
Early Echocardiographic and Cardiac MRI Findings in Multisystem Inflammatory Syndrome in Children

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Echocardiography
2.3. Cardiac MRI
2.4. Statistical Analysis
3. Results
4. Discussion
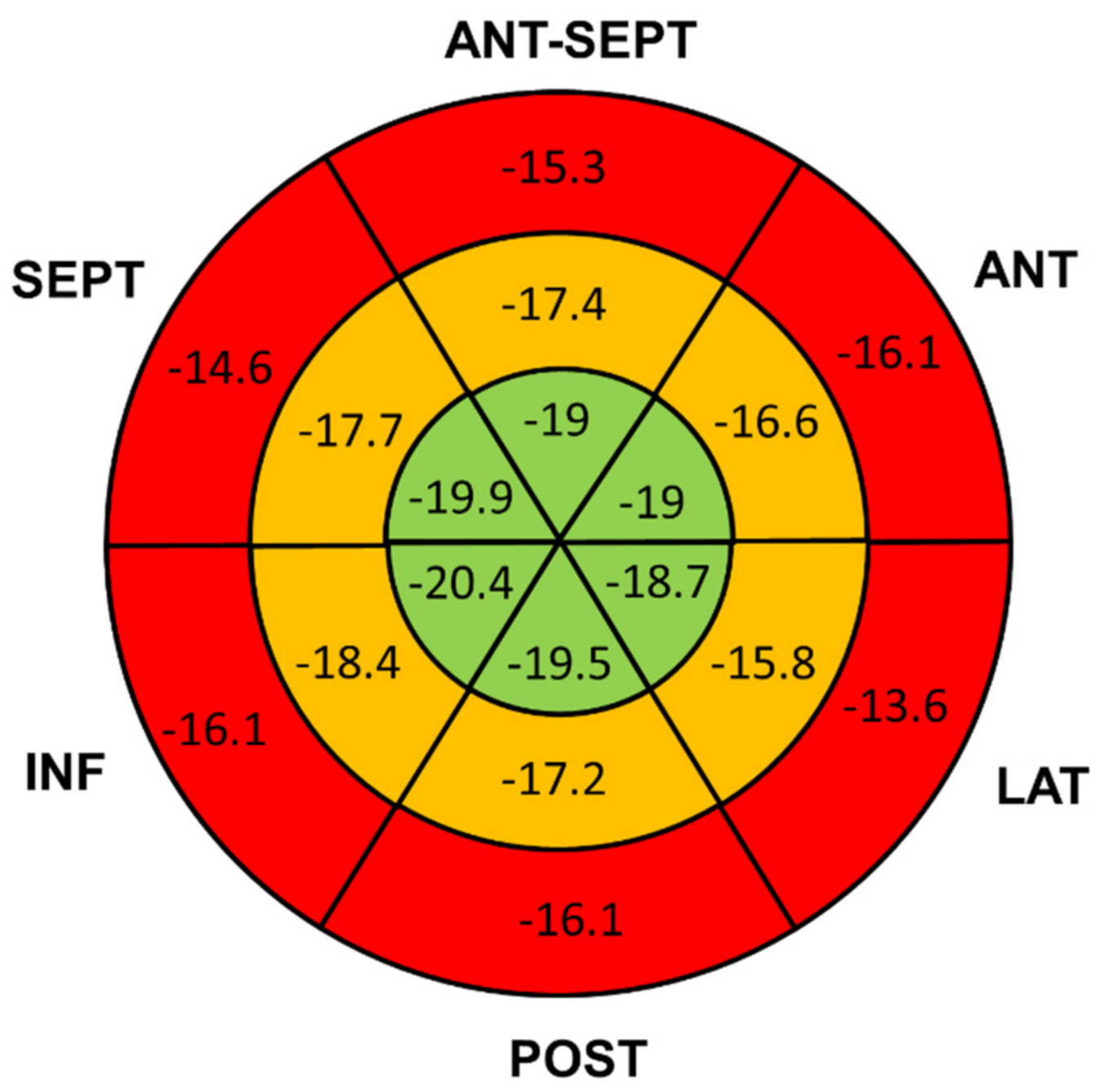
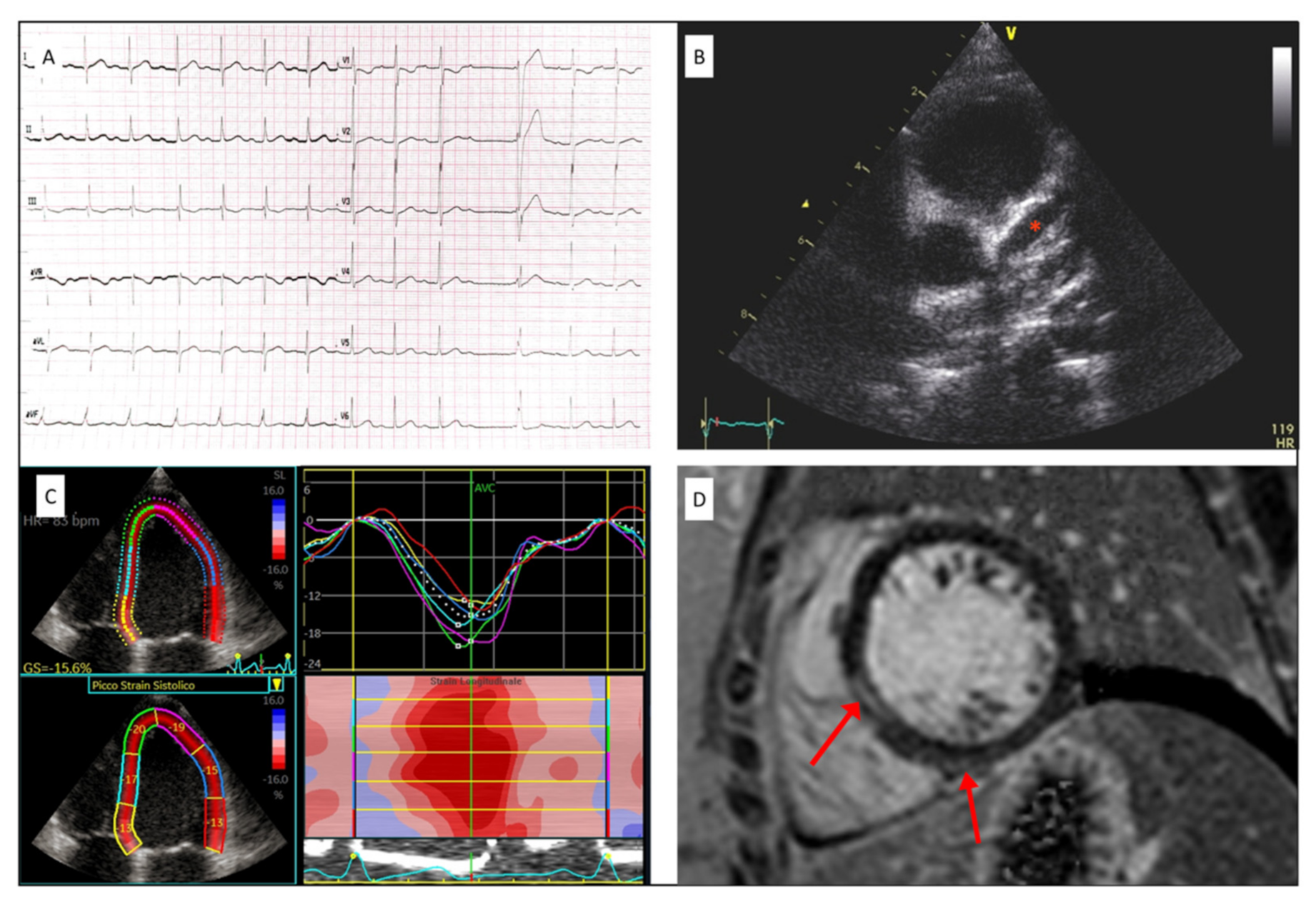
4.1. LV Longitudinal Strain
4.2. Cardiac Magnetic Resonance
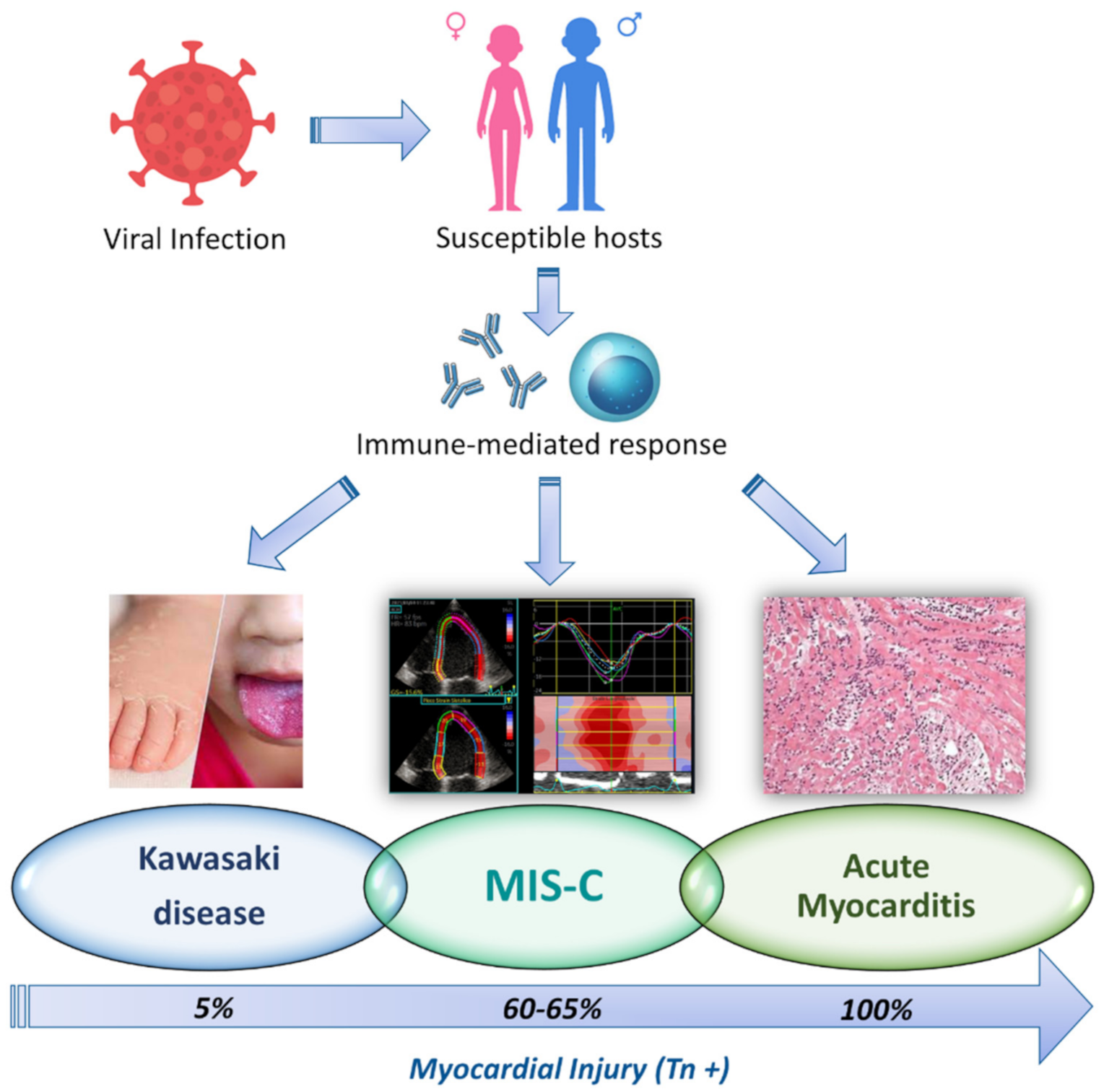
4.3. MIS-C and Kawasaki Disease
4.4. Physiopathologic Hypothesis
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shekerdemian, L.S.; Mahmood, N.R.; Wolfe, K.K.; Riggs, B.J.; Ross, C.E.; McKiernan, C.A.; Heidemann, S.M.; Kleinman, L.C.; Sen, A.I.; Hall, M.W.; et al. Characteristics and Outcomes of Children with Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. JAMA Pediatr. 2020, 174, 868. [Google Scholar] [CrossRef]
- Tagarro, A.; Epalza, C.; Santos, M.; Sanz-Santaeufemia, F.J.; Otheo, E.; Moraleda, C.; Calvo, C. Screening and Severity of Coronavirus Disease 2019 (COVID-19) in Children in Madrid, Spain. JAMA Pediatr. 2020, 175, 316–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parri, N.; Lenge, M.; Buonsenso, D. Coronavirus Infection in Pediatric Emergency Departments (CONFIDENCE) Research Group. Children with Covid-19 in Pediatric Emergency Departments in Italy. N. Engl. J. Med. 2020, 383, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Multisystem Inflammatory Syndrome in Children and Adolescents with COVID-19: Scientific Brief; World Health Organization: Geneva, Switzerland, 15 May 2020; Available online: https://apps.who.int/iris/handle/10665/332095 (accessed on 26 July 2021).
