
Combination Therapy for Neuropathic Pain: A Review of Recent Evidence


Abstract
:1. Introduction
2. Materials and Methods
2.1. Criteria for Study Selection
2.2. Types of Studies
2.3. Participants
2.4. Interventions
2.5. Outcomes
2.5.1. Primary Outcomes
2.5.2. Secondary Outcomes
2.6. Search Methods
- PubMed®. Search keywords: (“neuropathic pain” AND “combination”). The timeline was limited to articles published from 1 January 2012 to 3 March 2021. Language filter: English. The last search was performed on 3 March 2021.
- Google Scholar. Search keywords: (“neuropathic pain” AND “combination therapy”). The timeline was limited to articles published from 2012 to 2021. Language filter: English. The last search was performed on 15 March 2021.
- Web of Science. Search keywords: (“neuropathic pain” AND “combination therapy”). The search was performed on all databases except for the zoological one. The timeline was limited to articles published from 2012 to 2021. Filters were applied to exclude review articles, case reports, editorial material, books, meetings, and letters and corrections. Language filter: English. The last search was performed on 30 April 2021.
- SCOPUS. Search keywords: (“neuropathic pain” AND combination) in the title, abstract, or keywords. The timeline was limited to publication years after 2011. Filters: document type “articles” and only English language. The last search was performed on 30 April 2021.
- We further searched ClinicalTrials.gov. Keywords: (“neuropathic pain” AND “combination therapy”). No filters were used. The last search was performed on 3 March 2021.
- We searched within the reference lists of all the included studies.
- Finally, we also checked for relevant citations within other reviews and meta-analyses published between 2012 and 2021.
2.7. Data Collection and Analysis
2.7.1. Data Extraction
- The proportion of participants with 50% pain relief (primary outcome);
- The proportion of participants with 30% pain relief (whenever 50% was not reported and even if 50% was reported);
- The proportion of drop-outs due to treatment-emergent adverse events (secondary outcome);
- The proportion of dropouts for any other reason (secondary outcome);
- The proportion of participants reporting each specific adverse effect (i.e., sedation and dizziness) with moderate or greater severity; and
- The study drugs, including the names, doses, routes of administration, and treatment durations.
2.7.2. Risk of Bias
2.7.3. Measures of Effect
2.7.4. Unit of Analysis
2.7.5. Missing Data
2.7.6. Heterogeneity
2.7.7. Groups and Subgroups
3. Results
3.1. Description of Studies
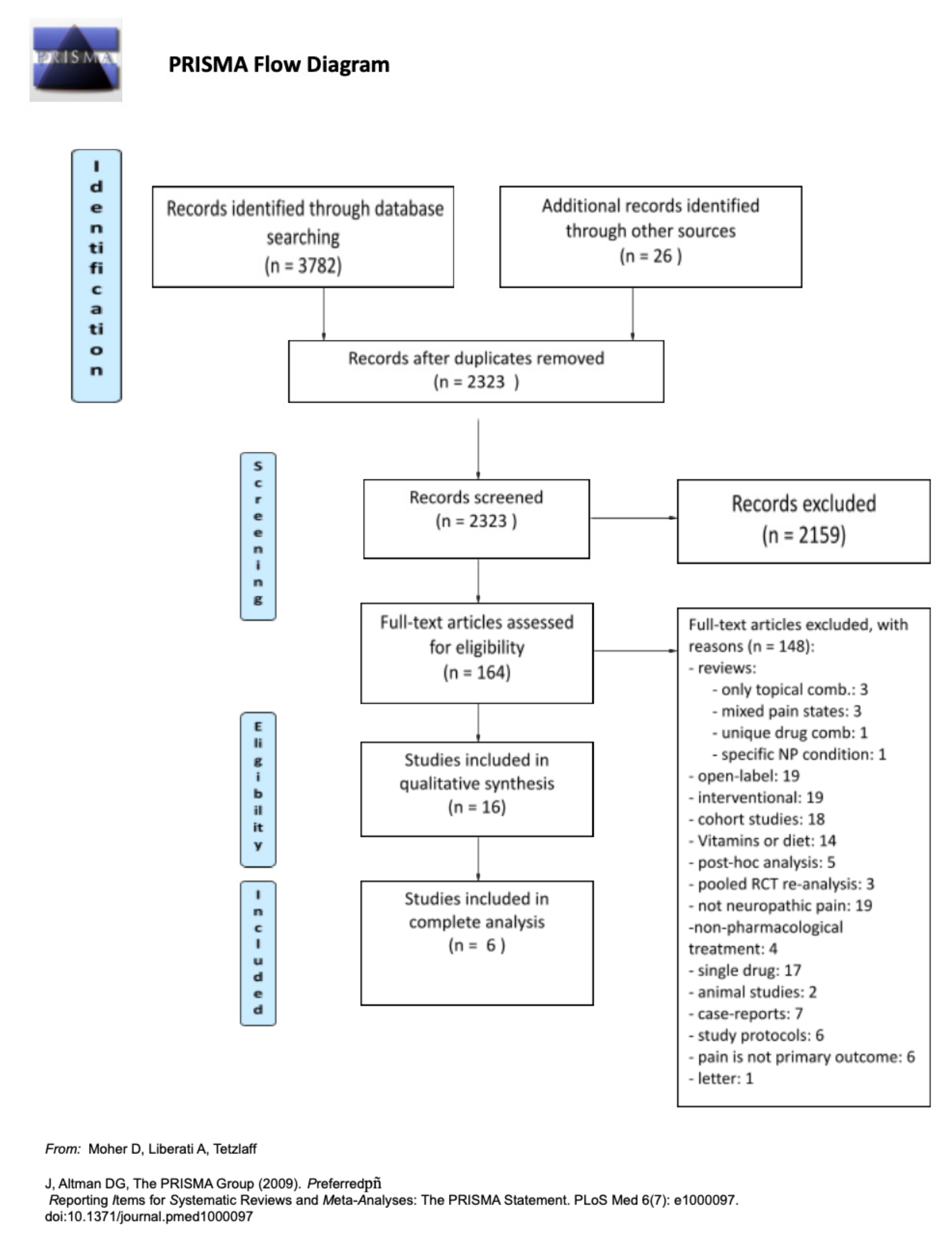
3.1.1. Study Selection
3.1.2. Study Design
3.1.3. Outcomes
3.1.4. Pain Conditions
3.1.5. Excluded Studies
3.2. Risk of Bias
3.2.1. Random Sequence Generation and Allocation Concealment (Selection Bias)
3.2.2. Blinding
3.2.3. Incomplete Outcome Data
3.2.4. Selective Reporting
3.2.5. Other Potential Sources of Bias
3.3. Effect of Interventions
4. Discussion
4.1. Main Results
4.2. Quality of Evidence
4.3. Data from the Other Unselected Studies and Articles Assessed for Eligibility
4.3.1. Cannabinoids in Combination
4.3.2. Topical Treatments in Combination
4.3.3. Gabapentinoid and Opioid Combinations
4.3.4. Antidepressant and Opioid Combinations
4.3.5. Gabapentinoids and Antidepressants in Combination
