
Custom 3D-Printed Cutting Guides for Femoral Osteotomy in Rotational Malalignment Due to Diaphyseal Fractures: Surgical Technique and Case Series

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
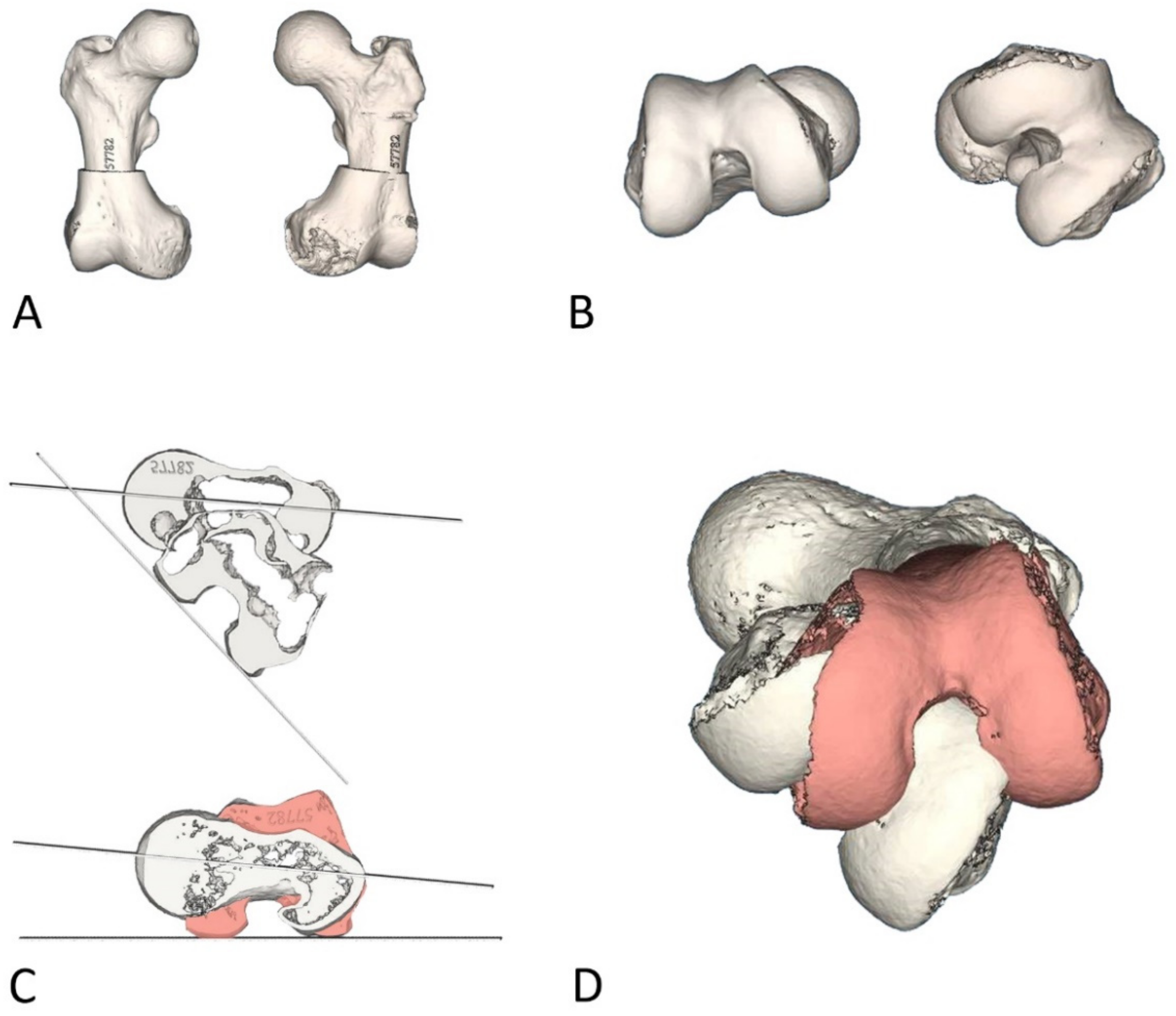
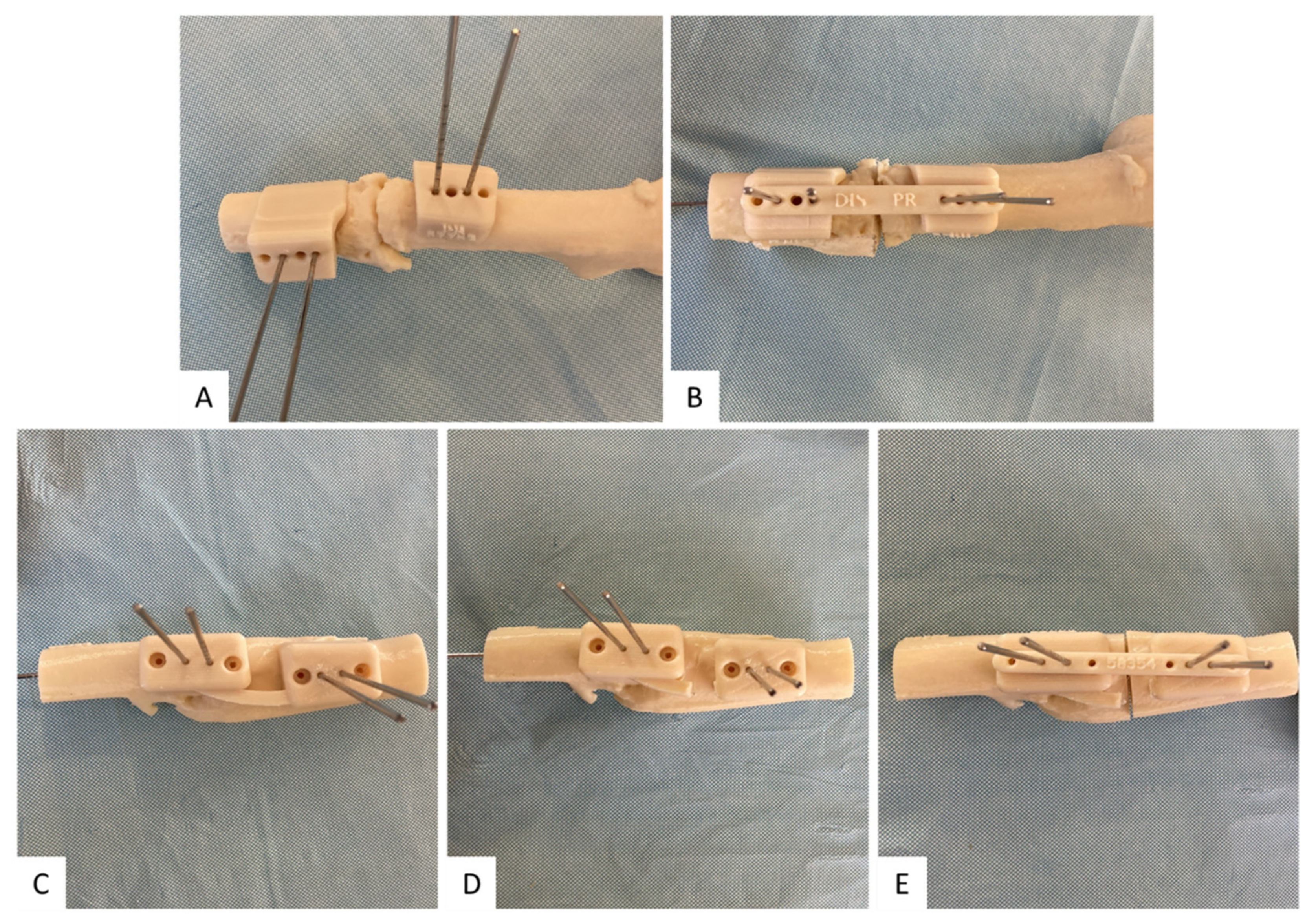
2.2. Design and 3D Printing
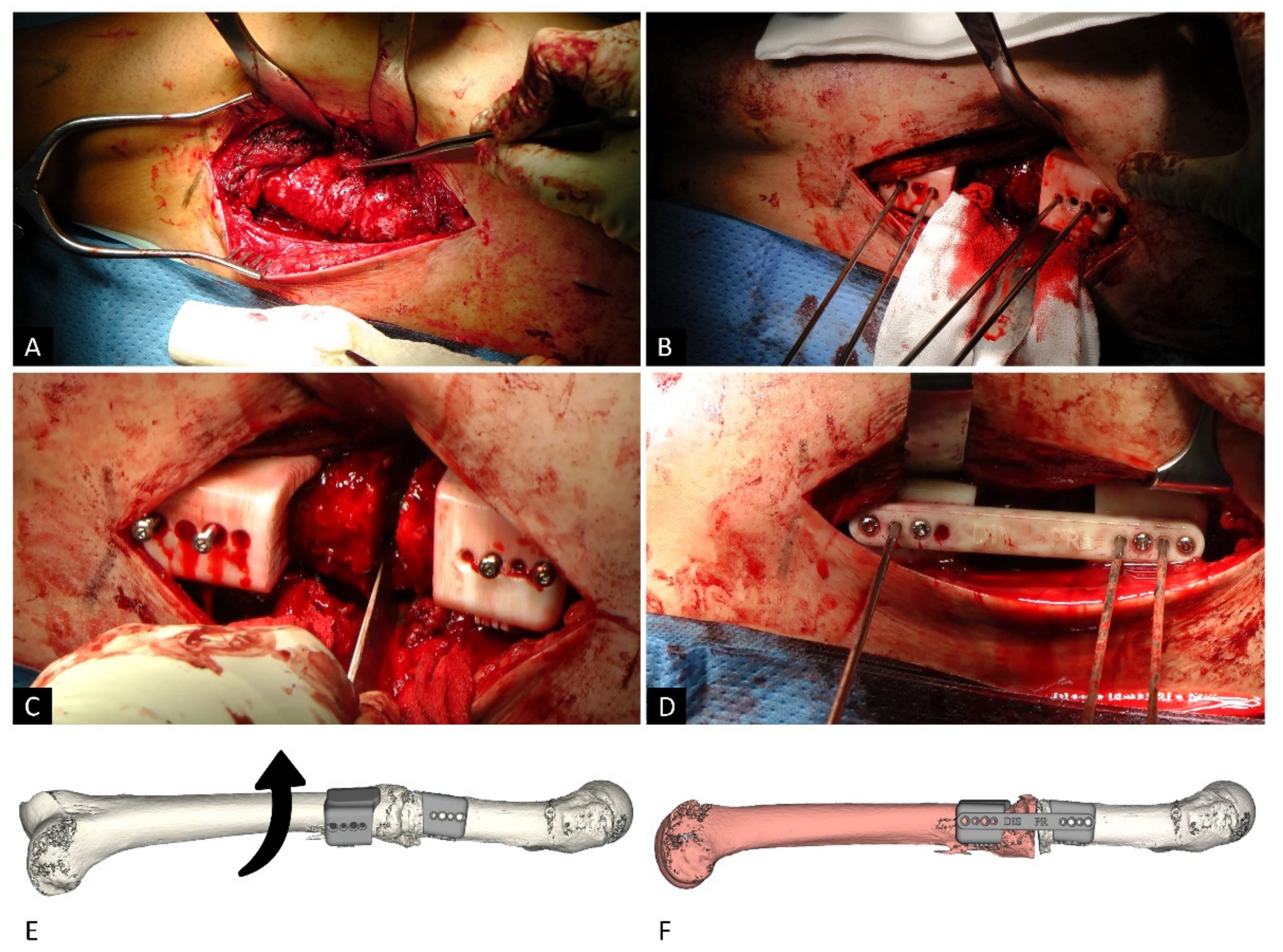
2.3. Surgical Technique
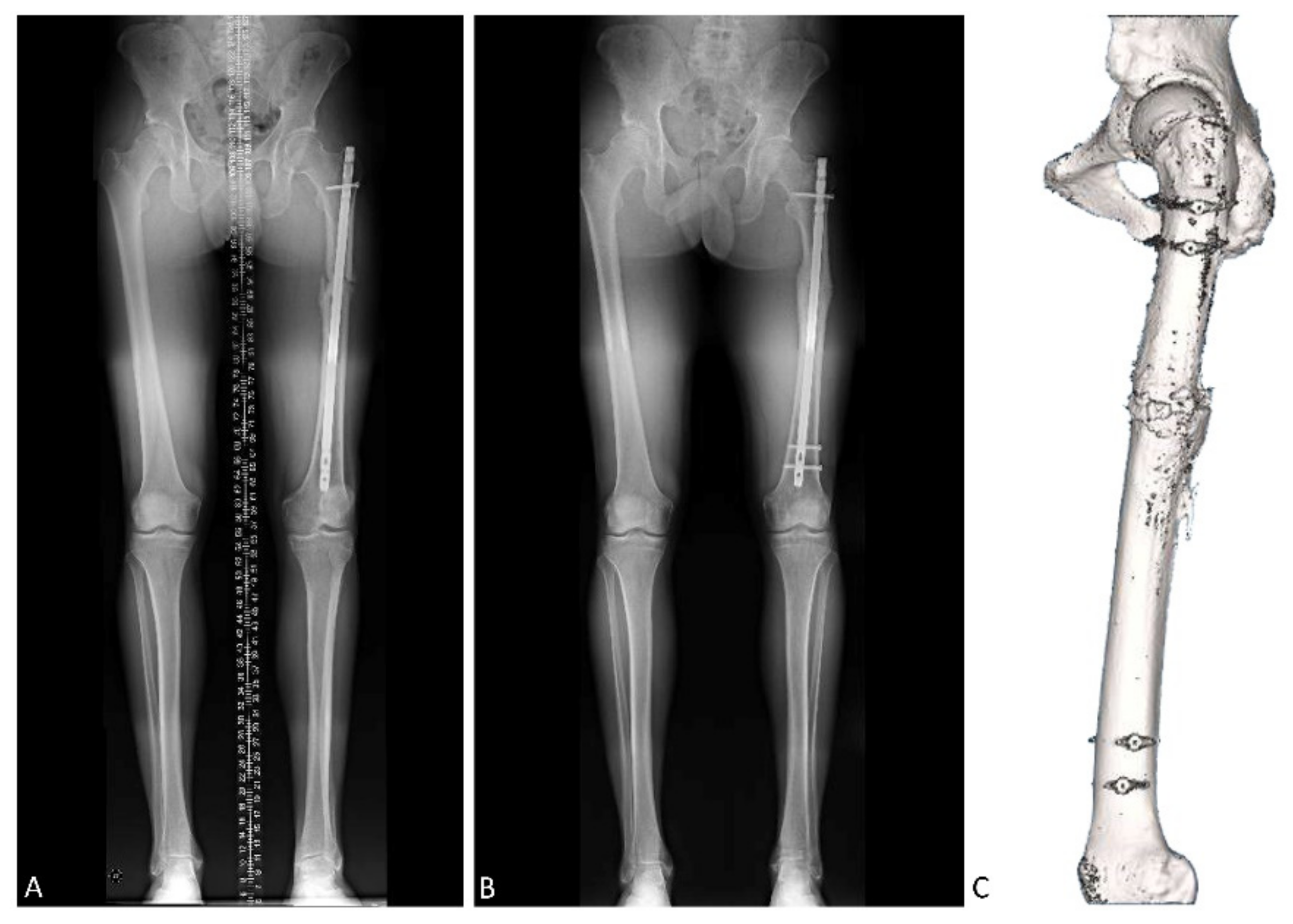
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weiss, R.J.; Montgomery, S.M.; Al Dabbagh, Z.; Jansson, K.-A. National Data of 6409 Swedish Inpatients with Femoral Shaft Fractures: Stable Incidence between 1998 and 2004. Injury 2009, 40, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Enninghorst, N.; McDougall, D.; Evans, J.A.; Sisak, K.; Balogh, Z.J. Population-Based Epidemiology of Femur Shaft Fractures. J. Trauma Acute Care Surg. 2013, 74, 1516–1520. [Google Scholar] [CrossRef] [PubMed]
- Denisiuk, M.; Afsari, A. Femoral Shaft Fractures. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Winquist, R.A.; Hansen, S.T.; Clawson, D.K. Closed Intramedullary Nailing of Femoral Fractures. A Report of Five Hundred and Twenty Cases. 1984. J. Bone Joint Surg. Am. 2001, 83, 1912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bucholz, R.W.; Jones, A. Fractures of the Shaft of the Femur. J. Bone Joint Surg. Am. 1991, 73, 1561–1566. [Google Scholar] [CrossRef]
- Bråten, M.; Terjesen, T.; Rossvoll, I. Femoral Shaft Fractures Treated by Intramedullary Nailing. A Follow-up Study Focusing on Problems Related to the Method. Injury 1995, 26, 379–383. [Google Scholar] [CrossRef]
