
The Associations between Sex Hormones and Lipid Profiles in Serum of Women with Different Phenotypes of Polycystic Ovary Syndrome

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Lipid Profile Parameters and Concentration of Glucose and Insulin
2.2. Hormone Assay
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- It seems that sex hormone concentrations are mainly indirectly associated with lipids.
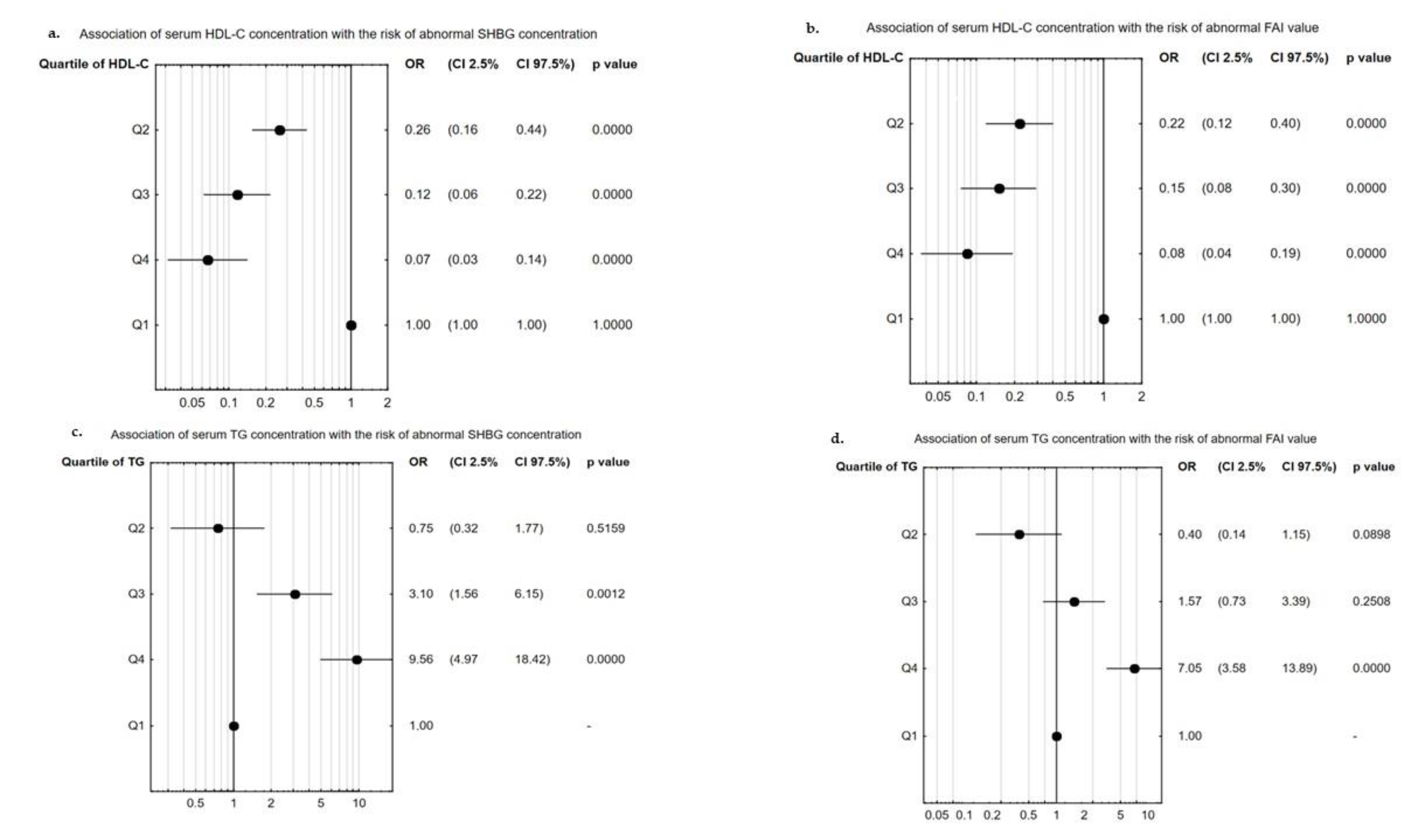
- Changes in concentration of SHBG and value of FAI were significantly associated with disturbance in HDL-C and TG levels.
- Higher quartiles of TG concentration increased the odds ratio of decreased concentration of SHBG or increased value of FAI, while higher quartiles of HDL-C level decreased disturbances in SHBG concentration and FAI value.
- The phenotypes of PCOS, BMI value, and hyperlipidemia are significant factors that influence androgen hormone concentrations in women with PCOS.
