
Effect of Progressive Head Extension Swallowing Exercise on Lingual Strength in the Elderly: A Randomized Controlled Trial

 ,
,
Abstract
:1. Introduction
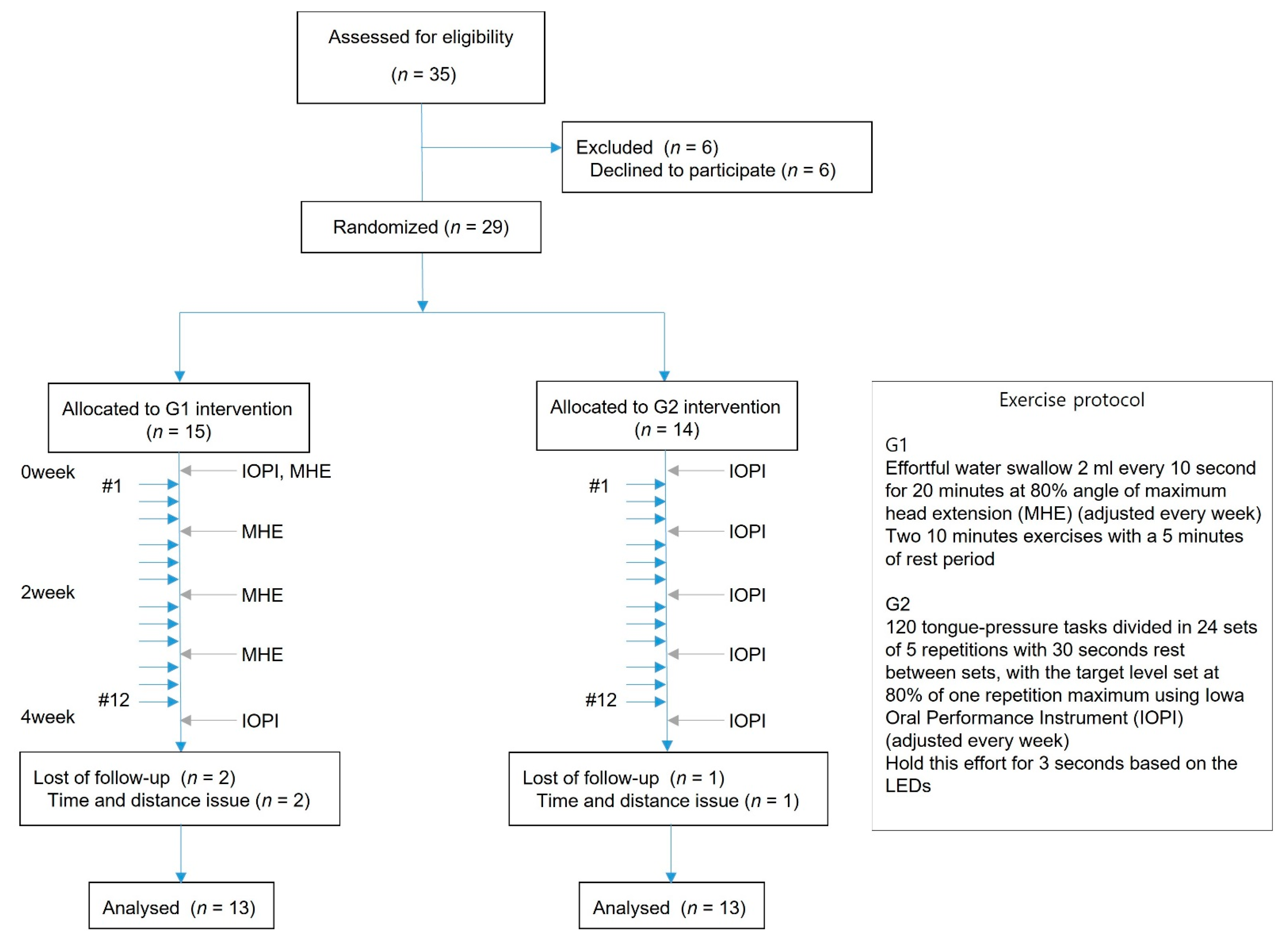
2. Materials and Methods
2.1. Participants
2.2. Experimental Protocol
2.3. Tongue Strengthening Training
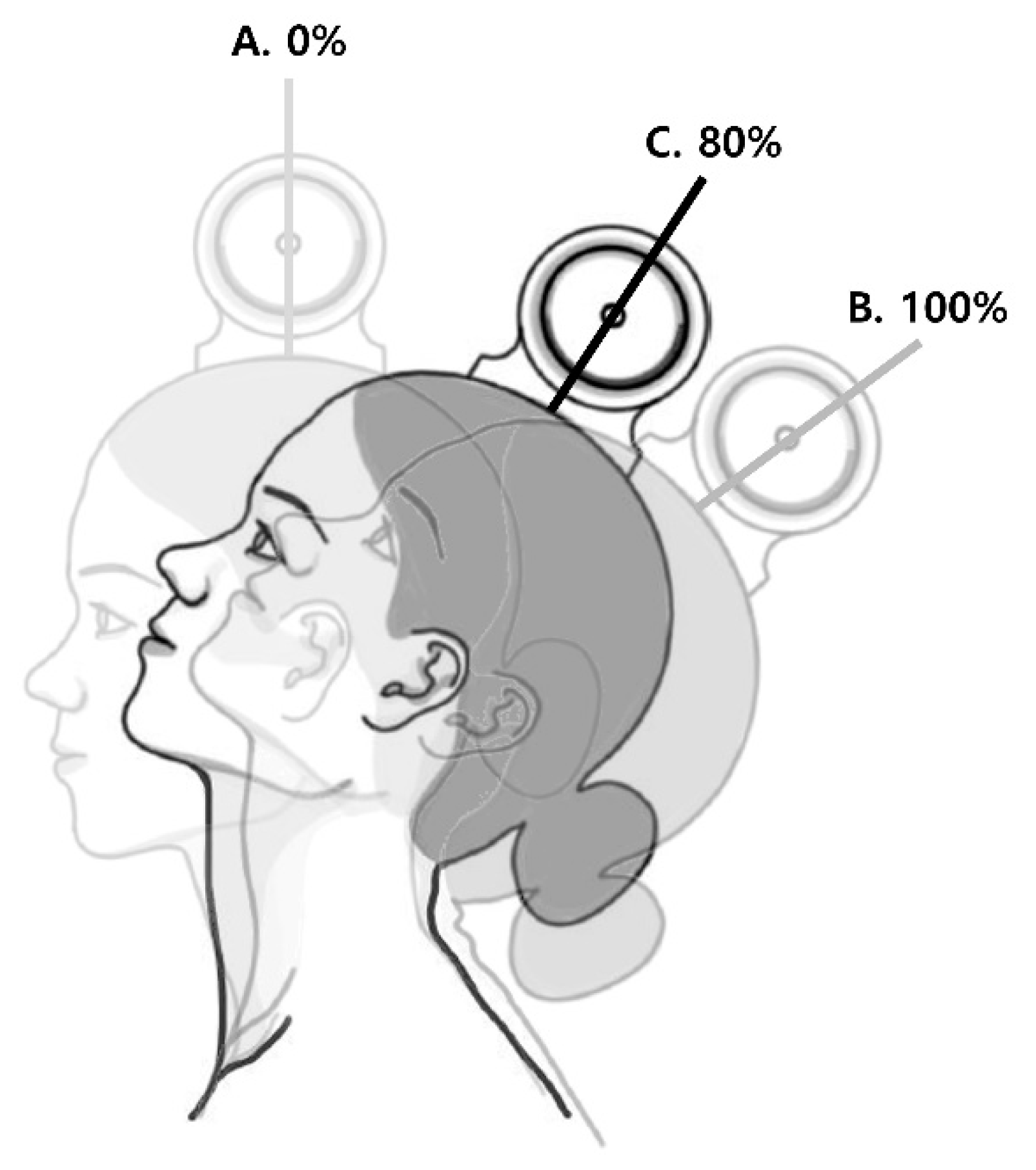
2.4. Head Extension Measurements
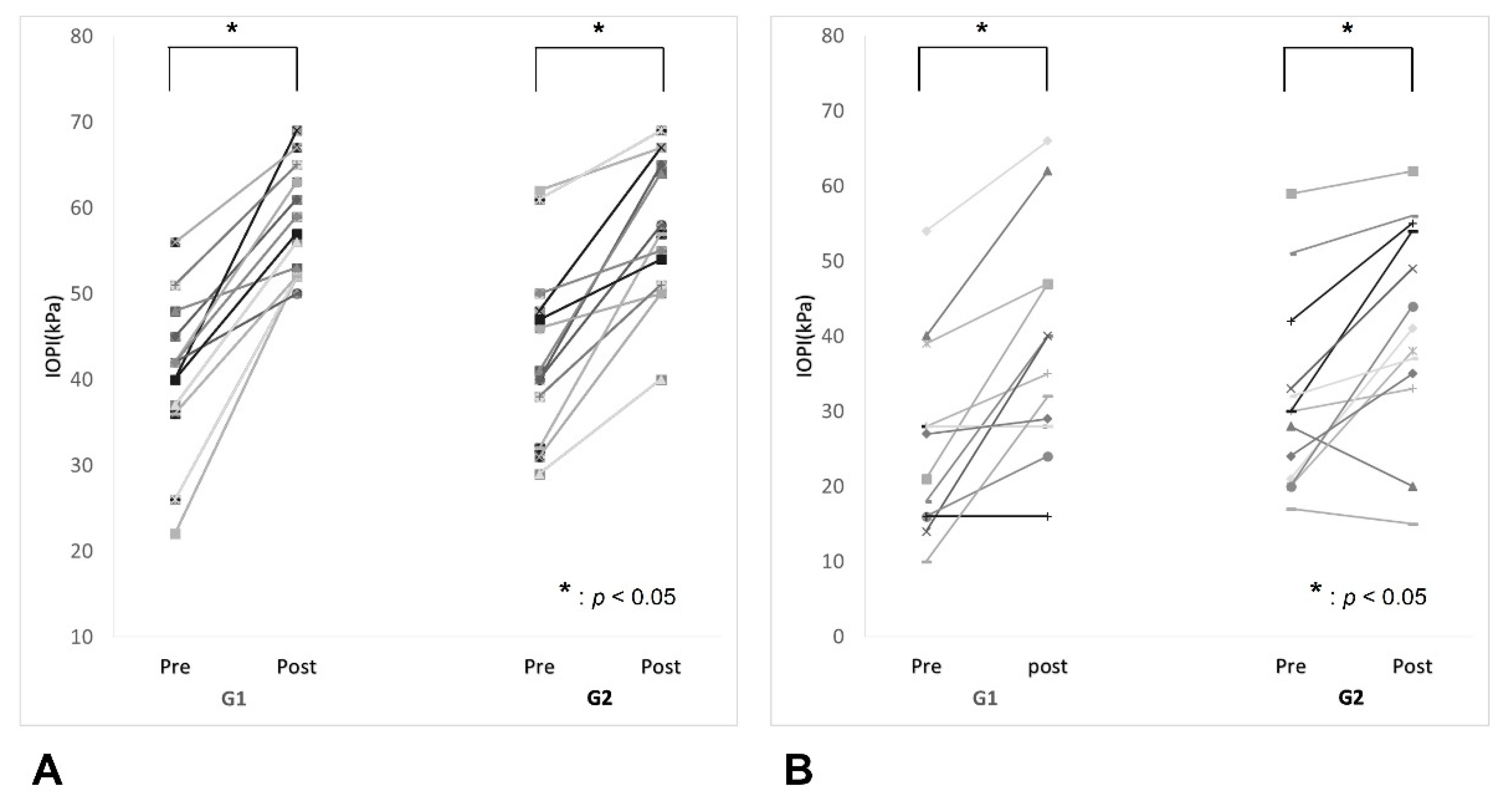
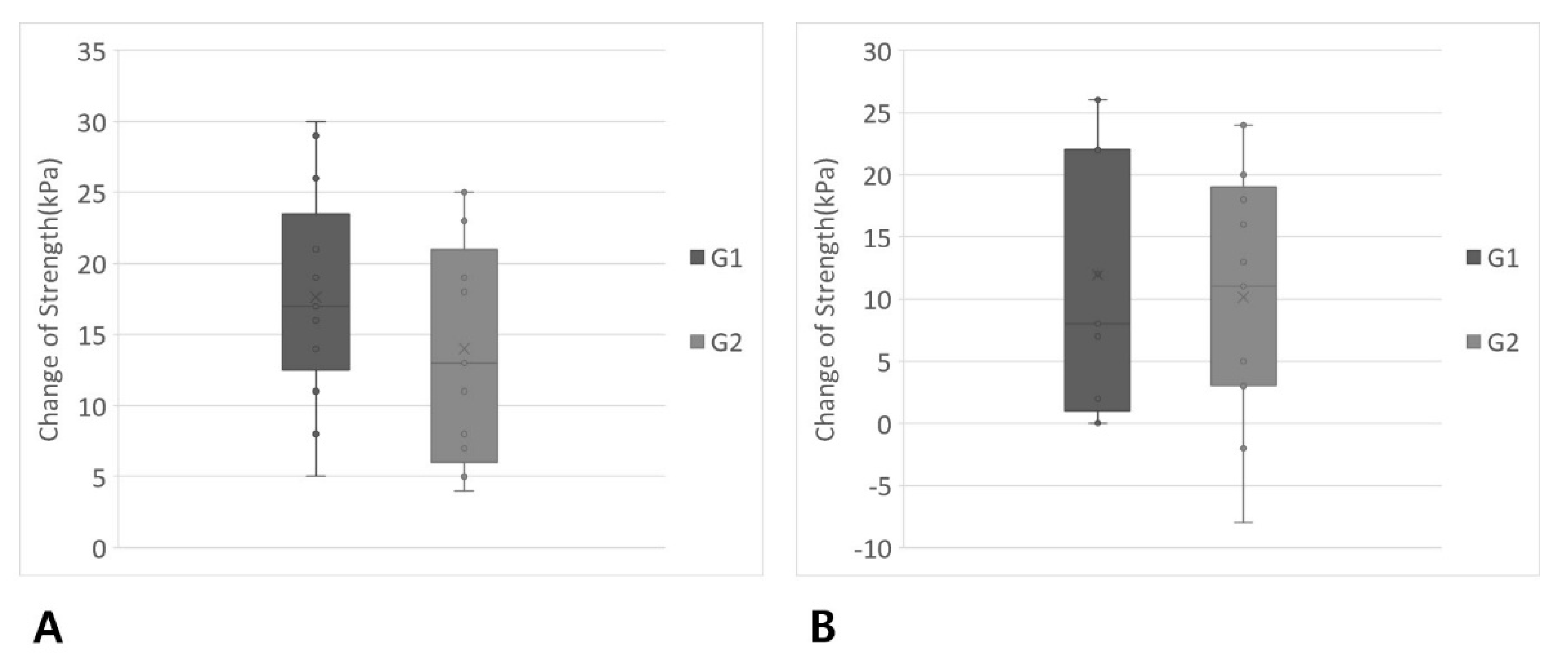
2.5. Tongue Strength Measurements
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Robbins, J.; Hamilton, J.W.; Lof, G.L.; Kempster, G.B. Oropharyngeal swallowing in normal adults of different ages. Gastroenterology 1992, 103, 823–829. [Google Scholar] [CrossRef]
- Rofes, L.; Arreola, V.; Romea, M.; Palomera, E.; Almirall, J.; Cabre, M.; Serra-Prat, M.; Clave, P. Pathophysiology of oropharyngeal dysphagia in the frail elderly. Neurogastroenterol. Motil. 2010, 22, 851–858.e230. [Google Scholar] [CrossRef]
- McConnel, F.M. Analysis of pressure generation and bolus transit during pharyngeal swallowing. Laryngoscope 1988, 98, 71–78. [Google Scholar] [CrossRef]
- Clark, H.M.; Henson, P.A.; Barber, W.D.; Stierwalt, J.A.; Sherrill, M. Relationships among subjective and objective measures of tongue strength and oral phase swallowing impairments. Am. J. Speech Lang. Pathol. 2003, 12, 40–50. [Google Scholar] [CrossRef]