4.3.6. Other Combinations
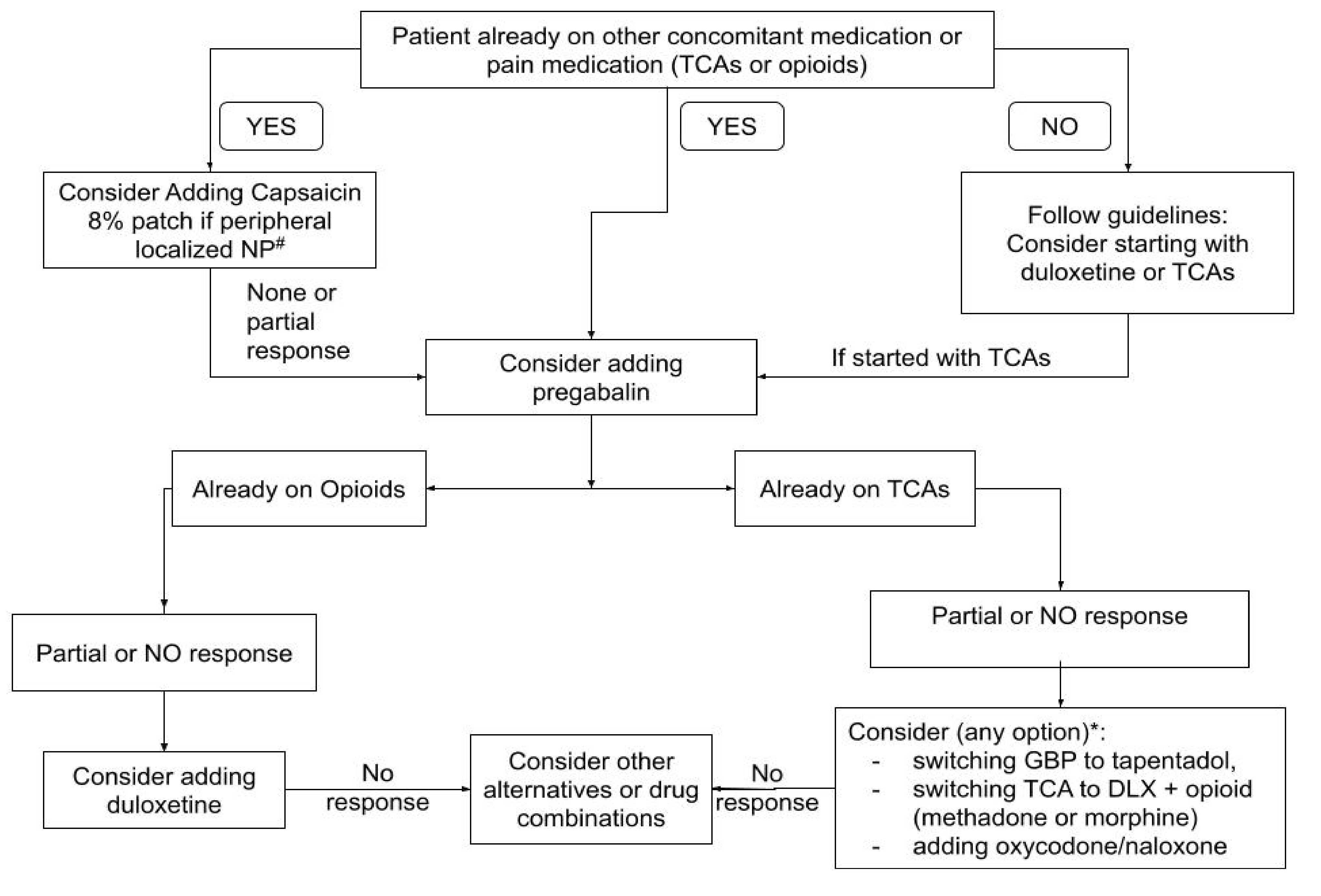
4.4. Implications for Clinical Practice
4.5. Implications for Research
4.6. Potential Biases and Limitations
4.7. Agreements or Disagreements with Other Studies or Reviews
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Treede, R.-D.; Jensen, T.S.; Campbell, J.N.; Cruccu, G.; Dostrovsky, J.O.; Griffin, J.W.; Hansson, P.; Hughes, R.; Nurmikko, T.; Serra, J. Neuropathic pain: Redefinition and a grading system for clinical and research purposes. Neurology 2007, 70, 1630–1635. [Google Scholar] [CrossRef]
- Van Hecke, O.; Austin, S.K.; Khan, R.A.; Smith, B.; Torrance, N. Neuropathic pain in the general population: A systematic review of epidemiological studies. Pain 2014, 155, 654–662. [Google Scholar] [CrossRef]
- O’Brien, T.; Breivik, H. The impact of chronic pain—European patients’ perspective over 12 months. Scand. J. Pain 2012, 3, 23–29. [Google Scholar] [CrossRef]
- Binder, A.; Baron, R. The Pharmacological Therapy of Chronic Neuropathic Pain. Dtsch. Aerzteblatt Online 2016, 113, 616–625. [Google Scholar] [CrossRef] [Green Version]
- Bates, D.; Schultheis, B.C.; Hanes, M.C.; Jolly, S.M.; Chakravarthy, K.V.; Deer, T.R.; Levy, R.M.; Hunter, C.W. A Comprehensive Algorithm for Management of Neuropathic Pain. Pain Med. 2019, 20, S2–S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pickering, G.; Marcoux, M.; Chapiro, S.; David, L.; Rat, P.; Michel, M.; Bertrand, I.; Voute, M.; Wary, B. An Algorithm for Neuropathic Pain Management in Older People. Drugs Aging 2016, 33, 575–583. [Google Scholar] [CrossRef] [Green Version]
- Cruccu, G.; Sommer, C.; Anand, P.; Attal, N.; Baron, R.; Garcia-Larrea, L.; Haanpaa, M.; Jensen, T.S.; Serra, J.; Treede, R.-D. EFNS guidelines on neuropathic pain assessment: Revised 2009. Eur. J. Neurol. 2010, 17, 1010–1018. [Google Scholar] [CrossRef] [PubMed]
- Finnerup, N.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Finnerup, N.B.; Haroutounian, S.; Kamerman, P.; Baron, R.; Bennett, D.; Bouhassira, D.; Cruccu, G.; Freeman, R.; Hansson, P.; Nurmikko, T.; et al. Neuropathic pain: An updated grading system for research and clinical practice. Pain 2016, 157, 1599–1606. [Google Scholar] [CrossRef] [Green Version]
- Finnerup, N.B.; Haroutounian, S.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpaa, M.; Jensen, T.S.; Kamerman, P.R.; McNicol, E.; Moore, A.; et al. Neuropathic pain clinical trials: Factors associated with decreases in estimated drug efficacy. Pain 2018, 159, 2339–2346. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER). Guidance for Industry Analgesic Indications: Developing Drug and Biological Products. DRAFT GUIDANCE. Feb-ruary 2014. 5150dft.doc. Available online: https://www.fdanews.com/ext/resources/files/02/02-05-14-Analgesic.pdf (accessed on 6 May 2021).
- Committee for Medicinal Products for Human Use (CHMP). Guideline on Clinical Medicinal Products Intended for the Treatment of Neuropathic Pain. London, 24 January 2007. Doc. Ref. CPMP/EWP/252/03 Rev. 1. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-medicinal-products-intended-treatment-neuropathic-pain_en.pdf (accessed on 1 August 2021).