- The concentration of estradiol in the blood of women with PCOS was not associated with lipid profile parameters.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Azziz, R.; Carmina, E.; Chen, Z.; Dunaif, A.; Laven, J.S.E.; Legro, R.S.; Lizneva, D.; Natterson-Horowtiz, B.; Teede, H.J.; Yildiz, B.O. Polycystic ovary syndrome. Nat. Rev. Dis. Primers 2016, 2, 16057. [Google Scholar] [CrossRef] [PubMed]
- Goodarzi, M.O.; Dumesic, D.A.; Chazenbalk, G.; Azziz, R. Polycystic ovary syndrome: Etiology, pathogenesis and diagnosis. Nat. Rev. Endocrinol. 2011, 7, 219–231. [Google Scholar] [CrossRef]
- Mumusoglu, S.; Yildiz, B.O. Polycystic ovary syndrome phenotypes and prevalence: Differential impact of diagnostic criteria and clinical versus unselected population. Curr. Opin. Endocr. Metab. Res. 2020, 12, 66–71. [Google Scholar] [CrossRef]
- Witchel, S.F.; Oberfield, S.E.; Peña, A.S. Polycystic Ovary Syndrome: Pathophysiology, Presentation, and Treatment with Emphasis on Adolescent Girls. J. Endocr. Soc. 2019, 3, 1545–1573. [Google Scholar] [CrossRef]
- McCartney, C.R.; Marshall, J.C. Clinical practice. Polycystic Ovary Syndrome. N. Engl. J. Med. 2016, 375, 54–64. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Garrido, M.A.; Tena-Sempere, M. Metabolic dysfunction in polycystic ovary syndrome: Pathogenic role of androgen excess and potential therapeutic strategies. Mol. Metab. 2020, 35, 100937. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Xie, Y.-J.; Qu, L.-H.; Zhang, M.-X.; Mo, Z.-C. Dyslipidemia involvement in the development of polycystic ovary syndrome. Taiwan J. Obstet. Gynecol. 2019, 58, 447–453. [Google Scholar] [CrossRef]
- Marshall, J.C.; Dunaif, A. Should all women with PCOS be treated for insulin resistance? Fertil. Steril. 2012, 97, 18–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, Y.; Zhang, Y.; Li, S.; Zhou, W.; Ye, L.; Wang, L.; Tao, T.; Gu, J.; Yang, Z.; Zhao, D.; et al. Steroid hormone profiling in obese and nonobese women with polycystic ovary syndrome. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kojta, I.; Chacińska, M.; Błachnio-Zabielska, A.U. Obesity, Bioactive Lipids, and Adipose Tissue Inflammation in Insulin Resistance. Nutrients 2020, 12, 1305. [Google Scholar] [CrossRef]
- Pasquali, R.; Oriolo, C. Obesity and Androgens in Women. Front. Horm. Res. 2019, 53, 120–134. [Google Scholar] [CrossRef] [PubMed]
- Mårin, P.; Arver, S. Androgens and abdominal obesity. Baillieres Clin. Endocrinol. Metab. 1998, 12, 441–451. [Google Scholar] [CrossRef]
- Glintborg, D. Endocrine and metabolic characteristics in polycystic ovary syndrome. Dan. Med. J. 2016, 63, B5232. [Google Scholar] [PubMed]
- Li, L.; Feng, Q.; Ye, M.; He, Y.; Yao, A.; Shi, K. Metabolic effect of obesity on polycystic ovary syndrome in adolescents: A meta-analysis. J. Obstet. Gynaecol. 2017, 37, 1036–1047. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Chen, Z.; Feng, W.-J.; Long, S.-L.; Mo, Z.-C. Sex hormone-binding globulin and polycystic ovary syndrome. Clin. Chim. Acta 2019, 499, 142–148. [Google Scholar] [CrossRef]
