdenes, J.; Kjaergaard, J.; Kuiper, M.; et al. Targeted temperature management at 33 degrees C versus 36 degrees C after cardiac arrest. N. Engl. J. Med. 2013, 369, 2197–2206. [Google Scholar] [CrossRef] [Green Version]
- Nolan, J.P.; Soar, J.; Cariou, A.; Cronberg, T.; Moulaert, V.R.; Deakin, C.D.; Bottiger, B.W.; Friberg, H.; Sunde, K.; Sandroni, C. European Resuscitation Council and European Society of Intensive Care Medicine 2015 guidelines for post-resuscitation care. Intensiv. Care Med. 2015, 41, 2039–2056. [Google Scholar] [CrossRef]
- Lascarrou, J.-B.; Merdji, H.; Le Gouge, A.; Colin, G.; Grillet, G.; Girardie, P.; Coupez, E.; Dequin, P.-F.; Cariou, A.; Boulain, T.; et al. Targeted Temperature Management for Cardiac Arrest with Nonshockable Rhythm. N. Engl. J. Med. 2019, 381, 2327–2337. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Sanfilippo, F.; La Via, L.; Tigano, S.; Morgana, A.; La Rosa, V.; Astuto, M. Trial sequential analysis: The evaluation of the robustness of meta-analyses findings and the need for further research. Euromediterranean Biomed. J. 2021, 16, 104–107. [Google Scholar]
- Afshari, A.; Wetterslev, J. When may systematic reviews and meta-analyses be considered reliable? Eur. J. Anaesthesiol. 2015, 32, 85–87. [Google Scholar] [CrossRef]
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N. Engl. J. Med. 2002, 346, 549–556. [Google Scholar] [CrossRef]
- Bernard, S.A.; Gray, T.W.; Buist, M.D.; Jones, B.M.; Silvester, W.; Gutteridge, G.; Smith, K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N. Engl. J. Med. 2002, 346, 557–563. [Google Scholar] [CrossRef]
- Hachimi-Idrissi, S.; Corne, L.; Ebinger, G.; Michotte, Y.; Huyghens, L. Mild hypothermia induced by a helmet device: A clinical feasibility study. Resuscitation 2001, 51, 275–281. [Google Scholar] [CrossRef]
- Hachimi-Idrissi, S.; Zizi, M.; Nguyen, D.N.; Schiettecate, J.; Ebinger, G.; Michotte, Y.; Huyghens, L. The evolution of serum astroglial S-100 beta protein in patients with cardiac arrest treated with mild hypothermia. Resuscitation 2005, 64, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Laurent, I.; Adrie, C.; Vinsonneau, C.; Cariou, A.; Chiche, J.-D.; Ohanessian, A.; Spaulding, C.; Carli, P.; Dhainaut, J.-F.; Monchi, M. High-volume hemofiltration after out-of-hospital cardiac arrest: A randomized study. J. Am. Coll. Cardiol. 2005, 46, 432–437. [Google Scholar] [CrossRef] [Green Version]
- Dankiewicz, J.; Cronberg, T.; Lilja, G.; Jakobsen, J.C.; Levin, H.; Ullén, S.; Rylander, C.; Wise, M.P.; Oddo, M.; Cariou, A.; et al. Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest. N. Engl. J. Med. 2021, 384, 2283–2294. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Neumar, R.W.; Adrie, C.; Aibiki, M.; Berg, R.A.; Böttiger, B.W.; Callaway, C.; Clark, R.S.; Geocadin, R.G.; Jauch, E.; et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation 2008, 79, 350–379. [Google Scholar]
- Pellis, T.; Sanfilippo, F.; Roncarati, A.; DiBenedetto, F.; Franceschino, E.; Lovisa, D.; Magagnin, L.; Mercante, W.; Mione, V. A 4-year implementation strategy of aggressive post-resuscitation care and temperature management after cardiac arrest. Resuscitation 2014, 85, 1251–1256. [Google Scholar] [CrossRef]