- Committee for Medicinal Products for Human Use (CHMP). Guideline on the Clinical Development of Medicinal Products Intended for the Treatment of Pain. 15 December 2016 EMA/CHMP/970057/201. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-development-medicinal-products-intended-treatment-pain-first-version_en.pdf (accessed on 1 August 2021).
- Gewandter, J.S.; McDermott, M.P.; Mbowe, O.; Edwards, R.R.; Katz, N.P.; Turk, D.C.; Dworkin, R.H. Navigating trials of personalized pain treatments: We’re going to need a bigger boat. Pain 2019, 160, 1235–1239. [Google Scholar] [CrossRef]
- Arakawa, A.; Kaneko, M.; Narukawa, M. An Investigation of Factors Contributing to Higher Levels of Placebo Response in Clinical Trials in Neuropathic Pain: A Systematic Review and Meta-Analysis. Clin. Drug Investig. 2015, 35, 67–81. [Google Scholar] [CrossRef]
- Moisset, X.; Bouhassira, D.; Couturier, J.A.; Alchaar, H.; Conradi, S.; Delmotte, M.; Lanteri-Minet, M.; Lefaucheur, J.; Mick, G.; Piano, V.; et al. Pharmacological and non-pharmacological treatments for neuropathic pain: Systematic review and French recommendations. Rev. Neurol. 2020, 176, 325–352. [Google Scholar] [CrossRef]
- Mu, A.; Weinberg, E.; Moulin, D.E.; Clarke, H. Pharmacologic management of chronic neuropathic pain: Review of the Canadian Pain Society consensus statement. Can. Fam. Phys. 2017, 63, 844–852. [Google Scholar]
- De Oliveira, R.A.A.; Baptista, A.F.; Sá, K.N.; Barbosa, L.M.; Nascimento, O.J.M.D.; Listik, C.; Moisset, X.; Teixeira, M.J.; De Andrade, D.C. Pharmacological treatment of central neuropathic pain: Consensus of the Brazilian Academy of Neurology. Arq. De Neuro-Psiquiatr. 2020, 78, 741–752. [Google Scholar] [CrossRef]
- Holbech, J.V.; Jung, A.; Jonsson, T.; Wanning, M.; Bredahl, C.; Bach, F. Combination treatment of neuropathic pain: Danish expert recommendations based on a Delphi process. J. Pain Res. 2017, 10, 1467–1475. [Google Scholar] [CrossRef] [Green Version]
- Baron, R.; Gierthmühlen, J. Neuropathic Pain. Semin. Neurol. 2016, 36, 462–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forstenpointner, J.; Otto, J.; Baron, R. Individualized neuropathic pain therapy based on phenotyping: Are we there yet? Pain 2018, 159, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.; Maier, C.; Attal, N.; Binder, A.; Bouhassira, D.; Cruccu, G.; Finnerup, N.B.; Haanpää, M.; Hansson, P.; Hüllemann, P.; et al. Peripheral neuropathic pain: A mechanism-related organizing principle based on sensory profiles. Pain 2017, 158, 261–272. [Google Scholar] [CrossRef] [Green Version]
- Gilron, I.; Jensen, T.S.; Dickenson, A.H. Combination pharmacotherapy for management of chronic pain: From bench to bedside. Lancet Neurol. 2013, 12, 1084–1095. [Google Scholar] [CrossRef]
- Eisenberg, E.; Suzan, E. Drug Combinations in the Treatment of Neuropathic Pain. Curr. Pain Headache Rep. 2014, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tesfaye, S.; Vileikyte, L.; Rayman, G.; Sindrup, S.; Perkins, B.A.; Baconja, M.; Vinik, A.I.; Boulton, A.J.M.; Toronto Expert Panel on Diabetic Neuropathy. Painful diabetic peripheral neuropathy: Consensus recommendations on diagnosis, assessment and management. Diabetes/Metab. Res. Rev. 2011, 27, 629–638. [Google Scholar] [CrossRef]
- Neuropathic Pain in Adults: Pharmacological Management in Non-Specialist Settings. Clinical Guideline [CG173] Published: 20 November 2013 Last Updated: 22 September 2020. Available online: https://www.nice.org.uk/guidance/cg173 (accessed on 11 August 2021).