- Gainder, S.; Sachdeva, G.; Suri, V.; Sachdeva, N.; Chopra, S. Comparison of the different pcos phenotypes based on clinical metabolic, and hormonal profile, and their response to clomiphene. Indian J. Endocrinol. Metab. 2019, 23, 326–331. [Google Scholar] [CrossRef]
- Pecks, U.; Rath, W.; Kleine-Eggebrecht, N.; Maass, N.; Voigt, F.; Goecke, T.W.; Mohaupt, M.G.; Escher, G. Maternal Serum Lipid, Estradiol, and Progesterone Levels in Pregnancy, and the Impact of Placental and Hepatic Pathologies. Geburtshilfe Frauenheilkd 2016, 76, 799–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, F.; Fan, F.; Wang, L.; Ye, W.; Zhang, Q.; Xie, S. Maternal Cadmium Levels During Pregnancy and the Relationship with Preeclampsia and Fetal Biometric Parameters. Biol. Trace Elem. Res. 2018, 186, 322–329. [Google Scholar] [CrossRef]
- Hu, J.; Zhang, Z.; Shen, W.-J.; Azhar, S. Cellular cholesterol delivery, intracellular processing and utilization for biosynthesis of steroid hormones. Nutr. Metab. 2010, 7, 47. [Google Scholar] [CrossRef] [Green Version]
- Nett, T.; Turzillo, A.; Baratta, M.; Rispoli, L. Pituitary effects of steroid hormones on secretion of follicle-stimulating hormone and luteinizing hormone. Domest. Anim. Endocrinol. 2002, 23, 33–42. [Google Scholar] [CrossRef]
- Ajmal, N.; Khan, S.Z.; Shaikh, R. Polycystic ovary syndrome (PCOS) and genetic predisposition: A review article. Eur. J. Obstet. Gynecol. Reprod. Biol. X 2019, 3, 100060. [Google Scholar] [CrossRef]
- Palmisano, B.T.; Zhu, L.; Eckel, R.H.; Stafford, J.M. Sex differences in lipid and lipoprotein metabolism. Mol. Metab. 2018, 15, 45–55. [Google Scholar] [CrossRef]
- Schiffer, L.; Kempegowda, P.; Arlt, W.; O’Reilly, M.W. MECHANISMS IN ENDOCRINOLOGY: The sexually dimorphic role of androgens in human metabolic disease. Eur. J. Endocrinol. 2017, 177, R125–R143. [Google Scholar] [CrossRef] [PubMed]
- Golden, S.H.; Robinson, K.A.; Saldanha, I.; Anton, B.; Ladenson, P.W. Clinical review: Prevalence and incidence of endocrine and metabolic disorders in the United States: A comprehensive review. J. Clin. Endocrinol. Metab. 2009, 94, 1853–1878. [Google Scholar] [CrossRef] [PubMed]
- Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Gayoso-Diz, P.; Otero-González, A.; Rodriguez-Alvarez, M.X.; Gude, F.; García, F.; De Francisco, A.; Quintela, A.G. Insulin resistance (HOMA-IR) cut-off values and the metabolic syndrome in a general adult population: Effect of gender and age: EPIRCE cross-sectional study. BMC Endocr. Disord. 2013, 13, 47. [Google Scholar] [CrossRef] [Green Version]
- Tabassum, F.; Jyoti, C.; Sinha, H.H.; Dhar, K.; Akhtar, S. Impact of polycystic ovary syndrome on quality of life of women in correlation to age, basal metabolic index, education and marriage. PLoS ONE 2021, 16, e0247486. [Google Scholar] [CrossRef]
