
An Updated Meta-Analysis of RCTs of Colchicine for Stroke Prevention in Patients with Coronary Artery Disease

 , ,
, ,
Abstract
:1. Introduction
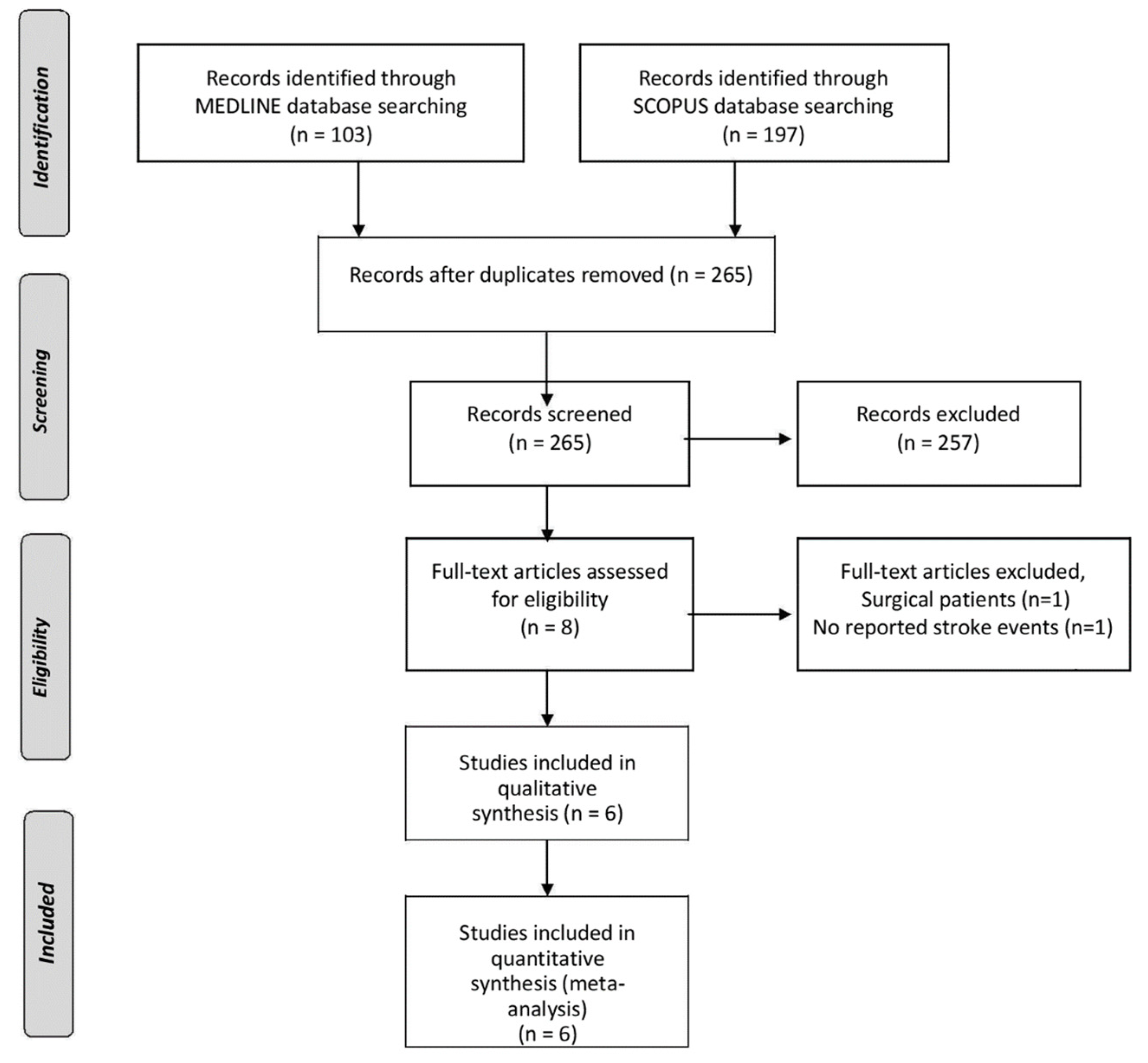
2. Materials
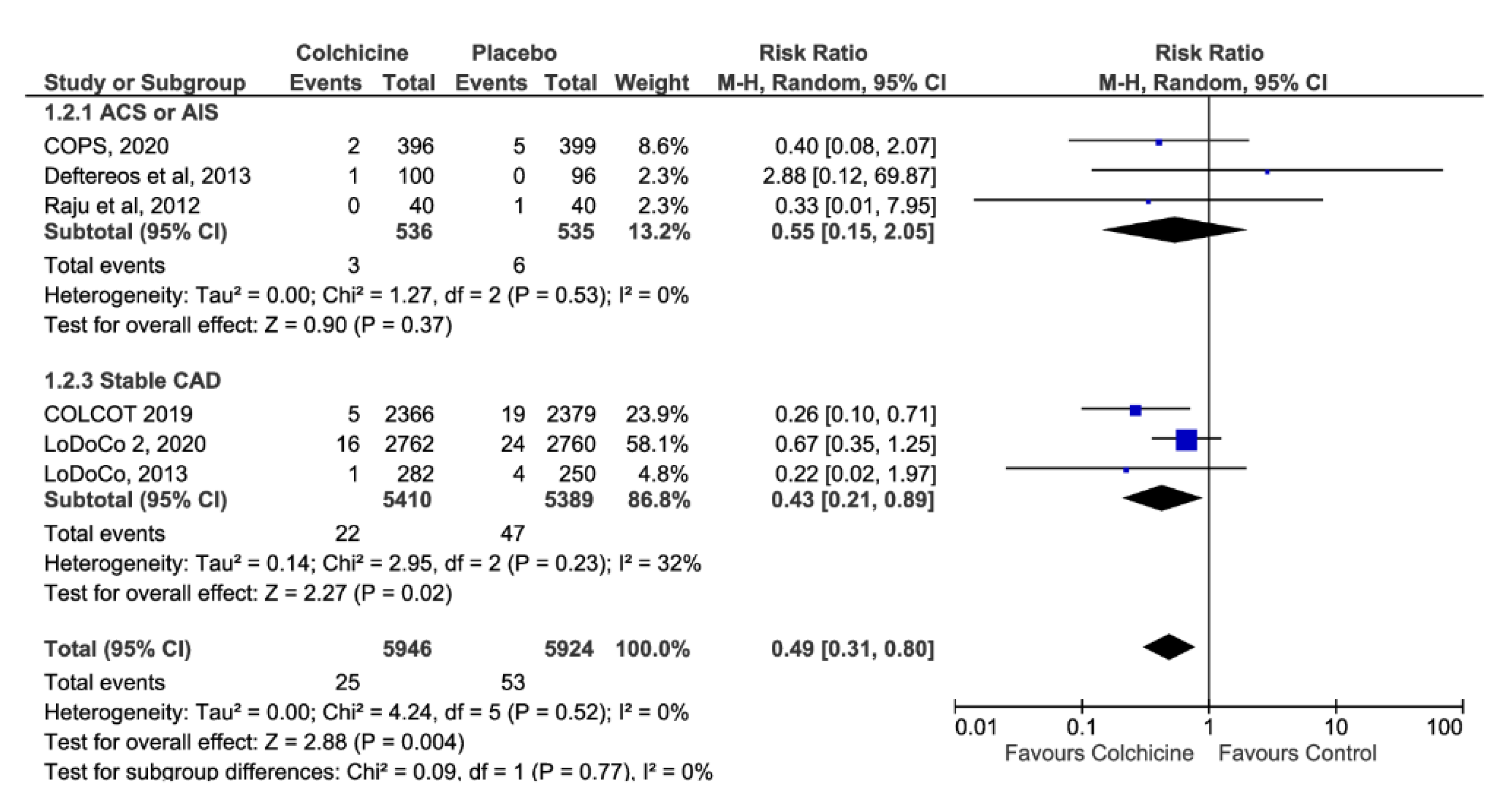
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tardif, J.-C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N. Engl. J. Med. 2019, 381, 2497–2505. [Google Scholar] [CrossRef] [PubMed]
- Deftereos, S.; Giannopoulos, G.; Raisakis, K.; Kossyvakis, C.; Kaoukis, A.; Panagopoulou, V.; Driva, M.; Hahalis, G.; Pyrgakis, V.; Alexopoulos, D.; et al. Colchicine treatment for the prevention of bare-metal stent restenosis in diabetic patients. J. Am. Coll. Cardiol. 2013, 61, 1679–1685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nidorf, S.M.; Eikelboom, J.; Budgeon, C.A.; Thompson, P.L. Low-Dose Colchicine for Secondary Prevention of Cardiovascular Disease. J. Am. Coll. Cardiol. 2013, 61, 404–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raju, N.C.; Yi, Q.; Nidorf, M.; Fagel, N.D.; Hiralal, R.; Eikelboom, J. Effect of colchicine compared with placebo on high sensitivity C-reactive protein in patients with acute coronary syndrome or acute stroke: A pilot randomized controlled trial. J. Thromb. Thrombolysis 2012, 33, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Katsanos, A.H.; Palaiodimou, L.; Price, C.; Giannopoulos, S.; Lemmens, R.; Kosmidou, M.; Georgakis, M.K.; Weimar, C.; Kelly, P.J.; Tsivgoulis, G. Colchicine for stroke prevention in patients with coronary artery disease: A systematic review and meta-analysis. Eur. J. Neurol. 2020, 27, 1035–1038. [Google Scholar] [CrossRef] [PubMed]