- Gilron, I.; Wiffen, P.J.; Moore, R.A. Combination pharmacotherapy for the treatment of neuropathic pain in adults. Cochrane Database Syst. Rev. 2011, 7, CD008943. [Google Scholar] [CrossRef]
- Gilron, I.; Max, M.B. Combination pharmacotherapy for neuropathic pain: Current evidence and future directions. Expert Rev. Neurother. 2005, 5, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in random-ised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, R.; Rao, H.K.; Singh, T.G. Comparison of safety and efficacy of pregabalin, duloxetine and their combination with epalrestat in diabetic neuropathy: A prospective, doubleblind, randomized, controlled trial. J. Appl. Pharm. Sci. 2021, 11 (Suppl. 1), 71–79. [Google Scholar]
- Pickering, G.; Pereira, B.; Morel, V.; Corriger, A.; Giron, F.; Marcaillou, F.; Bidar-Beauvallot, A.; Chandeze, E.; Lambert, C.; Bernard, L.; et al. Ketamine and Magnesium for Refractory Neuropathic Pain. Anesthesiology 2020, 133, 154–164. [Google Scholar] [CrossRef]
- Matsuoka, H.; Iwase, S.; Miyaji, T.; Kawaguchi, T.; Ariyoshi, K.; Oyamada, S.; Satomi, E.; Ishiki, H.; Hasuo, H.; Sakuma, H.; et al. Additive Duloxetine for Cancer-Related Neuropathic Pain Nonresponsive or Intolerant to Opioid-Pregabalin Therapy: A Randomized Controlled Trial (JORTC-PAL08). J. Pain Symptom Manag. 2019, 58, 645–653. [Google Scholar] [CrossRef] [Green Version]
- Dou, Z.; Jiang, Z.; Zhong, J. Efficacy and safety of pregabalin in patients with neuropathic cancer pain undergoing morphine therapy. Asia-Pac. J. Clin. Oncol. 2017, 13, e57–e64. [Google Scholar] [CrossRef]
- Rigo, F.K.; Trevisan, G.; Godoy, M.C.; Rossato, M.F.; Dalmolin, G.D.; Silva, M.A.; Menezes, M.S.; Caumo, W.; Ferreira, J. Management of Neuropathic Chronic Pain with Methadone Combined with Ketamine: A Randomized, Double Blind, Active-Controlled Clinical Trial. Pain Phys. 2017, 20, 207–215. [Google Scholar]
- Kim, H.-J.; Kim, J.H.; Park, Y.S.; Suk, K.-S.; Lee, J.H.; Park, M.S.; Moon, S.-H. Comparative study of the efficacy of limaprost and pregabalin as single agents and in combination for the treatment of lumbar spinal stenosis: A prospective, double-blind, randomized controlled non-inferiority trial. Spine J. 2016, 16, 756–763. [Google Scholar] [CrossRef]
- Baron, R.; Martin-Mola, E.; Müller, M.; Dubois, C.; Falke, D.; Steigerwald, I. Effectiveness and Safety of Tapentadol Prolonged Release (PR) Versus a Combination of Tapentadol PR and Pregabalin for the Management of Severe, Chronic Low Back Pain With a Neuropathic Component: A Randomized, Double-blind, Phase 3b Study. Pain Pract. 2014, 15, 455–470. [Google Scholar] [CrossRef]
- Gilron, I.; Tu, D.; Holden, R.R.; Jackson, A.; DuMerton-Shore, D. Combination of morphine with nortriptyline for neuropathic pain. Pain 2015, 156, 1440–1448. [Google Scholar] [CrossRef]
- Holbech, J.V.; Bach, F.; Finnerup, N.; Brosen, K.; Jensen, T.S.; Sindrup, S. Imipramine and pregabalin combination for painful polyneuropathy. Pain 2015, 156, 958–966. [Google Scholar] [CrossRef]
- Turcotte, D.; Doupe, M.; Torabi, M.; Gomori, A.; Ethans, K.; Esfahani, F.; Galloway, K.; Namaka, M. Nabilone as an Adjunctive to Gabapentin for Multiple Sclerosis-Induced Neuropathic Pain: A Randomized Controlled Trial. Pain Med. 2015, 16, 149–159. [Google Scholar] [CrossRef] [Green Version]
- Garassino, M.C.; Piva, S.; La Verde, N.; Spagnoletti, I.; Iorno, V.; Carbone, C.; Febbraro, A.; Bianchi, A.; Bramati, A.; Moretti, A.; et al. Randomised Phase II Trial (NCT00637975) Evaluating Activity and Toxicity of Two Different Escalating Strategies for Pregabalin and Oxycodone Combination Therapy for Neuropathic Pain in Cancer Patients. PLoS ONE 2013, 8, e59981. [Google Scholar] [CrossRef]
- Harrison, T.; Miyahara, S.; Lee, A.; Evans, S.; Bastow, B.; Simpson, D.; Gilron, I.; Dworkin, R.; Daar, E.S.; Wieclaw, L.; et al. Experience and Challenges Presented by a Multicenter Crossover Study of Combination Analgesic Therapy for the Treatment of Painful HIV-Associated Polyneuropathies. Pain Med. 2013, 14, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Tesfaye, S.; Wilhelm, S.; Lledo, A.; Schacht, A.; Tölle, T.; Bouhassira, D.; Cruccu, G.; Skljarevski, V.; Freynhagen, R. Duloxetine and pregabalin: High-dose monotherapy or their combination? The “COMBO-DN study”—A multinational, randomized, double-blind, parallel-group study in patients with diabetic peripheral neuropathic pain. Pain 2013, 154, 2616–2625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langford, R.M.; Mares, J.; Novotna, A.; Vachova, M.; Novakova, I.; Notcutt, W.; Ratcliffe, S. A double-blind, randomized, placebo-controlled, parallel-group study of THC/CBD oromucosal spray in combination with the existing treatment regimen, in the relief of central neuropathic pain in patients with multiple sclerosis. J. Neurol. 2013, 260, 984–997. [Google Scholar] [CrossRef] [PubMed]