- Wolf, W.M.; Wattick, R.A.; Kinkade, O.N.; Olfert, M.D. Geographical Prevalence of Polycystic Ovary Syndrome as Determined by Region and Race/Ethnicity. Int. J. Environ. Res. Public Health 2018, 15, 2589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazaridou, S.; Dinas, K.; Tziomalos, K. Prevalence, pathogenesis and management of prediabetes and type 2 diabetes mellitus in patients with polycystic ovary syndrome. Hormones 2017, 16, 373–380. [Google Scholar]
- Sharpless, J.L. Polycystic Ovary Syndrome and the Metabolic Syndrome. Clin. Diabetes 2003, 21, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Franik, G.; Krysta, K.; Witkowska, A.; Dudek, A.; Krzystanek, M.; Madej, P. The impact of sex hormones and metabolic markers on depressive symptoms and cognitive functioning in PCOS patients. Gynecol. Endocrinol. 2019, 35, 965–969. [Google Scholar] [CrossRef]
- Huang, T.; Balasubramanian, R.; Yao, Y.; Clish, C.B.; Shadyab, A.H.; Liu, B.; Tworoger, S.S.; Rexrode, K.M.; Manson, J.E.; Kubzansky, L.D.; et al. Associations of depression status with plasma levels of candidate lipid and amino acid metabolites: A meta-analysis of individual data from three independent samples of US postmenopausal women. Mol. Psychiatry 2020, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Carmina, E.; Nasrallah, M.P.; Guastella, E.; Lobo, R.A. Characterization of metabolic changes in the phenotypes of women with polycystic ovary syndrome in a large Mediterranean population from Sicily. Clin. Endocrinol. 2019, 91, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Gunning, M.N.; Fauser, B.C.J.M. Are women with polycystic ovary syndrome at increased cardiovascular disease risk later in life? Climacteric 2017, 20, 222–227. [Google Scholar] [CrossRef] [Green Version]
- de Groot, P.C.M.; Dekkers, O.M.; Romijn, J.A.; Dieben, S.W.M.; Helmerhorst, F.M. PCOS, coronary heart disease, stroke and the influence of obesity: A systematic review and meta-analysis. Hum. Reprod. 2011, 17, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Hestiantoro, A.; Karimah, P.D.; Shadrina, A.; Wiweko, B.; Muharam, R.; Astuti, B.P.K. Triglycerides, independent of Ferriman Gallwey Score, is a main determinant of free testosterone index in PCOS. F1000Research 2019, 8, 94. [Google Scholar] [CrossRef] [Green Version]
- Qu, X.; Donnelly, R. Sex Hormone-Binding Globulin (SHBG) as an Early Biomarker and Therapeutic Target in Polycystic Ovary Syndrome. Int. J. Mol. Sci. 2020, 21, 8191. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-J.; Yang, W.-S.; Yang, J.-H.; Hsiao, C.K.; Yang, Y.-S.; Ho, H.-N. Low sex hormone-binding globulin is associated with low high-density lipoprotein cholesterol and metabolic syndrome in women with PCOS. Hum. Reprod. 2006, 21, 2266–2271. [Google Scholar] [CrossRef] [Green Version]
- Keevil, B.G.; Adaway, J. Assessment of free testosterone concentration. J. Steroid Biochem. Mol. Biol. 2019, 190, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Pinola, P.; Piltonen, T.T.; Puurunen, J.; Vanky, E.; Sundström-Poromaa, I.; Stener-Victorin, E.; Ruokonen, A.; Puukka, K.; Tapanainen, J.S.; Morin-Papunen, L.C. Androgen Profile Through Life in Women with Polycystic Ovary Syndrome: A Nordic Multicenter Collaboration Study. J. Clin. Endocrinol. Metab. 2015, 100, 3400–3407. [Google Scholar] [CrossRef] [Green Version]