- Karaman, O.; Ayhan, E.; Kesmezacar, H.; Seker, A.; Unlu, M.C.; Aydingoz, O. Rotational Malalignment after Closed Intramedullary Nailing of Femoral Shaft Fractures and Its Influence on Daily Life. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 1243–1247. [Google Scholar] [CrossRef]
- Jaarsma, R.L.; Pakvis, D.F.M.; Verdonschot, N.; Biert, J.; van Kampen, A. Rotational Malalignment after Intramedullary Nailing of Femoral Fractures. J. Orthop. Trauma 2004, 18, 403–409. [Google Scholar] [CrossRef]
- Hüfner, T.; Citak, M.; Suero, E.M.; Miller, B.; Kendoff, D.; Krettek, C.; Citak, M. Femoral Malrotation after Unreamed Intramedullary Nailing: An Evaluation of Influencing Operative Factors. J. Orthop. Trauma 2011, 25, 224–227. [Google Scholar] [CrossRef]
- Kenawey, M.; Krettek, C.; Ettinger, M.; Hankemeier, S.; Breitmeier, D.; Liodakis, E. The Greater Trochanter-Head Contact Method: A Cadaveric Study with a New Technique for the Intraoperative Control of Rotation of Femoral Fractures. J. Orthop. Trauma 2011, 25, 549–555. [Google Scholar] [CrossRef]
- Stephen, D.J.G.; Kreder, H.J.; Schemitsch, E.H.; Conlan, L.B.; Wild, L.; McKee, M.D. Femoral Intramedullary Nailing: Comparison of Fracture-Table and Manual Traction. A Prospective, Randomized Study. J. Bone Joint Surg. Am. 2002, 84, 1514–1521. [Google Scholar] [CrossRef]
- Jeanmart, L.; Baert, A.L.; Wackenheim, A. Atlas of Pathological Computer Tomography: Volume 3: Computer Tomography of Neck, Chest, Spine and Limbs; Springer: Berlin/Heidelberg, Germany, 1983; ISBN 978-3-642-68538-5. [Google Scholar]