- Hameed, S.; Elbaaly, H.; Reid, C.E.L.; Santos, R.M.F.; Shivamurthy, V.; Wong, J.; Jogeesvaran, K.H. Spectrum of Imaging Findings at Chest Radiography, US, CT, and MRI in Multisystem Inflammatory Syndrome in Children Associated with COVID-19. Radiology 2021, 298, E1–E10. [Google Scholar] [CrossRef] [PubMed]
- Gruber, C.N.; Patel, R.S.; Trachtman, R.; Lepow, L.; Amanat, F.; Krammer, F.; Wilson, K.M.; Onel, K.; Geanon, D.; Tuballes, K.; et al. Mapping Systemic Inflammation and Antibody Responses in Multisystem Inflammatory Syndrome in Children (MIS-C). Cell 2020, 183, 982–995. [Google Scholar] [CrossRef]
- Kwak, J.H.; Lee, S.Y.; Choi, J.W. Korean Society of Kawasaki Disease. Clinical features, diagnosis, and outcomes of multisystem inflammatory syndrome in children associated with coronavirus disease 2019. Clin. Exp. Pediatr. 2021, 64, 68–75. [Google Scholar] [CrossRef]
- Sperotto, F.; Friedman, K.G.; Son, M.B.F.; VanderPluym, C.J.; Newburger, J.W.; Dionne, A. Cardiac manifestations in SARS-CoV-2-associated multisystem inflammatory syndrome in children: A comprehensive review and proposed clinical approach. Eur. J. Pediatr. 2021, 180, 307–322. [Google Scholar] [CrossRef]
- Alsaied, T.; Tremoulet, A.H.; Burns, J.C.; Saidi, A.; Dionne, A.; Lang, S.M.; Newburger, J.W.; de Ferranti, S.; Friedman, K.G. Review of Cardiac Involvement in Multisystem Inflammatory Syndrome in Children. Circulation 2021, 143, 78–88. [Google Scholar] [CrossRef]
- Matsubara, D.; Kauffman, H.L.; Wang, Y.; Calderon-Anyosa, R.; Nadaraj, S.; Elias, M.D.; White, T.J.; Torowicz, D.L.; Yubbu, P.; Giglia, T.M.; et al. Echocardiographic Findings in Pediatric Multisystem Inflammatory Syndrome Associated with COVID-19 in the United States. J. Am. Coll. Cardiol. 2020, 76, 1947–1961. [Google Scholar] [CrossRef]
- Bermejo, I.A.; Bautista-Rodriguez, C.; Fraisse, A.; Voges, I.; Gatehouse, P.; Kang, H.; Piccinelli, E.; Rowlinson, G.; Lane, M.; Semple, T.; et al. Short-Term sequelae of Multisystem Inflammatory Syndrome in Children Assessed by CMR. Cardiovasc. Imaging 2021. [Google Scholar] [CrossRef]
- Henderson, L.A.; Canna, S.W.; Friedman, K.G.; Gorelik, M.; Lapidus, S.K.; Bassiri, H.; Behrens, E.M.; Ferris, A.; Kernan, K.F.; Schulert, G.S.; et al. American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 1. Arthritis Rheumatol. 2020, 72, 1791–1805. [Google Scholar] [CrossRef] [PubMed]