- Stierwalt, J.A.; Youmans, S.R. Tongue measures in individuals with normal and impaired swallowing. Am. J. Speech Lang. Pathol 2007, 16, 148–156. [Google Scholar] [CrossRef]
- Robbins, J.; Gangnon, R.E.; Theis, S.M.; Kays, S.A.; Hewitt, A.L.; Hind, J.A. The effects of lingual exercise on swallowing in older adults. J. Am. Geriatr. Soc. 2005, 53, 1483–1489. [Google Scholar] [CrossRef]
- Wakabayashi, H.; Matsushima, M.; Momosaki, R.; Yoshida, S.; Mutai, R.; Yodoshi, T.; Murayama, S.; Hayashi, T.; Horiguchi, R.; Ichikawa, H. The effects of resistance training of swallowing muscles on dysphagia in older people: A cluster, randomized, controlled trial. Nutrition 2018, 48, 111–116. [Google Scholar] [CrossRef]
- Park, T.; Kim, Y. Effects of tongue pressing effortful swallow in older healthy individuals. Arch. Gerontol. Geriatr. 2016, 66, 127–133. [Google Scholar] [CrossRef]
- Brukner, P.; Khan, K. Brukner & Khan’s Clinical Sports Medicine, 3rd ed.; McGraw-Hill: Sydney, Australia; New York, NY, USA, 2010; 117p. [Google Scholar]
- Clark, H.M.; O’Brien, K.; Calleja, A.; Corrie, S.N. Effects of directional exercise on lingual strength. J. Speech Lang. Hear. Res. 2009, 52, 1034–1047. [Google Scholar] [CrossRef]
