
Investigation of the Trend of Selecting Anti-Vascular Endothelial Growth Factor Agents for the Initial Treatment of Neovascular Age-Related Macular Degeneration and Polypoidal Choroidal Vasculopathy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients, Examinations, and Treatment
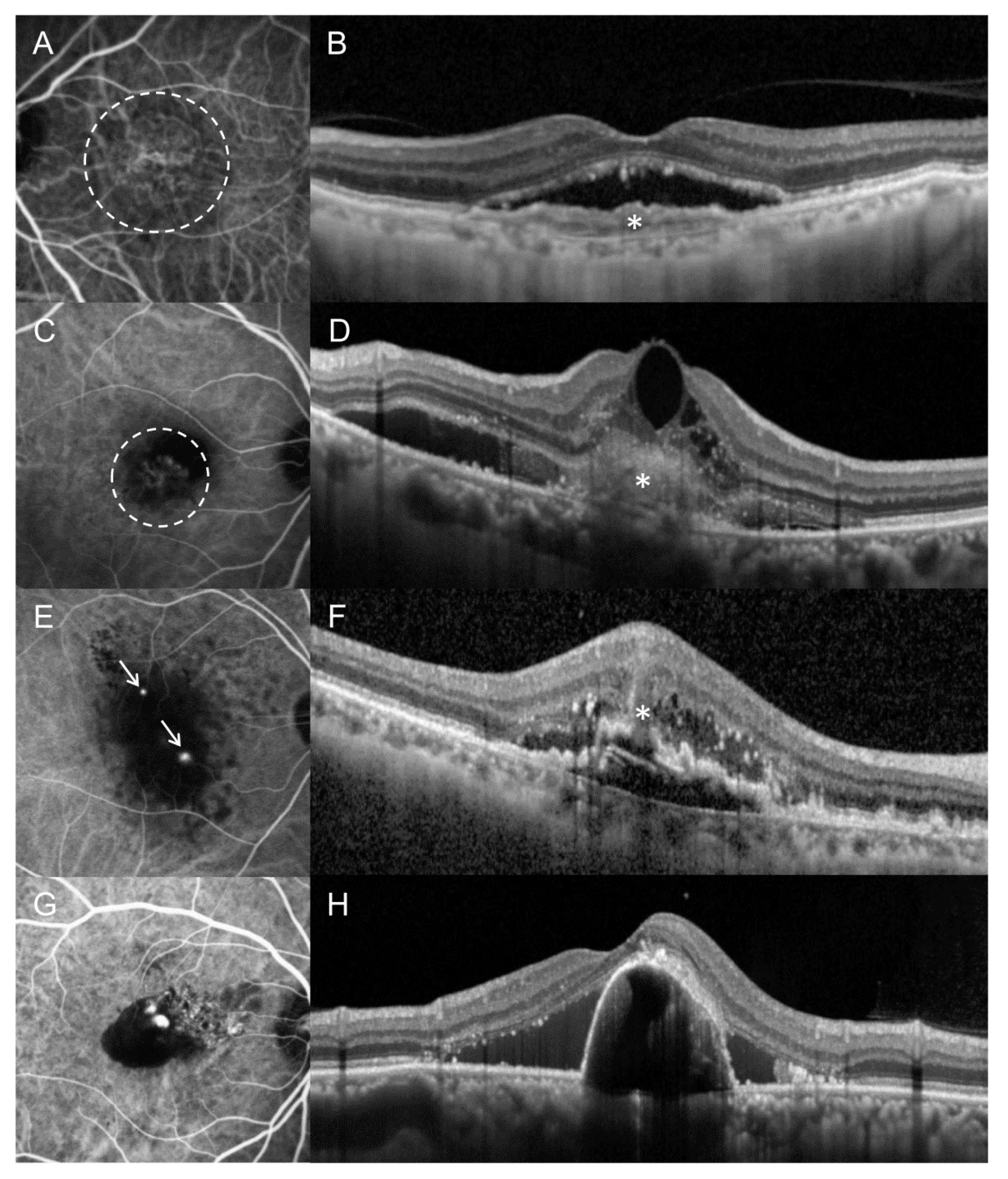
2.2. Classification of Subtypes of MNV
2.3. Result Analyses
2.4. Statistical Analyses
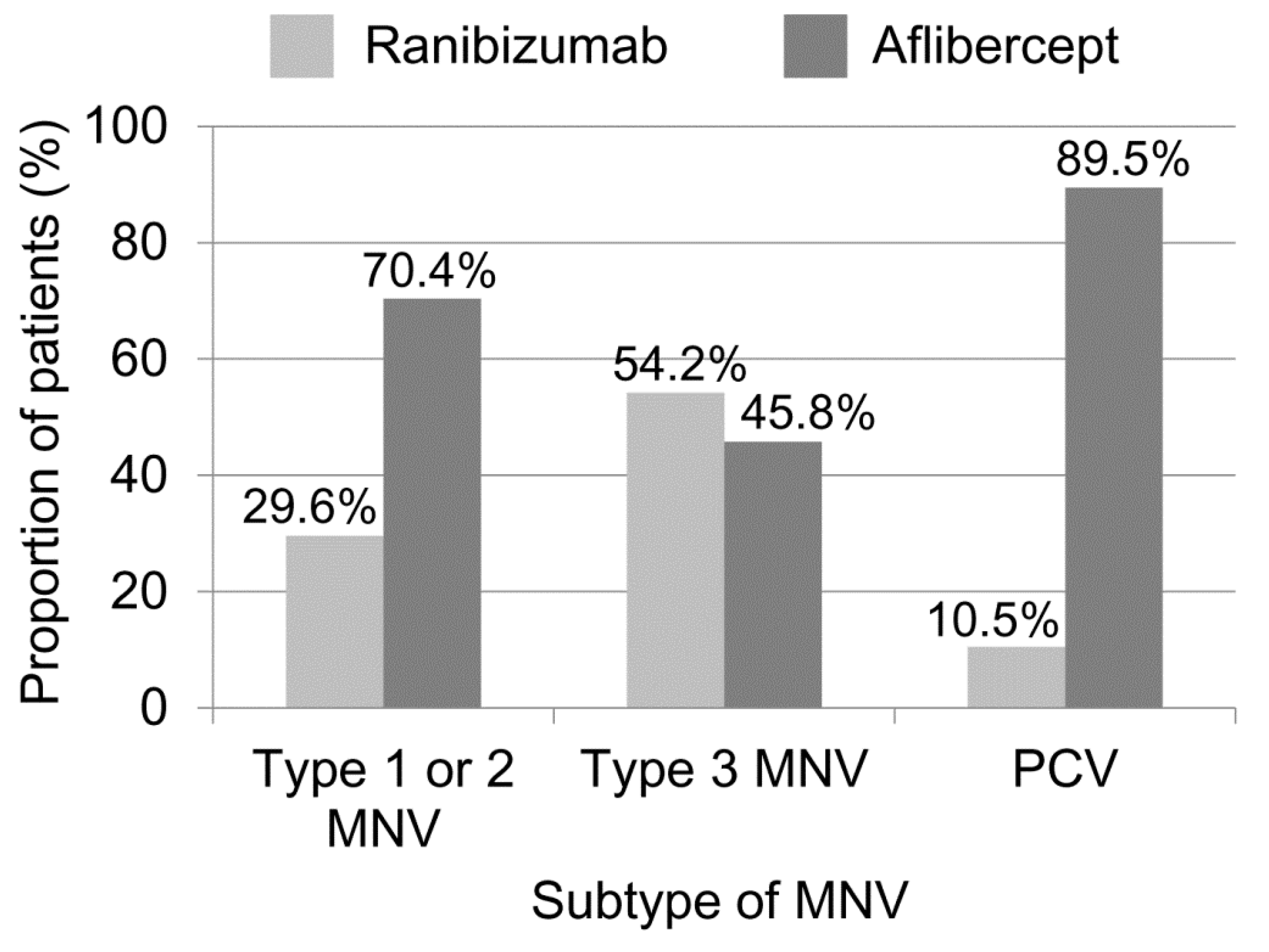
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [Green Version]
- Dansingani, K.K.; Gal-Or, O.; Sadda, S.R.; Yannuzzi, L.A.; Freund, K.B. Understanding aneurysmal type 1 neovascularization (polypoidal choroidal vasculopathy): A lesson in the taxonomy of ‘expanded spectra’—A review. Clin. Exp. Ophthalmol. 2018, 46, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.M.; Lai, T.Y.; Ruamviboonsuk, P.; Chen, S.J.; Chen, Y.; Freund, K.B.; Gomi, F.; Koh, A.H.; Lee, W.K.; Wong, T.Y. Polypoidal Choroidal Vasculopathy: Definition, Pathogenesis, Diagnosis, and Management. Ophthalmology 2018, 125, 708–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, C.M.G.; Lai, T.Y.; Ruamviboonsuk, P.; Chen, S.J.; Chen, Y.; Freund, K.B.; Gomi, F.; Koh, A.H.; Lee, W.K.; Wong, T.Y. Aflibercept for age-related macular degeneration: A game-changer or quiet addition? Am. J. Ophthalmol. 2012, 154, 222–226. [Google Scholar]
- Chhablani, J.; Shaikh, A.; Goud, A.; Kawasaki, R.; Kwon, O.W.; Chang, A.; Lam, D.; Das, T. Asia-Pacific Technology and Trend Survey 2016–2017. Asia Pac. J. Ophthalmol. 2019, 8, 43–54. [Google Scholar]
- Barthelmes, D.; Nguyen, V.; Walton, R.; Gillies, M.C.; Daien, V. A pharmacoepidemiologic study of ranibizumab and aflibercept use 2013-2016. The Fight Retinal Blindness! Project. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 1839–1846. [Google Scholar] [CrossRef]
- Nagiel, A.; Sarraf, D.; Sadda, S.R.; Spaide, R.F.; Jung, J.J.; Bhavsar, K.V.; Ameri, H.; Querques, G.; Freund, K.B. Type 3 neovascularization: Evolution, association with pigment epithelial detachment, and treatment response as revealed by spectral domain optical coherence tomography. Retina 2015, 35, 638–647. [Google Scholar] [CrossRef] [PubMed]