- Zoghbi, W.A.; DiCarli, M.F.; Blankstein, R.; Choi, A.D.; Dilsizian, V.; Flachskampf, F.A.; Geske, J.B.; Grayburn, P.A.; Jaffer, F.A.; Kwong, R.Y.; et al. Multimodality Cardiovascular Imaging in the Midst of the COVID-19 Pandemic. Cardiovasc. Imaging 2020, 13, 1615–1626. [Google Scholar] [CrossRef]
- Sirico, D.; Castaldi, B.; Ciliberti, P.; Sabatino, J.; Cazzoli, I.; Secinaro, A.; Calcaterra, G.; Oreto, L.; Calabrò, M.P.; Chessa, M.; et al. Cardiac imaging in congenital heart disease during the coronavirus disease-2019 pandemic: Recommendations from the Working Group on Congenital Heart Disease of the Italian Society of Cardiology. J. Cardiovasc. Med. 2020, 21, 467–471. [Google Scholar] [CrossRef]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals from the American Heart Association. Circulation 2017, 135, e927–e999. [Google Scholar] [CrossRef]
- Prota, C.; Di Salvo, G.; Sabatino, J.; Josen, M.; Paredes, J.; Sirico, D.; Pernia, M.U.; Hoschtitzky, A.; Michielon, G.; Citro, R.; et al. Prognostic value of echocardiographic parameters in pediatric patients with Ebstein’s anomaly. Int. J. Cardiol. 2019, 278, 76–83. [Google Scholar] [CrossRef]
- Voigt, J.U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. J. Am. Soc. Echocardiogr. 2015, 28, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Sabatino, J.; Di Salvo, G.; Prota, C.; Bucciarelli, V.; Josen, M.; Paredes, J.; Borrelli, N.; Sirico, D.; Prasad, S.; Indolfi, C.; et al. Left Atrial Strain to Identify Diastolic Dysfunction in Children with Cardiomyopathies. J. Clin. Med. 2019, 8, 1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dufort, E.M.; Koumans, E.H.; Chow, E.J.; Rosenthal, E.M.; Muse, A.; Rowlands, J.; Barranco, M.A.; Maxted, A.M.; Rosenberg, E.S.; Easton, D.; et al. Multisystem Inflammatory Syndrome in Children in New York State. N. Engl. J. Med. 2020, 383, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Kabeerdoss, J.; Pilania, R.K.; Karkhele, R.; Kumar, T.S.; Danda, D.; Singh, S. Severe COVID-19, multisystem inflammatory syndrome in children, and Kawasaki disease: Immunological mechanisms, clinical manifestations and management. Rheumatol. Int. 2021, 41, 19–32. [Google Scholar] [CrossRef]
- Kobayashi, R.; Dionne, A.; Ferraro, A.; Harrild, D.; Newburger, J.; VanderPluym, C.; Gauvreau, K.; Son, M.B.; Lee, P.; Baker, A.; et al. Detailed Assessment of Left Ventricular Function in Multisystem Inflammatory Syndrome in Children Using Strain Analysis. CJC Open 2021. [Google Scholar] [CrossRef]
