
Selective Laser Trabeculoplasty in the Treatment of Ocular Hypertension and Open-Angle Glaucoma: Clinical Review

 ,
,
Abstract
:1. Introduction
2. Methods
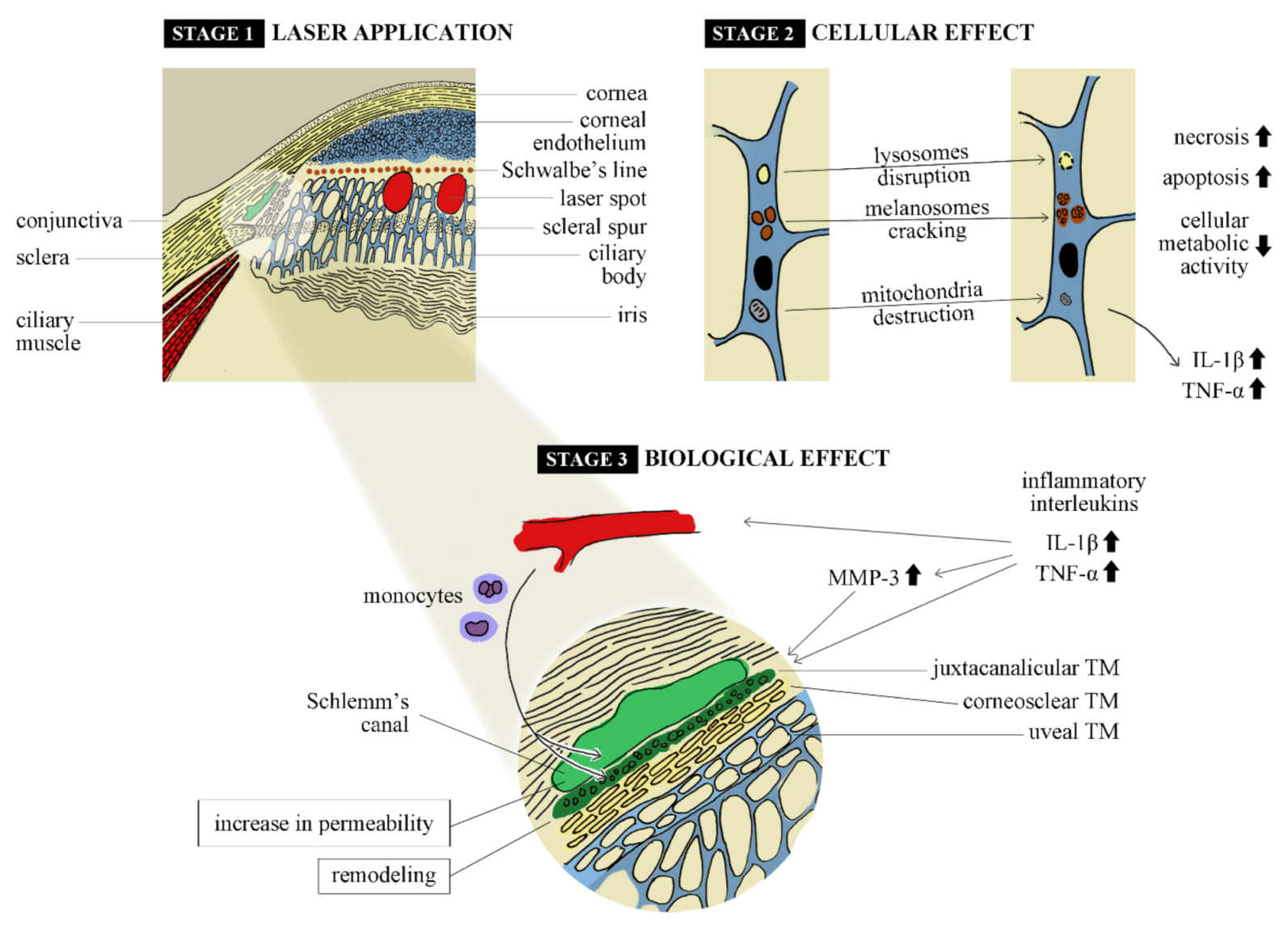
3. Mechanisms of Action
3.1. Cellular and Histopathological Changes
3.2. Biological Changes
4. Technique
5. Postoperative Treatment
5.1. Anti-inflammatory Therapy
5.2. Preventing IOP Spikes
5.3. Conclusions
6. Efficacy of Treatment
6.1. SLT as First-line Therapy
6.2. Replacement Therapy
6.3. Adjunctive Therapy
6.4. Young Patients
6.5. Exfoliative Glaucoma (XFG)
6.6. Pigmentary Glaucoma
6.7. Advanced Glaucoma
- Reduction in IOP to <21 mmHg and >20% compared with the baseline (achieved in 26 eyes, 59.1%);
- IOP reduction to <18 mmHg with no additional medication at all time points after SLT (achieved in 29 eyes, 65.9%);
- IOP reduction to <18 mmHg and >30% of baseline (achieved in 22 eyes, 50%);
- The number of eyes that underwent incisional surgery within 12 months after SLT (occurred in 8 eyes).