- Holladay, J.T. Visual acuity measurements. J. Cataract Refract. Surg. 2004, 30, 287–290. [Google Scholar] [CrossRef]
- Spaide, R.F.; Yannuzzi, L.A.; Slakter, J.S.; Sorenson, J.; Orlach, D.A. Indocyanine green videoangiography of idiopathic polypoidal choroidal vasculopathy. Retina 1995, 15, 100–110. [Google Scholar] [CrossRef]
- Cheung, C.M.; Yang, E.; Lee, W.K.; Lee, G.K.; Mathur, R.; Cheng, J.; Wong, D.; Wong, T.Y.; Lai, T.Y. The natural history of polypoidal choroidal vasculopathy: A multi-center series of untreated Asian patients. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 2075–2085. [Google Scholar] [CrossRef]
- Chung, S.E.; Kang, S.W.; Lee, J.H.; Kim, Y.T. Choroidal thickness in polypoidal choroidal vasculopathy and exudative age-related macular degeneration. Ophthalmology 2011, 118, 840–845. [Google Scholar] [CrossRef]
- Kim, J.H.; Chang, Y.S.; Kim, J.W.; Kim, C.G.; Lee, D.W. Age-related differences in the prevalence of subtypes of Neovascular age-related macular degeneration in the first diagnosed eye. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.J.; Kim, K.M.; Kim, H.S.; Han, J.I.; Kim, C.G.; Lee, T.G.; Kim, J.W. Intravitreal Aflibercept and Ranibizumab Injections for Polypoidal Choroidal Vasculopathy. Am. J. Ophthalmol. 2016, 165, 1–6. [Google Scholar] [CrossRef]
- Yamamoto, A.; Okada, A.A.; Kano, M.; Koizumi, H.; Saito, M.; Maruko, I.; Sekiryu, T.; Iida, T. One-Year Results of Intravitreal Aflibercept for Polypoidal Choroidal Vasculopathy. Ophthalmology 2015, 122, 1866–1872. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.; Kano, M.; Itagaki, K.; Oguchi, Y.; Sekiryu, T. Switching to intravitreal aflibercept injection for polypoidal choroidal vasculopathy refractory to ranibizumab. Retina 2014, 34, 2192–2201. [Google Scholar] [CrossRef]
