
Multidimensional Prognostic Index and Outcomes in Older Patients Undergoing Transcatheter Aortic Valve Implantation: Survival of the Fittest


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Cardiology Assessment
2.3. Comprehensive Geriatric Assessment
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
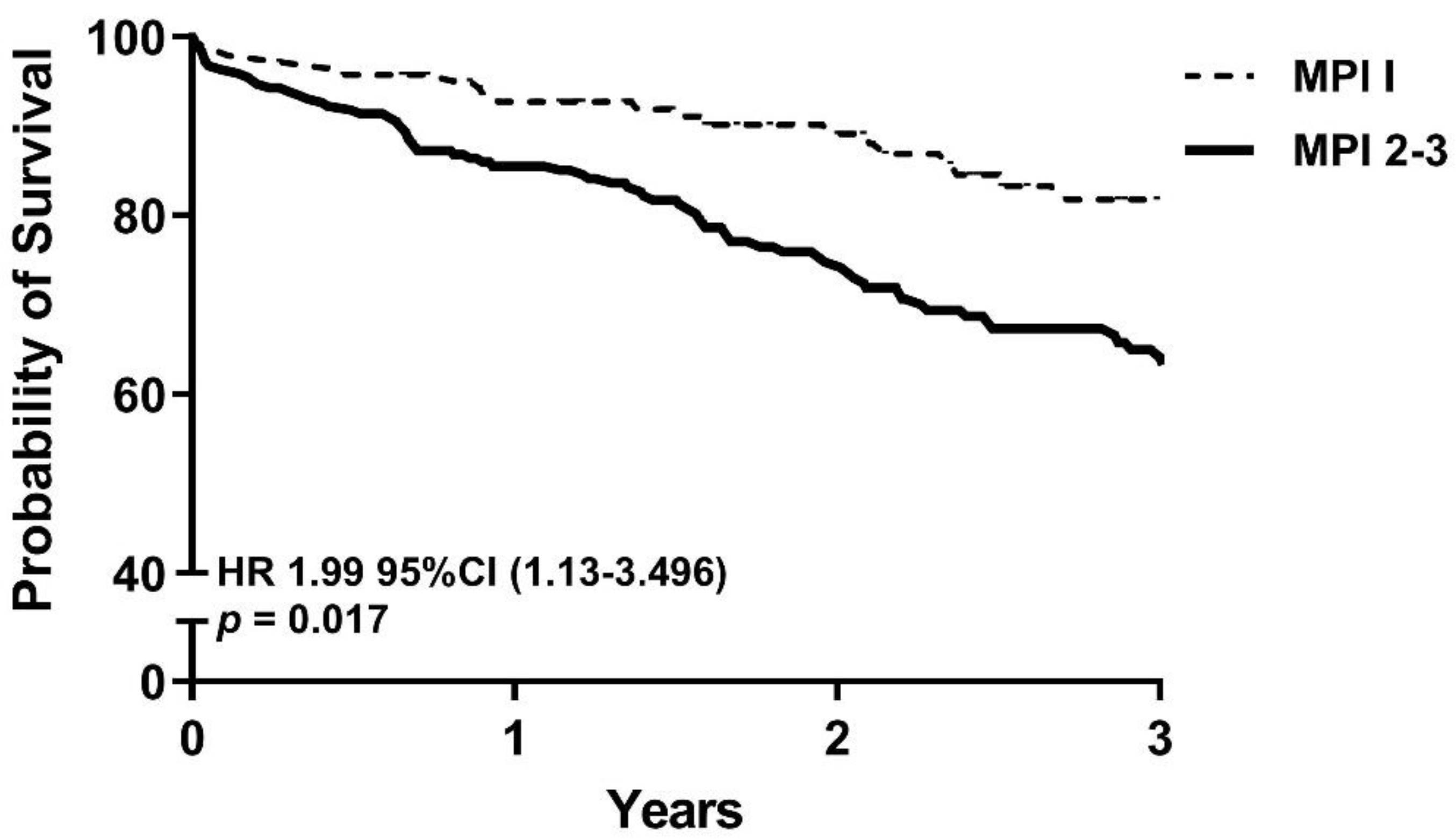
3.2. Primary Outcomes
3.3. Secondary Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
| Complication | Total | MPI-1 | MPI-2–3 | Univariable OR (95% CI) | p Value |
|---|---|---|---|---|---|
| Post procedural stroke | 12/374 (3.2%) | 3/141 (2.1%) | 9/233 (3.9%) | 1.85 (0.49–6.95) | 0.36 |
| New pacemaker | 63/376 (16.8%) | 25/141 (17.7%) | 38/233 (16.3%) | 0.90 (0.52–1.57) | 0.72 |
| Vascular complication | 56/376 (14.9%) | 14/141 (9.9%) | 42/233 (18.0%) | 2.00 (1.05–3.80) | 0.04 |
| Infection | 32/376 (8.5%) | 8/141 (5.7%) | 24/233 (10.3%) | 1.91 (0.83–4.37) | 0.13 |
| MI postprocedural | 1/323 (85.9%) | 1/119 (0.7%) | 0/233 | - | - |
| Delirium | 55/375 (14.6%) | 15/141 (10.6%) | 40/233 (17.2%) | 1.75 (0.93–3.30) | 0.08 |
| Any Complication | 145/322 (45.0%) | 47/119 (39.4%) | 98/201 (48.7%) | 1.15 (0.92–2.31) | 0.11 |
References
- Grimard, B.H.; Larson, J.M. Aortic stenosis: Diagnosis and treatment. Am. Fam. Physician 2008, 78, 717–724. [Google Scholar] [PubMed]
- Popma, J.J.; Adams, D.H.; Reardon, M.J.; Yakubov, S.J.; Kleiman, N.S.; Heimansohn, D.; Hermiller, J.; Hughes, G.C.; Harrison, J.K.; Coselli, J.; et al. Transcatheter aortic valve replacement using a self-expanding bioprosthesis in patients with severe aortic stenosis at extreme risk for surgery. J. Am. Coll. Cardiol. 2014, 63, 1972–1981. [Google Scholar] [CrossRef] [Green Version]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Voigtländer, L.; Seiffert, M. Expanding TAVI to low and intermediate risk patients. Front. Cardiovasc. Med. 2018, 5. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, M.; Webb, J.; Gilard, M.; Capodanno, D.; Tamburino, C. Transcatheter aortic valve implantation in 2017: State of the art. EuroIntervention 2017, 13, AA11–AA21. [Google Scholar] [CrossRef]
- Schoenenberger, A.W.; Stortecky, S.; Neumann, S.; Moser, A.; Jüni, P.; Carrel, T.; Huber, C.; Gandon, M.; Bischoff, S.; Schoenenberger, C.-M.; et al. Predictors of functional decline in elderly patients undergoing transcatheter aortic valve implantation (TAVI). Eur. Heart J. 2013, 34, 684–692. [Google Scholar] [CrossRef] [Green Version]
- Stortecky, S.; Schoenenberger, A.W.; Moser, A.; Kalesan, B.; Jüni, P.; Carrel, T.; Bischoff, S.; Schoenenberger, C.-M.; Stuck, A.E.; Windecker, S.; et al. Evaluation of multidimensional geriatric assessment as a predictor of mortality and cardiovascular events after transcatheter aortic valve implantation. JACC Cardiovasc. Interv. 2012, 5, 489–496. [Google Scholar] [CrossRef] [Green Version]