- Goodarzi, M.O.; Carmina, E.; Azziz, R. DHEA, DHEAS and PCOS. J. Steroid Biochem. Mol. Biol. 2015, 145, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, K.; Sowa, P.; Rutkowska-Talipska, J.; Kuryliszyn-Moskal, A.; Rutkowski, R. Dehydroepiandrosterone (DHEA): Hypes and Hopes. Drugs 2014, 74, 1195–1207. [Google Scholar] [CrossRef] [PubMed]
- Paschou, S.; Palioura, E.; Ioannidis, D.; Anagnostis, P.; Panagiotakou, A.; Loi, V.; Karageorgos, G.; Goulis, D.G.; Vryonidou, A. Adrenal hyperandrogenism does not deteriorate insulin resistance and lipid profile in women with PCOS. Endocr. Connect. 2017, 6, 601–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meirow, D.; Raz, I.; Yossepowitch, O.; Brzezinski, A.; Rosler, A.; Schenker, J.G.; Berry, E.M. Dyslipidaemia in polycystic ovarian syndrome: Different groups, different aetiologies? Hum. Reprod. 1996, 11, 1848–1853. [Google Scholar] [CrossRef] [Green Version]
- El Khoudary, S.R.; Brooks, M.M.; Thurston, R.C.; Matthews, K.A. Lipoprotein subclasses and endogenous sex hormones in women at midlife. J. Lipid. Res. 2014, 55, 1498–1504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naessen, T.; Rodriguez-Macias, K.; Lithell, H. Serum lipid profile improved by ultra-low doses of 17 beta-estradiol in elderly women. J. Clin. Endocrinol. Metab. 2001, 86, 2757–2762. [Google Scholar]
- Blumenfeld, Z.; Kaidar, G.; Zuckerman-Levin, N.; Dumin, E.; Knopf, C.; Hochberg, Z. Cortisol-Metabolizing Enzymes in Polycystic Ovary Syndrome. Clin. Med. Insights Reprod. Health 2016, 10, 9–13. [Google Scholar] [CrossRef] [Green Version]
- Fraser, R.; Ingram, M.C.; Anderson, N.H.; Morrison, C.; Davies, E.; Connell, J.M.C. Cortisol effects on body mass, blood pressure, and cholesterol in the general population. Hypertension 1999, 33, 1364–1368. [Google Scholar] [CrossRef] [Green Version]
- Bagir, G.S.; Bakiner, O.S.; Bozkirli, E.; Cavlak, G.; Serinsoz, H.; Ertorer, M.E. Body Mass Index below Obesity Threshold Implies Similar Cardiovascular Risk among Various Polycystic Ovary Syndrome Phenotypes. Med. Princ. Pr. 2015, 25, 61–66. [Google Scholar] [CrossRef] [Green Version]
- Neubronner, S.A.; Indran, I.R.; Chan, Y.H.; Thu, A.W.P.; Yong, E.-L. Effect of body mass index (BMI) on phenotypic features of polycystic ovary syndrome (PCOS) in Singapore women: A prospective cross-sectional study. BMC Women’s Health 2021, 21, 1–12. [Google Scholar] [CrossRef]
- Holst, J.P.; Soldin, O.P.; Guo, T.; Soldin, S.J. Steroid hormones: Relevance and measurement in the clinical laboratory. Clin. Lab. Med. 2004, 24, 105–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojas, J.; Chávez, M.; Olivar, L.C.; Rojas, M.; Morillo, J.; Mejías, J.; Calvo, M.; Bermudez, V. Polycystic Ovary Syndrome, Insulin Resistance, and Obesity: Navigating the Pathophysiologic Labyrinth. Int. J. Reprod. Med. 2014, 2014, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi-Mameghani, M.; Saghafi-Asl, M.; Pirouzpanah, S.; Aliasgharzadeh, A.; Aliashrafi, S.; Rezayi, N.; Mehrzad-Sadaghiani, M. Association of Insulin Resistance with Lipid Profile, Metabolic Syndrome, and Hormonal Aberrations in Overweight or Obese Women with Polycystic Ovary Syndrome. J. Health Popul. Nutr. 2015, 33, 157–167. [Google Scholar]