- Wissing, H.; Buddenbrock, B. Determining rotational errors of the femur by axial computerized tomography in comparison with clinical and conventional radiologic determination. Unfallchirurgie 1993, 19, 145–157. [Google Scholar] [CrossRef]
- Fabry, G.; MacEwen, G.D.; Shands, A.R. Torsion of the Femur. A Follow-up Study in Normal and Abnormal Conditions. J. Bone Joint Surg. Am. 1973, 55, 1726–1738. [Google Scholar] [CrossRef]
- Parikh, S.; Noyes, F.R. Patellofemoral Disorders: Role of Computed Tomography and Magnetic Resonance Imaging in Defining Abnormal Rotational Lower Limb Alignment. Sports Health 2011, 3, 158–169. [Google Scholar] [CrossRef] [Green Version]
- Steensen, R.N.; Bentley, J.C.; Trinh, T.Q.; Backes, J.R.; Wiltfong, R.E. The Prevalence and Combined Prevalences of Anatomic Factors Associated with Recurrent Patellar Dislocation: A Magnetic Resonance Imaging Study. Am. J. Sports Med. 2015, 43, 921–927. [Google Scholar] [CrossRef]
- Kitaoka, H.B.; Weiner, D.S.; Cook, A.J.; Hoyt, W.A.; Askew, M.J. Relationship between Femoral Anteversion and Osteoarthritis of the Hip. J. Pediatr. Orthop. 1989, 9, 396–404. [Google Scholar] [CrossRef]
- Tönnis, D.; Heinecke, A. Acetabular and Femoral Anteversion: Relationship with Osteoarthritis of the Hip. J. Bone Joint Surg. Am. 1999, 81, 1747–1770. [Google Scholar] [CrossRef]
- Eckhoff, D.G. Effect of Limb Malrotation on Malalignment and Osteoarthritis. Orthop. Clin. N. Am. 1994, 25, 405–414. [Google Scholar] [CrossRef]
