
Improvement of the Quality of Life in Aging by Stimulating Autobiographical Memory

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Instruments
2.3. Process
2.4. Description of the Treatment and Control Groups (AD, HA and MCI)
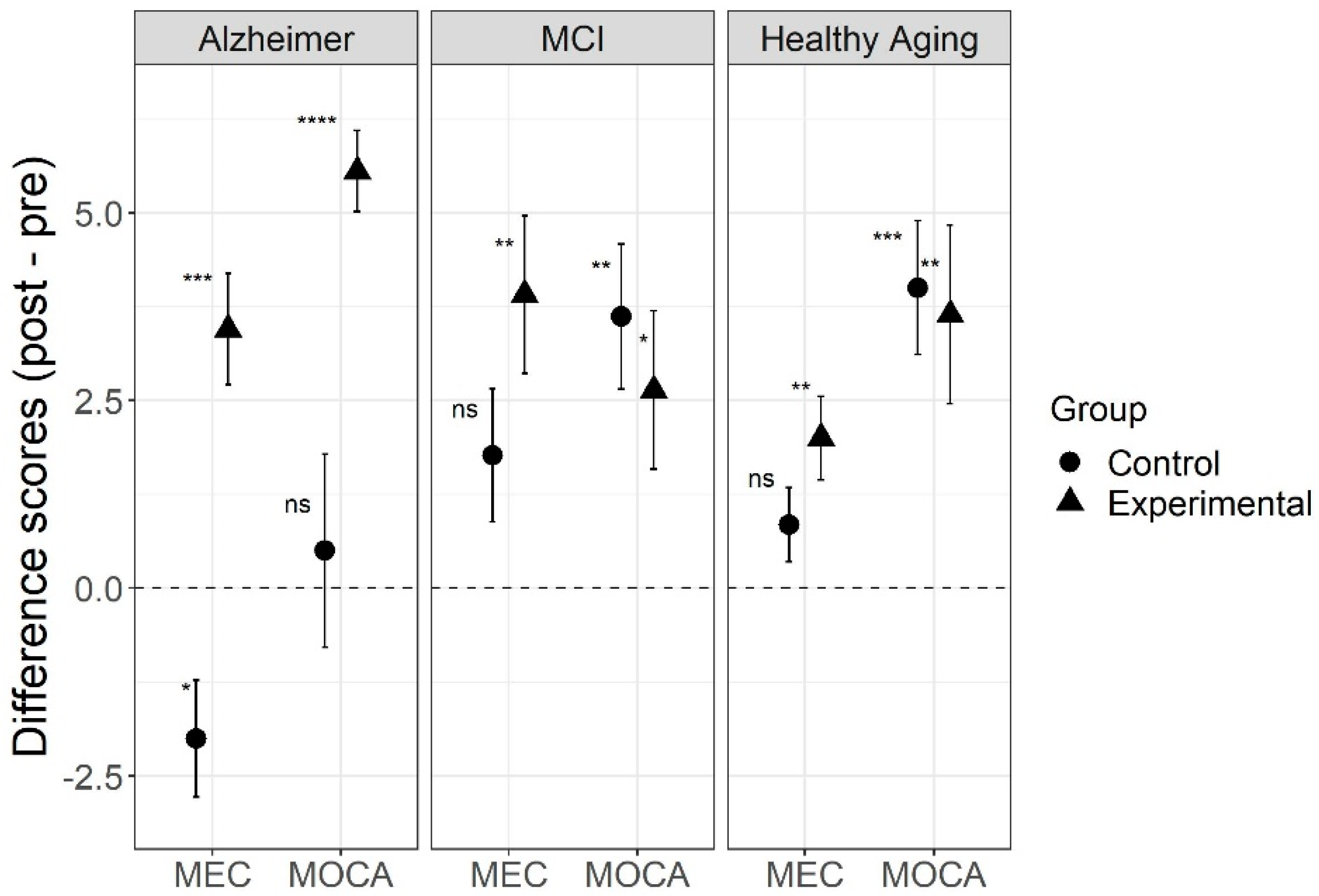
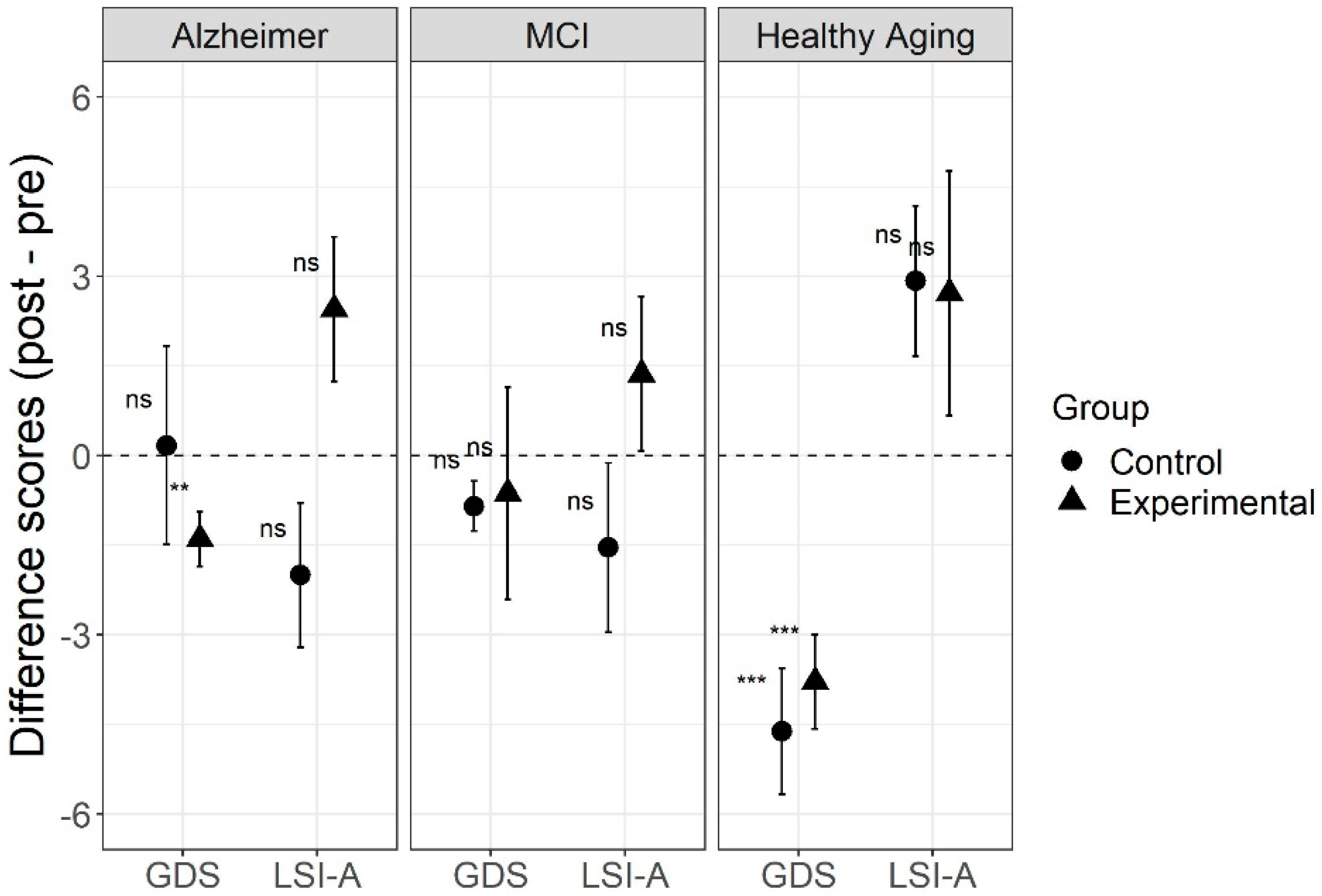
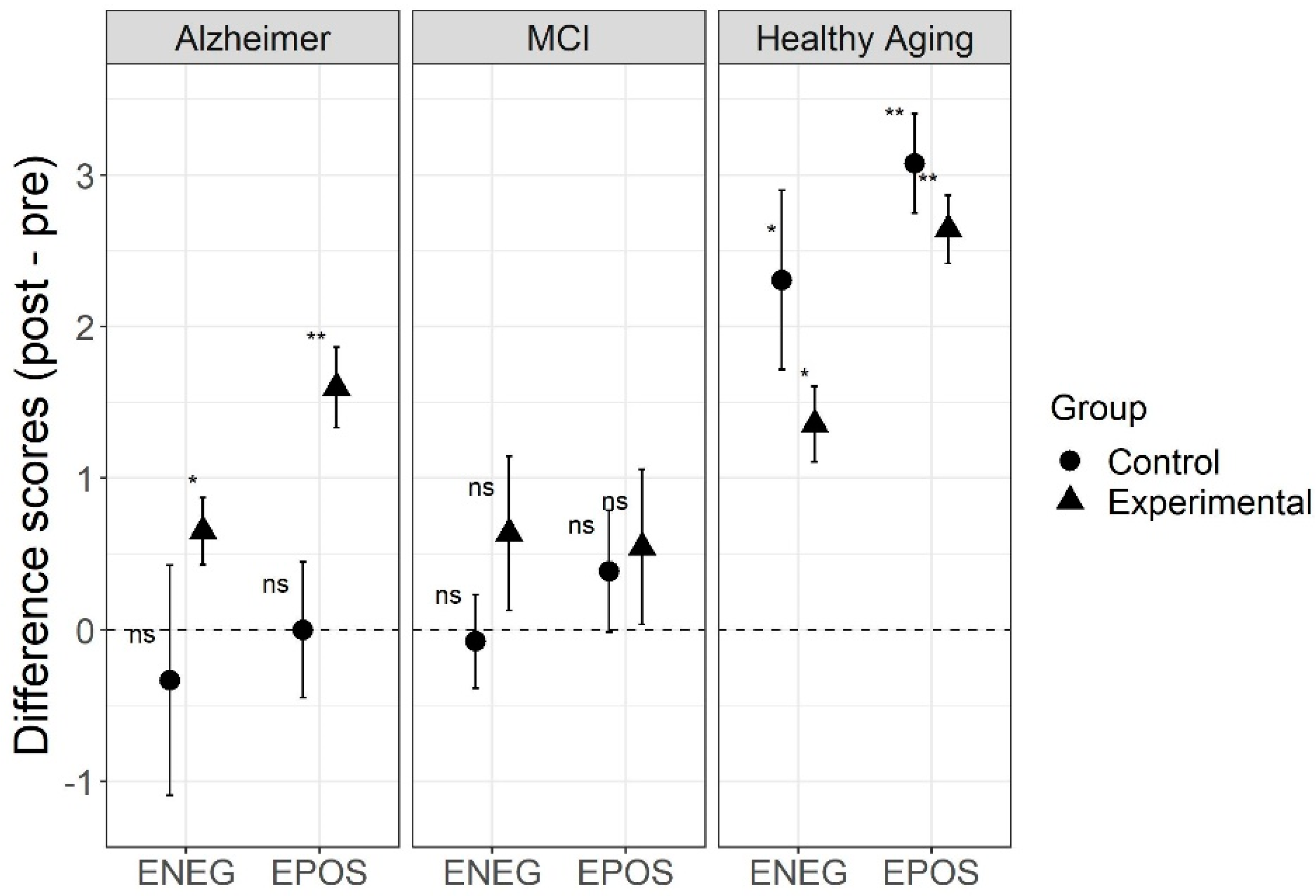
3. Results
Data Analyses
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andreu, M.; Pedra, M.; Pérez, M.E. La adaptación a la jubilación y sus fases: Afectación de los niveles de satisfacción y duración del proceso adaptativo. An. Psicol. 2010, 26, 80–88. [Google Scholar]
- Moral, M.J. Programas intergeneracionales y participación social: La integración de los adultos mayores españoles y latinoamericanos en la comunidad [Intergenerational programs and social participation: The integration of spanish and latin-american seniors in the community]. Univ. Psychol. 2017, 16, 157–175. [Google Scholar] [CrossRef] [Green Version]
- Nacional de Estadística y Geografía, INEGI. Available online: http://www.beta.inegi.org.mx/temas/estructura/ (accessed on 19 December 2018).
