
The Long-Term Effect of Treatment Using the Transcranial Magnetic Stimulation rTMS in Patients after Incomplete Cervical or Thoracic Spinal Cord Injury

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures and Intervention
2.2.1. Kinesiotherapy
2.2.2. Repetitive Transcranial Magnetic Stimulation (rTMS)
2.3. Neurophysiological Studies
2.3.1. Surface Electromyography Recordings (sEMG)
2.3.2. Motor Evoked Potentials (MEPs) Recordings
2.4. Data Analysis and Statistics
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oudega, M.; Perez, M. Corticospinal reorganization after spinal cord injury. J. Physiol. 2012, 590, 3647–3663. [Google Scholar] [CrossRef] [PubMed]
- Belci, M.; Catley, M.; Husain, M. Magnetic brain stimulation can improve clinical outcome in incomplete spinal cord injured patients. Spinal Cord 2004, 42, 417–419. [Google Scholar] [CrossRef]
- Kumru, H.; Murillo, N.; Samso, J.V.; Valls-Sole, J.; Edwards, D.; Pelayo, R.; Valero-Cabre, A.; Tormos, J.M.; Pascual-Leone, A. Reduction of spasticity with repetitive transcranial magnetic stimulation in patients with spinal cord injury. Neurorehabil. Neural Repair 2010, 24, 435–441. [Google Scholar] [CrossRef]
- Kuppuswamy, A.; Balasubramaniam, A.V.; Maksimovic, R.; Mathias, C.J.; Gall, A.; Craggs, M.D. Ellaway PHAction of 5Hz repetitive transcranial magnetic stimulation on sensory, motor and autonomic function in human spinal cord injury. Clin. Neurophysiol. 2011, 122, 2452–2461. [Google Scholar] [CrossRef] [PubMed]
- Benito, J.; Kumru, H.; Murillo, N.; Costa, U.; Medina, J.; Tormos, J.M.; Pascual-Leone, A.; Vidal, J. Motor and gait improvement in patients with incomplete spinal cord injury induced by high-frequency repetitive transcranial magnetic stimulation. Top. Spinal Cord Inj. Rehabil. 2012, 18, 106–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nardone, R.; Höller, Y.; Thomschewski, A.; Brigo, F.; Orioli, A.; Höller, P.; Golaszewski, S.; Trinka, E. rTMS modulates reciprocal inhibition in patients with traumatic spinal cord injury. Spinal Cord 2014, 52, 831–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Araújo, A.V.L.; Barbosa, V.R.N.; Galdino, G.S.; Fregni, F.; Massetti, T.; Fontes, S.L.; de Oliveira Silva, D.; da Silva, T.D.; Monteiro, C.B.M.; Tonks, J.; et al. Effects of high-frequency transcranial magnetic stimulation on functional performance in individuals with incomplete spinal cord injury: Study protocol for a randomized controlled trial. Trials 2017, 18, 522. [Google Scholar] [CrossRef] [Green Version]