- Irving, G.A.; Backonja, M.; Rauck, R.; Webster, L.R.; Tobias, J.; Vanhove, G.F. NGX-4010, a Capsaicin 8% Dermal Patch, Administered Alone or in Combination With Systemic Neuropathic Pain Medications, Reduces Pain in Patients With Postherpetic Neuralgia. Clin. J. Pain 2012, 28, 101–107. [Google Scholar] [CrossRef]
- Shaibani, A.I.; Pope, L.E.; Thisted, R.; Hepner, A. Efficacy and Safety of Dextromethorphan/Quinidine at Two Dosage Levels for Diabetic Neuropathic Pain: A Double-Blind, Placebo-Controlled, Multicenter Study. Pain Med. 2012, 13, 243–254. [Google Scholar] [CrossRef] [Green Version]
- Committee for Medicinal Products for Human Use (CHMP). Guideline on the Clinical Development of Medicinal Products Intended for the Treatment of Pain. Available online: https://www.ema.europa.eu/en/clinical-development-medicinal-products-intended-treatment-pain (accessed on 23 May 2021).
- Dworkin, R.H.; Turk, D.C.; Peirce-Sandner, S.; Burke, L.B.; Farrar, J.T.; Gilron, I.; Jensen, M.P.; Katz, N.P.; Raja, S.N.; Rappaport, B.A.; et al. Considerations for improving assay sensitivity in chronic pain clinical trials: IMMPACT recommendations. Pain 2012, 153, 1148–1158. [Google Scholar] [CrossRef]
- Moore, R.; Derry, S.; Wiffen, P. Challenges in design and interpretation of chronic pain trials. Br. J. Anaesth. 2013, 111, 38–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dykukha, I.; Malessa, R.; Essner, U.; Überall, M.A. Nabiximols in Chronic Neuropathic Pain: A Meta-Analysis of Randomized Placebo-Controlled Trials. Pain Med. 2021, 22, 861–874. [Google Scholar] [CrossRef] [PubMed]
- Atwal, N.; Casey, S.L.; Mitchell, V.A.; Vaughan, C.W. THC and gabapentin interactions in a mouse neuropathic pain model. Neuropharmacology 2019, 144, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Ramírez, E.L. Treatment of acute and chronic focal neuropathic pain in cancer patients with lidocaine 5 % patches. A radiation and oncology department experience. Support. Care Cancer 2012, 21, 1329–1334. [Google Scholar] [CrossRef]
- Martini, A.; Del Balzo, G.; Schweiger, V.; Zanzotti, M.; Picelli, A.; Parolini, M.; Chinellato, E.; Tamburin, S.; Polati, E. Efficacy of lidocaine 5% medicated plaster (VERSATIS®) in patients with localized neuropathic pain poorly responsive to pharmacological therapy. Minerva Med. 2018, 109, 344–351. [Google Scholar] [CrossRef]
- Palladini, M.; Boesl, I.; Koenig, S.; Buchheister, B.; Attal, N. Lidocaine medicated plaster, an additional potential treatment option for localized post-surgical neuropathic pain: Efficacy and safety results of a randomized, placebo-controlled trial. Curr. Med. Res. Opin. 2019, 35, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Correa-Illanes, G.; Roa, R.G.; Piñeros, J.L.B.; Ferrer, F.T.; Adriasola, V.R. Retrospective analysis of 4 years of clinical experience with transdermal buprenorphine (Transtec®) in post-traumatic pain. Pain Manag. 2014, 4, 181–190. [Google Scholar] [CrossRef]
- Fulas, O.A.; Laferrière, A.; Ware, D.M.A.; Shir, Y.; Coderre, T.J. The effect of a topical combination of clonidine and pentoxifylline on post-traumatic neuropathic pain patients: Study protocol for a randomized, double-blind placebo-controlled trial. Trials 2021, 22, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Teng, L.; Zhao, L.; Zou, H. The combined analgesic effect of pregabalin and morphine in the treatment of pancreatic cancer pain, a retrospective study. Cancer Med. 2021, 10, 1738–1744. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yang, H.; Shen, C.; Luo, J. Morphine and pregabalin in the treatment of neuropathic pain. Exp. Ther. Med. 2017, 13, 1393–1397. [Google Scholar] [CrossRef] [Green Version]
- De La Calle, J.-L.; De Andrés, J.; Pérez, M.; Lopez, V. Add-on treatment with pregabalin for patients with uncontrolled neuropathic pain who have been referred to pain clinics. Clin. Drug Investig. 2014, 34, 833–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, J.-M.; Chung, C.K.; Kim, C.H.; Yang, S.H.; Choi, Y. Comparison of the use of opioids only and pregabalin add-on for the treatment of neuropathic pain in cervical myelopathy patients: A pilot trial. Sci. Rep. 2020, 10, 8120. [Google Scholar] [CrossRef] [PubMed]
- Lazzari, M.; Sabato, A.F.; Caldarulo, C.; Casali, M.; Gafforio, P.; Marcassa, C.; Leonardis, F. Effectiveness and tolerability of low-dose oral oxycodone/naloxone added to anticonvulsant therapy for noncancer neuropathic pain: An observational analysis. Curr. Med. Res. Opin. 2013, 30, 555–564. [Google Scholar] [CrossRef] [Green Version]