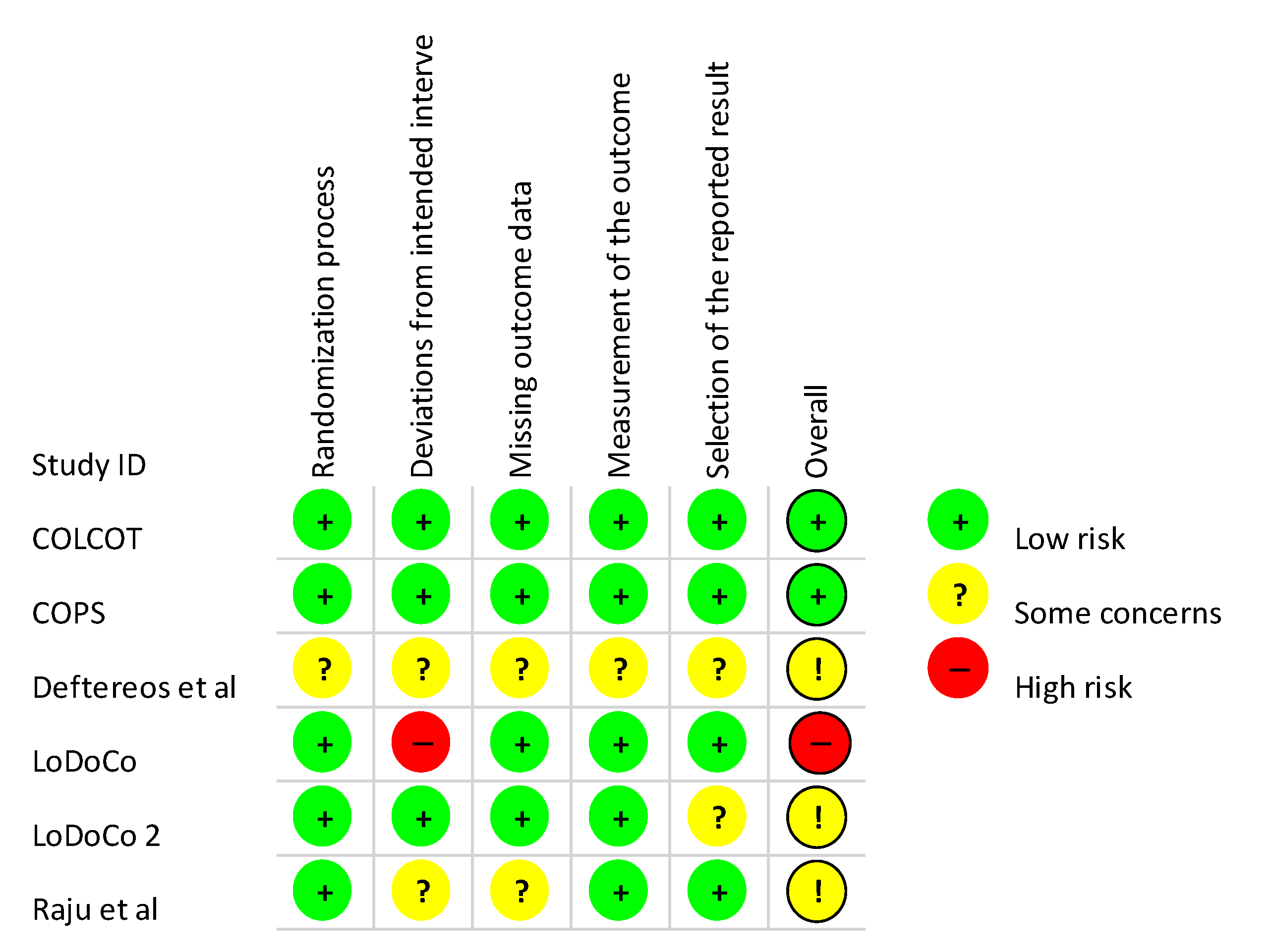
- Sterne, J.A.C.; Savović, J.; Page, M.; Elbers, R.G.; Blencowe, N.; Boutron, I.; Cates, C.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nidorf, S.M.; Fiolet, A.T.; Mosterd, A.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.; The, S.H.; Xu, X.-F.; Ireland, M.A.; Lenderink, T.; et al. Colchicine in Patients with Chronic Coronary Disease. N. Engl. J. Med. 2020, 383, 1838–1847. [Google Scholar] [CrossRef] [PubMed]
- Tong, D.C.K.; Quinn, S.; Nasis, A.; Hiew, C.; Roberts-Thomson, P.; Adams, H.; Sriamareswaran, R.; Htun, N.M.; Wilson, W.; Stub, D.; et al. Colchicine in Patients with Acute Coronary Syndrome: The Australian COPS Randomized Clinical Trial. Circulation 2020, 142, 1890–1900. [Google Scholar] [CrossRef] [PubMed]
- Falk, E.; Shah, P.K.; Fuster, V. Coronary Plaque Disruption. Circulation 1995, 92, 657–671. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Progress and challenges in translating the biology of atherosclerosis. Nature 2011, 473, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Abela, G.S. Cholesterol crystals piercing the arterial plaque and intima trigger local and systemic inflammation. J. Clin. Lipidol. 2010, 4, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Duewell, P.; Kono, H.; Rayner, K.; Sirois, C.M.; Vladimer, G.; Bauernfeind, F.G.; Abela, G.S.; Franchi, L.; Nuñez, G.; Schnurr, M.; et al. NLRP3 inflammasomes are required for