6.8. Angle Closure
7. Predictive Factors
8. Repeatability
9. Complications
9.1. IOP Spikes
9.2. Anterior Chamber Inflammation
9.3. Eye pain, Discomfort and Redness
9.4. Peripheral Anterior Synechiae
9.5. Corneal Adverse Events
9.6. Other
10. Summary
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heijl, A. Reduction of Intraocular Pressure and Glaucoma Progression: Results From the Early Manifest Glaucoma Trial. Arch. Ophthalmol. 2002, 120, 1268. [Google Scholar] [CrossRef]
- Agis Investigators. The advanced glaucoma intervention study (AGIS): 7. the relationship between control of intraocular pressure and visual field deterioration. Am. J. Ophthalmol. 2000, 130, 429–440. [Google Scholar] [CrossRef]
- Latina, M.A.; Park, C. Selective targeting of trabecular meshwork cells: In vitro studies of pulsed and CW laser interactions. Exp. Eye Res. 1995, 60, 359–371. [Google Scholar] [CrossRef]
- Kramer, T.R.; Noecker, R.J. Comparison of the morphologic changes after selective laser trabeculoplasty and argon laser trabeculoplasty in human eye bank eyes. Ophthalmology 2001, 108, 773–779. [Google Scholar] [CrossRef]
- Latina, M.A.; Sibayan, S.A.; Shin, D.H.; Noecker, R.J.; Marcellino, G. Q-switched 532-nm Nd:YAG laser trabeculoplasty (selective laser trabeculoplasty): A multicenter, pilot, clinical study11Dr. Mark A. Latina has financial interest in this technology. Ophthalmology 1998, 105, 2082–2090. [Google Scholar] [CrossRef]
- Mäepea, O.; Bill, A. Pressures in the juxtacanalicular tissue and Schlemm’s canal in monkeys. Exp. Eye Res. 1992, 54, 879–883. [Google Scholar] [CrossRef]
- SooHoo, J.R.; Seibold, L.K.; Ammar, D.A.; Kahook, M.Y. Ultrastructural Changes in Human Trabecular Meshwork Tissue after Laser Trabeculoplasty. J. Ophthalmol. 2015, 2015, 476138. [Google Scholar] [CrossRef]
- Bradley, J.M.; Anderssohn, A.M.; Colvis, C.M.; Parshley, D.E.; Zhu, X.H.; Ruddat, M.S.; Samples, J.R.; Acott, T.S. Mediation of laser trabeculoplasty-induced matrix metalloproteinase expression by IL-1beta and TNFalpha. Investig. Ophthalmol. Vis. Sci. 2000, 41, 422–430. [Google Scholar]
- Parshley, D.E.; Bradley, J.M.; Fisk, A.; Hadaegh, A.; Samples, J.R.; Van Buskirk, E.M.; Acott, T.S. Laser trabeculoplasty induces stromelysin expression by trabecular juxtacanalicular cells. Investig. Ophthalmol. Vis. Sci. 1996, 37, 795–804. [Google Scholar]
- Lee, J.Y.; Kagan, D.B.; Roumeliotis, G.; Liu, H.; Hutnik, C.M. Secretion of matrix metalloproteinase-3 by co-cultured pigmented and non-pigmented human trabecular meshwork cells following selective laser trabeculoplasty. Clin. Exp. Ophthalmol. 2016, 44, 33–42. [Google Scholar] [CrossRef]
- Alvarado, J.A.; Katz, L.J.; Trivedi, S.; Shifera, A.S. Monocyte modulation of aqueous outflow and recruitment to the trabecular meshwork following selective laser trabeculoplasty. Arch. Ophthalmol. 2010, 128, 731–737. [Google Scholar] [CrossRef] [Green Version]
- Alvarado, J.A.; Iguchi, R.; Martinez, J.; Trivedi, S.; Shifera, A.S. Similar effects of selective laser trabeculoplasty and prostaglandin analogs on the permeability of cultured Schlemm canal cells. Am. J. Ophthalmol. 2010, 150, 254–264. [Google Scholar] [CrossRef]
- Gazzard, G.; Konstantakopoulou, E.; Garway-Heath, D.; Garg, A.; Vickerstaff, V.; Hunter, R.; Ambler, G.; Bunce, C.; Wormald, R.; Nathwani, N.; et al. Selective laser trabeculoplasty versus drops for newly diagnosed ocular hypertension and glaucoma: The LiGHT RCT. Health Technol. Assess. 2019, 23, 1. [Google Scholar] [CrossRef] [PubMed]
- Gazzard, G.; Konstantakopoulou, E.; Garway-Heath, D.; Garg, A.; Vickerstaff, V.; Hunter, R.; Ambler, G.; Bunce, C.; Wormald, R.; Nathwani, N.; et al. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): A multicentre randomised controlled trial. Lancet 2019, 393, 1505–1516. [Google Scholar] [CrossRef] [Green Version]