- Feldstein, L.R.; Rose, E.B.; Horwitz, S.M.; Collins, J.P.; Newhams, M.M.; Son, M.B.F.; Newburger, J.W.; Kleinman, L.C.; Heidemann, S.M.; Martin, A.A.; et al. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N. Engl. J. Med. 2020, 383, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Arenas, I.A.; Podesta, C.A.; Issa, O.; Lin, J.; Brenes, J.C. Myocardial longitudinal strain, fitness, and heart failure risk factors in young adults. Echocardiography 2020, 37, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Sirico, D.; Di Chiara, C.; Costenaro, P.; Bonfante, F.; Cozzani, S.; Plebani, M.; Reffo, E.; Castaldi, B.; Donà, D.; Da Dalt, L.; et al. Left ventricular longitudinal strain alterations in asymptomatic or mildly symptomatic paediatric patients with SARS-CoV-2 infection. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 167. [Google Scholar] [CrossRef]
- Civieri, G.; Castaldi, B.; Martini, G.; Meneghel, A.; Milanesi, O.; Zulian, F. Early detection of ventricular dysfunction in juvenile systemic sclerosis by speckle tracking echocardiography. Rheumatology 2021, 60, 103–107. [Google Scholar] [CrossRef]
- Blondiaux, E.; Parisot, P.; Redheuil, A.; Tzaroukian, L.; Levy, Y.; Sileo, C.; Schnuriger, A.; Lorrot, M.; Guedj, R.; Ducou le Pointe, H. Cardiac MRI in Children with Multisystem Inflammatory Syndrome Associated with COVID-19. Radiology 2020, 297, E283–E288. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, E.; Bamford, A.; Kenny, J.; Kaforou, M.; Jones, C.E.; Shah, P.; Ramnarayan, P.; Fraisse, A.; Miller, O.; Davies, P.; et al. Clinical Characteristics of 58 Children with a Pediatric Inflammatory Multisystem Syndrome Temporally Associated With SARS-CoV-2. JAMA 2020, 324, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Falcini, F.; Cimaz, R.; Calabri, G.B.; Picco, P.; Martini, G.; Marazzi, M.G.; Simonini, G.; Zulian, F. Kawasaki’s disease in northern Italy: A multicenter retrospective study of 250 patients. Clin. Exp. Rheumatol. 2002, 20, 421–426. [Google Scholar]
- Reffo, E.; Stritoni, V.; Di Salvo, G. Inflammatory syndrome in children associated with COVID-19 complicated by acute myocardial infarction. Eur. Heart J. 2021. [Google Scholar] [CrossRef]
- Ramcharan, T.; Nolan, O.; Lai, C.Y.; Prabhu, N.; Krishnamurthy, R.; Richter, A.G.; Jyothish, D.; Kanthimathinathan, H.K.; Welch, S.B.; Hackett, S.; et al. Paediatric Inflammatory Multisystem Syndrome: Temporally Associated with SARS-CoV-2 (PIMS-TS): Cardiac Features, Management and Short-Term Outcomes at a UK Tertiary Paediatric Hospital. Pediatr. Cardiol. 2020, 41, 1391–1401. [Google Scholar] [CrossRef]