atherogenesis and activated by cholesterol crystals. Nature 2010, 464, 1357–1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajamäki, K.; Lappalainen, J.; Öörni, K.; Välimäki, E.; Matikainen, S.; Kovanen, P.T.; Eklund, K.K. Cholesterol Crystals Activate the NLRP3 Inflammasome in Human Macrophages: A Novel Link between Cholesterol Metabolism and Inflammation. PLoS ONE 2010, 5, e11765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libby, P. Inflammation in atherosclerosis. Nature 2002, 420, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Katsanos, A.H.; Hart, R.G. New Horizons in Pharmacologic Therapy for Secondary Stroke Prevention. JAMA Neurol. 2020, 77, 1308. [Google Scholar] [CrossRef] [PubMed]
- Colchicine for Prevention of Vascular Inflammation in Non-CardioEmbolic Stroke (CONVINCE)—A Randomised Clinical Trial of Low-Dose Colchicine for Secondary Prevention after Stroke. Available online: https://clinicaltrials.gov/ct2/show/NCT02898610 (accessed on 23 November 2019).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Name | Population | Number of Patients | Dose | Median Follow-Up | Age (Years) | Males | Smoking | HTN | DM | History of ASCVD | History of Stroke/TIA |
|---|---|---|---|---|---|---|---|---|---|---|---|
| COLCOT, 2019 [1] | MI within 1 month | 4745 | 0.5 mg OD | 22.6 months | 60.6 ± 10.7 | 81% | 30% | 51% | 20% | 16% | 3% |
| COPS, 2020 [8] | ASCVD | 795 | 0.5 mg BID (1 month)/0.5 mg OD (11 months) | 12 months | 59.8 ± 10.3 | 79% | 35% | 50% | 19% | 15% | 2% |
