
Strength Training to Prevent Falls in Older Adults: A Systematic Review with Meta-Analysis of Randomized Controlled Trials

 ,
,  ,
,  ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
- Participants: older individuals (age ≥ 60 years), of any sex. Fragility and/or comorbidities could be either present or absent. They could be community-dwelling older adults or patients living in residential facilities or in the hospital.
- Intervention: strength training (e.g., resistance training, calisthenics). Studies that combined strength training with other exercise protocols (e.g., endurance, stretching) were not considered.
- Comparator: non-exercise controls or multimodal or unimodal exercise interventions (e.g., stretching, balance). Studies that did not provide these types of comparator group(s) were excluded.
- Outcomes: the primary outcome was risk of falling as measured by the number of falls or fall rates. Risk of falling was considered as a metric or statistical analysis where actual falls have been reported, and not as more generic, proxy assessments that may place the person at a higher risk of fall. Timepoints for assessments of the outcomes: in case studies that had multiple timepoints, we considered only the endpoint, i.e., the final assessments, performed after the intervention cessation.
- Study design: supervised RCTs—the limitation to RCTs provides reduced risk of bias and balances participants between the groups [39] and is in line with previous reviews with older adults [4,19]. Studies with other designs or studies where the intervention or comparators were supervised by professionals not qualified for exercise prescription were excluded.
2.3. Information Sources
2.4. Study Selection
2.5. Data Extraction
2.6. Risk of Bias in Individual Studies
2.7. Quantitative Syntheses
2.8. Certainty of Evidence
3. Results
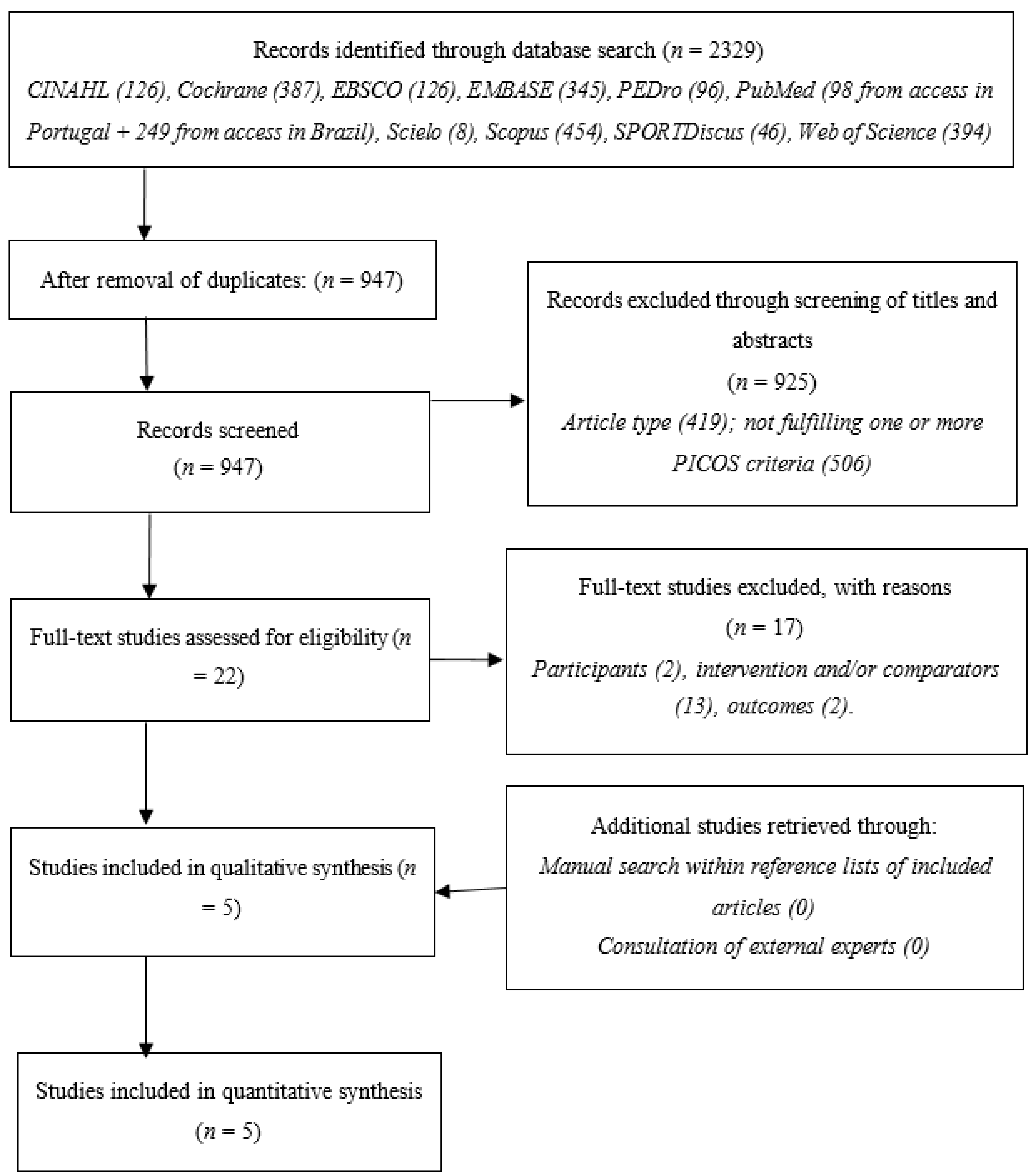
3.1. Study Selection
3.2. Study Characteristics and Results
3.3. Risk of Bias within Studies
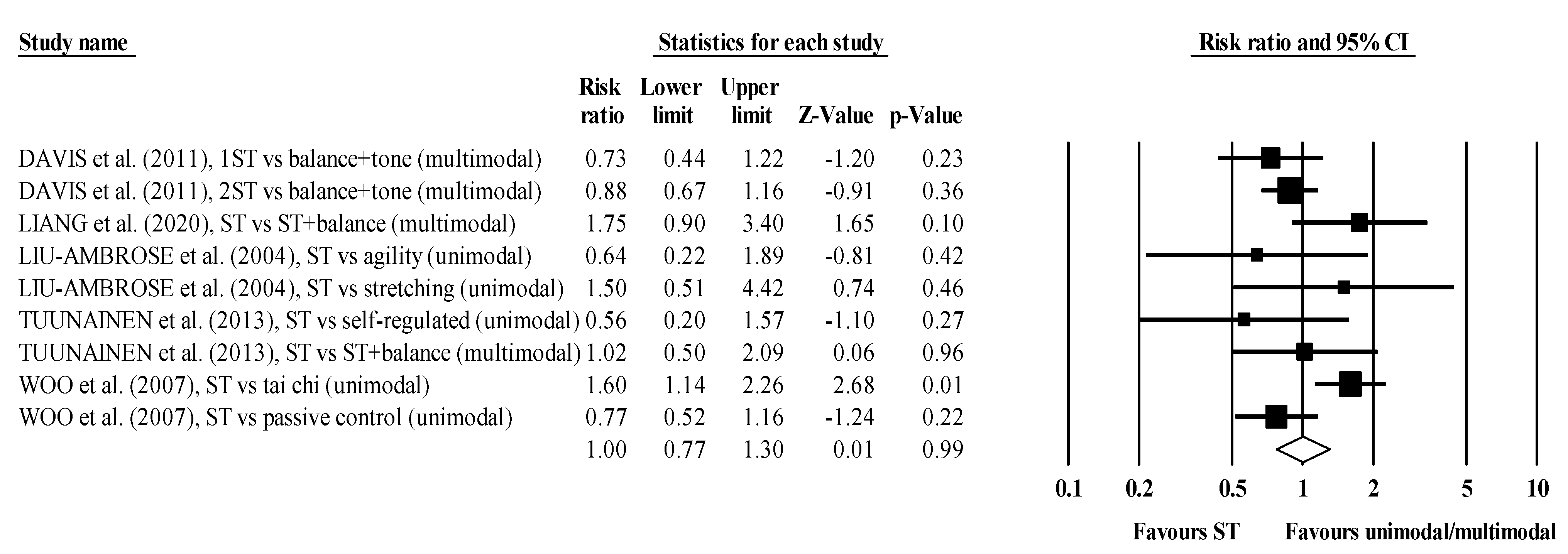
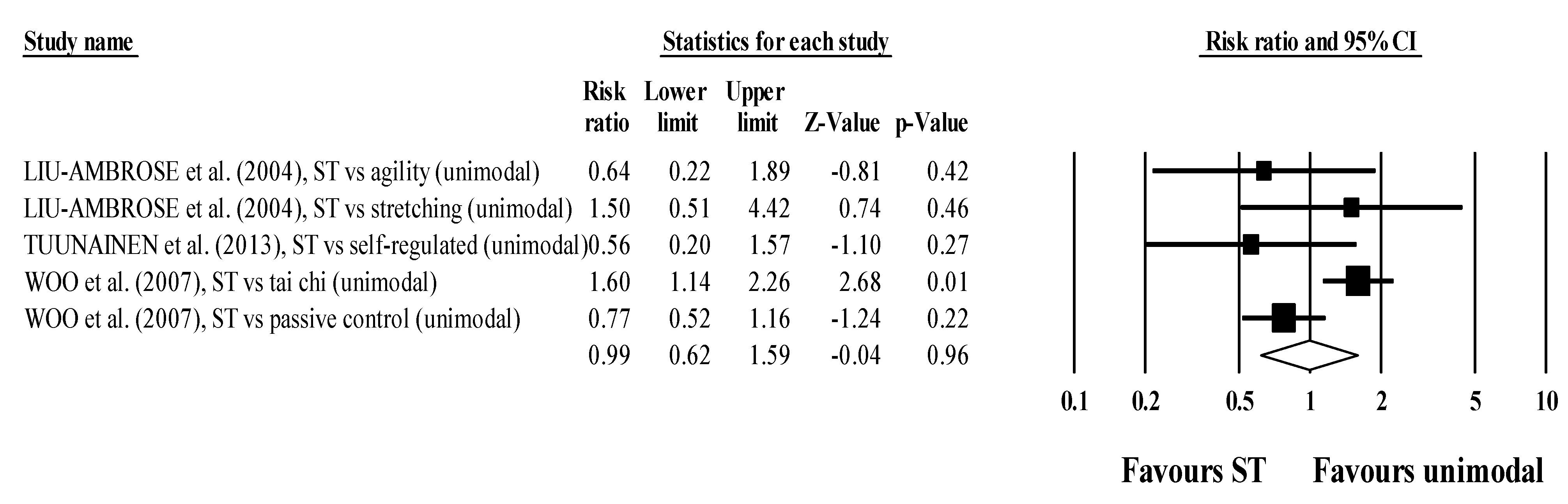
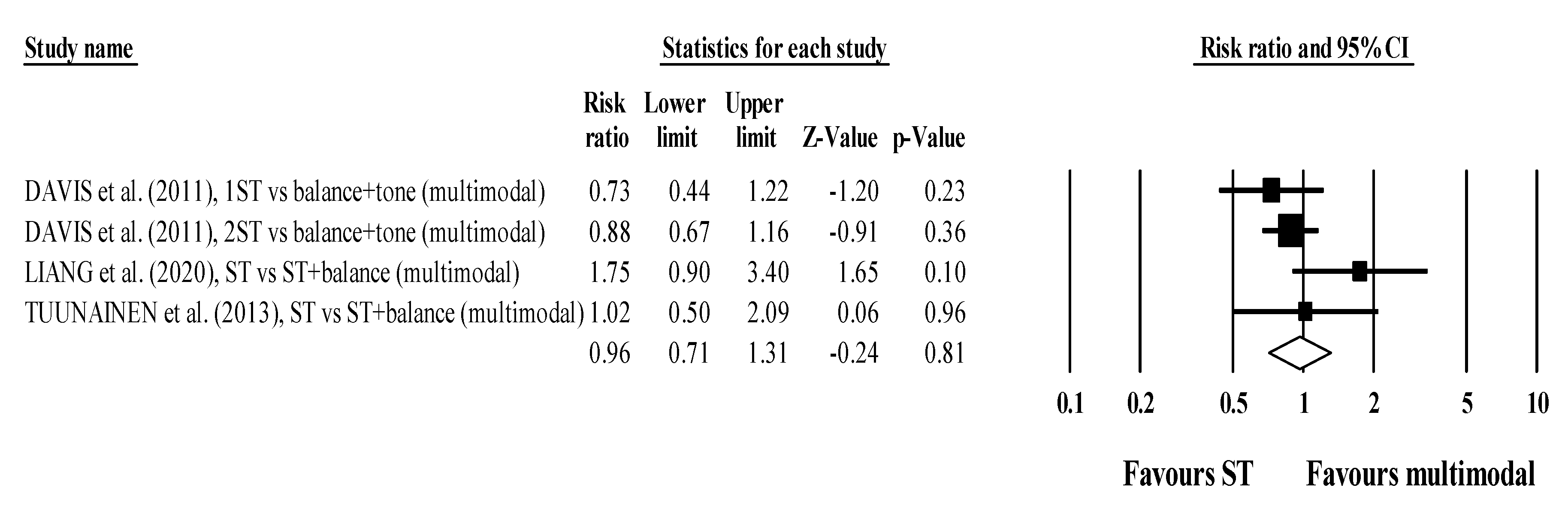
3.4. Syntheses of Results
3.5. Sensitivity Analyses
3.6. Certainty of Evidence
3.7. Narrative Overview of Secondary Outcomes
4. Discussion
4.1. Summary of Evidence
4.2. Real-World Applications
4.3. Limitations
4.4. Suggestions for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Falls. Available online: https://www.who.int/news-room/fact-sheets/detail/falls#:~:text=Key%20facts,greatest%20number%20of%20fatal%20falls (accessed on 27 October 2020).
- Figgins, E.; Pieruccini-Faria, F.; Speechley, M.; Montero-Odasso, M. Potentially modifiable risk factors for slow gait in community-dwelling older adults: A systematic review. Ageing Res. Rev. 2021, 66, 101253. [Google Scholar] [CrossRef] [PubMed]
- Okubo, Y.; Schoene, D.; Caetano, M.J.D.; Pliner, E.M.; Osuka, Y.; Toson, B.; Lord, S.R. Stepping impairment and falls in older adults: A systematic review and meta-analysis of volitional and reactive step tests. Ageing Res. Rev. 2021, 66, 101238. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Ramirez-Vélez, R.; Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Valenzuela, P.L.; Lucia, A.; Izquierdo, M. Safety and Effectiveness of Long-Term Exercise Interventions in Older Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Sports Med. 2020, 50, 1095–1106. [Google Scholar] [CrossRef]
- Falck, R.S.; Davis, J.C.; Best, J.R.; Crockett, R.A.; Liu-Ambrose, T. Impact of exercise training on physical and cognitive function among older adults: A systematic review and meta-analysis. Neurobiol. Aging 2019, 79, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Mattle, M.; Chocano-Bedoya, P.O.; Fischbacher, M.; Meyer, U.; Abderhalden, L.A.; Lang, W.; Mansky, R.; Kressig, R.W.; Steurer, J.; Orav, E.J.; et al. Association of Dance-Based Mind-Motor Activities With Falls and Physical Function Among Healthy Older Adults: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2017688. [Google Scholar] [CrossRef]