{kind=link}
| Parameters | Phenotype 1 n = 363 | Phenotype 2 n = 73 | Phenotype 3 n = 73 | Phenotype 4 n = 97 | p Value |
|---|---|---|---|---|---|
| Age (years) | 24.0 (22.0–28.0) | 27.0 (23.0–33.0) | 25.0 (22.0–28.5) | 25.0 (22.0–29.0) | >0.05 |
| BMI (kg/m2) | 24.0 (21.0–30.1) | 22.8 (19.6–27.1) | 22.4 (19.8–26.5) | 22.9 (20.4–27.2) | 0.016 |
| WHR | 0.8 (0.8–0.9) | 0.8 (0.8–0.9) | 0.8 (0.8–0.9) | 0.8 (0.8–0.9) | 0.017 |
| CHO (mg/dL) | 177.0 (160.0–197.0) | 176.0 (161.0–201.0) | 167.5 (153.0–194.0) | 179.0 (158.0–197.0) | >0.05 |
| HDL-C (mg/dL) | 51.2 ± 12.2 | 56.5 ± 11.9 | 57.4 ± 10.2 | 55.7 ± 11.3 | 0.001 |
| LDL-C (mg/dL) | 104.0 (90.0–122.0) | 104.0 (84.0–118.0) | 95.0 (80.0–110.0) | 104.5 (90.5–119.0) | >0.05 |
| TG (mg/dL) | 97.0 (68.0–154.0) | 81.5 (60.0–119.0) | 78.0 (65.0–96.0) | 82.0 (61.5–111.5) | 0.001 |
| Glucose (mg/dl) | 89.9 (85.0; 93.0) | 91.0 (84.5; 94.5) | 87.0 (84.0; 90.0) | 88.0 (84.5; 91.5) | >0.05 |
| Insulin (mU/ml) | 8.0 (5.5; 12.8) | 8.8 (5.2; 12.5) | 7.0 (5.6; 9.3) | 6.3 (4.9; 8.6) | 0.002 |
| Glucose after OGTT | 107.0 (89.0; 128.0) | 98.0 (83.0; 116.0) | 93.5 (80.0; 112.0) | 94.0 (85.0; 110.0) | 0.007 |
| Insulin after OGTT | 45.2 (27.4; 83.7) | 34.4 (22.5; 64.4) | 29.3 (19.0; 49.9) | 28.8 (20.9; 42.9) | 0.000 |
| LH (lU/L) | 7.9 (5.5–11.0) | 6.0 (3.6–7.5) c | 5.6 (4.7–6.7) | 6.8 (4.7–8.6) | 0.045 |
| FSH (lU/L) | 5.8 (4.9–6.6) | 6.0 (4.9–7.2) | 6.4 (5.2–7.4) | 5.9 (5.0–7.3) | >0.05 |
| LH/FSH | 1.3 (1.0–1.9) | 0.9 (0.6–1.4) | 0.8 (0.7–1.1) | 1.1 (0.8–1.4) | >0.05 |
| DHEA-S (µg/mL) | 310.9 (234.9–402.0) | 297.3 (230.5–383.1) | 336.4 (206.1–429.5) | 259.2 (192.9–310.9) | 0.010 |
| SHBG (nmol/L) | 47.5 (29.0–67.7) | 59.3 (31.2–90.0) | 69.2 (47.1–87.7) | 56.5 (42.9–82.5) | 0.001 |
| TT (ng/mL) | 0.4 (0.3–0.6) | 0.3 (0.2–0.5) | 0.3 (0.2–0.4) | 0.3 (0.2–0.3) | 0.001 |
| FT (pg/mL) | 1.9 (1.2–2.7) f | 1.3 (1.0–2.0) | 1.4 (0.9–2.3) | 1.0 (0.7–1.5) | 0.001 |
| FAI | 0.9 (0.5–1.5) | 0.5 (0.3–0.9) | 0.4 (0.2–0.9) | 0.4 (0.2–0.8) | 0.011 |
| AD (ng/mL) | 3.6 (2.6–4.6) | 3.0 (2.3–4.0) | 2.8 (2.2–3.6) | 2.3 (1.8–2.8) | 0.001 |
| 17-β-E2 (pg/mL) | 33.5 (22.9–47.2) | 35.2 (26.6–49.2) | 32.1 (23.8–39.1) | 29.9 (18.2–37.9) | 0.157 |
| 17α-OHP (nmol/L) | 1.8 (1.4–2.2) | 1.5 (1.2–1.9) | 1.5 (1.3–1.9) | 1.4 (1.2–1.8) | 0.003 |
| Cortisol (µg/dL) | 13.6 (11.1–16.1) | 13.7 (11.3–16.4) | 13.3 (10.2–14.8) | 13.2 (10.7–15.1) | 0.359 |
| Parameters | BMI | ||||
|---|---|---|---|---|---|
| <18.5n = 43 | 18.5–25.0 n = 336 | 25.0–30.0 n = 98 | >30.0 n = 129 | p Value | |
| Age (years) | 25.0 (21.0–31.0) | 25.0 (22.0–29.0) | 25.5 (23.0–31.0) | 27.0 (23.0–32.0) | >0.05 |
| WHR | 0.8 (0.7–0.8) d/e/f | 0.8 (0.8–0.9) | 0.9 (0.8–0.9) | 0.9 (0.9–1.0) | 0.001 |
| CHO (mg/dL) | 170.0 (156.0–189.0) | 174.0 (156.0–194.0 | 179.0 (162.0–200.5) | 189.0 (169.0–209.0) | 0.003 |