- Terjesen, T.; Benum, P.; Anda, S.; Svenningsen, S. Increased Femoral Anteversion and Osteoarthritis of the Hip Joint. Acta Orthop. Scand. 1982, 53, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Siebenrock, K.A.; Steppacher, S.D.; Haefeli, P.C.; Schwab, J.M.; Tannast, M. Valgus Hip with High Antetorsion Causes Pain Through Posterior Extraarticular FAI. Clin. Orthop. Relat. Res. 2013, 471, 3774–3780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez-Hoyos, J.; Schröder, R.; Reddy, M.; Palmer, I.J.; Martin, H.D. Femoral Neck Anteversion and Lesser Trochanteric Retroversion in Patients With Ischiofemoral Impingement: A Case-Control Magnetic Resonance Imaging Study. Arthroscopy 2016, 32, 13–18. [Google Scholar] [CrossRef]
- Eckhoff, D.G.; Montgomery, W.K.; Kilcoyne, R.F.; Stamm, E.R. Femoral Morphometry and Anterior Knee Pain. Clin. Orthop. Relat. Res. 1994, 64–68. [Google Scholar] [CrossRef]
- Bruce, W.D.; Stevens, P.M. Surgical Correction of Miserable Malalignment Syndrome. J. Pediatr. Orthop. 2004, 24, 392–396. [Google Scholar] [CrossRef]
- MacWilliams, B.A.; McMulkin, M.L.; Davis, R.B.; Westberry, D.E.; Baird, G.O.; Stevens, P.M. Biomechanical Changes Associated with Femoral Derotational Osteotomy. Gait Posture 2016, 49, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Moya, L.; Buly, R.; Henn, F.; Kelly, B.; Ma, Y.; Molisani, D. Femoral Retroversion in Patients with Femoroacetabular Impingement: A Cofactor in the Development of Hip Osteoarthritis. Orthop. Proc. 2010, 92-B, 526. [Google Scholar] [CrossRef]