- Sherrington, C.; Michaleff, Z.A.; Fairhall, N.; Paul, S.S.; Tiedemann, A.; Whitney, J.; Cumming, R.G.; Herbert, R.D.; Close, J.C.T.; Lord, S.R. Exercise to prevent falls in older adults: An updated systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1750–1758. [Google Scholar] [CrossRef]
- Gardner, M.M.; Robertson, M.C.; Campbell, A.J. Exercise in preventing falls and fall related injuries in older people: A review of randomised controlled trials. Br. J. Sports Med. 2000, 34, 7. [Google Scholar] [CrossRef] [Green Version]
- de Souto Barreto, P.; Rolland, Y.; Vellas, B.; Maltais, M. Association of Long-term Exercise Training With Risk of Falls, Fractures, Hospitalizations, and Mortality in Older Adults: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2019, 179, 394–405. [Google Scholar] [CrossRef] [Green Version]
- Hamed, A.; Bohm, S.; Mersmann, F.; Arampatzis, A. Follow-up efficacy of physical exercise interventions on fall incidence and fall risk in healthy older adults: A systematic review and meta-analysis. Sports Med. Open 2018, 4, 56. [Google Scholar] [CrossRef]
- Cadore, E.L.; Rodríguez-Mañas, L.; Sinclair, A.; Izquierdo, M. Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: A systematic review. Rejuvenation Res. 2013, 16, 105–114. [Google Scholar] [CrossRef] [Green Version]
- Tavoian, D.; Russ, D.W.; Consitt, L.A.; Clark, B.C. Perspective: Pragmatic Exercise Recommendations for Older Adults: The Case for Emphasizing Resistance Training. Front. Physiol. 2020, 11. [Google Scholar] [CrossRef]
- Medina-Mirapeix, F.; Escolar-Reina, P.; Gascón-Cánovas, J.J.; Montilla-Herrador, J.; Jimeno-Serrano, F.J.; Collins, S.M. Predictive factors of adherence to frequency and duration components in home exercise programs for neck and low back pain: An observational study. BMC Musculoskelet. Disord. 2009, 10, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinetti, M.E.; Kumar, C. The patient who falls: “It’s always a trade-off”. JAMA 2010, 303, 258–266. [Google Scholar] [CrossRef]
- Peterson, M.D.; Rhea, M.R.; Sen, A.; Gordon, P.M. Resistance exercise for muscular strength in older adults: A meta-analysis. Ageing Res. Rev. 2010, 9, 226–237. [Google Scholar] [CrossRef] [Green Version]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults: Position Statement From the National Strength and Conditioning Association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Garofolini, A.; Orazem, J.; Sabol, F.; Schoenfeld, B.J.; Pedisic, Z. Effects of Resistance Training on Muscle Size and Strength in Very Elderly Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sports Med. 2020, 50, 1983–1999. [Google Scholar] [CrossRef]
- Maestroni, L.; Read, P.; Bishop, C.; Papadopoulos, K.; Suchomel, T.J.; Comfort, P.; Turner, A. The Benefits of Strength Training on Musculoskeletal System Health: Practical Applications for Interdisciplinary Care. Sports Med. 2020, 50, 1431–1450. [Google Scholar] [CrossRef]
- Afonso, J.; Ramirez-Campillo, R.; Moscão, J.; Rocha, T.; Zacca, R.; Martins, A.; Milheiro, A.A.; Ferreira, J.; Sarmento, H.; Clemente, F.M. Strength Training versus Stretching for Improving Range of Motion: A Systematic Review and Meta-Analysis. Healthcare 2021, 9, 427. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Chen, H.C.; Kuo, Y.C.; Tsauo, J.Y.; Huang, S.W.; Liou, T.H. Effects of Muscle Strength Training on Muscle Mass Gain and Hypertrophy in Older Adults With Osteoarthritis: A Systematic Review and Meta-Analysis. Arthritis Care Res. (Hoboken) 2020, 72, 1703–1718. [Google Scholar] [CrossRef]
- Pina, F.L.C.; Nunes, J.P.; Nascimento, M.A.; Ribeiro, A.S.; Mayhew, J.L.; Cyrino, E.S. Similar Effects of 24 Weeks of Resistance Training Performed with Different Frequencies on Muscle Strength, Muscle Mass, and Muscle Quality in Older Women. Int. J. Exerc. Sci. 2019, 12, 623–635. [Google Scholar] [PubMed]