- Green, P.; Woglom, A.E.; Genereux, P.; Daneault, B.; Paradis, J.-M.; Schnell, S.; Hawkey, M.; Maurer, M.S.; Kirtane, A.J.; Kodali, S. The impact of frailty status on survival after transcatheter aortic valve replacement in older adults with severe aortic stenosis: A single-center experience. JACC Cardiovasc. Interv. 2012, 5, 974–981. [Google Scholar] [CrossRef] [Green Version]
- Goudzwaard, J.A.; de Ronde-Tillmans, M.J.; El Faquir, N.; Acar, F.; Van Mieghem, N.M.; Lenzen, M.J.; de Jaegere, P.P.; Mattace-Raso, F.U. The Erasmus Frailty Score is associated with delirium and 1-year mortality after Transcatheter Aortic Valve Implantation in older patients. The TAVI Care & Cure program. Int. J. Cardiol. 2019, 276, 48–52. [Google Scholar] [CrossRef]
- Pilotto, A.; Ferrucci, L.; Franceschi, M.; D’Ambrosio, L.P.; Scarcelli, C.; Cascavilla, L.; Paris, F.; Placentino, G.; Seripa, D.; Dallapiccola, B.; et al. Development and validation of a multidimensional prognostic index for one-year mortality from comprehensive geriatric assessment in hospitalized older patients. Rejuvenation Res. 2008, 11, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Pilotto, A.; Addante, F.; Franceschi, M.; Leandro, G.; Rengo, G.; D’Ambrosio, P.; Longo, M.G.; Rengo, F.; Pellegrini, F.; Dallapiccola, B.; et al. Multidimensional prognostic index based on a comprehensive geriatric assessment predicts short-term mortality in older patients with heart failure. Circ. Heart Fail. 2010, 3, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Cammalleri, V.; Bonanni, M.; Bueti, F.M.; Matteucci, A.; Cammalleri, L.; Stifano, G.; Muscoli, S.; Romeo, F. Multidimensional Prognostic Index (MPI) in elderly patients with acute myocardial infarction. Aging Clin. Exp. Res. 2021, 33, 1875–1883. [Google Scholar] [CrossRef]
- Pilotto, A.; Veronese, N.; Daragjati, J.; Cruz-Jentoft, A.J.; Polidori, M.C.; Mattace-Raso, F.; Paccalin, M.; Topinkova, E.; Siri, G.; Greco, A.; et al. Using the multidimensional prognostic index to predict clinical outcomes of hospitalized older persons: A prospective, multicenter, international study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 74, 1643–1649. [Google Scholar] [CrossRef]
- Bureau, M.-L.; Liuu, E.; Christiaens, L.; Pilotto, A.; Mergy, J.; Bellarbre, F.; Ingrand, P.; Paccalin, M.; Cruz-Jentoft, A.J.; Maggi, S.; et al. Using a multidimensional prognostic index (MPI) based on comprehensive geriatric assessment (CGA) to predict mortality in elderly undergoing transcatheter aortic valve implantation. Int. J. Cardiol. 2017, 236, 381–386. [Google Scholar] [CrossRef]