- Ang, G.S.; Fenwick, E.K.; Constantinou, M.; Gan, A.T.L.; Man, R.E.K.; Casson, R.J.; Finkelstein, E.A.; Goldberg, I.; Healey, P.R.; Pesudovs, K.; et al. Selective laser trabeculoplasty versus topical medication as initial glaucoma treatment: The glaucoma initial treatment study randomised clinical trial. Br. J. Ophthalmol. 2020, 104, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; Golchin, S.; Blomdahl, S. A Comparison Between 90° and 180° Selective Laser Trabeculoplasty. J. Glaucoma 2004, 13, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Beltran-Agullo, L.; Rashid, S.; Shah, S.P.; Nath, R.; Obi, A.; Lim, K.S. Effect of primary selective laser trabeculoplasty on tonographic outflow facility: A randomised clinical trial. Br. J. Ophthalmol. 2010, 94, 1443–1447. [Google Scholar] [CrossRef]
- Shibata, M.; Sugiyama, T.; Ishida, O.; Ueki, M.; Kojima, S.; Okuda, T.; Ikeda, T. Clinical Results of Selective Laser Trabeculoplasty in Open-angle Glaucoma in Japanese Eyes: Comparison of 180 Degree with 360 Degree SLT. J. Glaucoma 2012, 21, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Francis, B.A.; Loewen, N.; Hong, B.; Dustin, L.; Kaplowitz, K.; Kinast, R.; Bacharach, J.; Radhakrishnan, S.; Iwach, A.; Rudavska, L.; et al. Repeatability of selective laser trabeculoplasty for open-angle glaucoma. BMC Ophthalmol. 2016, 16, 128. [Google Scholar] [CrossRef] [Green Version]
- Tawfique, K.; Khademi, P.; Quérat, L.; Khadamy, J.; Chen, E. Comparison between 90-degree and 360-degree selective laser trabeculoplasty (SLT): A 2-year follow-up. Acta Ophthalmol. 2019, 97, 427–429. [Google Scholar] [CrossRef]
- Özen, B.; Öztürk, H.; Yüce, B. Comparison of the effects of 180° and 360° applications of selective laser trabeculoplasty on intraocular pressure and cornea. Int. Ophthalmol. 2020, 40, 1103–1110. [Google Scholar] [CrossRef] [PubMed]
- Nirappel, A.; Klug, E.; Ye, R.; Hall, N.; Chachanidze, M.; Chang, T.C.; Solá-Del Valle, D. Effectiveness of Selective Laser Trabeculoplasty Applied to 360° vs. 180° of the Angle. J. Ophthalmol. 2021, 2021. [Google Scholar] [CrossRef] [PubMed]
- Groth, S.L.; Albeiruti, E.; Nunez, M.; Fajardo, R.; Sharpsten, L.; Loewen, N.; Schuman, J.S.; Goldberg, J.L. SALT Trial: Steroids after Laser Trabeculoplasty: Impact of Short-Term Anti-inflammatory Treatment on Selective Laser Trabeculoplasty Efficacy. Ophthalmology 2019, 126, 1511–1516. [Google Scholar] [CrossRef]
- Jinapriya, D.; D’Souza, M.; Hollands, H.; El-Defrawy, S.R.; Irrcher, I.; Smallman, D.; Farmer, J.P.; Cheung, J.; Urton, T.; Day, A.; et al. Anti-inflammatory therapy after selective laser trabeculoplasty: A randomized, double-masked, placebo-controlled clinical trial. Ophthalmology 2014, 121, 2356–2361. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.; Vickerstaff, V.; Nathwani, N.; Garway-Heath, D.; Konstantakopoulou, E.; Ambler, G.; Bunce, C.; Wormald, R.; Barton, K.; Gazzard, G.; et al. Primary Selective Laser Trabeculoplasty for Open-Angle Glaucoma and Ocular Hypertension: Clinical Outcomes, Predictors of Success, and Safety from the Laser in Glaucoma and Ocular Hypertension Trial. Ophthalmology 2019, 126, 1238–1248. [Google Scholar] [CrossRef] [Green Version]
- De Keyser, M.; De Belder, M.; De Groot, V. Randomized Prospective Study of the Use of Anti-Inflammatory Drops After Selective Laser Trabeculoplasty. J. Glaucoma 2017, 26, e22–e29. [Google Scholar] [CrossRef] [PubMed]
- Rebenitsch, R.L.; Brown, E.N.; Binder, N.R.; Jani, A.; Bonham, A.J.; Krishna, R.; Pikey, K. Effect of topical loteprednol on intraocular pressure after selective laser trabeculoplasty for open-angle glaucoma. Ophthalmol. Ther. 2013, 2, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Wong, M.O.M.; Lee, J.W.Y.; Choy, B.N.K.; Chan, J.C.H.; Lai, J.S.M. Systematic review and meta-analysis on the efficacy of selective laser trabeculoplasty in open-angle glaucoma. Surv. Ophthalmol. 2015, 60, 36–50. [Google Scholar] [CrossRef]