- Aragão-Santos, J.C.; De Resende-Neto, A.G.; Nogueira, A.C.; Feitosa-Neta, M.L.; Brandão, L.H.; Chaves, L.M.; Da Silva-Grigoletto, M.E. The effects of functional and traditional strength training on different strength parameters of elderly women: A randomized and controlled trial. J. Sports Med. Phys. Fit. 2019, 59, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Andersson, E.A.; Frank, P.; Pontén, M.; Ekblom, B.; Ekblom, M.; Moberg, M.; Sahlin, K. Improving Strength, Power, Muscle Aerobic Capacity, and Glucose Tolerance through Short-term Progressive Strength Training Among Elderly People. J. Vis. Exp. 2017, 125, 55518. [Google Scholar] [CrossRef] [PubMed]
- Frank, P.; Andersson, E.; Pontén, M.; Ekblom, B.; Ekblom, M.; Sahlin, K. Strength training improves muscle aerobic capacity and glucose tolerance in elderly. Scand. J. Med. Sci. Sports 2016, 26, 764–773. [Google Scholar] [CrossRef] [PubMed]
- Carral, J.M.C.; Rodríguez, A.L.; Cardalda, I.M.; Bezerra, J. Muscle strength training program in nonagenarians—A randomized controlled trial. Rev. Assoc. Med. Bras. 2019, 65, 851–856. [Google Scholar] [CrossRef]
- Joshua, A.M.; D’Souza, V.; Unnikrishnan, B.; Mithra, P.; Kamath, A.; Acharya, V.; Venugopal, A. Effectiveness of progressive resistance strength training versus traditional balance exercise in improving balance among the elderly—A randomised controlled trial. J. Clin. Diagn. Res. 2014, 8, 98–102. [Google Scholar] [CrossRef]
- Connelly, D.M.; Vandervoort, A.A. Effects of isokinetic strength training on concentric and eccentric torque development in the ankle dorsiflexors of older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, B465–B472. [Google Scholar] [CrossRef] [Green Version]
- Fatouros, I.G.; Taxildaris, K.; Tokmakidis, S.P.; Kalapotharakos, V.; Aggelousis, N.; Athanasopoulos, S.; Zeeris, I.; Katrabasas, I. The effects of strength training, cardiovascular training and their combination on flexibility of inactive older adults. Int. J. Sports Med. 2002, 23, 112–119. [Google Scholar] [CrossRef]
- Alves, W.M.; Alves, T.G.; Ferreira, R.M.; Lima, T.A.; Pimentel, C.P.; Sousa, E.C.; Abrahin, O.; Alves, E.A. Strength training improves the respiratory muscle strength and quality of life of elderly with Parkinson disease. J. Sports Med. Phys. Fit. 2019, 59, 1756–1762. [Google Scholar] [CrossRef]
- Copeland, J.L.; Good, J.; Dogra, S. Strength training is associated with better functional fitness and perceived healthy aging among physically active older adults: A cross-sectional analysis of the Canadian Longitudinal Study on Aging. Aging Clin. Exp. Res. 2019, 31, 1257–1263. [Google Scholar] [CrossRef]
- Davis, J.C.; Bryan, S.; Marra, C.A.; Sharma, D.; Chan, A.; Beattie, B.L.; Graf, P.; Liu-Ambrose, T. An economic evaluation of resistance training and aerobic training versus balance and toning exercises in older adults with mild cognitive impairment. PLoS ONE 2013, 8, e63031. [Google Scholar] [CrossRef] [PubMed]
- Mayer, F.; Scharhag-Rosenberger, F.; Carlsohn, A.; Cassel, M.; Müller, S.; Scharhag, J. The intensity and effects of strength training in the elderly. Dtsch. Arztebl. Int. 2011, 108, 359–364. [Google Scholar] [CrossRef]
- Bhasin, S.; Gill, T.M.; Reuben, D.B.; Latham, N.K.; Ganz, D.A.; Greene, E.J.; Dziura, J.; Basaria, S.; Gurwitz, J.H.; Dykes, P.C.; et al. A Randomized Trial of a Multifactorial Strategy to Prevent Serious Fall Injuries. N. Engl. J. Med. 2020, 383, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Hunter, J.R.; Gordon, B.A.; Bird, S.R.; Benson, A.C. Exercise Supervision Is Important for Cardiometabolic Health Improvements: A 16-Week Randomized Controlled Trial. J. Strength Cond. Res. 2020, 34, 866–877. [Google Scholar] [CrossRef]