- Córdoba, A.M.; Rodríguez, A.F.; Camacho, Y.J.; Gómez, H.V. Functional dependence and chronic pain associated with the quality of life among the elderly. Psicogente 2017, 20, 398–409. [Google Scholar] [CrossRef] [Green Version]
- Niu, H.; Álvarez-Álvarez, I.; Guillén-Grima, F.; Aguinaga-Ontoso, I. Prevalence and incidence of Alzheimer’s disease in Europe: A meta-analysis. Neurología 2017, 32, 523–532. [Google Scholar] [CrossRef]
- Bayard, R.I.; Rodríguez, J.D.; Llerena, T.Z.; Ulloa, E.H. Overcome the stigma to dementia, a challenge to the Cuban society. Rev. Habanera Cienc. Méd. 2017, 16, 135–145. [Google Scholar]
- Gramunt-Fombuena, N. Vive el Envejecimiento Activo; Obra Social Fundación “la Caixa”: Barcelona, Spain, 2010. [Google Scholar]
- González-Arévalo, K.A. Terapia de reminiscencia y sus efectos en los pacientes mayores con demencia. Psicogeriatría 2015, 5, 101–111. [Google Scholar]
- Irazoki, E.; García-Casal, J.A.; Sánchez-Meca, J.; Franco-Martín, M. Efficacy of group reminiscence therapy for people with dementia. Systematic literature review and meta-analysis. Rev. Neurol. 2017, 65, 447–456. [Google Scholar] [CrossRef]
- Carballo-García, V.; Arroyo-Arroyo, M.R.; Portero-Díaz, M.; de León, J.R.S. Effects of non-pharmacological therapy on normal ageing and on cognitive decline: Reflections on treatment objectives. Neurología 2013, 28, 160–168. [Google Scholar] [CrossRef]
- Olazarán, J.; Reisberg, B.; Clare, L.; Cruz, I.; Peña-Casanova, J.; Del Ser, T.; Woods, B.; Beck, C.; Auer, S.; Lai, C.; et al. Nonpharmacological therapies in Alzheimer’s disease: A systematic review of efficacy. Dement. Geriatr. Cogn. Disord. 2010, 30, 161–178. [Google Scholar] [CrossRef]
- Woods, B.; O’Philbin, L.; Farrell, E.M.; Spector, A.E.; Orrell, M. Reminiscence therapy for dementia. Cochrane Database Syst. Rev. 2018, 2018, CD001120. [Google Scholar] [CrossRef] [Green Version]
- Dempsey, L.; Murphy, K.; Cooney, A.; Casey, D.; O´Shea, E.; Devane, D.; Jordan, F.; Hunter, A. Reminiscence in dementia: A concept analysis. Dementia 2014, 13, 176–192. [Google Scholar] [CrossRef]
- Justo-Henriques, S.I.; Pérez-Sáez, E.; Apóstolo, J.L. Individual intervention protocol based on reminiscence therapy for older people with neurocognitive disorders. Rev. Enferm. Ref. 2020, 5, e20043. [Google Scholar] [CrossRef]
- Salazar-Villanea, M. Identidad personal y memoria en adultos mayores sin demencia y con enfermedad de Alzheimer. Actual. Psicol. 2007, 21, 1–37. [Google Scholar] [CrossRef] [Green Version]
- Terrero, F.B. Reminiscencia en Adultos Mayores no Institucionalizados de República Dominicana: Seguimiento de una Intervención. Ph.D. Thesis, Universidad de Valencia, Valencia, Spain, 2016. [Google Scholar]
- Afonso, R.M.; Bueno, B.; Loureiro, M.J.; Pereira, H. Reminiscence, psychological well-being, and ego integrity in Portuguese elderly people. Educ. Gerontol. 2011, 37, 1063–1080. [Google Scholar] [CrossRef]