- Yeates, E.M.; Molfenter, S.M.; Steele, C.M. Improvements in tongue strength and pressure-generation precision following a tongue-pressure training protocol in older individuals with dysphagia: Three case reports. Clin. Interv. Aging 2008, 3, 735–747. [Google Scholar] [CrossRef] [Green Version]
- Clark, H.M.; Shelton, N. Training effects of the effortful swallow under three exercise conditions. Dysphagia 2014, 29, 553–563. [Google Scholar] [CrossRef]
- Oh, J.C. Effect of the head extension swallowing exercise on suprahyoid muscle activity in elderly individuals. Exp. Gerontol. 2018, 110, 133–138. [Google Scholar] [CrossRef]
- Van den Steen, L.; Schellen, C.; Verstraelen, K.; Beeckman, A.S.; Vanderwegen, J.; De Bodt, M.; Van Nuffelen, G. Tongue-Strengthening Exercises in Healthy Older Adults: Specificity of Bulb Position and Detraining Effects. Dysphagia 2018, 33, 337–344. [Google Scholar] [CrossRef]
- Robbins, J.; Levine, R.; Wood, J.; Roecker, E.B.; Luschei, E. Age effects on lingual pressure generation as a risk factor for dysphagia. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, M257–M262. [Google Scholar] [CrossRef]