- Lemos, E.C.W.M.; Guadagnin, E.C.; Mota, C.B. Influence of strength training and multicomponent training on the functionality of older adults: Systematic review and meta-analysis. Rev. Bras. Cineantropom. Desempenho Hum. 2020, 22. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Hariton, E.; Locascio, J.J. Randomised controlled trials—The gold standard for effectiveness research: Study design: Randomised controlled trials. BJOG 2018, 125, 1716. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V. Cochrane for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Gross, A.; Schirm, S.; Scholz, M. Ycasd– a tool for capturing and scaling data from graphical representations. BMC Bioinform. 2014, 15, 219. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Skrede, T.; Steene-Johannessen, J.; Anderssen, S.A.; Resaland, G.K.; Ekelund, U. The prospective association between objectively measured sedentary time, moderate-to-vigorous physical activity and cardiometabolic risk factors in youth: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 55–74. [Google Scholar] [CrossRef] [Green Version]
- García-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Is Muscular Fitness Associated with Future Health Benefits in Children and Adolescents? A Systematic Review and Meta-Analysis of Longitudinal Studies. Sports Med. 2019, 49, 1079–1094. [Google Scholar] [CrossRef]
- Abt, G.; Boreham, C.; Davison, G.; Jackson, R.; Nevill, A.; Wallace, E.; Williams, M. Power, precision, and sample size estimation in sport and exercise science research. J. Sports Sci. 2020, 38, 1933–1935. [Google Scholar] [CrossRef]
- Lohse, K.R.; Sainani, K.L.; Taylor, J.A.; Butson, M.L.; Knight, E.J.; Vickers, A.J. Systematic review of the use of “magnitude-based inference” in sports science and medicine. PLoS ONE 2020, 15, e0235318. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions: The Cochrane Collaboration; Higgins, J.P., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2008; pp. 243–296. [Google Scholar]
- Kontopantelis, E.; Springate, D.A.; Reeves, D. A re-analysis of the Cochrane Library data: The dangers of unobserved heterogeneity in meta-analyses. PLoS ONE 2013, 8, e69930. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Johansson, J.; Nordström, A.; Nordström, P. Greater Fall Risk in Elderly Women Than in Men Is Associated With Increased Gait Variability During Multitasking. J. Am. Med. Dir. Assoc. 2016, 17, 535–540. [Google Scholar] [CrossRef]
- Gale, C.R.; Cooper, C.; Aihie Sayer, A. Prevalence and risk factors for falls in older men and women: The English Longitudinal Study of Ageing. Age Ageing 2016, 45, 789–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vu, T.; Finch, C.F.; Day, L. Patterns of comorbidity in community-dwelling older people hospitalised for fall-related injury: A cluster analysis. BMC Geriatr. 2011, 11, 45. [Google Scholar] [CrossRef] [Green Version]
- Liguori, G.; ACSM. ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2021. [Google Scholar]
- Moran, J.; Sandercock, G.; Ramirez-Campillo, R.; Clark, C.C.T.; Fernandes, J.F.T.; Drury, B. A Meta-Analysis of Resistance Training in Female Youth: Its Effect on Muscular Strength, and Shortcomings in the Literature. Sports Med. 2018, 48, 1661–1671. [Google Scholar] [CrossRef] [Green Version]
- Moran, J.; Clark, C.C.T.; Ramirez-Campillo, R.; Davies, M.J.; Drury, B. A Meta-Analysis of Plyometric Training in Female Youth: Its Efficacy and Shortcomings in the Literature. J. Strength Cond. Res. 2019, 33, 1996–2008. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Li, F.; Harmer, P.; Fitzgerald, K.; Eckstrom, E.; Stock, R.; Galver, J.; Maddalozzo, G.; Batya, S.S. Tai chi and postural stability in patients with Parkinson’s disease. N. Engl. J. Med. 2012, 366, 511–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGinley, J.L.; Martin, C.; Huxham, F.E.; Menz, H.B.; Danoudis, M.; Murphy, A.T.; Watts, J.J.; Iansek, R.; Morris, M.E. Feasibility, safety, and compliance in a randomized controlled trial of physical therapy for parkinson’s disease. Parkinson’s Dis. 2012, 2012, 1–9. [Google Scholar] [CrossRef]
- Boongird, C.; Keesukphan, P.; Phiphadthakusolkul, S.; Rattanasiri, S.; Thakkinstian, A. Effects of a simple home-based exercise program on fall prevention in older adults: A 12-month primary care setting, randomized controlled trial. Geriatr. Gerontol. Int. 2017, 17, 2157–2163. [Google Scholar] [CrossRef]