- Pouletty, M.; Borocco, C.; Ouldali, N.; Caseris, M.; Basmaci, R.; Lachaume, N.; Bensaid, P.; Pichard, S.; Kouider, H.; Morelle, G.; et al. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): A multicentre cohort. Ann. Rheum. Dis. 2020, 79, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Kumrah, R.; Vignesh, P.; Rawat, A.; Singh, S. Immunogenetics of Kawasaki disease. Clinic. Rev. Allerg. Immunol. 2020, 59, 122–139. [Google Scholar] [CrossRef]
- Rowley, A.H.; Baker, S.C.; Shulman, S.T.; Rand, K.H.; Tretiakova, M.S.; Perlman, E.J.; Garcia, F.L.; Tajuddin, N.F.; Fox, L.M.; Huang, J.H.; et al. Ultrastructural, immunofluorescence, and RNA evidence support the hypothesis of a “new” virus associated with Kawasaki disease. J. Infect. Dis. 2011, 203, 1021–1030. [Google Scholar] [CrossRef] [PubMed]
- Elakabawi, K.; Lin, J.; Jiao, F.; Guo, N.; Yuan, Z. Kawasaki Disease: Global Burden and Genetic Background. Cardiol. Res. 2020, 11. [Google Scholar] [CrossRef] [Green Version]
- Ammirati, E.; Frigerio, M.; Adler, E.D.; Basso, C.; Birnie, D.H.; Brambatti, M.; Friedrich, M.G.; Klingel, K.; Lehtonen, J.; Moslehi, J.J.; et al. Management of Acute Myocarditis and Chronic Inflammatory Cardiomyopathy: An Expert Consensus Document. Circ. Heart Fail. 2020, 13, e007405. [Google Scholar] [CrossRef]
- Ammirati, E.; Veronese, G.; Bottiroli, M.; Wang, D.W.; Cipriani, M.; Garascia, A.; Pedrotti, P.; Adler, E.D.; Frigerio, M. Update on acute myocarditis. Trends Cardiovasc. Med. 2020, 31. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MIS-C Patients (n = 23) | |
|---|---|
| Age at onset (years) | 8.1 ± 4 |
| Male | 13 (56) |
| Comorbidities | 2 (8.7) |
| Associated CHD | 1 bicuspid aortic valve |
| positive SARS-CoV-2 NP swab | 4 (17) |
| positive SARS-CoV-2 IgG title | 18 (78) |
| CLINICAL MANIFESTATIONS | |
| Fever | 23 (100) |
| GI | 19 (82) |
| Muco-cutaneous | 19 (82) |
| Neurological | 6 (26) |
| Hypotension | 7 (30) |
| Sinus bradycardia | 7 (30) |
| KD like | 9 (39) |
| ICU admission | 4 (17) |
| LABORATORY | |
| TnI ≤ 34 ng/L | 8 (35) |
| TnI > 34 ng/L | 15 (65) |
| BNP (pg/mL) | 581 ± 736 |
| CRP (mg/L) | 181 ± 94.4 |
| PCT (ng/mL) | 53 ± 102 |
| ESR (mm/h) | 57.9 ± 36.2 |
| Ferritin (mcg/L) | 882.8 ± 662.8 |
| D-dimer (mcg/mL) | 2311.6 ± 2853 |
| LDH (U/L) | 336.6 ± 93 |
| MIS-C Patients (n = 23) | |
|---|---|
| EKG | |
| EKG abnormalities | 11 (48) |
| Ripolarization abnormalities | 8 (35) |
| Sinus bradycardia | 7 (30) |