- Kawashima, Y.; Oishi, A.; Tsujikawa, A.; Yamashiro, K.; Miyake, M.; Ueda-Arakawa, N.; Yoshikawa, M.; Takahashi, A.; Yoshimura, N. Effects of aflibercept for ranibizumab-resistant neovascular age-related macular degeneration and polypoidal choroidal vasculopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 1471–1477. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, T.G.; Chang, Y.S.; Kim, C.G.; Cho, S.W. Short-term choroidal thickness changes in patients treated with either ranibizumab or aflibercept: A comparative study. Br. J. Ophthalmol. 2016, 100, 1634–1639. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.; Ogura, Y.; Lee, W.K.; Iida, T.; Chen, S.J.; Mitchell, P.; Cheung, C.M.; Zhang, Z.; Leal, S.; Ishibashi, T. Efficacy and Safety of Intravitreal Aflibercept for Polypoidal Choroidal Vasculopathy: Two-Year Results of the Aflibercept in Polypoidal Choroidal Vasculopathy Study. Am. J. Ophthalmol. 2019, 204, 80–89. [Google Scholar] [CrossRef]
- Yannuzzi, L.A.; Negrão, S.; Tomohiro, I.I.; Carvalho, C.; Rodriguez-Coleman, H.; Slakter, J.; Freund, K.B.; Sorenson, J.; Orlock, D.; Borodoker, N. Retinal angiomatous proliferation in age-related macular degeneration. Retina 2001, 21, 416–434. [Google Scholar] [CrossRef]
- Freund, K.B.; Ho, I.V.; Barbazetto, I.A.; Koizumi, H.; Laud, K.; Ferrara, D.; Matsumoto, Y.; Sorenson, J.A.; Yannuzzi, L. Type 3 neovascularization: The expanded spectrum of retinal angiomatous proliferation. Retina 2008, 28, 201–211. [Google Scholar] [CrossRef]
- Daniel, E.; Shaffer, J.; Ying, G.S.; Grunwald, J.E.; Martin, D.F.; Jaffe, G.J.; Maguire, M.G. Outcomes in Eyes with Retinal Angiomatous Proliferation in the Comparison of Age-Related Macular Degeneration Treatments Trials (CATT). Ophthalmology 2016, 123, 609–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Kim, J.W.; Kim, C.G.; Lee, D.W. Long-Term Treatment Outcomes in Type 3 Neovascularization: Focus on the Difference in Outcomes between Geographic Atrophy and Fibrotic Scarring. J. Clin. Med. 2020, 9, 1145. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, J.W.; Kim, C.G.; Lee, D.W. Long-term Changes in Choroidal Thickness in Eyes with Type 3 Macular Neovascularization. Retina 2021, 41, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.; Lee, J.H.; Kim, J.Y.; Kim, N.H.; Lee, W.K. Geographic Atrophy and Activity of Neovascularization in Retinal Angiomatous Proliferation. Investig. Ophthalmol. Vis. Sci. 2016, 57, 1500–1505. [Google Scholar] [CrossRef] [Green Version]
- Gillies, M.C.; Hunyor, A.P.; Arnold, J.J.; Guymer, R.H.; Wolf, S.; Pecheur, F.L.; Munk, M.R.; McAllister, I.L. Macular Atrophy in Neovascular Age-Related Macular Degeneration: A Randomized Clinical Trial Comparing Ranibizumab and Aflibercept (RIVAL Study). Ophthalmology 2020, 127, 198–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, H.J.; Hwang, H.J.; Kim, H.S.; Han, J.I.; Lee, D.W.; Kim, J.W. Intravitreal Aflibercept and Ranibizumab Injections for Type 3 Neovascularization. Retina 2018, 38, 2150–2158. [Google Scholar] [CrossRef] [PubMed]
- Avery, R.L.; Castellarin, A.A.; Steinle, N.C.; Dhoot, D.S.; Pieramici, D.J.; See, R.; Couvillion, S.; Ma’an, A.N.; Rabena, M.D.; Le, K.; et al. Systemic pharmacokinetics following intravitreal injections of ranibizumab, bevacizumab or aflibercept in patients with neovascular AMD. Br. J. Ophthalmol. 2014, 98, 1636–1641. [Google Scholar] [CrossRef]
- Yashkin, A.P.; Hahn, P.; Sloan, F.A. Introducing Anti-Vascular Endothelial Growth Factor Therapies for AMD Did Not Raise Risk of Myocardial Infarction, Stroke, and Death. Ophthalmology 2016, 123, 2225–2231. [Google Scholar] [CrossRef]
- Avery, R.L.; Gordon, G.M. Systemic Safety of Prolonged Monthly Anti-Vascular Endothelial Growth Factor Therapy for Diabetic Macular Edema: A Systematic Review and Meta-analysis. JAMA Ophthalmol. 2016, 134, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Avery, R.L. What is the evidence for systemic effects of intravitreal anti-VEGF agents, and should we be concerned? Br. J. Ophthalmol. 2014, 98 (Suppl. 1), i7–i10. [Google Scholar] [CrossRef]