- Langhelle, A.; Tyvold, S.S.; Lexow, K.; Hapnes, S.A.; Sunde, K.; Steen, P.A. In-hospital factors associated with improved outcome after out-of-hospital cardiac arrest. A comparison between four regions in Norway. Resuscitation 2003, 56, 247–263. [Google Scholar] [CrossRef]
- Hasselqvist-Ax, I.; Riva, G.; Herlitz, J.; Rosenqvist, M.; Hollenberg, J.; Nordberg, P.; Ringh, M.; Jonsson, M.; Axelsson, C.; Lindqvist, J.; et al. Early cardiopulmonary resuscitation in out-of-hospital cardiac arrest. N. Engl. J. Med. 2015, 372, 2307–2315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stær-Jensen, H.; Sunde, K.; Olasveengen, T.M.; Jacobsen, D.; Drægni, T.; Nakstad, E.R.; Eritsland, J.; Andersen, G. Bradycardia during therapeutic hypothermia is associated with good neurologic outcome in comatose survivors of out-of-hospital cardiac arrest. Crit. Care Med. 2014, 42, 2401–2408. [Google Scholar] [CrossRef] [PubMed]
- Fernando, S.M.; Di Santo, P.; Sadeghirad, B.; Lascarrou, J.-B.; Rochwerg, B.; Mathew, R.; Sekhon, M.S.; Munshi, L.; Fan, E.; Brodie, D.; et al. Targeted temperature management following out-of-hospital cardiac arrest: A systematic review and network meta-analysis of temperature targets. Intensiv. Care Med. 2021, 1–11. [Google Scholar] [CrossRef]
- Zeiner, A.; Holzer, M.; Sterz, F.; Schörkhuber, W.; Eisenburger, P.; Havel, C.; Kliegel, A.; Laggner, A.N. Hyperthermia after cardiac arrest is associated with an unfavorable neurologic outcome. Arch. Intern. Med. 2001, 161, 2007–2012. [Google Scholar] [CrossRef] [PubMed]
- Gräsner, J.T.; Wnent, J.; Herlitz, J.; Perkins, G.D.; Lefering, R.; Tjelmeland, I.; Koster, R.W.; Masterson, S.; Rossell-Ortiz, F.; Maurer, H.; et al. Survival after out-of-hospital cardiac arrest in Europe—Results of the EuReCa TWO study. Resuscitation 2020, 148, 218–226. [Google Scholar] [CrossRef]
- Thomsen, J.H.; Hassager, C.; Bro-Jeppesen, J.; Søholm, H.; Nielsen, N.; Wanscher, M.; Køber, L.; Pehrson, S.; Kjaergaard, J. Sinus bradycardia during hypothermia in comatose survivors of out-of-hospital cardiac arrest—A new early marker of favorable outcome? Resuscitation 2015, 89, 36–42. [Google Scholar] [CrossRef]
- Thomsen, J.H.; Nielsen, N.; Hassager, C.; Wanscher, M.; Pehrson, S.; Køber, L.; Bro-Jeppesen, J.; Søholm, H.; Winther-Jensen, M.; Pellis, T.; et al. Bradycardia During Targeted Temperature Management: An Early Marker of Lower Mortality and Favorable Neurologic Outcome in Comatose Out-of-Hospital Cardiac Arrest Patients. Crit. Care Med. 2016, 44, 308–318. [Google Scholar] [CrossRef]
- Huang, C.-H.; Tsai, M.-S.; Ong, H.N.; Chen, W.; Wang, C.-H.; Chang, W.-T.; Wang, T.-D.; Chen, S.-C.; Ma, M.H.-M.; Chen, W.-J. Association of hemodynamic variables with in-hospital mortality and favorable neurological outcomes in post-cardiac arrest care with targeted temperature management. Resuscitation 2017, 120, 146–152. [Google Scholar] [CrossRef]
- Taccone, F.S.; Lascarrou, J.-B.; Skrifvars, M.B. Targeted temperature management and cardiac arrest after the TTM-2 study. Crit. Care 2021, 25, 275. [Google Scholar] [CrossRef]
- Vargas, M.; Servillo, G.; Sutherasan, Y.; Rodríguez-González, R.; Brunetti, I.; Pelosi, P. Effects of in-hospital low targeted temperature after out of hospital cardiac arrest: A systematic review with meta-analysis of randomized clinical trials. Resuscitation 2015, 91, 8–18. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICOS CRITERIA | |