- Ungar, A.; Mannarino, G.; Van Der Velde, N.; Baan, J.; Thibodeau, M.-P.; Masson, J.-B.; Santoro, G.; Van Mourik, M.; Jansen, S.; Deutsch, C.; et al. Comprehensive geriatric assessment in patients undergoing transcatheter aortic valve implantation—results from the CGA-TAVI multicentre registry. BMC Cardiovasc. Disord. 2018, 18, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Mourik, M.S.; van der Velde, N.; Mannarinom, G.; Thibodeau, M.-P.; Masson, J.-B.; Santoro, G.; Baan, J.; Jansen, S.; Kurucova, J.; Thoenes, M. Value of a comprehensive geriatric assessment for predicting one-year outcomes in patients undergoing transcatheter aortic valve implantation: Results from the CGA-TAVI multicentre registry. J. Geriatr. Cardiol. JGC 2019, 16, 468. [Google Scholar] [PubMed]
- Skaar, E.; Eide, L.S.P.; Norekvål, T.M.; Ranhoff, A.H.; Nordrehaug, J.E.; Forman, D.E.; Schoenenberger, A.W.; Hufthammer, K.O.; Kuiper, K.K.-J.; Bleie, Ø. A novel geriatric assessment frailty score predicts 2-year mortality after transcatheter aortic valve implantation. Eur. Heart J. Qual. Care Clin. Outcomes 2018, 5, 153–160. [Google Scholar] [CrossRef]
- Martin, G.P.; Sperrin, M.; Ludman, P.F.; Mark, A.; Gunning, M.; Townend, J.; Redwood, S.R.; Kadam, U.T.; Buchan, I.; Mamas, M.A. Do frailty measures improve prediction of mortality and morbidity following transcatheter aortic valve implantation? An analysis of the UK TAVI registry. BMJ Open 2018, 8, e022543. [Google Scholar] [PubMed]
- De Ronde-Tillmans, M.; Goudzwaard, J.A.; El Faquir, N.; van Mieghem, N.M.; Mattace-Raso, F.U.S.; Cummins, P.A.; Lenzen, M.J.; de Jaegere, P.P.T. TAVI Care and Cure, the Rotterdam multidisciplinary program for patients undergoing transcatheter aortic valve implantation: Design and rationale. Int. J. Cardiol. 2020, 302, 36–41. [Google Scholar] [CrossRef]
- De Ronde-Tillmans, M.J.; Lenzen, M.J.; Abawi, M.; Van Mieghem, N.M.; Zijlstra, F.; De Jaegere, P.P. 10 years of transcatheter aortic valve implantation: An overview of the clinical applicability and findings. Ned. Tijdschr. Voor Geneeskd. 2013, 158, A7768–A7768. [Google Scholar]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Muñoz, D.R.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. J. Cardiothorac. Surg. 2017, 52, 616–664. [Google Scholar] [CrossRef]
- Schultz, C.J.; Moelker, A.D.; Tzikas, A.; Rossi, A.; Van Geuns, R.-J.; De Feyter, P.J.; Serruys, P.W. Cardiac CT: Necessary for precise sizing for transcatheter aortic implantation. EuroIntervention 2010, 6, G6–G13. [Google Scholar]
- Angleman, S.B.; Santoni, G.; Pilotto, A.; Fratiglioni, L.; Welmer, A.-K. Investigators MAP: Multidimensional prognostic index in association with future mortality and number of hospital days in a population-based sample of older adults: Results of the EU funded MPI_AGE project. PLoS ONE 2015, 10, e0133789. [Google Scholar] [CrossRef] [Green Version]