| HDL-C (mg/dL) | 62.0 ± 13.1 | 58.4 ± 11.0 | 49.8 ± 11.3 | 45.2 ± 9.4 | 0.001 |
| LDL-C (mg/dL) | 93.0 (83.0–106.0) | 102.0 (86.0–116.0) | 107.0 (92.0–122.0) | 114.0 (93.5–131.0) | 0.001 |
| TG (mg/dL) | 65.5 (56.0–85.0) | 73.0 (60.0–93.0) | 105.0 (80.0–162.0) | 148.0 (105.0–200.0) | 0.001 |
| Glucose (mg/dL) | 86.0 (81.0; 90.0) | 88.0 (84.0; 91.0) | 91.0 (87.0; 95.0) | 92.0 (88.0; 97.0) | 0.001 |
| Insulin (mU/mL) | 4.8 (3.3; 6.1) | 6.0 (4.2; 8.2) | 8.3 (7.0; 12.1) | 13.8 (10.0; 18.9) | 0.001 |
| Glucose after OGTT | 93.5 (79.0; 112.0) | 93.5 (82.0; 109.0) | 109.0 (92.0; 130.0) | 115.5 (97.5; 137.0) | 0.001 |
| Insulin after OGTT | 27.4 (17.9; 45.0) | 28.8 (20.0; 45.1) | 45.3 (28.6; 70.6) | 45.3 (28.6; 70.6) | 0.001 |
| LH (lU/L) | 6.8 (3.4–8.7) | 6.6 (4.7–10.4) | 6.4 (4.4–9.4) | 6.8 (3.4–8.7) | >0.05 |
| FSH (lU/L) | 6.2 (4.6–8.7) | 6.1 (5.1–7.2) | 5.8 (4.8–6.9) | 6.0 (5.0–6.7) | >0.05 |
| LH/FSH | 0.8 (0.5–1.4) | 1.1 (0.7–1.6) | 1.1 (0.7–1.6) | 1.0 (0.7–1.4) | >0.05 |
| DHEA-S (µg/mL) | 255.7 (180.5–315.6) | 282.8 (212.3–367.5) | 330.2 (254.3–439.9) | 305.0 (204.9–397.3) | 0.001 |
| SHBG (nmol/L) | 90.7 (69.1–123.7) | 66.3 (50.2–87.3) | 40.8 (29.9–57.0) | 30.0 (20.4–44.3) | 0.001 |
| TT (ng/mL) | 0.2 (0.2–0.4) | 0.3 (0.2–0.4) | 0.4 (0.3–0.5) | 0.4 (0.3–0.5) | 0.001 |
| FT (pg/mL) | 1.1 (0.7–1.7) | 1.3 (0.8–2.0) | 1.8 (1.1–2.6) | 1.8 (1.1–2.7) | 0.001 |
| FAI | 0.3 (0.2–0.5) | 0.4 (0.2–0.8) | 0.9 (0.5–1.5) | 1.2 (0.7–2.0) | 0.001 |
| AD (ng/mL) | 2.5 (1.7–3.4) | 2.7 (1.9–3.7) | 3.4 (2.6–4.8) | 3.0 (2.1–3.9) | 0.001 |
| 17-β-E2 (pg/mL) | 34.1 (19.9–48.0) | 33.0 (22.9–46.1) | 31.1 (19.9–45.0) | 32.8 (25.5–43.8) | >0.05 |
| 17α-OHP (nmol/L) | 1.5 (1.0–1.9) | 1.6 (1.2–2.0) | 1.9 (1.5–2.3) | 1.6 (1.3–2.0) | 0.003 |
| Cortisol (µg/dL) | 13.6 (11.1–16.1) | 14.0 (11.7–16.2) | 12.7 (10.8–15.8) | 13.3 (10.7–15.8) | 0.026 |
| Parameters | Lipid Profile | ||
|---|---|---|---|
| Normal Value n = 557 | Hyperlipidemia n = 49 | p Value | |
| Age (years) | 25.0 (22.0–30.0) | 28.0 (24.0–34.0) | <0.013 |
| BMI (kg/m2) | 22.5 (20.1–27.2) | 31.1 (25.5–35.2) | <0.001 |
| WHR | 0.8 (0.8–0.9) | 0.9 (0.9–1.0) | <0.001 |
| Glucose (mg/dL) | 89.0 (85.0–93.0) | 91.0 (88.0–95.0) | >0.05 |
| Insulin (mU/mL) | 6.7 (4.8–10.7) | 12.9 (8.1–15.7) | >0.05 |
| Glucose after OGTT | 100.0 (85.0–117.0) | 121.0 (98.0–148.0) | >0.05 |
| Insulin after OGTT | 35.1 (21.9–57.5) | 79.1 (39.8–114.0) | >0.05 |
| LH (lU/L) | 6.4 (4.4–9.5) | 6.6 (4.1–10.2) | >0.05 |
| FSH (lU/L) | 6.1 (5.0–7.2) | 5.7 (5.1–6.8) | >0.05 |
| LH/FSH | 1.0 (0.7–1.5) | 1.1 (0.8–1.5) | >0.05 |
| DHEA-S (µg/mL) | 291.6 (211.2–376.2) | 297.5 (221.4–352.3) | >0.05 |
| SHBG (nmol/L) | 57.1 (36.5–82.1) | 38.5 (23.7–52.6) | <0.001 |
| TT (ng/mL) | 0.3 (0.2–0.5) | 0.4 (0.2–0.6) | 0.045 |
| FT (pg/mL) | 1.4 (0.9–2.2) | 2.0 (0.8–3.0) | 0.003 |
| FAI | 0.6 (0.3–1.1) | 1.2 (0.7–1.7) | 0.018 |
| AD (ng/mL) | 2.8 (1.9–3.8) | 3.7 (2.7–4.7) | 0.009 |
| 17-β-E2 (pg/mL) | 33.0 (23.8–45.8) | 32.5 (21.3–49.1) | >0.05 |
| 17α-OHP (nmol/L) | 1.6 (1.2–2.0) | 1.6 (1.2–2.0) | >0.05 |