- Gianoudis, J.; Bailey, C.A.; Ebeling, P.R.; Nowson, C.A.; Sanders, K.M.; Hill, K.; Daly, R.M. Effects of a targeted multimodal exercise program incorporating high-speed power training on falls and fracture risk factors in older adults: A community-based randomized controlled trial. J. Bone Mineral. Res. 2014, 29, 182–191. [Google Scholar] [CrossRef]
- Kronhed, A.C.G.; Hallberg, I.; Ödkvist, L.; Möller, M. Effect of training on health-related quality of life, pain and falls in osteoporotic women. Adv. Physiother. 2009, 11, 154–165. [Google Scholar] [CrossRef]
- LaStayo, P.; Marcus, R.; Dibble, L.; Wong, B.; Pepper, G. Eccentric versus traditional resistance exercise for older adult fallers in the community: A randomized trial within a multi-component fall reduction program. BMC Geriatr. 2017, 17, 149. [Google Scholar] [CrossRef] [Green Version]
- Lipardo, D.S.; Tsang, W.W.N. Effects of combined physical and cognitive training on fall prevention and risk reduction in older persons with mild cognitive impairment: A randomized controlled study. Clin. Rehabil. 2020, 34, 773–782. [Google Scholar] [CrossRef]
- Lord, S.R.; Ward, J.A.; Williams, P.; Strudwick, M. The Effect of a 12-Month Exercise Trial on Balance, Strength, and Falls in Older Women: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 1995, 43, 1198–1206. [Google Scholar] [CrossRef]
- Morris, M.E.; Menz, H.B.; McGinley, J.L.; Watts, J.J.; Huxham, F.E.; Murphy, A.T.; Danoudis, M.E.; Iansek, R. A Randomized Controlled Trial to Reduce Falls in People With Parkinson’s Disease. Neurorehabilit. Neural Repair 2015, 29, 777–785. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.Z.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, Physical, Cognitive, and Combination Interventions and Frailty Reversal among Older Adults: A Randomized Controlled Trial. Am. J. Med. 2015, 128, 1225–1236.e1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra-Rexach, J.A.; Bustamante-Ara, N.; Hierro Villarán, M.; González Gil, P.; Sanz Ibáñez, M.J.; Blanco Sanz, N.; Ortega Santamaría, V.; Gutiérrez Sanz, N.; Marín Prada, A.B.; Gallardo, C.; et al. Short-term, light- to moderate-intensity exercise training improves leg muscle strength in the oldest old: A randomized controlled trial. J. Am. Geriatr. Soc. 2011, 59, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Uusi-Rasi, K.; Patil, R.; Karinkanta, S.; Kannus, P.; Tokola, K.; Lamberg-Allardt, C.; Sievänen, H. A 2-Year Follow-Up After a 2-Year RCT with Vitamin D and Exercise: Effects on Falls, Injurious Falls and Physical Functioning Among Older Women. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 1239–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zieschang, T.; Schwenk, M.; Becker, C.; Uhlmann, L.; Oster, P.; Hauer, K. Falls and Physical Activity in Persons with Mild to Moderate Dementia Participating in an Intensive Motor Training Randomized Controlled Trial. Alzheimer Dis. Assoc. Disord. 2017, 31, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Twiss, J.J.; Waltman, N.L.; Berg, K.; Ott, C.D.; Gross, G.J.; Lindsey, A.M. An exercise intervention for breast cancer survivors with bone loss. J. Nurs. Scholarsh. 2009, 41, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.S.; Canning, C.G.; Song, J.; Fung, V.S.; Sherrington, C. Leg muscle power is enhanced by training in people with Parkinson’s disease: A randomized controlled trial. Clin. Rehabil. 2014, 28, 275–288. [Google Scholar] [CrossRef]
- Kim, S.; Lockhart, T. Lower limb control and mobility following exercise training. J. Neuroeng. Rehabil. 2012, 9, 15. [Google Scholar] [CrossRef] [Green Version]
- Buchner, D.M.; Cress, M.E.; De Lateur, B.J.; Esselman, P.C.; Margherita, A.J.; Price, R.; Wagner, E.H. The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1997, 52, M218–M224. [Google Scholar] [CrossRef] [Green Version]
- Davis, J.C.; Marra, C.A.; Robertson, M.C.; Khan, K.M.; Najafzadeh, M.; Ashe, M.C.; Liu-Ambrose, T. Economic evaluation of dose-response resistance training in older women: A cost-effectiveness and cost-utility analysis. Osteoporos. Int. 2011, 22, 1355–1366. [Google Scholar] [CrossRef] [Green Version]