- Pauloski, B.R. Rehabilitation of dysphagia following head and neck cancer. Phys. Med. Rehabil. Clin. N Am. 2008, 19, 889–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, J.C. A Pilot Study of the Head Extension Swallowing Exercise: New Method for Strengthening Swallowing-Related Muscle Activity. Dysphagia 2016, 31, 680–686. [Google Scholar] [CrossRef]
- Kier, W.M. Tongues, tentacles and trunks: The biomechanics of movement in muscular-hydrostats. Zool. J. Linn. Soc. 1985, 83, 30–324. [Google Scholar] [CrossRef]
- Oh, J.C.; Park, J.W.; Cha, T.H.; Woo, H.S.; Kim, D.K. Exercise using tongue-holding swallow does not improve swallowing function in normal subjects. J. Oral Rehabil. 2012, 39, 364–369. [Google Scholar] [CrossRef]
- Park, J.W.; Hong, H.J.; Nam, K. Comparison of three exercises on increasing tongue strength in healthy young adults. Arch. Oral Biol. 2020, 111, 104636. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tongue Progressive Resistance Exercise; G1 (n = 13) | Tongue Isometric Exercise; G2 (n = 13) | p-Value | |
|---|---|---|---|
| Age (years) | 72.7 ± 7.3 (65–87) | 73.2 ± 5.7 (65–82) | 0.835 |
| Sex | |||
| Male | 4 | 1 | 0.135 |
| Female | 9 | 12 | |
| Mini-mental status exam | 28.6 ± 1.3 (26–30) | 28.2 ± 1.3 (26–30) | 0.387 |