| AV block | 2 (9) |
| ECHOCARDIOGRAPHY | |
| LVEF (%) | 59 ± 10 |
| GLS (%) | −17 ± 4.3 |
| E/A ratio | 1.9 ± 0.5 |
| Deceleration time (msec) | 147 ± 31 |
| Averaged E/e’ ratio | 8 ± 2.1 |
| TAPSE (mm) | 18.8 ± 4.7 |
| RV FAC (%) | 45 ± 7 |
| coronary dilatation | 6 (26) |
| coronary thrombosis | 1 (4) |
| pericardial effusion | 6 (26) |
| CARDIAC MRI (n = 17/23) | |
| LVEF | 60 ± 13 |
| LV edema | 1 (4) |
| LV LGE | 6 (26) |
| RVEF | 62.8 ± 3.9 |
| TnI+ (n = 15) | TnI− (n = 8) | p-Value | |
|---|---|---|---|
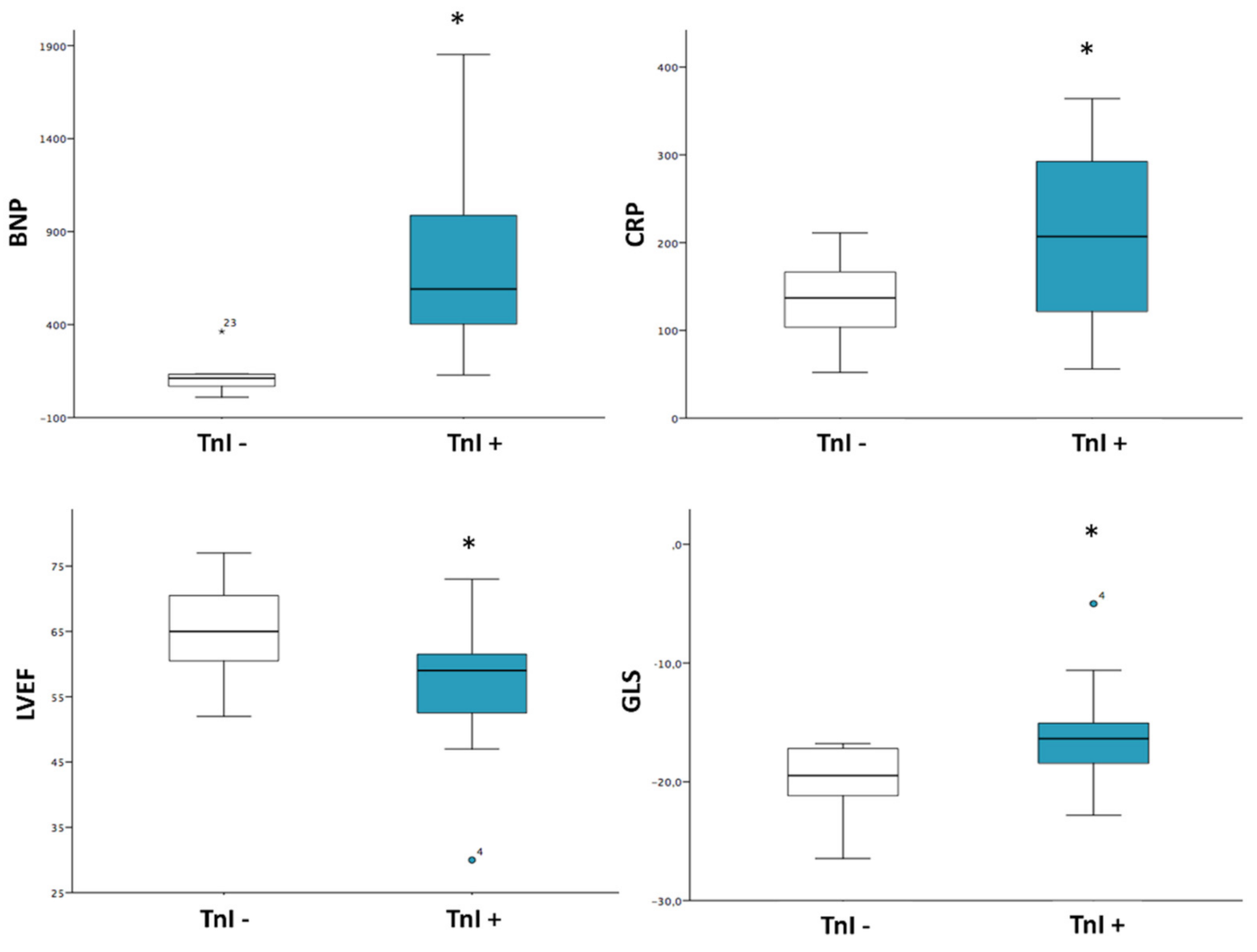
| BNP (pc/mL) | 824 ± 815 | 125 ± 105 | 0.03 * |
| CRP (mg/L) | 205 ± 104 | 135 ± 49 | 0.038 * |
| PCT (ng/mL) | 62.6 ± 118 | 31.1 ± 44.8 | 0.54 |
| ESR (mm/h) | 62 ± 36 | 49 ± 37 | 0.42 |
| D-dimer (mcg/mL) | 2032 ± 3112 | 2834 ± 2394 | 0.53 |
| SARS-CoV-2 Ig title (kAU/L) | 11.6 ± 28.1 | 10.3 ± 8.6 | 0.90 |
| echo LVEF (%) | 56 ± 10 | 65 ± 8 | 0.04 * |
| GLS (%) | −16.1 ± 4.2 | −19.8 ± 3.2 | 0.04 * |
| E/A ratio | 1.99 ± 0.51 | 1.9 ± 0.54 | 0.70 |
| Averaged E/e’ ratio | 8.2 ± 1.8 | 7.7 ± 2.6 | 0.64 |
| TAPSE (mm) | 20 ± 4.9 | 16.4 ± 3.4 | 0.09 |
| RV FAC (%) | 46 ± 8.2 | 44 ± 4.9 | 0.63 |
| coronary dilatation | 6 (40) | 2 (25) | 0.47 (X2 0.52, p 0.65 FET) |
| pericardial effusion | 3 (20) | 3 (37) | 0.36 (X2 0.82) |
| CMR (n = 17) | TnI+ (n = 13) | TnI − (n = 4) | p-Value |
| CMR LVEF (%) | 59.4 ± 11.4 | 64 ± 1.3 | 0.38 |
| CMR LV LGE | 4 (30) | 2 (50) | 0.91 (X2 0.01, p 0.58 FET) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sirico, D.; Basso, A.; Reffo, E.; Cavaliere, A.; Castaldi, B.; Sabatino, J.; Meneghel, A.; Martini, G.; Da Dalt, L.; Zulian, F.; et al. Early Echocardiographic and Cardiac MRI Findings in Multisystem Inflammatory Syndrome in Children. J. Clin. Med. 2021, 10, 3360. https://doi.org/10.3390/jcm10153360
Sirico D, Basso A, Reffo E, Cavaliere A, Castaldi B, Sabatino J, Meneghel A, Martini G, Da Dalt L, Zulian F, et al. Early Echocardiographic and Cardiac MRI Findings in Multisystem Inflammatory Syndrome in Children. Journal of Clinical Medicine. 2021; 10(15):3360. https://doi.org/10.3390/jcm10153360
Chicago/Turabian StyleSirico, Domenico, Alessia Basso, Elena Reffo, Annachiara Cavaliere, Biagio Castaldi, Jolanda Sabatino, Alessandra Meneghel, Giorgia Martini, Liviana Da Dalt, Francesco Zulian, and et al. 2021. "Early Echocardiographic and Cardiac MRI Findings in Multisystem Inflammatory Syndrome in Children" Journal of Clinical Medicine 10, no. 15: 3360. https://doi.org/10.3390/jcm10153360