- Hall, G.C.; Morant, S.V.; Carroll, D.; Gabriel, Z.L.; McQuay, H.J. An observational descriptive study of the epidemiology and treatment of neuropathic pain in a UK general population. BMC Fam. Pract. 2013, 14, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curry, Z.A.; Dang, M.C.; Sima, A.P.; Abdullaziz, S.; Del Fabbro, E.G. Combination therapy with methadone and duloxetine for cancer-related pain: A retrospective study. Ann. Palliat. Med. 2021, 10, 62. [Google Scholar] [CrossRef]
- Nayak, M.K.; Kapadia, J.D.; Desai, C.K.; Desai, M.K.; Shah, B.J. An Evaluation of Efficacy and Safety of Commonly Prescribed Drugs and Effect of These Drugs on Quality of Sleep in Patients Suffering From Zoster-Associated Pain. J. Clin. Pharmacol. 2018, 58, 1406–1417. [Google Scholar] [CrossRef]
- Bril, V.; England, J.B.A.; Franklin, G.M.; Backonja, M.M.; Cohen, J.M.; Del Toro, D.; Feldman, E.; Iverson, D.J.; Perkins, B.A.; Russell, J.W.; et al. Evidence-based guideline: Treatment of painful diabetic neuropathy: Report of the American Academy of Neurology, the American Association of Neuromuscular and Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation. Neurology 2011, 76, 1758–1765. [Google Scholar] [CrossRef] [Green Version]
- Robertson, K.L.; Marshman, L.A. Gabapentin Superadded to a Pre-Existent Regime Containing Amytriptyline for Chronic Sciatica. Pain Med. 2016, 17, 2095–2099. [Google Scholar] [CrossRef] [Green Version]
- Tanenberg, R.J.; Clemow, D.B.; Giaconia, J.M.; Risser, R.C. Duloxetine Compared with Pregabalin for Diabetic Peripheral Neuropathic Pain Management in Patients with Suboptimal Pain Response to Gabapentin and Treated with or without Antidepressants: A Post Hoc Analysis. Pain Pract. 2013, 14, 640–648. [Google Scholar] [CrossRef] [PubMed]
- McKinley, E.C.; Richardson, E.J.; McGwin, G.; Zhang, J. Evaluating the effectiveness of antidepressant therapy adjuvant to gabapentin and pregabalin for treatment of SCI-related neuropathic pain. J. Spinal Cord. Med. 2018, 41, 637–644. [Google Scholar] [CrossRef]
- Tarrio, E.B.; Mateos, R.G.; Bayarri, E.Z.; Gómez, V.L.; Páramo, M.P. Effectiveness of Pregabalin as Monotherapy or Combination Therapy for Neuropathic Pain in Patients Unresponsive to Previous Treatments in a Spanish Primary Care Setting. Clin. Drug Investig. 2013, 33, 633–645. [Google Scholar] [CrossRef] [Green Version]
- Kanbayashi, Y.; Onishi, K.; Hosokawa, T. Factors predicting adverse events associated with pregabalin administered for neuropathic pain relief. Pain Res. Manag. 2014, 19, e164–e167. [Google Scholar] [CrossRef]
- Schug, S.A.; Parsons, B.; Almas, M.; Whalen, E. Effect of Concomitant Pain Medications on Response to Pregabalin in Patients with Postherpetic Neuralgia or Spinal Cord Injury-Related Neuropathic Pain. Pain Phys. 2017, 20, E53–E63. [Google Scholar] [CrossRef]
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.; et al. Neuropathic pain. Nat. Rev. Dis. Prim. 2017, 3, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Vranken, J.H. Elucidation of pathophysiology and treatment of neuropathic pain. Cent. Nerv. Syst. Agents Med. Chem. 2012, 12, 304–314. [Google Scholar] [CrossRef]
- De Santis, S.; Borghesi, C.; Ricciardi, S.; Giovannoni, D.; Fulvi, A.; Migliorino, M.R.; Marcassa, C. Analgesic effectiveness and tolerability of oral oxycodone/naloxone and pregabalin in patients with lung cancer and neuropathic pain: An observational analysis. OncoTargets Ther. 2016, 9, 4043–4052. [Google Scholar] [CrossRef] [Green Version]
- López-Cedrún, J.; Videla, S.; Burgueno, M.; Juárez, I.; Aboul-Hosn, S.; Martín-Granizo, R.; Grau, J.; Puche, M.; Gil-Diez, J.L.; Hueto, J.A.; et al. Co-crystal of Tramadol-Celecoxib in Patients with Moderate to Severe Acute Post-Surgical Oral Pain: A Dose-Finding, Randomised, Double-Blind, Placebo- and Active-Controlled, Multicentre, Phase II Trial. Drugs RD 2018, 18, 137–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blondell, R.D.; Azadfard, M.; Wisniewski, A.M. Pharmacologic therapy for acute pain. Am. Fam. Phys. 2013, 87, 23939498. [Google Scholar]
- Moore, R.A.; Derry, S.; Aldington, D.; Wiffen, P.J. Single dose oral analgesics for acute postoperative pain in adults—an overview of Cochrane reviews. Cochrane Database Syst. Rev. 2015, 2015, CD008659. [Google Scholar] [CrossRef] [PubMed]
- Hamidi, G.A.; Jafari-Sabet, M.; Abed, A.; Mesdaghinia, A.; Mahlooji, M.; Banafshe, H.R. Gabapentin enhances anti-nociceptive ef-fects of morphine on heat, cold, and mechanical hyperalgesia in a rat model of neuropathic pain. Iran J. Basic Med. Sci. 2014, 17, 753–759. [Google Scholar] [PubMed]