- Zhang, L.; Weizer, J.S.; Musch, D.C. Perioperative medications for preventing temporarily increased intraocular pressure after laser trabeculoplasty. Cochrane Database Syst. Rev. 2017, CD010746. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Garg, A.; Vickerstaff, V.; Nathwani, N.; Garway-Heath, D.; Konstantakopoulou, E.; Ambler, G.; Bunce, C.; Wormald, R.; Barton, K.; Gazzard, G. Efficacy of Repeat Selective Laser Trabeculoplasty in Medication-Naive Open-Angle Glaucoma and Ocular Hypertension during the LiGHT Trial. Ophthalmology 2020, 127, 467–476. [Google Scholar] [CrossRef] [Green Version]
- Chi, S.C.; Kang, Y.-N.; Hwang, D.-K.; Liu, C.J. Selective laser trabeculoplasty versus medication for open-angle glaucoma: Systematic review and meta-analysis of randomised clinical trials. Br. J. Ophthalmol. 2020, 104, 1500–1507. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.S.M.; Chua, J.K.H.; Tham, C.C.Y.; Lam, D.S.C. Five-year follow up of selective laser trabeculoplasty in Chinese eyes. Clin. Exp. Ophthalmol. 2004, 32, 368–372. [Google Scholar] [CrossRef]
- Nagar, M.; Luhishi, E.; Shah, N. Intraocular pressure control and fluctuation: The effect of treatment with selective laser trabeculoplasty. Br. J. Ophthalmol. 2009, 93, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Kiddee, W.; Atthavuttisilp, S. The effects of selective laser trabeculoplasty and travoprost on circadian intraocular pressure fluctuations. Medicine 2017, 96. [Google Scholar] [CrossRef] [PubMed]
- Ansari, E. 10-year outcomes of first-line selective laser trabeculoplasty (SLT) for primary open-angle glaucoma (POAG). Graefe’s Arch. Clin. Exp. Ophthalmol. 2021. [Google Scholar] [CrossRef]
- Sakata, R.; Shirato, S.; Miyata, K.; Aihara, M. Incidence of deepening of the upper eyelid sulcus in prostaglandin-associated periorbitopathy with a latanoprost ophthalmic solution. Eye 2014, 28, 1446–1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stapleton, F.; Alves, M.; Bunya, V.Y.; Jalbert, I.; Lekhanont, K.; Malet, F.; Na, K.-S.; Schaumberg, D.; Uchino, M.; Vehof, J.; et al. TFOS DEWS II Epidemiology Report. Ocul. Surf. 2017, 15, 334–365. [Google Scholar] [CrossRef]
- Filippopoulos, T.; Paula, J.S.; Torun, N.; Hatton, M.P.; Pasquale, L.R.; Grosskreutz, C.L. Periorbital changes associated with topical bimatoprost. Ophthalmic Plast. Reconstr. Surg. 2008, 24, 302–307. [Google Scholar] [CrossRef]
- Francis, B.A.; Ianchulev, T.; Schofield, J.K.; Minckler, D.S. Selective laser trabeculoplasty as a replacement for medical therapy in open-angle glaucoma. Am. J. Ophthalmol. 2005, 140, 524–525. [Google Scholar] [CrossRef] [PubMed]
- Tufan, A.K.; Onur, İ.U.; Yiğit, F.U.; Ağaçhan, A.; Aşık Nacaroğlu, Ş. Selective Laser Trabeculoplasty vs. Fixed Combinations with Timolol in Practice: A Replacement Study in Primary Open Angle Glaucoma. Turk. J. Ophthalmol. 2017, 47, 198–204. [Google Scholar] [CrossRef] [PubMed]
- De Keyser, M.; De Belder, M.; De Belder, J.; De Groot, V. Selective laser trabeculoplasty as replacement therapy in medically controlled glaucoma patients. Acta Ophthalmol. 2018, 96, e577–e581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Keyser, M.; De Belder, M.; De Groot, V. Quality of life in glaucoma patients after selective laser trabeculoplasty. Int. J. Ophthalmol. 2017, 10, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; El Hawy, E.; Waisbourd, M.; Zangalli, C.; Shapiro, D.M.; Gupta, L.; Hsieh, M.; Kasprenski, A.; Katz, L.J.; Spaeth, G.L. Long-term outcomes in patients initially responsive to selective laser trabeculoplasty. Int. J. Ophthalmol. 2015, 8, 960–964. [Google Scholar] [CrossRef]
- Khawaja, A.P.; Campbell, J.H.; Kirby, N.; Chandwani, H.S.; Keyzor, I.; Parekh, M.; McNaught, A.I.; Vincent, D.; Angela, K.; Nitin, A.; et al. Real-World Outcomes of Selective Laser Trabeculoplasty in the United Kingdom. Ophthalmology 2020, 127, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Ghosh, S.; Sujeeth, M.; Chaudhary, S.; Gupta, S.; Chaurasia, A.K.; Sihota, R.; Gupta, A.; Kapoor, K.S. Selective laser trabeculoplasty for primary open-angle glaucoma patients younger than 40 years. Can. J. Ophthalmol. 2018, 53, 81–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, D.; Chen, D.; Tan, Q.; Xia, X.; Jiang, H.; Jiang, J. Outcome of Selective Laser Trabeculoplasty in Young Patients with Primary Open-Angle Glaucoma and Ocular Hypertension. J. Ophthalmol. 2020, 2020, 5742832. [Google Scholar] [CrossRef]