- Kirk, M.; Rasmussen, K.W.; Overgaard, S.B.; Berntsen, D. Five weeks of immersive reminiscence therapy improves autobiographical memory in Alzheimer’s disease. Memory 2019, 27, 441–454. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, C.Y. Envejecimiento: Evaluación e Interpretación Psicológica; Manual Moderno: Mexico City, Mexico, 2017. [Google Scholar]
- Justo-Henriques, S.I.; Pérez-Sáez, E.; Alves Apóstolo, J.L. Multicentre randomised controlled trial about the effect of individual reminiscence therapy in older adults with neurocognitive disorders. Int. J. Geriatr. Psychiatry 2021, 36, 704–712. [Google Scholar] [CrossRef]
- Pérez-Sáez, E.; Justo-Henriques, S.I.; Alves Apóstolo, J.L. Multicenter randomized controlled trial of the effects of individual reminiscence therapy on cognition, depression and quality of life: Analysis of a sample of older adults with Alzheimer’s disease and vascular dementia. Clin. Neuropsychol. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Huang, H.C.; Chen, Y.T.; Chen, P.Y.; Huey-Lan Hu, S.; Liu, F.; Kuo, Y.L.; Chiu, H.Y. Reminiscence therapy improves cognitive functions and reduces depressive symptoms in elderly people with dementia: A meta-analysis of randomized controlled trials. J. Am. Med. Dir. Assoc. 2015, 16, 1087–1094. [Google Scholar] [CrossRef]
- Park, K.; Lee, S.; Yang, J.; Song, T. A systematic review and meta-analysis on the effect of reminiscence therapy for people with dementia. Int. Psychogeriatr. 2019, 31, 1581–1597. [Google Scholar] [CrossRef] [Green Version]
- Subramaniam, P.; Woods, B.; Whitaker, C. Life review and life story books for people with mild to moderate dementia: A randomised controlled trial. Aging Ment. Health 2014, 18, 363–375. [Google Scholar] [CrossRef]
- Cabaco, A.S. Los Niveles de Cognición Instruccional Positiva: Programa de Reminiscencia Cip-Cetys Para Optimizar el Bienestar en Adultos Mayores; Cetys Universidad: Mexicali, Mexico, 2019. [Google Scholar]
- Villar, F.; Serrat, R. Talk to them: Narrative care within a person-centered care framework. Rev. Esp. Geriatría Gerontol. 2017, 52, 216–222. [Google Scholar] [CrossRef]
- Gallego, M.L.; Ferrándiz, M.H.; Garriga, O.T.; Nierga, I.P.; López-Pousa, S.; Franch, J.V. Validación del Montreal Cognitive Assessment (MoCA): Test de cribado para el deterioro cognitivo leve. Datos preliminares. Alzheimer Real Investig. Demenc. 2009, 43, 4–11. [Google Scholar]
- Larner, A.J. Screening utility of the Montreal Cognitive Assessment (MoCA): In place of-or as well as-the MMSE? Int. Psychogeriatr. 2012, 24, 391–396. [Google Scholar] [CrossRef]
- Olazarán, J.; Clare, L. S2-04-02: Non-pharmacological therapies in Alzheimer’s disease: A systematic review of efficacy. Alzheimer’s Dement. 2006, 2, S28. [Google Scholar] [CrossRef]
- Lobo, A.; López-Antón, R.; De-La-Cámara, C.; Quintanilla, M.Á.; Campayo, A.; Saz, P.; Zarademp Workgroup. Non-cognitive psychopathological symptoms associated with incident mild cognitive impairment and dementia, Alzheimer’s type. Neurotox Res. 2008, 14, 263–272. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1983, 17, 37–49. [Google Scholar] [CrossRef]