- Tazoe, T.; Perez, M.A. Effects of repetitive transcranial magnetic stimulation on recovery of function after spinal cord injury. Arch. Phys. Med. Rehabil. 2015, 96, 145–155. [Google Scholar] [CrossRef]
- Jo, H.J.; Richardson, M.S.; Oudega, M.; Perez, M. The Potential of Corticospinal-Motoneuronal Plasticity for Recovery after Spinal Cord Injury. Curr. Phys. Med. Rehabil. Rep. 2020, 8, 293–298. [Google Scholar] [CrossRef]
- Leszczyńska, K.; Wincek, A.; Fortuna, W.; Huber, J.; Łukaszek, J.; Okurowski, S.; Chmielak, K.; Tabakow, P. Treatment of patients with cervical and upper thoracic incomplete spinal cord injury using repetitive transcranial magnetic stimulation. Int. J. Artif. Organs 2019, 43, 323–331. [Google Scholar] [CrossRef]
- Tabakow, P.; Raisman, G.; Fortuna, W.; Czyż, M.; Huber, J.; Li, D.; Szewczyk, P.; Okurowski, S.; Międzybrodzki, R.; Czapiga, B.; et al. Functional regeneration of supraspinal connections in a patient with transected spinal cord following transplantation of bulbar olfactory ensheathing cells with peripheral nerve bridging. Cell Transplant. 2014, 23, 1631–1655. [Google Scholar] [CrossRef] [Green Version]
- Flynn, J.R.; Graham, B.A.; Galea, M.P.; Callister, R.J. The role of propriospinal interneurons in recovery from spinal cord injury. Neuropharmacology 2011, 60, 809–822. [Google Scholar] [CrossRef]
- Jankowska, E. Interneuronal relay in spinal pathways from proprioceptors. Prog. Neurobiol. 1992, 38, 335–378. [Google Scholar] [CrossRef]
- Ditunno, J.F.; Ditunno, P.L.; Scivoletto, G.; Patrick, M.; Dijkers, M.; Barbeau, H.; Burns, A.S.; Marino, R.J.; Schmidt-Read, M. The Walking Index for Spinal Cord Injury (WISCI/WISCI II): Nature, metric properties, use and misuse. Spinal Cord 2013, 51, 346–355. [Google Scholar] [CrossRef] [Green Version]
- Lisiński, P.; Huber, J. Evolution of Muscles Dysfunction from Myofascial Pain Syndrome Through Cervical Disc-Root Conflict to Degenerative Spine Disease. Spine 2017, 42, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Huber, J.; Lisiński, P. Early results of supervised versus unsupervised rehabilitation of patients with cervical pain. Int. J. Artif. Organs 2019, 42, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, G.; Marchand-Pauvert, V.; Burke, D.; Pierrot-Deseilligny, E. Corticospinal excitation of presumed cervical propriospinal neurones and its reversal to inhibition in humans. J. Physiol. 2001, 533, 903–919. [Google Scholar] [CrossRef] [PubMed]