| Baseline maximum head extension angle (degrees) | 39.6 ± 9.9 (25–55) | ||
| 4th week maximum head extension angle (degrees) | 57.7 ± 7.8 (40–70) | ||
| Baseline maximum isometric pressure (kPa) | 40.5 ± 9.2 (22–56) | 43.5 ± 10.4 (29–62) | 0.455 |
| Baseline peak pressure during swallowing (kPa) | 26.1 ± 12.4 (10–54) | 31.3 ± 12.6 (17–59) | 0.297 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-W.; Oh, C.-H.; Choi, B.-U.; Hong, H.-J.; Park, J.-H.; Kim, T.-Y.; Cho, Y.-J. Effect of Progressive Head Extension Swallowing Exercise on Lingual Strength in the Elderly: A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 3419. https://doi.org/10.3390/jcm10153419
Park J-W, Oh C-H, Choi B-U, Hong H-J, Park J-H, Kim T-Y, Cho Y-J. Effect of Progressive Head Extension Swallowing Exercise on Lingual Strength in the Elderly: A Randomized Controlled Trial. Journal of Clinical Medicine. 2021; 10(15):3419. https://doi.org/10.3390/jcm10153419
Chicago/Turabian StylePark, Jin-Woo, Chi-Hoon Oh, Bo-Un Choi, Ho-Jin Hong, Joong-Hee Park, Tae-Yeon Kim, and Yong-Jin Cho. 2021. "Effect of Progressive Head Extension Swallowing Exercise on Lingual Strength in the Elderly: A Randomized Controlled Trial" Journal of Clinical Medicine 10, no. 15: 3419. https://doi.org/10.3390/jcm10153419