- Fernández-San Martín, M.I.; Andrade-Rosa, C.; Molina, J.D.; Muñoz, P.E.; Carretero, B.; Rodríguez, M.; Silva, A. Validation of the Spanish version of the geriatric depression scale (GDS) in primary care. Int. J. Geriatr. Psychiatry 2002, 17, 279–287. [Google Scholar] [CrossRef]
- Camacho-Conde, J.A.; Galán-López, J.M. The relationship between depression and cognitive deterioration in elderly persons. Psicol. Teoria Pesqui. 2021, 37, e37413. [Google Scholar] [CrossRef]
- Neugarten, B.L.; Havighurst, R.J.; Tobin, S.S. The measurement of life satisfaction. J. Gerontol. 1961, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Latorre, J.M.; Ricarte, J.J.; Serrano, J.P.; Ros, L.; Navarro, B.; Aguilar, M.J. Performance in autobiographical memory of older adults with depression symptoms. Appl. Cogn. Psychol. 2013, 27, 167–172. [Google Scholar] [CrossRef]
- Ocampo, L.P.L.; Oviedo, L.M.F.; Ceballos, F.V. Predictive capacity of a battery of neuropsychological tests in the early diagnosis of mild cognitive impairment (MCI) in a group of adults. Encuentros 2015, 13, 25–35. [Google Scholar] [CrossRef] [Green Version]
- Cabaco, A.S. La cognicion instruccional positiva para promover habitos saludables en adultos mayores ¿una propuesta para la decada del envejecimiento activo? In Guia Practica de Memoria; A. S. Cabaco (Coord.); UPSA: Salamanca, Spain, 2016; pp. 13–22. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.r-project.org/ (accessed on 13 March 2021).
- Rstatix: Pipe-Friendly Framework for Basic Statistical Tests. Available online: https://CRAN.R-project.org/package=rstatix (accessed on 13 March 2021).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Mair, P.; Wilcox, R.R. Robust statistical methods in R using the WRS2 package. Behav. Res. 2020, 52, 464–488. [Google Scholar] [CrossRef] [PubMed]
- MOTE: Measure of the Effect. Available online: http://github.com/doomlab/MOTE (accessed on 13 March 2021).
- Petersen, R.C. MCI treatment trials: Failure or not? Lancet Neurol. 2007, 6, 473–475. [Google Scholar] [CrossRef]
- Forlenza, O.V.; Chiu, E. Mild cognitive impairment: A concept ready to move on? Curr. Opin. Psychiatry 2008, 21, 529–532. [Google Scholar] [CrossRef]
- Afonso, R.; Bueno, B. Reminiscencia con distintos tipos de recuerdos autobiográficos: Efectos sobre la reducción de la sintomatología depresiva en la vejez [Reminiscence with different types of autobiographical memories: Effects on the reduction of depressive symptomatology in old age]. Psicothema 2010, 22, 213–220. [Google Scholar]
- Bohlmeijer, E.; Smit, F.; Cuijpers, P. Effects of reminiscence and life review on late-life depression: A meta-analysis. Int. J. Geriatr. Psychiatry 2003, 18, 1088–1094. [Google Scholar] [CrossRef] [PubMed]
- Cappeliez, P.; O’Rourke, N. Empirical validation of a model of reminiscence and health in later life. J. Gerontol. Ser. B 2006, 61, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Rueda, A.V. Reminiscencia Positiva en el Adulto Mayor con Deterioro Cognitivo Leve. Master’s Thesis, Universidad de Sevilla, Sevilla, Spain, 2017. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Groups | AD | MCI | HA | Total |
|---|---|---|---|---|
| Control | 6 | 13 | 13 | 32 |