- Katz, S. Studies of illness in the aged. The index of ADL: A standardized measure of biologic and psychologic function. JaMa 1963, 185, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Parmelee, P.A.; Thuras, P.D.; Katz, I.R.; Lawton, M.P. Validation of the Cumulative Illness Rating Scale in a Geriatric Residential Population. J. Am. Geriatr. Soc. 1995, 43, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Elia, M. Nutritional Screening of Adults: A Multidisciplinary Responsibility; Malnutrition Advisory Group (MAG): Redditch, UK; BAPEN: Reditch, UK, 2003. [Google Scholar]
- Balzer, K.; Pohl, C.; Dassen, T.; Halfens, R. The norton, waterlow, braden, and care dependency scalesl comparing their validity when identifying patients’ pressure sore risk. J. Wound Ostomy Cont. Nurs. 2007, 34, 389–398. [Google Scholar] [CrossRef]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age and gender-related test performance in community-dwelling elderly people: Six-minute walk test, berg balance scale, timed up & go test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar] [CrossRef] [Green Version]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; Van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.-A. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The valve academic research consortium-2 consensus document. J. Am. Coll. Cardiol. 2012, 60, 1438–1454. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roques, F.; Nashef, S.A.M.; Michel, P.; Gauducheau, E.; De Vincentiis, C.; Baudet, E.; Cortina, J.; David, M.; Faichney, A.; Gavrielle, F.; et al. Risk factors and outcome in European cardiac surgery: Analysis of the EuroSCORE multinational database of 19030 patients. Eur. J. Cardio-Thorac. Surg. 1999, 15, 816–823. [Google Scholar] [CrossRef] [Green Version]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Pilotto, A.; Custodero, C.; Maggi, S.; Polidori, M.C.; Veronese, N.; Ferrucci, L. A multidimensional approach to frailty in older people. Ageing Res. Rev. 2020, 60, 101047. [Google Scholar] [CrossRef]
- Lilamand, M.; Dumonteil, N.; Nourhashémi, F.; Hanon, O.; Marcheix, B.; Toulza, O.; Elmalem, S.; van Kan, G.A.; Raynaud-Simon, A.; Vellas, B.; et al. Gait speed and comprehensive geriatric assessment: Two keys to improve the management of older persons with aortic stenosis. Int. J. Cardiol. 2014, 173, 580–582. [Google Scholar] [CrossRef]
- Sancarlo, D.; Pilotto, A.; Panza, F.; Copetti, M.; Longo, M.G.; D’Ambrosio, P.; D’Onofrio, G.; Ferrucci, L.; Pilotto, A. A Multidimensional Prognostic Index (MPI) based on a comprehensive geriatric assessment predicts short and long-term all-cause mortality in older hospitalized patients with transient ischemic attack. J. Neurol. 2011, 259, 670–678. [Google Scholar] [CrossRef] [Green Version]
- Goudzwaard, J.A.; Ronde-Tillmans, M.J.A.G.D.; Jager, T.A.J.D.; Lenzen, M.J.; Nuis, R.-J.; van Mieghem, N.M.; Daemen, J.; de Jaegere, P.P.T.; Mattace-Raso, F.U.S. Incidence, determinants and consequences of delirium in older patients after transcatheter aortic valve implantation. Age Ageing 2020, 49, 389–394. [Google Scholar] [CrossRef]