- Liang, Y.; Wang, R.; Jiang, J.; Tan, L.; Yang, M. A randomized controlled trial of resistance and balance exercise for sarcopenic patients aged 80-99 years. Sci. Rep. 2020, 10, 18756. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Khan, K.M.; Eng, J.J.; Janssen, P.A.; Lord, S.R.; McKay, H.A. Resistance and Agility Training Reduce Fall Risk in Women Aged 75 to 85 with Low Bone Mass: A 6-Month Randomized, Controlled Trial. J. Am. Geriatr. Soc. 2004, 52, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Hong, A.; Lau, E.; Lynn, H. A randomised controlled trial of Tai Chi and resistance exercise on bone health, muscle strength and balance in community-living elderly people. Age Ageing 2007, 36, 262–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuunainen, E.; Rasku, J.; Jäntti, P.; Moisio-Vilenius, P.; Mäkinen, E.; Toppila, E.; Pyykkö, I. Postural stability and quality of life after guided and self-training among older adults residing in an institutional setting. Clin. Interv. Aging 2013, 8, 1237–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, A.J.; Robertson, M.C. Rethinking individual and community fall prevention strategies: A meta-regression comparing single and multifactorial interventions. Age Ageing 2007, 36, 656–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherrington, C.; Fairhall, N.J.; Wallbank, G.K.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S.E. Exercise for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2019, 1. [Google Scholar] [CrossRef]
- Gómez-Cabello, A.; Ara, I.; González-Agüero, A.; Casajús, J.A.; Vicente-Rodríguez, G. Effects of Training on Bone Mass in Older Adults. Sports Med. 2012, 42, 301–325. [Google Scholar] [CrossRef]
- Lacroix, A.; Hortobágyi, T.; Beurskens, R.; Granacher, U. Effects of Supervised vs. Unsupervised Training Programs on Balance and Muscle Strength in Older Adults: A Systematic Review and Meta-Analysis. Sports Med. 2017, 47, 2341–2361. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Ratamess, N.A. Fundamentals of resistance training: Progression and exercise prescription. Med. Sci. Sports Exerc. 2004, 36, 674–688. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.S.; Nunes, J.P.; Schoenfeld, B.J. Selection of Resistance Exercises for Older Individuals: The Forgotten Variable. Sports Med. 2020, 50, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.J.; Mercer, V.S.; Giuliani, C.A.; Morey, M.C.; Sloane, C.; Williams, S. HIP ABDUCTOR EXERCISE AND LATERAL STABILITY IN OLDER ADULTS AT RISK OF FALLS. J. Geriatr. Phys. Ther. 2007, 30, 146–147. [Google Scholar] [CrossRef]
- Gafner, S.C.; Bastiaenen, C.H.G.; Ferrari, S.; Gold, G.; Trombetti, A.; Terrier, P.; Hilfiker, R.; Allet, L. The Role of Hip Abductor Strength in Identifying Older Persons at Risk of Falls: A Diagnostic Accuracy Study. Clin. Interv. Aging 2020, 15, 645–654. [Google Scholar] [CrossRef]
- Lanza, M.B.; Addison, O.; Ryan, A.S.; Perez, W.J.; Gray, V. Kinetic, muscle structure, and neuromuscular determinants of weight transfer phase prior to a lateral choice reaction step in older adults. J. Electromyogr. Kinesiol. 2020, 55, 102484. [Google Scholar] [CrossRef]
- McKinnon, N.B.; Connelly, D.M.; Rice, C.L.; Hunter, S.W.; Doherty, T.J. Neuromuscular contributions to the age-related reduction in muscle power: Mechanisms and potential role of high velocity power training. Ageing Res. Rev. 2017, 35, 147–154. [Google Scholar] [CrossRef]
- Jones, M.D.; Wewege, M.A.; Hackett, D.A.; Keogh, J.W.L.; Hagstrom, A.D. Sex Differences in Adaptations in Muscle Strength and Size Following Resistance Training in Older Adults: A Systematic Review and Meta-analysis. Sports Med. 2021, 51, 503–517. [Google Scholar] [CrossRef]
- Ejupi, A.; Lord, S.R.; Delbaere, K. New methods for fall risk prediction. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 407–411. [Google Scholar] [CrossRef]