- Shazly, T.A.; Smith, J.; Latina, M.A. Long-term safety and efficacy of selective laser trabeculoplasty as primary therapy for the treatment of pseudoexfoliation glaucoma compared with primary open-angle glaucoma. Clin. Ophthalmol. 2011, 5, 5–10. [Google Scholar] [CrossRef] [Green Version]
- Belitsky, Y.; Škiljić, D.; Zetterberg, M.; Kalaboukhova, L. Evaluation of selective laser trabeculoplasty as an intraocular pressure lowering option. Acta Ophthalmol. 2019, 97, 707–713. [Google Scholar] [CrossRef]
- Miraftabi, A.; Nilforushan, N.; Nassiri, N.; Nouri-Mahdavi, K. Selective laser trabeculoplasty in patients with pseudoexfoliative glaucoma vs primary open angle glaucoma: A one-year comparative study. Int. J. Ophthalmol. 2016, 9, 406–410. [Google Scholar] [CrossRef]
- Kara, N.; Altan, C.; Yuksel, K.; Tetikoglu, M. Comparison of the efficacy and safety of selective laser trabeculoplasty in cases with primary open-angle glaucoma and pseudoexfoliative glaucoma. Kaohsiung J. Med. Sci. 2013, 29, 500–504. [Google Scholar] [CrossRef] [Green Version]
- Ayala, M. Long-term Outcomes of Selective Laser Trabeculoplasty (SLT) Treatment in Pigmentary Glaucoma Patients. J. Glaucoma 2014, 23, 616–619. [Google Scholar] [CrossRef]
- McAlinden, C. Selective laser trabeculoplasty (SLT) vs other treatment modalities for glaucoma: Systematic review. Eye 2014, 28, 249–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagar, M.; Ogunyomade, A.; O’Brart, D.P.S.; Howes, F.; Marshall, J. A randomised, prospective study comparing selective laser trabeculoplasty with latanoprost for the control of intraocular pressure in ocular hypertension and open angle glaucoma. Br. J. Ophthalmol. 2005, 89, 1413–1417. [Google Scholar] [CrossRef] [Green Version]
- McIlraith, I.; Strasfeld, M.; Colev, G.; Hutnik, C.M.L. Selective Laser Trabeculoplasty as Initial and Adjunctive Treatment for Open-Angle Glaucoma. J. Glaucoma 2006, 15, 124–130. [Google Scholar] [CrossRef]
- Schlote, T.; Kynigopoulos, M. Selective laser trabeculoplasty (SLT): 1-year results in early and advanced open angle glaucoma. Int. Ophthalmol. 2016, 36, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, R.A.; Kammerdiener, L.L.; Williams, D.B.; Das, S.K.; Nutaitis, M.J. Efficacy of selective laser trabeculoplasty following incisional glaucoma surgery. Int. J. Ophthalmol. 2018, 11, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Yang, Y.; Xu, J.; Yu, M. Selective laser trabeculoplasty in treating post-trabeculectomy advanced primary open-angle glaucoma. Exp. Ther. Med. 2016, 11, 1090–1094. [Google Scholar] [CrossRef] [Green Version]
- Narayanaswamy, A.; Leung, C.K.; Istiantoro, D.V.; Perera, S.A.; Ho, C.-L.; Nongpiur, M.E.; Baskaran, M.; Htoon, H.M.; Wong, T.T.; Goh, D.; et al. Efficacy of selective laser trabeculoplasty in primary angle-closure glaucoma: A randomized clinical trial. JAMA Ophthalmol. 2015, 133, 206–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali Aljasim, L.; Owaidhah, O.; Edward, D.P. Selective Laser Trabeculoplasty in Primary Angle-closure Glaucoma after Laser Peripheral Iridotomy: A Case-Control Study. J. Glaucoma 2016, 25, e253–e258. [Google Scholar] [CrossRef] [PubMed]
- Kurysheva, N.I.; Lepeshkina, L.V. Selective Laser Trabeculoplasty Protects Glaucoma Progression in the Initial Primary Open-Angle Glaucoma and Angle-Closure Glaucoma after Laser Peripheral Iridotomy in the Long Term. BioMed Res. Int. 2019, 2019, 4519412. [Google Scholar] [CrossRef]
- Hodge, W.G.; Damji, K.F.; Rock, W.; Buhrmann, R.; Bovell, A.M.; Pan, Y. Baseline IOP predicts selective laser trabeculoplasty success at 1 year post-treatment: Results from a randomised clinical trial. Br. J. Ophthalmol. 2005, 89, 1157–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirabayashi, M.; Ponnusamy, V.; An, J. Predictive Factors for Outcomes of Selective Laser Trabeculoplasty. Sci. Rep. 2020, 10, 9428. [Google Scholar] [CrossRef] [PubMed]