- Goudzwaard, J.A.; Ronde-Tillmans, M.J.A.G.D.; Hoorn, F.E.D.V.; Kwekkeboom, E.H.C.; Lenzen, M.J.; van Wiechen, M.P.H.; Ooms, J.F.W.; Nuis, R.-J.; Van Mieghem, N.M.; Daemen, J.; et al. Impact of frailty on health-related quality of life 1 year after transcatheter aortic valve implantation. Age Ageing 2020, 49, 989–994. [Google Scholar] [CrossRef] [PubMed]

| Assessment | No Problem (Value = 0) | Minor Problem (Value = 0.5) | Severe Problem (Value = 1) |
|---|---|---|---|
| ADL | 0 | 1–6 | 7–12 |
| IADL | 0–1 | 2–7 | 8–14 |
| MMSE | 28–30 | 25–27 | 0–24 |
| CIRS-CI | 0 | 1–2 | ≥3 |
| MUST | 0 | 1 | ≥2 |
| Waterlow score | 3–9 | 10–14 | 15–45 |
| Number of medications | 0–3 | 4–6 | ≥7 |
| Social support network | Living with family | Institutionalized | Living alone |
| Characteristic | Total (377) | MPI-1 N = 141 | MPI-2–3 N = 233 | p Value |
|---|---|---|---|---|
| Age (y) | 81.54 (±6.1) | 80.68 (±5.7) | 82.03 (±6.4) | 0.040 |
| Men (%) | 189 (49.7%) | 96 (68.1%) | 89 (38.2%) | <0.001 |
| BMI (kg/m2) | 27.2 (±4.8) | 27.35 (±4.25) | 27.14 (±5.20) | 0.697 |
| Cardiovascular risk factors | ||||
| Hypertension (%) | 294 (78.2%) | 101 (71.6%) | 192 (82.8%) | 0.013 |
| Hypercholesterolemia (%) | 231 (61.4%) | 83 (58.9%) | 147 (63.9%) | 0.378 |
| Diabetes mellitus (%) | 124 (33.1%) | 28 (19.9%) | 95 (40.9%) | <0.001 |
| Current smoker (%) | 30 (8.0%) | 13 (9.2%) | 17 (7.3%) | 0.558 |
| Comorbidities | ||||
| Previous myocardial infarction (%) | 73 (19.4%) | 27 (19.1%) | 46 (19.7%) | 1.00 |
| Previous stroke (%) | 82 (21.8%) | 21 (14.9%) | 49 (21.1%) | 0.028 |
| COPD (%) | 82 (21.8%) | 35 (24.8%) | 47 (20.4%) | 0.367 |
| Renal dysfunction (%) | 162 (43.5%) | 47 (33.3%) | 115 (49.4%) | 0.002 |
| CIRS index | 1.91 (±0.27) | 1.84 (± 0.26) | 1.96 (±0.26) | <0.001 |
| Symptoms | ||||
| NYHA Class 3 or 4 (%) | 244 (64.9%) | 73 (51.8%) | 171 (73.4%) | <0.001 |
| Angina CCS classification 3 or 4 (%) | 43 (11.4%) | 13 (9.4%) | 30 (13.2%) | 0.318 |
| Vertigo (%) | 143 (41.4%) | 53 (40.5%) | 90 (42.5%) | 0.736 |
| Echocardiography | ||||
| AV area (cm2) | 0.76 (± 0.24) | 0.8 (±0.23) | 0.74 (±0.25) | 0.052 |
| Peak AoV, (m/s) | 4.0 (± 0.70) | 4.0 (±0.69) | 4.0 (±0.71) | 0.923 |
| Cardiovascular risk scores | ||||
| Logistic Euroscore | 16.82 (±11.03) | 14.80 (±9.55) | 18.02 (±11.70) | 0.006 |
| STS score | 5.47 (±3.03) | 4.29 (±2.19) | 6.17 (±3.25) | 0.228 |
| CGA domains | ||||
| Cognitive impairment probable (%) | 111 (29.5%) | 20 (14.2%) | 91 (39.1%) | <0.001 |
| Malnutrition probable (%) | 41 (10.9%) | 5 (3.5%) | 36 (15.5%) | <0.001 |
| Limitation of mobility, TUGT (%) | 48 (12.8%) | 5 (3.9%) | 43 (21.6%) | <0.001 |