- Pierrot-Deseilligny, E. Propriospinal transmission of part of the corticospinal excitation in humans. Muscle Nerve 2002, 26, 155–172. [Google Scholar] [CrossRef] [PubMed]
- Bunday, K.L.; Perez, M.A. Motor Recovery After Spinal Cord Injury Enhanced by Strengthening Corticospinal Synaptic Transmission. Curr. Biol. 2012, 22, 2355–2361. [Google Scholar] [CrossRef] [Green Version]
- Bareyre, F.M.; Kerschensteiner, M.; Raineteau, O.; Mettenleiter, T.C.; Weinmann, O.; Schwab, M.E. The injured spinal cord spontaneously forms a new intraspinal circuit in adult rats. Nat. Neurosci. 2004, 7, 269–277. [Google Scholar] [CrossRef]
- Calancie, B.; Alexeeva, N.; Broton, J.G.; Molano, M.R. Interlimb reflex activity after spinal cord injury in man: Strengthening response patterns are consistent with ongoing synaptic plasticity. Clin. Neurophysiol. 2005, 116, 75–86. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| K Group | K + rTMS Group | |||
|---|---|---|---|---|
| Mean ± SD | Min–Max | Mean ± SD | Min–Max | |
| Age | 36.7 ± 5.3 | 23–46 | 37.3 ± 4.7 | 25–45 |
| Height (cm) | 175.3 ± 4.3 | 165–181 | 165.0 ± 4.3 | 158–172 |
| Weight (kg) | 62.0 ± 6.1 | 51–79 | 59.0 ± 5.5 | 51–83 |
| n | n | |||
| AIS scale | C = 19 D = 6 | C = 20 D = 6 | ||
| Spinal injury level | C2–C7 = 14 Th1–Th12 = 11 | C2–C7 = 15 Th2–Th12 = 11 | ||
| Recording | Measured Parameter | Healthy Volunteers |
|---|---|---|
| sEMG APB | Amplitude at rest (µV) | 15–30 25.3 ± 2.6 |
| Amplitude during maximal contraction (µV) | 900–1800 1025 ± 105 | |
| Frequency index | 3-3 3.0 | |
| sEMG TA | Amplitude at rest (µV) | 15–30 25.6 ± 2.2 |
| Amplitude during maximal contraction (µV) | 600–1450 725 ± 110 | |
| Frequency index | 3-3 3.0 | |
| MEP APB | Amplitude (µV) | 1125–3650 1662.5 ± 472.8 |
| Latency (ms) | 18.6–22.7 20.65 ± 2.05 | |
| MEP TA | Amplitude (µV) | 1200–2975 1656 ± 370.7 |
| Latency (ms) | 25.9–31.75 28.8 ± 1.7 |
| Recording | Measured Parameter | 1st Observation (Before Treatment) | 2nd Observation (After 2–3 Months of Treatment) | 3rd Observation (After 5 Months of Treatment) | Difference 1st vs. 3rd | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Before rTMS Sessions | After rTMS Sessions | p | Before rTMS Sessions | After rTMS Sessions | p | Before rTMS Sessions | After rTMS Sessions | p | p | ||