- Alaghband, P.; Galvis, E.A.; Daas, A.; Nagar, A.; Beltran-Agulló, L.; Khawaja, A.P.; Goyal, S.; Lim, K.S. Predictors of selective laser trabeculoplasty success in open angle glaucoma or ocular hypertension: Does baseline tonography have a predictive role? Br. J. Ophthalmol. 2020, 104, 1390–1393. [Google Scholar] [CrossRef]
- Chun, M.; Gracitelli, C.P.B.; Lopes, F.S.; Biteli, L.G.; Ushida, M.; Prata, T.S. Selective laser trabeculoplasty for early glaucoma: Analysis of success predictors and adjusted laser outcomes based on the untreated fellow eye. BMC Ophthalmol. 2016, 16, 206. [Google Scholar] [CrossRef] [Green Version]
- Pillunat, K.R.; Spoerl, E.; Elfes, G.; Pillunat, L.E. Preoperative intraocular pressure as a predictor of selective laser trabeculoplasty efficacy. Acta Ophthalmol. 2016, 94, 692–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.W.; Liu, C.C.; Chan, J.C.; Wong, R.L.; Wong, I.Y.; Lai, J.S. Predictors of success in selective laser trabeculoplasty for primary open angle glaucoma in Chinese. Clin. Ophthalmol. 2014, 8, 1787–1791. [Google Scholar] [CrossRef] [Green Version]
- Hong, B.K.; Winer, J.C.; Martone, J.F.; Wand, M.; Altman, B.; Shields, B. Repeat selective laser trabeculoplasty. J. Glaucoma 2009, 18, 180–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polat, J.; Grantham, L.; Mitchell, K.; Realini, T. Repeatability of selective laser trabeculoplasty. Br. J. Ophthalmol. 2016, 100, 1437–1441. [Google Scholar] [CrossRef] [Green Version]
- Avery, N.; Ang, G.S.; Nicholas, S.; Wells, A. Repeatability of primary selective laser trabeculoplasty in patients with primary open-angle glaucoma. Int. Ophthalmol. 2013, 33, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Song, J. Complications of selective laser trabeculoplasty: A review. Clin. Ophthalmol. 2016, 10, 137–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harasymowycz, P.J.; Papamatheakis, D.G.; Latina, M.; De Leon, M.; Lesk, M.R.; Damji, K.F. Selective Laser Trabeculoplasty (SLT) Complicated by Intraocular Pressure Elevation in Eyes with Heavily Pigmented Trabecular Meshworks. Am. J. Ophthalmol. 2005, 139, 1110–1113. [Google Scholar] [CrossRef] [PubMed]
- Realini, T.; Shillingford-Ricketts, H.; Burt, D.; Balasubramani, G.K. West Indies Glaucoma Laser Study (WIGLS) 3. Anterior Chamber Inflammation Following Selective Laser Trabeculoplasty in Afro-Caribbeans with Open-Angle Glaucoma. J. Glaucoma 2019, 28, 622–625. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Singh, A. Severe Iritis and Choroidal Effusion Following Selective Laser Trabeculoplasty. Ophthalmic Surg. Lasers Imaging Retin. 2008, 39, 409–411. [Google Scholar] [CrossRef]
- Baser, E.F.; Akbulut, D. Significant peripheral anterior synechiae after repeat selectıve laser trabeculoplasty. Can. J. Ophthalmol. 2015, 50, e36–e38. [Google Scholar] [CrossRef] [PubMed]
- Liu, E.T.; Seery, L.S.; Arosemena, A.; Lamba, T.; Chaya, C.J. Corneal edema and keratitis following selective laser trabeculoplasty. Am. J. Ophthalmol. Case Rep. 2017, 6, 48–51. [Google Scholar] [CrossRef]
- Wood, S.D.; Elam, A.; Moroi, S. Rare corneal complication following selective laser trabeculoplasty. Am. J. Ophthalmol. Case Rep. 2018, 10, 28–31. [Google Scholar] [CrossRef]
- Chadha, N.; Belyea, D.A.; Grewal, S. Herpetic Stromal Keratitis following Selective Laser Trabeculoplasty. Case Rep. Ophthalmol. Med. 2016, 2016, e5768524. [Google Scholar] [CrossRef] [Green Version]
- Bettis, D.I.; Whitehead, J.J.; Farhi, P.; Zabriskie, N.A. Intraocular Pressure Spike and Corneal Decompensation Following Selective Laser Trabeculoplasty in Patients with Exfoliation Glaucoma. J. Glaucoma 2016, 25, e433. [Google Scholar] [CrossRef]
- Lee, J.W.Y.; Chan, J.C.H.; Chang, R.T.; Singh, K.; Liu, C.C.L.; Gangwani, R.; Wong, M.O.M.; Lai, J.S.M. Corneal changes after a single session of selective laser trabeculoplasty for open-angle glaucoma. Eye 2014, 28, 47–52. [Google Scholar] [CrossRef] [Green Version]