| Cortisol (µg/dL) | 13.6 (11.5–16.1) | 14.8 (12.3–17.4) | 0.022 |
| Covariate | HDL-C (mg/dL) | TG (mg/dL) |
|---|---|---|
| Whole group of women with PCOS | ||
| Glucose (mg/dL) | β = −0.36; p = 0.014 | NS |
| Insulin (mU/mL) | NS | β = 0.49; p < 0.001 |
| Insulin after OGTT | NS | β = 0.27; p = 0.046 |
| FSH (lU/L) | β = 0.09; p = 0.032 | NS |
| SHBG (nmol/L) | β = 0.33; p < 0.001 | β = −0.29; p < 0.001 |
| TT (ng/mL) | β = −0.20; p < 0.001 | β = 0.17; p < 0.001 |
| FT (pg/mL) | β = −0.18; p < 0.001 | β = 0.19; p < 0.001 |
| FAI | β = −0.37; p < 0.001 | β = 0.38; p < 0.001 |
| AD (ng/mL) | β = −0.10; p = 0.015 | β = 0.10; p = 0.018 |
| Phenotype 1 of PCOS | ||
| Insulin after OGTT | β = −0.30; p < 0.001 | NS |
| LH (lU/L) | β = 0.19; p = 0.002 | NS |
| FSH (lU/L) | β = 0.16; p = 0.011 | β = −0.17; p = 0.011 |
| LH/FSH | β = 0.15; p = 0.002 | NS |
| SHBG (nmol/L) | β = 0.26; p < 0.001 | β = −0.26; p < 0.001 |
| TT (ng/mL) | β = −0.15; p = 0.016 | β = 0.18; p = 0.004 |
| FT (pg/mL) | β = −0.13; p = 0.047 | β = 0.19; p = 0.003 |
| FAI | β = −0.38; p < 0.001 | β = 0.39; p < 0.001 |
| 17α-OHP (nmol/L) | NS | β = −0.16; p = 0.010 |
| Cortisol (µg/dL) | β = 0.19; p = 0.003 | NS |
| Whole Group of PCOS | β Value | Summarized Multiple Regression Analysis | |
|---|---|---|---|
| SHBG (nmol/L) | HDL-C (mg/dL) | β = 0.25; p < 0.001 | R = 0.37; R2 = 0.14; Adjusted R2 = 0.13; F = 46.5; p < 0.001 |
| TG (mg/dL) | β = −0.18; p < 0.001 | ||
| FAI | HDL-C (mg/dL) | β = −0.25; p < 0.001 | R = 0.44; R2 = 0.20; Adjusted R2 = 0.20; F = 71.26; p < 0.001 |
| TG (mg/dL) | β = 0.28; p < 0.001 | ||
| Phenotype 1 of PCOS | β Value | Summarized Multiple Regression Analysis | |
| SHBG (nmol/L) | HDL-C (mg/dL) | β = 0.18; p = 0.010 | R = 0.30; R2 = 0.09; Adjusted R2 = 0.08; F = 12.19; p < 0.001 |
| TG (mg/dL) | β = −0.18; p = 0.010 | ||
| FAI | HDL-C (mg/dL) | β = −0.24; p < 0.001 | R = 0.45; R2 = 0.20; Adjusted R2 = 0.19; F = 30.88; p < 0.001 |
| TG (mg/dL) | β = 0.28; p < 0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bizoń, A.; Franik, G.; Niepsuj, J.; Czwojdzińska, M.; Leśniewski, M.; Nowak, A.; Szynkaruk-Matusiak, M.; Madej, P.; Piwowar, A. The Associations between Sex Hormones and Lipid Profiles in Serum of Women with Different Phenotypes of Polycystic Ovary Syndrome. J. Clin. Med. 2021, 10, 3941. https://doi.org/10.3390/jcm10173941
Bizoń A, Franik G, Niepsuj J, Czwojdzińska M, Leśniewski M, Nowak A, Szynkaruk-Matusiak M, Madej P, Piwowar A. The Associations between Sex Hormones and Lipid Profiles in Serum of Women with Different Phenotypes of Polycystic Ovary Syndrome. Journal of Clinical Medicine. 2021; 10(17):3941. https://doi.org/10.3390/jcm10173941
Chicago/Turabian StyleBizoń, Anna, Grzegorz Franik, Justyna Niepsuj, Marta Czwojdzińska, Marcin Leśniewski, Artur Nowak, Malwina Szynkaruk-Matusiak, Paweł Madej, and Agnieszka Piwowar. 2021. "The Associations between Sex Hormones and Lipid Profiles in Serum of Women with Different Phenotypes of Polycystic Ovary Syndrome" Journal of Clinical Medicine 10, no. 17: 3941. https://doi.org/10.3390/jcm10173941