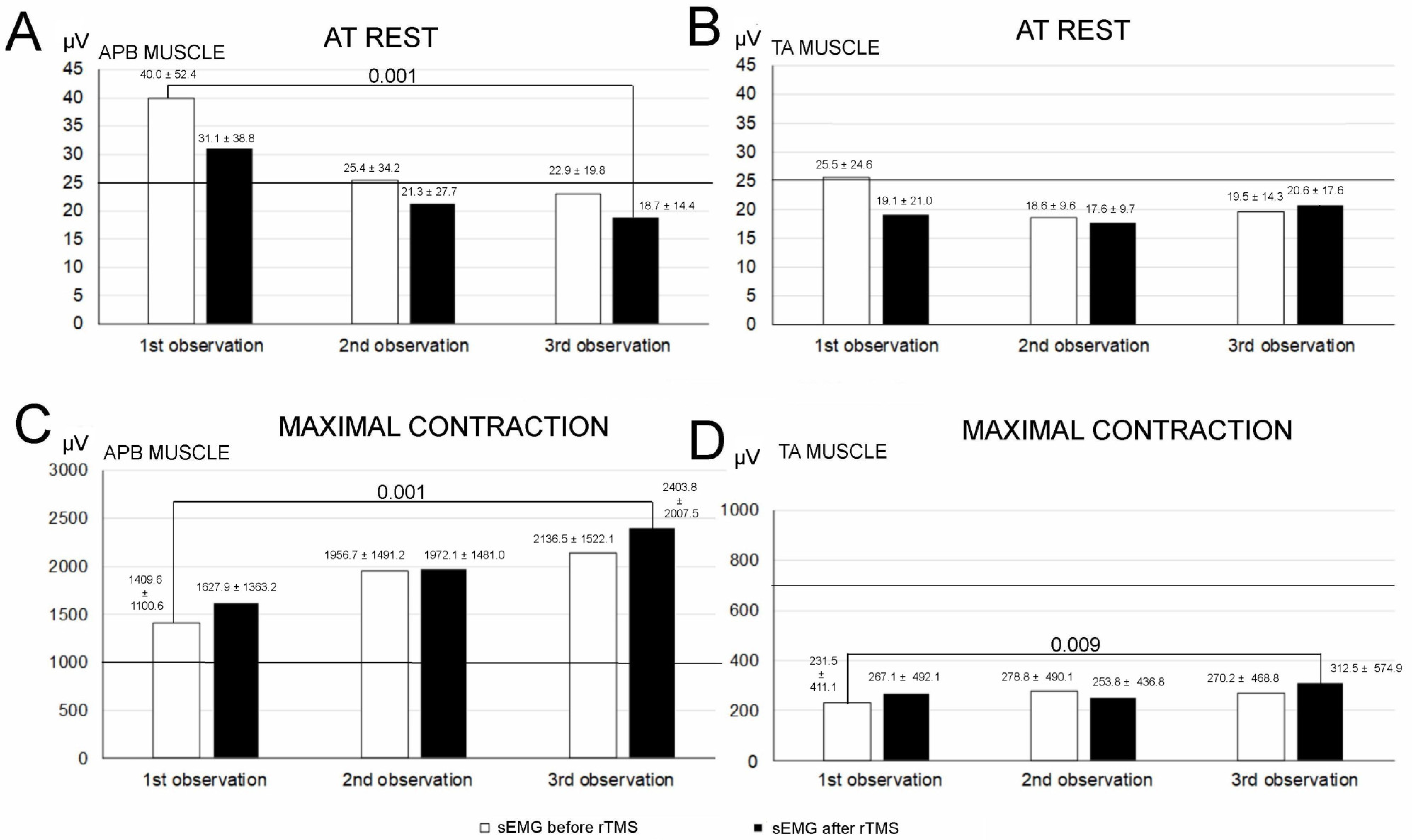
| sEMG APB | Amplitude at rest (µV) | 5–200 40.0 ± 52.4 | 5–200 31.1 ± 38.8 | 0.011 * | 5–200 25.4 ± 34.2 | 5–200 21.3 ± 27.7 | 0.007 * | 10–100 22.9 ± 19.8 | 10–100 18.7 ± 14.4 | 0.004 * | <0.001 * |
| Amplitude during maximal contraction (µV) | 100–4000 1409.6 ± 1100.6 | 100–7000 1627.9 ± 1363.2 | 0.002 * | 100–6000 1956.7 ± 1491.2 | 100–7000 1972.1 ± 1481.0 | 0.334 | 100–6000 2136.5 ± 1522.1 | 100–10500 2403.8 ± 2007.5 | 0.030 * | <0.001 * | |
| Frequency index | 1-3 2.2 ± 0.7 | 1-3 2.2 ± 0.7 | 0.779 | 1-3 2.1 ± 0.7 | 1-3 2.2 ± 0.7 | 0.128 | 1-3 2.5 ± 0.7 | 0-3 2.5 ± 0.7 | 0.767 | 0.003 * | |
| sEMG TA | Amplitude at rest (µV) | 5–200 25.5 ± 34.6 | 5–150 19.1 ± 21.0 | 0.021 * | 10–50 18.6 ± 9.6 | 10–50 17.6 ± 9.7 | 0.046 * | 10–100 19.5 ± 14.3 | 10–100 20.6 ± 17.6 | 0.917 | 0.331 |
| Amplitude during maximal contraction (µV) | 0–2000 231.5 ± 411.1 | 0–2200 267.1 ± 492.1 | 0.064 | 0–2000 278.8 ± 490.1 | 0–1700 253.8 ± 436.8 | 0.069 | 0–2100 270.2 ± 468.8 | 0–3000 312.5 ± 574.9 | 0.05 * | 0.009 * | |
| Frequency index | 0-3 0.9 ± 1.0 | 0-3 0.9 ± 0.9 | 1.0 | 0-3 1 ± 1.0 | 0-3 1 ± 1.0 | 1.0 | 0-3 0.9 ± 1.0 | 0-3 1.0 ± 1.1 | 0.109 | 0.320 | |
| MEP APB | Amplitude (µV) | 50–12500 2052.9 ± 2511.0 | 0–10000 1960.6 ± 2294.8 | 1.0 | 0–10000 2351.9 ± 2599.3 | 0–12000 2353.8 ± 2911.2 | 0.602 | 100–15000 1942.3 ± 2668.9 | 100–11000 2725.1 ± 2524.1 | 0.05 * | 0.008 * |
| Latency (ms) | 16.8–43.5 23.4 ± 5.2 | 0–37.7 22.7 ± 5.4 | 0.373 | 0–38.7 22.3 ± 5.4 | 0–38.7 22.7 ± 5.3 | 0.172 | 15.5–33.4 22.3 ± 3.9 | 14.6–33.0 23.3 ± 4.5 | 0.655 | 0.081 | |
| MEP TA | Amplitude (µV) | 0–1000 76.9 ± 162.8 | 0–1000 80.5 ± 169.4 | 0.530 | 0–2200 128.8 ± 354.7 | 0–1100 107.9 ± 250.7 | 0.683 | 0–800 78.8 ± 157.6 | 0–1100 162.1 ± 123.6 | 0.05 * | 0.05 * |
| Latency (ms) | 0–49.3 29.1 ± 18.5 | 0–48.0 28.7 ± 18.5 | 0.691 | 0–45.1 28.5 ± 16.4 | 0–45.1 28.3 ± 16.6 | 0.687 | 0–45.0 28.5 ± 17.6 | 0–45.0 28.1 ± 15.6 | 0.052 | 0.332 | |
| Recording | Measured Parameter | K Group | K + rTMS Group | K vs. K + rTMS Difference before | K vs. K + rTMS Difference after | ||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | Change (%) | Before | After | Change (%) | p | p | ||
| sEMG APB | Amplitude at rest (µV) | 5–150 45.3 ± 22.1 | 5–200 35.7 ± 24.3 | 21.1 | 5–200 40.0 ± 52.4 | 10–100 18.7 ± 14.4 | 53.2 | 0.06 | 0.03 * |