| Deftereos et al., 2013 [2] | Diabetics undergoing PCI | 196 | 0.5 mg BID | 6 months | 63.6 ± 7.0 | 65% | 38% | 49% | 100% | 31% | N/A |
| LoDoCo, 2013 [3] | ASCVD | 532 | 0.5 mg OD | 36 months | 66 ± 9.2 | 89% | 5% | N/A | 30% | 23% | N/A |
| LoDoCo 2, 2020 [7] | ASCVD | 5522 | 0.5 mg OD | 28.6 months | 66 ± 8.6 | 85% | 12% | 51% | 18% | 84% | N/A |
| Raju et al., 2012 [4] | ASCVD or AIS | 80 | 1 mg OD | 1 month | 57.2 ± 10.0 | 89% | 79% | 43% | 16% | 18% | 4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katsanos, A.H.; Palaiodimou, L.; Price, C.; Themistocleous, M.; Lemmens, R.; Michopoulos, I.; Georgakis, M.K.; Weimar, C.; Kelly, P.; Tsivgoulis, G. An Updated Meta-Analysis of RCTs of Colchicine for Stroke Prevention in Patients with Coronary Artery Disease. J. Clin. Med. 2021, 10, 3110. https://doi.org/10.3390/jcm10143110
Katsanos AH, Palaiodimou L, Price C, Themistocleous M, Lemmens R, Michopoulos I, Georgakis MK, Weimar C, Kelly P, Tsivgoulis G. An Updated Meta-Analysis of RCTs of Colchicine for Stroke Prevention in Patients with Coronary Artery Disease. Journal of Clinical Medicine. 2021; 10(14):3110. https://doi.org/10.3390/jcm10143110
Chicago/Turabian StyleKatsanos, Aristeidis H., Lina Palaiodimou, Christopher Price, Marios Themistocleous, Robin Lemmens, Ioannis Michopoulos, Marios K. Georgakis, Christian Weimar, Peter Kelly, and Georgios Tsivgoulis. 2021. "An Updated Meta-Analysis of RCTs of Colchicine for Stroke Prevention in Patients with Coronary Artery Disease" Journal of Clinical Medicine 10, no. 14: 3110. https://doi.org/10.3390/jcm10143110