- Ramme, A.J.; Egol, J.; Chang, G.; Davidovitch, R.I.; Konda, S. Evaluation of Malrotation Following Intramedullary Nailing in a Femoral Shaft Fracture Model: Can a 3D c-Arm Improve Accuracy? Injury 2017, 48, 1603–1608. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, R.G.; Lou, K.K.; Neo, C.B.; Yew, K.S.; Rozman, I.; George, J. A Technique to Obtain Correct Rotational Alignment during Closed Locked Intramedullary Nailing of the Femur. Injury 1998, 29, 207–210. [Google Scholar] [CrossRef]
- Hawi, N.; Kabbani, A.-R.; O’Loughlin, P.; Krettek, C.; Citak, M.; Liodakis, E. Intraoperative Measurement of Femoral Antetorsion Using the Anterior Cortical Angle Method: A Novel Use for Smartphones. Int J. Med. Robot. 2013, 9, 29–35. [Google Scholar] [CrossRef]
- Jaarsma, R.L.; Verdonschot, N.; van der Venne, R.; van Kampen, A. Avoiding Rotational Malalignment after Fractures of the Femur by Using the Profile of the Lesser Trochanter: An in Vitro Study. Arch. Orthop. Trauma Surg. 2005, 125, 184–187. [Google Scholar] [CrossRef]
- Hawi, N.; Liodakis, E.; Suero, E.M.; Stuebig, T.; Citak, M.; Krettek, C. Radiological Outcome and Intraoperative Evaluation of a Computer-Navigation System for Femoral Nailing: A Retrospective Cohort Study. Injury 2014, 45, 1632–1636. [Google Scholar] [CrossRef]
- Lal, H.; Patralekh, M.K. 3D Printing and Its Applications in Orthopaedic Trauma: A Technological Marvel. J. Clin. Orthop. Trauma 2018, 9, 260–268. [Google Scholar] [CrossRef]
- Wong, K.C. 3D-Printed Patient-Specific Applications in Orthopedics. Orthop. Res. Rev. 2016, 8, 57–66. [Google Scholar] [CrossRef] [Green Version]