- Ong, K.; Ong, L.; Ong, L. Corneal endothelial changes after selective laser trabeculoplasty. Clin. Exp. Ophthalmol. 2013, 41, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Koenig, L.R.; Kovacs, K.D.; Gupta, M.P.; Van Tassel, S.H. Hypopyon following selective laser trabeculoplasty. Am. J. Ophthalmol. Case Rep. 2020, 18, 100675. [Google Scholar] [CrossRef]
- Rhee, D.J.; Krad, O.; Pasquale, L.R. Hyphema following selective laser trabeculoplasty. Ophthalmic Surg. Lasers Imaging Retin. 2009, 40, 493–494. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.H.; Bowling, B.; Chen, S.D. Cystoid macular oedema following selective laser trabeculoplasty in a diabetic patient. Clin. Exp. Ophthalmol. 2014, 42, 200–201. [Google Scholar] [CrossRef]
- Liyanage, S.E.; Kumaran, N.; Alwis, D.D. Macular burns resulting from the accidental use of selective laser trabeculoplasty mode during a laser capsulotomy. Br. J. Ophthalmol. 2014, 98, 141–142. [Google Scholar] [CrossRef] [PubMed]
- Örnek, N.; Örnek, K.; Oğurel, T.; Büyüktortop Gökçınar, N. Cystoid macular edema following selective laser trabeculoplasty in a patient with ocular hypertension. Int. Ophthalmol. 2019, 39, 1891–1893. [Google Scholar] [CrossRef]
- Wright, D.M.; Konstantakopoulou, E.; Montesano, G.; Nathwani, N.; Garg, A.; Garway-Heath, D.; Crabb, D.P.; Gazzard, G.; Laser in Glaucoma and Ocular Hypertension Trial (LiGHT) Study Group. Visual Field Outcomes from the Multicenter, Randomized Controlled Laser in Glaucoma and Ocular Hypertension Trial (LiGHT). Ophthalmology 2020, 127, 1313–1321. [Google Scholar] [CrossRef]


{kind=link}
| Research | Type of Study | Number of Subjects | Diagnosis | Indications | IOP Reduction | Differences in Procedure | Observation Time |
|---|---|---|---|---|---|---|---|
| Chen et al. 2004 [16] | Prospective, single-masked randomized clinical trial | N90 = 32 | OAG, OHT | Adjunctive | 5.1 mmHg (1 mo) | 90 degrees, some patients received ALT | Up to 7 months |
| 6.3 mmHg (4 mo) | |||||||
| 6.2 mmHg (7 mo) | |||||||
| N180 = 32 | OAG, OHT | Adjunctive | 4.2 mmHg (1 mo) | 180 degrees, some patients received ALT | Up to 7 months | ||
| 5.6 mmHg (4 mo) | |||||||
| 7.1 mmHg (7 mo) | |||||||
| Goyal et al. 2010 [17] | Prospective, single-masked randomized clinical trial | N180 = 18 | OAG = 12, | Primary | 6.1 mmHg (1 mo) | 180 degrees | 1 month |
| OHT = 6 | |||||||
| N360 = 19 | OAG = 15, | Primary | 9.0 mmHg (1 mo) | 360 degrees | 1 month | ||
| OHT = 4 | |||||||
| Shibata et al. 2012 [18] | Retrospective cohort study | N180 = 35 | OAG | Additive | 2.6 mmHg (6 mo) | 180 degrees | Up to 36 months |
| N360 = 34 | OAG | Additive | 5.6 mmHg (6 mo) | 360 degrees | Up to 36 months | ||
| Francis et al. 2016 [19] | Open-label prospective study | N360 = 137 | POAG | Additive | 4.1 mmHg (6–12 mo) | 360 degrees | Up to 15 months |
| 3.5 mmHg (12–15 mo) | |||||||
| Tawfique et al. 2019 [20] | Prospective, single-masked randomized clinical trial | N90 = 32 | OAG, OHT, XFG | Primary or Additive | nd (only survival analysis was conducted | 90 degrees | Up to 24 months |
| N180 = 35 | OAG, OHT, XFG | Primary or Additive | nd (only survival analysis was conducted) | 360 degrees | Up to 24 months | ||
| Özen et al. 2020 [21] | Open-label prospective study | N180 = 26 | POAG | Additive | 7.8 mmHg (1 mo) | 180 degrees | Up to 6 months |
| 9.0 mmHg (3 mo) | |||||||
| 9.1 mmHg (6 mo) | |||||||
| N360 = 26 | POAG | Additive | 8.5 mmHg (1 mo) | 360 degrees | Up to 6 months | ||
| 10.1 mmHg (3 mo) | |||||||
| 10.3 mmHg (6 mo) | |||||||
| Nirappel et al. 2021 [22] | Retrospective cohort study | N180 = 196 | OAG, OHT | Additive | 2.9 mmHg (6 wk) | 180 degrees | Up to 24 months |
| 3.0 mmHg (12 mo) | |||||||
| 2.2 mmHg (24 mo) | |||||||
| N360 = 258 | OAG, OHT | Additive | 3.2 mmHg (6 wk) | 360 degrees | Up to 24 months | ||
| 3.4 mmHg (12 mo) | |||||||
| 2.4 mmHg (24 mo) | |||||||
| Research | Hong et al. in 2009 [68] | Avery et al. in 2013 [70] | Francis et al. in 2016 [19] | Polat et al. 2016 [69] | Garg et al. 2020 [31] |
|---|---|---|---|---|---|