| Amplitude during maximal contraction (µV) | 100–4500 1443.7 ± 1241.7 | 100–6500 1445.1 ± 1126.8 | 0.09 | 100–4000 1409.6 ± 1100.6 | 100–10500 2403.8 ± 2007.5 | 41.3 | 0.13 | 0.03 * | |
| Frequency index | 1–3 2.0 ± 0.5 | 1–3 2.0 ± 0.6 | 0 | 1–3 2.2 ± 0.7 | 0–3 2.5 ± 0.7 | 12.0 | 0.06 | 0.04 * | |
| sEMG TA | Amplitude at rest (µV) | 10–100 22.1.6 ± 6.4 | 10–50 22.3 ± 7.1 | 0.89 | 5–200 25.5 ± 34.6 | 10–100 20.6 ± 17.6 | 19.2 | 0.07 | 0.06 |
| Amplitude during maximal contraction (µV) | 0–1900 245.8 ± 381.2 | 0–2700 246.5 ± 321.3 | 0.28 | 0–2000 231.5 ± 411.1 | 0–3000 312.5 ± 574.9 | 25.9 | 0.08 | 0.05 * | |
| Frequency index | 0–3 1 ± 1.0 | 0–3 1 ± 1.0 | 0 | 0–3 0.9 ± 1.0 | 0–3 1.0 ± 1.1 | 10.0 | 0.06 | 0.06 | |
| MEP APB | Amplitude (µV) | 50–11200 1925.3 ± 1724.3 | 50–1050 2105.6 ± 1855.3 | 9.5 | 50–12500 2052.9 ± 2511.0 | 100–11000 2725.1 ± 2524.1 | 24.6 | 0.07 | 0.05 * |
| Latency (ms) | 16.2–33.4 23.1 ± 4.6 | 17.1–34.6 23.6 ± 3.9 | 2.1 | 16.8–43.5 23.4 ± 5.2 | 14.6–33.0 23.3 ± 4.5 | 0.42 | 0.14 | 0.13 | |
| MEP TA | Amplitude (µV) | 0–1200 77.1 ± 133.5 | 0–1000 100.9 ± 131.6 | 23.5 | 0–1000 76.9 ± 162.8 | 0–1100 162.1 ± 123.6 | 52.5 | 0.11 | 0.05 * |
| Latency (ms) | 0–50.1 30.4 ± 17.1 | 0–49.2 29.4 ± 13.6 | 3.2 | 0–49.3 29.1 ± 18.5 | 0–45.0 28.1 ± 15.6 | 3.4 | 0.13 | 0.12 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wincek, A.; Huber, J.; Leszczyńska, K.; Fortuna, W.; Okurowski, S.; Chmielak, K.; Tabakow, P. The Long-Term Effect of Treatment Using the Transcranial Magnetic Stimulation rTMS in Patients after Incomplete Cervical or Thoracic Spinal Cord Injury. J. Clin. Med. 2021, 10, 2975. https://doi.org/10.3390/jcm10132975
Wincek A, Huber J, Leszczyńska K, Fortuna W, Okurowski S, Chmielak K, Tabakow P. The Long-Term Effect of Treatment Using the Transcranial Magnetic Stimulation rTMS in Patients after Incomplete Cervical or Thoracic Spinal Cord Injury. Journal of Clinical Medicine. 2021; 10(13):2975. https://doi.org/10.3390/jcm10132975
Chicago/Turabian StyleWincek, Agnieszka, Juliusz Huber, Katarzyna Leszczyńska, Wojciech Fortuna, Stefan Okurowski, Krzysztof Chmielak, and Paweł Tabakow. 2021. "The Long-Term Effect of Treatment Using the Transcranial Magnetic Stimulation rTMS in Patients after Incomplete Cervical or Thoracic Spinal Cord Injury" Journal of Clinical Medicine 10, no. 13: 2975. https://doi.org/10.3390/jcm10132975