| Limitation of mobility, 5MGS (%) | 219 (58.2%) | 61 (48.8%) | 158 (77.5%) | <0.001 |
| Reduced muscle strength, male (%) | 65 (17.3%) | 24 (17%) | 39 (16.7%) | 0.004 |
| Reduces muscle strength, female (%) | 100 (26.6%) | 17 (12.1%) | 83 (35.6%) | 0.016 |
| Limitation in ADL activity (%) | 111 (29.5%) | 9 (6.4%) | 102 (43.8%) | <0.001 |
| Limitation in IADL activity (%) | 200 (53.2%) | 35 (24.8%) | 165 (70.8%) | <0.001 |
| Variable | HR | 95% CI | p-Value |
|---|---|---|---|
| Age | 0.99 | 0.95–1.03 | 0.51 |
| Sex (men) | 0.63 | 0.84–1.03 | 0.07 |
| MPI-1 vs. MPI-2–3 | 1.99 | 1.13–3.50 | 0.02 |
| Diabetes mellitus | 1.16 | 0.71–1.90 | 0.56 |
| Hypercholesterolemia | 0.80 | 0.50–0.32 | 0.003 |
| Peripheral artery disease | 1.34 | 0.84–2.12 | 0.23 |
| Renal dysfunction | 1.85 | 1.19–2.87 | 0.006 |
| Limitation of mobility (5MGST) | 2.09 | 1.15–3.65 | 0.02 |
| Logistic Euroscore | 1.01 | 0.99–1.03 | 0.43 |
| Post procedural stroke | 2.96 | 1.26–6.99 | 0.01 |
| Delirium | 1.22 | 0.71–2.10 | 0.48 |
| Variable | HR | 95% CI | p-Value |
|---|---|---|---|
| Age | 0.99 | 0.95–1.04 | 0.66 |
| Sex (women) | 2.09 | 1.23–3.56 | 0.006 |
| Diabetes mellitus | 0.88 | 0.51–1.50 | 0.63 |
| Hypercholesterolemia | 0.47 | 0.28–0.80 | 0.005 |
| Peripheral artery disease | 1.42 | 0.82–2.46 | 0.21 |
| Renal dysfunction | 1.98 | 1.18–3.33 | 0.01 |
| Limitation of mobility (5MGST) | 1.19 | 0.97–3.79 | 0.06 |
| Logistic Euroscore | 1.01 | 0.98–1.03 | 0.66 |
| Post procedural stroke | 3.98 | 1.59–10.05 | 0.003 |
| Delirium | 0.97 | 0.52–1.81 | 0.93 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goudzwaard, J.A.; Chotkan, S.; De Ronde-Tillmans, M.J.A.G.; Lenzen, M.J.; van Wiechen, M.P.H.; Ooms, J.F.W.; Polinder-Bos, H.A.; de Beer-Leentfaar, M.; Van Mieghem, N.M.; Daemen, J.; et al. Multidimensional Prognostic Index and Outcomes in Older Patients Undergoing Transcatheter Aortic Valve Implantation: Survival of the Fittest. J. Clin. Med. 2021, 10, 3529. https://doi.org/10.3390/jcm10163529
Goudzwaard JA, Chotkan S, De Ronde-Tillmans MJAG, Lenzen MJ, van Wiechen MPH, Ooms JFW, Polinder-Bos HA, de Beer-Leentfaar M, Van Mieghem NM, Daemen J, et al. Multidimensional Prognostic Index and Outcomes in Older Patients Undergoing Transcatheter Aortic Valve Implantation: Survival of the Fittest. Journal of Clinical Medicine. 2021; 10(16):3529. https://doi.org/10.3390/jcm10163529
Chicago/Turabian StyleGoudzwaard, Jeannette A., Sadhna Chotkan, Marjo J. A. G. De Ronde-Tillmans, Mattie J. Lenzen, Maarten P. H. van Wiechen, Joris F. W. Ooms, Harmke A. Polinder-Bos, Madelon de Beer-Leentfaar, Nicolas M. Van Mieghem, Joost Daemen, and et al. 2021. "Multidimensional Prognostic Index and Outcomes in Older Patients Undergoing Transcatheter Aortic Valve Implantation: Survival of the Fittest" Journal of Clinical Medicine 10, no. 16: 3529. https://doi.org/10.3390/jcm10163529