| Patient characteristics | POAG, XFG, and PG uncontrolled on medication | Treatment-naïve POAG | Primary and secondary glaucoma (except uveitic) on medication | POAG, XFG and PG uncontrolled on medication | Treatment-naïve OHT and OAG that required repeated SLT |
| Interval between 1st and 2nd SLT (time in which 1st SLT remained successful) | Not specified | Not specified | At least 6 months | At least 6 months | Maximum 18 months |
| Sample size | 44 eyes of 35 patients | 42 eyes of 42 patients | 137 eyes of 137 patients | 38 eyes of 38 patients | 115 eyes of 90 patients |
| Range of SLT | 360° | 360°(40–50 spots) | 360° (80–132) | 360° (100 spots) | 360° (100 spots) |
| Definition of success | ≥20% reduction from baseline | IOP reduction of ≥20% of baseline IOP and IOP at or below predefined target | 1st definition: | “Real-world” definition: IOP control without additional IOP-lowering medications, glaucoma laser procedures or incisional glaucoma surgery; | IOP at or below target IOP without additional IOP-lowering medications, further laser procedures or incisional glaucoma surgery |
| IOP 5–21 mmHg, IOP reduction >20%, no addition of medication or procedure; | “formal” definition IOP reduction ≥20% | ||||
| 2nd definition: | |||||
| IOP 5–21 mmHg, no additional glaucoma procedure, either IOP reduction of >20% or reduction in medication | |||||
| Success rate of first SLT | 50% | 55% | 1st definition: | Not specified; “real-world” definition: | Not specified; |
| (p = 0.52) | 55% at 6 months and 34% at 12 months; | Kaplan–Meier survival analysis showed a median survival time of 570 days; | |||
| 2nd definition: | “Formal” definition: | Kaplan–Meier survival analysis | |||
| 65% at 6 months and 44% at 12 months | Kaplan–Meier survival analysis showed a median survival time of 270 days | showed a median duration of effect of 189 days | |||
| Success rate of second SLT | 43.2% (p = 0.52) | 66% | 1st definition: 37% at 6 months and 19% at 12 months; | Not specified; | Not specified; |
| 2nd definition: 48% at 6 months and 27% at 12 months | “real-world” definition: | ||||
| Kaplan–Meier survival analysis showed a median survival time of 1054 days; | Kaplan–Meier survival analysis could not be conducted, as 50% of eyes had not reached the endpoint by the end of follow-up | ||||
| “Formal” definition: | |||||
| Kaplan–Meier survival analysis showed a median survival time of 360 days | |||||
| Time of evaluation or follow-up period | 5–8 months follow-up | Mean duration of follow-up: | 12–15 months’ follow-up | up to 24 months | 18 months’ follow-up |
| 1st SLT: mean duration of follow-up was 10.5 months; | |||||
| 2nd SLT: 15.1 months; | |||||
| 3rd SLT: 9.0 months | |||||
| Mean IOP reduction after 1st SLT [mmHg] | 4.0 (5.3,2.7) at 5–8 months | 3.6 (4.8) at second visit (4–5 months) | 4.1 (SD 4.8) at 6–12 months (p < 0.001) | 2.9–5.7 at different points in 24-month follow-up | 5.3 (4.5–6.0) [95% CI] at 2 months |
| Mean IOP reduction after 2nd SLT | 2.9 (4.2,1.5) mmHg at 5–8 months (p = 0.16) | 4.5 (4.5) at second visit (4–5 months) | 2.9 (SD 4.7) at 6–12 months (p < 0.001) | 2.3–4.4 at different points in 24-month follow-up | 4.6 (4.0–5.2) [95% CI] at 2 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zgryźniak, A.; Przeździecka-Dołyk, J.; Szaliński, M.; Turno-Kręcicka, A. Selective Laser Trabeculoplasty in the Treatment of Ocular Hypertension and Open-Angle Glaucoma: Clinical Review. J. Clin. Med. 2021, 10, 3307. https://doi.org/10.3390/jcm10153307
Zgryźniak A, Przeździecka-Dołyk J, Szaliński M, Turno-Kręcicka A. Selective Laser Trabeculoplasty in the Treatment of Ocular Hypertension and Open-Angle Glaucoma: Clinical Review. Journal of Clinical Medicine. 2021; 10(15):3307. https://doi.org/10.3390/jcm10153307
Chicago/Turabian StyleZgryźniak, Aleksandra, Joanna Przeździecka-Dołyk, Marek Szaliński, and Anna Turno-Kręcicka. 2021. "Selective Laser Trabeculoplasty in the Treatment of Ocular Hypertension and Open-Angle Glaucoma: Clinical Review" Journal of Clinical Medicine 10, no. 15: 3307. https://doi.org/10.3390/jcm10153307