- Chai, W.; Xu, M.; Zhang, G.; Zhang, L.; Gou, W.; Ni, M.; Chen, J. Computer-Aided Design and Custom-Made Guide in Corrective Osteotomy for Complex Femoral Deformity. J. Huazhong Univ. Sci. Technol. Med. Sci. 2013, 33, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Krettek, C.; Bruns, N. Aktueller Stand und neue Entwicklungen des 3D-Drucks in der Unfallchirurgie. Unfallchirurg 2019, 122, 256–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrés-Cano, P.; Calvo-Haro, J.A.; Fillat-Gomà, F.; Andrés-Cano, I.; Perez-Mañanes, R. Papel del cirujano ortopédico y traumatólogo en la impresión 3D: Aplicaciones actuales y aspectos legales para una medicina personalizada. Rev. Esp. Cir. Ortop. Traumatol. 2021, 65, 138–151. [Google Scholar] [CrossRef]
- Fiz, N.; Delgado, D.; Sánchez, X.; Sánchez, P.; Bilbao, A.M.; Oraa, J.; Sánchez, M. Application of 3D Technology and Printing for Femoral Derotation Osteotomy: Case and Technical Report. Ann. Transl Med. 2017, 5, 400. [Google Scholar] [CrossRef] [Green Version]
- Victor, J.; Premanathan, A. Virtual 3D Planning and Patient Specific Surgical Guides for Osteotomies around the Knee: A Feasibility and Proof-of-Concept Study. Bone Joint J. Bone Joint J. 2013, 95-B, 153–158. [Google Scholar] [CrossRef]
- Krettek, C.; Miclau, T.; Grün, O.; Schandelmaier, P.; Tscherne, H. Intraoperative Control of Axes, Rotation and Length in Femoral and Tibial Fractures. Technical Note. Injury 1998, 29 (Suppl. 3), C29–C39. [Google Scholar] [CrossRef]