| Experimental | 20 | 11 | 14 | 45 |
| Total | 26 | 24 | 27 | 77 |
| Session | Positive Reminiscence | Cognitive Stimulation |
|---|---|---|
| 1 | Introduction to reminiscence | Keys to optimize registration: concentration |
| 2 | Things of everyday life | Organization of information |
| 3 | I present-past-future | Display and erroneous attributions |
| 4 | Relationships | Importance of language |
| 5 | Important dates | Routes and semantic knowledge |
| 6 | Popular parties | Understanding of texts and procedural knowledge |
| 7 | Work and labor | Calculation and arithmetic |
| 8 | Games | Calculation capacity development |
| 9 | Remembering loved ones | Relational memory training I |
| 10 | Music and memories | Relational memory training II |
| 11 | Reirpos (positive emotions through laughter) | Importance of care and self-regulation |
| 12 | Laugh more live more | Breathe |
| Control | Experimental | |||
|---|---|---|---|---|
| Pre | Post | Pre | Post | |
| AD group | n = 6 | n = 20 | ||
| MoCA | 19.2 (5.23) | 19.7 (2.58) | 11.7 (3.21) | 17.2 (3.32) |
| MEC | 28 (1.90) | 26 (2.45) | 20.4 (3.22) | 23.9 (2.77) |
| GDS-30 | 7.67 (2.16) | 7.83 (4.62) | 9.2 (4.20) | 7.8 (4.03) |
| LSI-A | 27 (6.51) | 25 (7.69) | 24.6 (5.46) | 27.0 (5.84) |
| AMT-EPOS | 2.17 (0.75) | 2.17 (0.41) | 1.9 (0.97) | 3.5 (0.89) |
| AMT-ENEG | 2.5 (1.23) | 2.17 (0.75) | 2.15 (1.09) | 2.8 (0.89) |
| MCI group | n = 13 | n = 11 | ||
| MoCA | 11.2 (4.25) | 14.8 (3.36) | 13.1 (4.59) | 15.7 (5.08) |
| MEC | 19.9 (3.45) | 21.7 (3.40) | 19.6 (3.98) | 23.5 (4.53) |
| GDS-30 | 13.5 (5.55) | 12.6 (6.53) | 13.4 (5.57) | 12.7 (6.40) |
| LSI-A | 22.6 (6.5) | 21.1 (6.75) | 20.4 (4.41) | 21.7 (6.25) |
| AMT-EPOS | 1.23 (1.17) | 1.62 (0.77) | 1.36 (1.12) | 1.91 (1.14) |
| AMT-ENEG | 2.46 (0.88) | 2.38 (1.04) | 1.73 (1.42) | 2.36 (1.21) |
| HA group | n = 13 | n = 14 | ||
| MoCA | 17.6 (3.62) | 21.6 (2.53) | 20.7 (4.27) | 24.4 (3.15) |
| MEC | 26.4 (1.39) | 27.2 (2.24) | 28.6 (2.53) | 30.6 (2.85) |
| GDS-30 | 15.1 (4.70) | 10.5 (3.53) | 11.9 (5.10) | 8.07 (3.91) |
| LSI-A | 18.5 (5.88) | 21.5 (3.69) | 22.4 (5.26) | 25.1 (5.01) |
| AMT-EPOS | 1.23 (0.93) | 4.31 (0.95) | 1.79 (0.80) | 4.43 (1.02) |
| AMT-ENEG | 1.62 (1.50) | 3.92 (1.60) | 2.86 (0.54) | 4.21 (0.98) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villasán Rueda, A.; Sánchez Cabaco, A.; Mejía-Ramírez, M.; Justo-Henriques, S.I.; Carvalho, J.O. Improvement of the Quality of Life in Aging by Stimulating Autobiographical Memory. J. Clin. Med. 2021, 10, 3168. https://doi.org/10.3390/jcm10143168
Villasán Rueda A, Sánchez Cabaco A, Mejía-Ramírez M, Justo-Henriques SI, Carvalho JO. Improvement of the Quality of Life in Aging by Stimulating Autobiographical Memory. Journal of Clinical Medicine. 2021; 10(14):3168. https://doi.org/10.3390/jcm10143168
Chicago/Turabian StyleVillasán Rueda, Alba, Antonio Sánchez Cabaco, Manuel Mejía-Ramírez, Susana I. Justo-Henriques, and Janessa O. Carvalho. 2021. "Improvement of the Quality of Life in Aging by Stimulating Autobiographical Memory" Journal of Clinical Medicine 10, no. 14: 3168. https://doi.org/10.3390/jcm10143168