- Beaumont, P.E.; Petocz, P.; Kang, H.K. Is there risk of stroke with aflibercept? Ophthalmology 2014, 121, e4. [Google Scholar] [CrossRef]
- Ohji, M.; Lanzetta, P.; Korobelnik, J.F.; Wojciechowski, P.; Taieb, V.; Deschaseaux, C.; Janer, D.; Tuckmantel, C. Efficacy and Treatment Burden of Intravitreal Aflibercept Versus Intravitreal Ranibizumab Treat-and-Extend Regimens at 2 Years: Network Meta-Analysis Incorporating Individual Patient Data Meta-Regression and Matching-Adjusted Indirect Comparison. Adv. Ther. 2020, 37, 2184–2198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gong, D.; Chang, J.S.; Barbany, M.; Corcostegui, B.F.; Değirmenci, M.F.; Ishikawa, H.; Mammo, Z.; Ozmert, E.; Rossi, T.; Chang, S. Comparison of United States and International Ophthalmic Drug Pricing. Ophthalmology 2019, 126, 1358–1365. [Google Scholar] [CrossRef]
- Parikh, R.; Pirakitikulr, N.; Chhablani, J.; Sakurada, Y.; Singh, R.P.; Modi, Y.S. A Multinational Comparison of Anti-Vascular Endothelial Growth Factor Use: The United States, the United Kingdom, and Asia-Pacific. Ophthalmol. Retina 2019, 3, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Coscas, G.; Yamashiro, K.; Coscas, F.; De Benedetto, U.; Tsujikawa, A.; Miyake, M.; Cheung, C.M.; Wong, T.Y.; Yoshimura, N. Comparison of exudative age-related macular degeneration subtypes in Japanese and French Patients: Multicenter diagnosis with multimodal imaging. Am. J. Ophthalmol. 2014, 158, 309–318. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Age (years) | 71.3 ± 8.9 |
| Sex (male: female) | 255 (60.7%): 165 (39.3%) |
| Diabetes mellitus | 89 (21.2%) |
| Hypertension | 200 (47.6%) |
| Type of MNV | |
| Type 1 or 2 MNV | 162 (38.6%) |
| Type 3 MNV | 48 (11.4%) |
| Polypoidal choroidal vasculopathy | 210 (50.0%) |
| Lens status | |
| Phakic | 287 (68.3%) |
| Pseudophakic | 133 (31.7%) |
| Best-corrected visual acuity (logMAR) | 0.62 ± 0.53 |
| Type of anti-VEGF agent | |
| Ranibizumab | 96 (22.9%) |
| Aflibercept | 324 (77.1%) |