- Jagernauth, S.; Tindall, A.J.; Kohli, S.; Allen, P. New Technique: A Novel Femoral Derotation Osteotomy for Malrotation Following Intramedullary Nailing. Case Rep. Orthop. 2012, 2012, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, C.; Sathy, A.K.; Moore, D.S.; Starr, A.J.; Reinert, C.M. Use of Inherent Anteversion of an Intramedullary Nail to Avoid Malrotation in Femur Fractures. J. Orthop. Trauma 2014, 28, e34–e38. [Google Scholar] [CrossRef]
- Stambough, J.B.; Davis, L.; Szymanski, D.A.; Smith, J.C.; Schoenecker, P.L.; Gordon, J.E. Knee Pain and Activity Outcomes After Femoral Derotation Osteotomy for Excessive Femoral Anteversion. J. Pediatr. Orthop. 2018, 38, 503–509. [Google Scholar] [CrossRef]
- Buly, R.L.; Sosa, B.R.; Poultsides, L.A.; Caldwell, E.; Rozbruch, S.R. Femoral Derotation Osteotomy in Adults for Version Abnormalities. J. Am. Acad. Orthop. Surg. 2018, 26, e416–e425. [Google Scholar] [CrossRef]
- Stahl, J.-P.; Alt, V.; Kraus, R.; Hoerbelt, R.; Itoman, M.; Schnettler, R. Derotation of Post-Traumatic Femoral Deformities by Closed Intramedullary Sawing. Injury 2006, 37, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Gérard, R.; Stindel, E.; Moineau, G.; Le Nen, D.; Lefèvre, C. Rotational Femoral Osteotomies Using an Endomedullary Saw. Orthop. Traumatol. Surg. Res. 2009, 95, 414–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosseels, W.; Herteleer, M.; Sermon, A.; Nijs, S.; Hoekstra, H. Corrective Osteotomies Using Patient-Specific 3D-Printed Guides: A Critical Appraisal. Eur. J. Trauma Emerg Surg. 2019, 45, 299–307. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | |
|---|---|---|---|---|---|---|
| Age (years) | 23 | 72 | 40 | 30 | 59 | 35 |
| Sex | Female | Male | Male | Male | Female | Male |
| Side | Left | Left | Left | Right | Right | Left |
| Previous distal femur deformity | Internal rotation | External rotation | External rotation | Internal rotation | External rotation | Internal rotation |
| Pre-angulation (°) | −60 | 40 | 43 | −44 | 1 | −24 |
| Correction (°) | 45 | 50 | 50 | 33 | 15 | 19 |
| Post-angulation (ª) | −15 | −10 | −7 | −11 | −14 | −5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oraa, J.; Beitia, M.; Fiz, N.; González, S.; Sánchez, X.; Delgado, D.; Sánchez, M. Custom 3D-Printed Cutting Guides for Femoral Osteotomy in Rotational Malalignment Due to Diaphyseal Fractures: Surgical Technique and Case Series. J. Clin. Med. 2021, 10, 3366. https://doi.org/10.3390/jcm10153366
Oraa J, Beitia M, Fiz N, González S, Sánchez X, Delgado D, Sánchez M. Custom 3D-Printed Cutting Guides for Femoral Osteotomy in Rotational Malalignment Due to Diaphyseal Fractures: Surgical Technique and Case Series. Journal of Clinical Medicine. 2021; 10(15):3366. https://doi.org/10.3390/jcm10153366
Chicago/Turabian StyleOraa, Jaime, Maider Beitia, Nicolás Fiz, Sergio González, Xabier Sánchez, Diego Delgado, and Mikel Sánchez. 2021. "Custom 3D-Printed Cutting Guides for Femoral Osteotomy in Rotational Malalignment Due to Diaphyseal Fractures: Surgical Technique and Case Series" Journal of Clinical Medicine 10, no. 15: 3366. https://doi.org/10.3390/jcm10153366