- Howcroft, J.; Kofman, J.; Lemaire, E.D. Prospective Fall-Risk Prediction Models for Older Adults Based on Wearable Sensors. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 1812–1820. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, R.; Litvan, I.; Jung, T.P. Fall Prediction and Prevention Systems: Recent Trends, Challenges, and Future Research Directions. Sensors 2017, 17, 2509. [Google Scholar] [CrossRef] [Green Version]
- Hua, A.; Quicksall, Z.; Di, C.; Motl, R.; LaCroix, A.Z.; Schatz, B.; Buchner, D.M. Accelerometer-based predictive models of fall risk in older women: A pilot study. NPJ Digit. Med. 2018, 1, 25. [Google Scholar] [CrossRef]
- Noh, H.M.; Song, H.J.; Park, Y.S.; Han, J.; Roh, Y.K. Fall predictors beyond fall risk assessment tool items for acute hospitalized older adults: A matched case-control study. Sci. Rep. 2021, 11, 1503. [Google Scholar] [CrossRef] [PubMed]
- GholamHosseini, H.; Baig, M.M.; Connolly, M.J.; Lindén, M. A multifactorial falls risk prediction model for hospitalized older adults. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2014, 2014, 3484–3487. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.; Tham, Y.-C.; Chee, M.-L.; Tan, N.Y.Q.; Wong, K.-H.; Majithia, S.; Sabanayagam, C.; Lamoureux, E.; Wong, T.-Y.; Cheng, C.-Y. Falls and Recurrent Falls among Adults in A Multi-ethnic Asian Population: The Singapore Epidemiology of Eye Diseases Study. Sci. Rep. 2018, 8, 7575. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Davis, Marra, Robertson, Khan, Najafzadeh, Ashe and Liu-Ambrose [76], 2011 1 | Liang, Wang, Jiang, Tan and Yang [77], 2020 | Liu-Ambrose, Khan, Eng, Janssen, Lord and McKay [78], 2004 | Tuunainen, Rasku, Jäntti, Moisio-Vilenius, Mäkinen, Toppila and Pyykkö [80], 2013 | Woo, Hong, Lau and Lynn [79], 2007 | ||
|---|---|---|---|---|---|---|
| Sample | ||||||
| Age (years; mean ± SD) | 70 ± 0 | 69 ± 3 | 87 ± 5 | 80 ± 2 | 85 ± 6 | 69 ± 3 |
| Sex | 100% female | 100% female | 37% female | 100% female | 66% female | 50% female |
| Intervention participants (n) | 54 | 52 | 30 | 32 | 18 | 60 |
| Comparator participants (n) | 49 | 30 | 66 | 37 | 120 | |
| Training status | 116.2 ± 61.4 2 | 121.2 ± 60.4 2 | 3.8 ± 1.8 3 | 98.0 ± 51.8 2 | Not reported | Physically active |
| Intervention country | Canada | China | Canada | Finland | China | |
| Single/multicenter | Multi (community-dwelling) | Single (post-acute care unit in a public hospital) | Multi (community-dwelling) | Single (residential facility) | Multi (community-dwelling) | |
| Interventions | ||||||
| Days | 365 | 365 | 84 | 175 | 91 | 365 |
| Follow-up | Not reported | Not reported | Not reported | 3 years | Not reported | |
| Weekly frequency | 1× | 2× | 2× | 2× | 2× | 3× |
| Type of ST | ST | ST | ST | ST | ST | ST |
| Volume | 2 sets of 6–8 repetitions | 2 sets of 6–8 repetitions | 3 sets of 8–12 repetitions each (2-min rest between sets) | 2 sets of 6–8 repetitions | 3 repetitions and after 9th training session with 2 sets of 10–20 repetitions | 1 set of 30 repetitions |
| Exercises | (n = 10) 4 | (n = 10) 4 | (n = 7) 5 | (n = 10) 6 | (n = 11) 7 | (n = 6) 8 |
| Intensity | High and increased using the 7-RM method | High and increased using the 7-RM method | 70–80% of 1-RM | High and increased using the 7-RM method | Progressive intensity | Medium and not progressive |
| Duration | 60 min | 60 min | 55 min | 50 min | 60 min | Not reported |
| Prescription | Individualized | Individualized | Individualized | Individualized | Individualized | Group-based |
| Professional qualification of supervisors | ST certified (fitness coach) | ST certified (fitness coach) | No ST certified (physiotherapist) | ST certified (fitness coach) | ST certified (physiotherapist) | Not reported |
| Supervision ratio | Not reported | Not reported | Not reported | 1:2 | 1:2.5 | Not reported |
| Attendance rates | 71% | 70% | Not reported | 85% | Not reported | 76% |
| Funding sources | ||||||
| Vancouver Foundation, Michael Smith Foundation for Health Research, Centre for Hip Health and Mobility | National Key R&D Program of China | Vancouver Foundation | EU PROFANE and the Pirkanmaa Cultural and Science Foundation | Council of Hong Kong | ||