- Corona-Ramos, J.N.; De la O Arciniega, M.; Déciga-Campos, M.; Medina, J.R.; Domínguez-Ramírez, A.M.; Jaramillo-Morales, O.A.; Espinosa-Juarez, J.V.; López-Muñoz, F.J. The Antinociceptive Effects of Tramadol and/or Gabapentin on Rat Neuropathic Pain Induced by a Chronic Constriction Injury. Drug Dev. Res. 2016, 77, 217–226. [Google Scholar] [CrossRef]
- Miranda, H.F.; Noriega, V.; Prieto, J.C.; Zanetta, P.; Castillo, R.; Aranda, N.; Sierralta, F. Antinociceptive Interaction of Tramadol with Gabapentin in Experimental Mononeuropathic Pain. Basic Clin. Pharmacol. Toxicol. 2016, 119, 210–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zbârcea, C.E.; Ciotu, I.C.; Bild, V.; ChiriŢă, C.; Tănase, A.M.; Şeremet, O.C.; Ştefănescu, E.; Arsene, A.L.; Bastian, A.E.; Ionică, F.E.; et al. Therapeutic potential of certain drug combinations on paclitaxel-induced peripheral neuropathy in rats. Rom. J. Morphol. Embryol. 2017, 58, 507–516. [Google Scholar]
- Miranda, H.F.; Sierralta, F.; Aranda, N.; Poblete, P.; Noriega, V.; Prieto, J.C. Synergism between gabapentin-tramadol in experimental diabetic neuropathic pain. Fundam. Clin. Pharmacol. 2018, 32, 581–588. [Google Scholar] [CrossRef]
- Kazantzis, N.P.; Casey, S.L.; Seow, P.W.; Mitchell, V.A.; Vaughan, C.W. Opioid and cannabinoid synergy in a mouse neuropathic pain model. Br. J. Pharmacol. 2016, 173, 2521–2531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunduz, O.; Topuz, R.; Karadag, C.; Ulugöl, A. Analysis of the anti-allodynic effects of combination of a synthetic cannabinoid and a selective noradrenaline re-uptake inhibitor in nerve injury-induced neuropathic mice. Eur. J. Pain 2015, 20, 465–471. [Google Scholar] [CrossRef]
- Hahm, T.S.; Ahn, H.J.; Ryu, S.; Gwak, M.S.; Choi, S.J.; Kim, J.K.; Yu, J.M. Combined carbamazepine and pregabalin therapy in a rat model of neuropathic pain. Br. J. Anaesth. 2012, 109, 968–974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, T.; Hao, J.-X.; Wiesenfeld-Hallin, Z.; Xu, X.-J. Gabapentin and NMDA receptor antagonists interacts synergistically to alleviate allodynia in two rat models of neuropathic pain. Scand. J. Pain 2018, 18, 687–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Kim, Y.; Lee, J.J.S.; Im, G.; Cho, J.-Y.; Chung, J.-Y.; Yoon, S. A pharmacokinetic drug-drug interaction study between pregabalin and tramadol in healthy volunteers. Eur. J. Clin. Pharmacol. 2018, 74, 1605–1613. [Google Scholar] [CrossRef]
- Kamble, S.; Poul, B.; Udapurkar, P. Bilayer tablet of tramadol and gabapentin for combination pharmacotherapy of neuropathic pain: Development and characterization. Int. J. Appl. Pharm. 2018, 10, 100–107. [Google Scholar]
- Benavides, R.; Vsevolozhskaya, O.; Cattaneo, S.; Zaykin, D.; Brenton, A.; Parisien, M.; Verma, V.; Khoury, S.; Gilron, I.; Diatchenko, L. A functional polymorphism in the ATP-Binding Cassette B1 transporter predicts pharmacologic response to combination of nortriptyline and morphine in neuropathic pain patients. Pain 2020, 161, 619–629. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008, PMCID: PMC5833365. [Google Scholar] [CrossRef] [Green Version]
- Casale, R.; Symeonidou, Z.; Bartolo, M. Topical Treatments for Localized Neuropathic Pain. Curr Pain Headache Rep. 2017, 21, 15. [Google Scholar] [CrossRef] [Green Version]
- Guan, J.; Tanaka, S.; Kawakami, K. Anticonvulsivants in combination pharmacotherapy for treatment of neuropathic pain in cancer patients: A systematic review and meta-analysis. Clin. J. Pain. 2016, 32, 719–725. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Name | Pain Condition | RCT | Treatment Duration (Weeks) | Combination | Target Ceiling Dose or MTD per Day | Route | Sample Size RD (CS) | Control | Target Ceiling Dose or MTD per Day | Route | Sample Size RD (CS) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Langford 2013 [43] | Central neuropathic pain in patients with multiple sclerosis | DB; PARALLEL | 14 | THC/CBD + concomitant analgesic medication | 32.4/30 mg | oromucosal (spay) + oral | 167 (41) | Placebo | oromucosal (spray) + oral | 172 (156) | |
| Shaibani 2012 [45] | Diabetic neuropathic pain | DB; PARALLEL | 13 | DMQ | 90/60 mg 60/60 mg | oral oral | 131 (79) 125 (74) | Placebo | oral | 123 (89) | |
| Irving 2012 [44] | Postherpetic neuralgia | DB; PARALLEL | 12 | Capsaicin + concomitant neuropathic medication | 640 µg/cm2 | topical (skin) + oral | 597 (544) | Placebo | topical (skin) + oral | 530 (480) | |
| Tesfaye 2013 [42] | Diabetic neuropathic pain in patients who are non-responders to duloxetine or pregabalin | DB; PARALLEL | 8 | Duloxetine + Pregabalin | 60 + 300 mg | oral | 170 (141) | Duloxetine Pregabalin | 120 mg 600 mg | oral oral | 74 (?) 99 (?) |
| Holbech 2015 [38] | Painful polyneuropathy | DB; CROSSOVER | 5 | Imipramine + Pregabalin | 75 + 300 mg | oral | 18 (15)–16 (15) –15 (12)–16 (14) | Placebo Imipramine Pregabalin | 75 mg 300 mg; | oral oral oral | 19 (18)–16 (15)–15 (13) 12 (11) 18 (17)–17 (14)–14 (14)–12 (12) 18 (15)–16 (14)–14 (14)–13 (13) |