| Parameters | Ranibizumab Group (n = 96) | Aflibercept Group (n = 324) | p Value |
|---|---|---|---|
| Age (years) | 74.3 ± 8.4 | 70.4 ± 8.8 | <0.001 * |
| Sex (men: women) | 37 (38.5%): 59 (61.5%) | 218 (67.3%): 106 (32.7%) | <0.001 † |
| Diabetes mellitus | 22 (22.9%) | 67 (20.7%) | 0.637 † |
| Hypertension | 48 (50.0%) | 152 (46.9%) | 0.595 † |
| Type of MNV | <0.001 † | ||
| Type 1 or 2 MNV | 48 (50.0%) | 114 (35.2%) | |
| Type 3 MNV | 26 (27.1%) | 22 (6.8%) | |
| Polypoidal choroidal vasculopathy | 22 (22.9%) | 188 (58.0%) | |
| Lens status | 0.016 † | ||
| Phakic | 56 (58.3%) | 231 (71.3%) | |
| Pseudophakic | 40 (41.7%) | 93 (28.7%) | |
| Best-corrected visual acuity (logMAR) | 0.69 ± 0.52 | 0.60 ± 0.53 | 0.055 ‡ |
| Characteristics | Type 1 or 2 MNV (n = 162) | Type 3 MNV (n = 48) | PCV (n = 210) | p Value |
|---|---|---|---|---|
| Age (years) | 72.5 ± 8.9 | 76.6 ± 6.6 | 69.2 ± 8.6 | <0.001 * |
| Sex (male: female) | 92 (56.8%): 70 (43.2%) | 6 (12.5%): 42 (87.5%) | 157 (74.8%): 53 (25.2%) | <0.001 † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-H.; Kim, J.-W.; Kim, C.-G. Investigation of the Trend of Selecting Anti-Vascular Endothelial Growth Factor Agents for the Initial Treatment of Neovascular Age-Related Macular Degeneration and Polypoidal Choroidal Vasculopathy. J. Clin. Med. 2021, 10, 3580. https://doi.org/10.3390/jcm10163580
Kim J-H, Kim J-W, Kim C-G. Investigation of the Trend of Selecting Anti-Vascular Endothelial Growth Factor Agents for the Initial Treatment of Neovascular Age-Related Macular Degeneration and Polypoidal Choroidal Vasculopathy. Journal of Clinical Medicine. 2021; 10(16):3580. https://doi.org/10.3390/jcm10163580
Chicago/Turabian StyleKim, Jae-Hui, Jong-Woo Kim, and Chul-Gu Kim. 2021. "Investigation of the Trend of Selecting Anti-Vascular Endothelial Growth Factor Agents for the Initial Treatment of Neovascular Age-Related Macular Degeneration and Polypoidal Choroidal Vasculopathy" Journal of Clinical Medicine 10, no. 16: 3580. https://doi.org/10.3390/jcm10163580