| Conflicts of interest | ||||||
| None | None | Not reported | None | None | ||
| Davis, Marra, Robertson, Khan, Najafzadeh, Ashe and Liu-Ambrose [76], 2011 | ||||||
| Primary outcomes | Once-weekly ST | Twice-weekly ST | Twice-weekly balance and tone | |||
| Total number of falls | 30 | 32 a | 38 | |||
| Falls rate per person | 0.56 | 0.62 | 0.78 | |||
| Incidence Rate Ratio (falls) | −27% (0.73; 95%IC = 0.44–1.23) ns | −12% (0.88; 95%IC = 0.67–1.16) ns | Reference | |||
| Liang, Wang, Jiang, Tan and Yang [77], 2020 | ||||||
| Primary outcomes | ST Group | ST + Balance Group | ||||
| Fallers | 23% (7/30) | 13% (4/30) | ||||
| Risk ratio (RR) | +11% (0.89; 95%IC = 0.69–1.13) ns | Reference | ||||
| Liu-Ambrose, Khan, Eng, Janssen, Lord and McKay [78], 2004 | ||||||
| Primary outcomes | ST Group | Stretching Group | Agility Group | |||
| Total number of falls | 18 (one subject fell seven times) | 10 | 11 | |||
| Frequent fallers a | 9% (3/32) | 6% (2/32) | 15% (5/34) | |||
| PPA fall-risk scores | −57% | −20% | −48% | |||
| ES | (95% CI) | ES | (95% CI) | ES | (95% CI) | |
| Fall-risk score (points) | −1.39 | (–1.94 to −0.84) | −0.39 | (−0.89–0.10) | −0.78 | (−1.78 to −0.28) |
| Tuunainen, Rasku, Jäntti, Moisio-Vilenius, Mäkinen, Toppila and Pyykkö [80], 2013 | ||||||
| Primary outcomes | ST Group | Self-administered training Group | ST + Balance Group | |||
| Fallers (follow up) | 7 | 14 | 6 | |||
| Frequent fallers (follow up) | 6 | 9 | 5 | |||
| Total number of falls (range in follow up) | 42 (1–21) | 64 (1–30) | 24 (1–8) | |||
| Mean risk of fall | 0.47 ± 0.52 | 0.73 ± 0.37 | 0.42 ± 0.49 | |||
| Woo, Hong, Lau and Lynn [79], 2007 | ||||||
| Primary outcomes | ST Group | Tai Chi Group | Control Group | |||
| Total number of falls | 24 (24/60) | 15 (15/60) | 31 (31/60) | |||
| Study | D1 | D2 | D3 | D4 | D5 | Overall |
|---|---|---|---|---|---|---|
| Davis, Marra, Robertson, Khan, Najafzadeh, Ashe and Liu-Ambrose [76], 2011 |  | | | | | |
| Liang, Wang, Jiang, Tan and Yang [77], 2020 | | | | |  | |
| Liu-Ambrose, Khan, Eng, Janssen, Lord and McKay [78], 2004 |  | | | | | |
| Tuunainen, Rasku, Jäntti, Moisio-Vilenius, Mäkinen, Toppila and Pyykkö [80], 2013 | | | | | | |
| Woo, Hong, Lau and Lynn [79], 2007 | | | | | | |
Low risk of bias. Some concerns. High risk of bias.| Outcomes | Study Design | Risk of Bias in Individual Studies | Risk of Publication Bias | Inconsistency | Indirectness | Imprecision | Certainty of Evidence | Recommendation |
|---|---|---|---|---|---|---|---|---|
| Risk of falling | 5 RCTs with 6 trials and 541 participants. | Moderate to high 1 | Not assessed 2 | Low 3 | Moderate 4 | High 5 | ⨁◯◯◯ Very-low 6 | ST produces favorable effects that are similar to other unimodal or multimodal training programs on falls among older adults. Currently, no recommendation can be provided in favor (or against) of any ST program. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Claudino, J.G.; Afonso, J.; Sarvestan, J.; Lanza, M.B.; Pennone, J.; Filho, C.A.C.; Serrão, J.C.; Espregueira-Mendes, J.; Vasconcelos, A.L.V.; de Andrade, M.P.; et al. Strength Training to Prevent Falls in Older Adults: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 3184. https://doi.org/10.3390/jcm10143184
Claudino JG, Afonso J, Sarvestan J, Lanza MB, Pennone J, Filho CAC, Serrão JC, Espregueira-Mendes J, Vasconcelos ALV, de Andrade MP, et al. Strength Training to Prevent Falls in Older Adults: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2021; 10(14):3184. https://doi.org/10.3390/jcm10143184
Chicago/Turabian StyleClaudino, João Gustavo, José Afonso, Javad Sarvestan, Marcel Bahia Lanza, Juliana Pennone, Carlos Alberto Cardoso Filho, Julio Cerca Serrão, João Espregueira-Mendes, Ana Luiza Vilefort Vasconcelos, Monique Paula de Andrade, and et al. 2021. "Strength Training to Prevent Falls in Older Adults: A Systematic Review with Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 10, no. 14: 3184. https://doi.org/10.3390/jcm10143184