|---|---|
| Population | Patients experiencing CA both in and out-of-hospital, independently from the initially detected rhythm (shockable or not), with TTM performed after hospital arrival |
| Intervention | TTM with temperature range set at 32–34 °C |
| Comparison | TTM with either actively controlled or uncontrolled normothermia |
| Outcome(s) | Survival and neurological outcome at longest follow-up (primary); adverse effects (secondary) |
| Study design | Randomized controlled trial only |
| First Author Year | Location of Arrest | First Rhythm Detected | Treatment in the Intervention Group Treatment in the Control Group | Longest Follow Up GNO Assessment | Ref. |
|---|---|---|---|---|---|
| Dankiewicz 2021 N = 1861 | OHCA | Shockable 74% Non-shockable 26% | TTM (surface/ iv, 33 °C, 28 h) + active RW (12 h) Normothermia (≤37.5 °C + surface/iv if ≥37.8 °C) | 6-months mRS | [12] |
| Lascarrou 2019 N = 548 | Mixed (73% OHCA) | Non-shockable 100% | TTM (any method, 33 °C, 24 h) + active RW (8–16 h, 36 °C, 24 h) TTM (any method, 37 °C, 48 h) | 90-days CPC | [15] |
| Nielsen 2013 N = 939 | OHCA | Shockable 80% Non-shockable 20% | TTM (any method, 33 °C, 28 h) + active RW (8 h) TTM (any method, 36 °C, 28 h) + active RW (2 h) | 6-months—End trial CPC—mRS | [11] |
| Laurent 2005 * N = 42 | OHCA | Shockable 74% Non-shockable 26% | TTM (HF + ice-packs, 32 °C, 24 h) + passive RW Normothermia + HF 8 h (37 °C) | 6-months CPC | [16] |
| Hachimi-idrissi 2005 N = 61 | OHCA | Non-shockable 54% | TTM (Helmet, 33 °C, brief *) + passive RW Normothermia (37 °C) | 6-months CPC | [17] |
| Shockable 46% | TTM (mattress, 33 °C, 24 h) + passive RW Normothermia (37 °C) | ||||
| Holzer 2002 N = 136 | OHCA | Shockable 96% Other 4% | TTM (mattress, 32–34 °C, 24 h) + passive RW Normothermia (no target) | 6-months CPC | [18] |
| Bernard 2002 N = 77 | OHCA | Shockable 100% | TTM (ice-packs, 33 °C, 12 h) + active RW (6 h) Normothermia (37 °C) | Hospital discharge Home/short term rehab | [19] |
| Hachimi-idrissi 2001 N = 30 | OHCA | Non-shockable 100% | TTM (Helmet, 34 °C, brief *) + passive RW Normothermia + treatment of fever (38 °C) | 2-weeks CPC | [20] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanfilippo, F.; La Via, L.; Lanzafame, B.; Dezio, V.; Busalacchi, D.; Messina, A.; Ristagno, G.; Pelosi, P.; Astuto, M. Targeted Temperature Management after Cardiac Arrest: A Systematic Review and Meta-Analysis with Trial Sequential Analysis. J. Clin. Med. 2021, 10, 3943. https://doi.org/10.3390/jcm10173943
Sanfilippo F, La Via L, Lanzafame B, Dezio V, Busalacchi D, Messina A, Ristagno G, Pelosi P, Astuto M. Targeted Temperature Management after Cardiac Arrest: A Systematic Review and Meta-Analysis with Trial Sequential Analysis. Journal of Clinical Medicine. 2021; 10(17):3943. https://doi.org/10.3390/jcm10173943
Chicago/Turabian StyleSanfilippo, Filippo, Luigi La Via, Bruno Lanzafame, Veronica Dezio, Diana Busalacchi, Antonio Messina, Giuseppe Ristagno, Paolo Pelosi, and Marinella Astuto. 2021. "Targeted Temperature Management after Cardiac Arrest: A Systematic Review and Meta-Analysis with Trial Sequential Analysis" Journal of Clinical Medicine 10, no. 17: 3943. https://doi.org/10.3390/jcm10173943