| Matsuoka 2019 [32] | Neuropathic pain in cancer patients who are non-responders to opioid–pregabalin | DB; PARALLEL | 1,5 (10 days) | Duloxetine + Opioid–Pregabalin | 40 mg + ?—300 mg | oral | 35 (34) | Placebo + Opioid- Pregabalin | ?- 300 mg | oral | 35 (33) |
| Name | Pain Condition | RCT | Treatment Duration (Weeks) | Combination | Target Ceiling Dose or MTD per Day | Route | Sample Size RD (CS) | Control | Target Ceiling Dose or MTD per Day | Route | Sample Size RD (CS) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Singh 2021 [30] | Diabetic neuropathic pain | DB; PARALLEL | 24 (6 months) | Epalrestat + pregabalin Epalrestat + duloxetine | 100 + 150 mg 100 + 60 mg | oral oral | 50? (?) 50? (?) | Pregabalin Duloxetine | 150 mg 60 mg | Oral oral | 50? (?) 50? (?) |
| Rigo 2017 [34] | Neuropathic pain in patients whose responses to neuropathic medication are poor | DB; PARALLEL | 13 (3 months) | Methadone + ketamine | 9 + 90 mg | oral | 14 (13) | Methadone Ketamine | 9 mg 90 mg | oral oral | 14 (13) 14 (11) |
| Turcotte 2015 [39] | Central neuropathic pain in patients with multiple sclerosis and treated with gabapentin | DB; PARALLEL | 9 | Nabilone + gabapentin | 2 + 1800 mg | oral | 8 (7) | Placebo + gabapentin | 1800 mg | oral oral | 7 (7) |
| Kim 2016 [35] | Lumbar spinal stenosis | DB; DD; PARALLEL | 8 | Limaprost + pregabalin | 15 µg + 225 mg | oral | 61 (43) | Limaprost Pregabalin | 15 µg 225 mg | oral oral | 61 (40) 60 (43) |
| Baron 2014 [36] | Low back pain (with a neuropathic component) in patients treated with tapentadol PR | DB; PARALLEL | 8 | Tapentadol PR + pregabalin | 300 + 300 mg | oral | 159 (133) | Tapentadol PR | 500 mg | oral | 154 (126) |
| Gilron 2015 [37] | Neuropathic pain | DB; CROSSOVER | 6 (period) | Nortriptyline + Morphine | 100 + 100 mg | oral | 15 (13) –11 (9)–18 (15) | Nortriptyline Morphine | 100 mg 100 mg | oral oral | 13 (13)–16 (14)–16 (16) 17 (14) –14 (10)–16 (14) |
| Pickering 2020 [31] | Neuropathic pain (long-standing refractory) | DB; CROSSOVER | 5 (period) | Ketamine + magnesium | 0.5 mg/kg + 3g | i.v. | 20 (20) | Placebo Ketamine | 0.5 mg/kg | i.v. i.v. | 20 (20) 20 (20) |
| Harrison 2013 [41] | HIV-associated polyneuropathy | DB; CROSSOVER | 4 (period) | Duloxetine + methadone | 60 + 30 mg | oral | 4 (3) -3 (3)?–3 (3) –4 (3)? | Placebo Duloxetine Methadone | 60 mg 30 mg | oral oral oral | 4 (4)? –4 (3)?–2 (2)? –4 (3) 4 (4) -3 (3)?–3 (2) –4 (4)? 4 (4)–4 (2)–2 (2)? –3 (3)? |
| Garassino 2013 [40] | Neuropathic pain in cancer patients | PARALLEL | 2 | Pregabalin ↑ + oxycodone fix Pregabalin fix + oxycodone ↑ | 300 + 20 mg 50 + 20 mg? | oral oral | 38 (32) 37 (35) | ||||
| Dou 2017 [33] | Neuropathic pain in cancer patients treated with morphine | DB; CROSSOVER | 2 (period) | Pregabalin + morphine PR | 300 + ≥180 mg | oral | 20 (?)–20 (?) | Placebo + morphine PR | + ≥ 180 mg | oral | 20 (?)–20 (?) |
| Study | Bias Arising from the Randomization Process | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Outcome Data | Bias in the Measurement of the Outcome | Bias in the Selection of the Reported Result | Other Potential Sources of Bias |
|---|---|---|---|---|---|---|
| Langford 2013 [43] | + | + | + | + | ? | ? |
| Irving 2012 [44] | + | + | + | ? | ? | ? |
| Shaibani 2012 [45] | + | + | + | + | + | + |
| Tesfaye 2013 [42] | + | + | + | + | ? | - |
| Holbech 2015 [38] | + | + | + | + | ? | - |
| Matsuoka 2019 [32] | + | + | + | + | ? | - |
| Singh 2021 [30] | ? | - | - | + | ? | - |
| Rigo 2017 [34] | + | + | + | + | ? | . |
| Kim 2016 [35] | + | + | + | + | ? | - |
| Baron 2014 [36] | ? | + | + | + | ? | - |
| Gilron 2015 [37] | + | + | + | + | ? | - |
| Pickering 2020 [31] | + | + | + | + | ? | - |
| Turcotte 2015 [39] | + | - | + | + | + | - |
| Harrison 2013 [41] | + | - | + | + | ? | - |
| Dou 2017 [33] | + | + | + | + | ? | - |
| Garassino 2013 [40] | ? | - | + | ? | ? | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serrano Afonso, A.; Carnaval, T.; Videla Cés, S. Combination Therapy for Neuropathic Pain: A Review of Recent Evidence. J. Clin. Med. 2021, 10, 3533. https://doi.org/10.3390/jcm10163533
Serrano Afonso A, Carnaval T, Videla Cés S. Combination Therapy for Neuropathic Pain: A Review of Recent Evidence. Journal of Clinical Medicine. 2021; 10(16):3533. https://doi.org/10.3390/jcm10163533
Chicago/Turabian StyleSerrano Afonso, Ancor, Thiago Carnaval, and Sebastià Videla Cés. 2021. "Combination Therapy for Neuropathic Pain: A Review of Recent Evidence" Journal of Clinical Medicine 10, no. 16: 3533. https://doi.org/10.3390/jcm10163533