
The Role of Conventional and Stereotactic Microwave Ablation for Intrahepatic Cholangiocarcinoma


Abstract
:1. Introduction
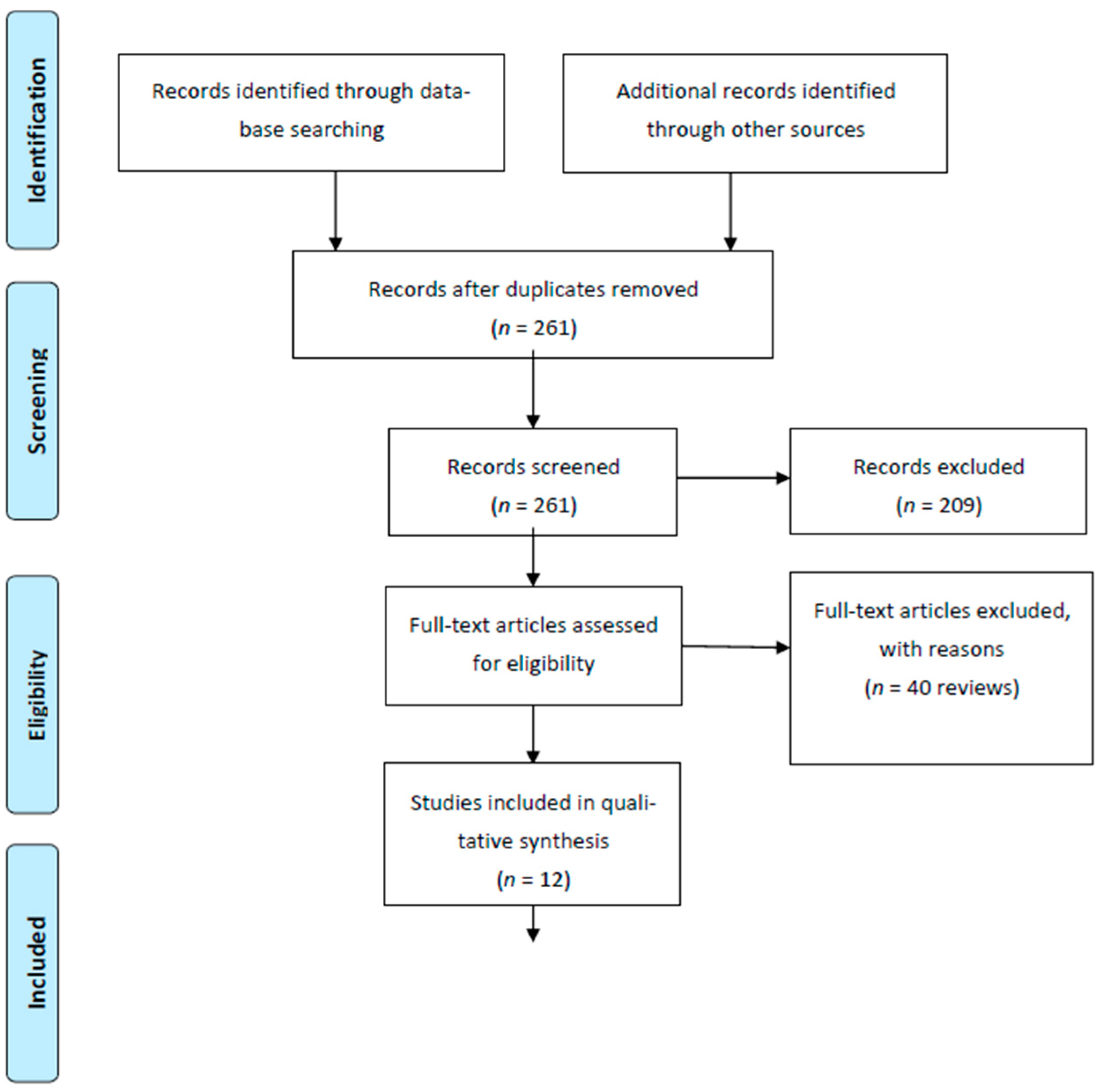
2. Materials and Methods
3. Results
3.1. Current Guideline Recommendation for ICCA Ablation
3.2. MWA for ICCA
3.3. Ablation vs. Surgery
3.4. RFA vs. MWA
3.5. MWA and TACE
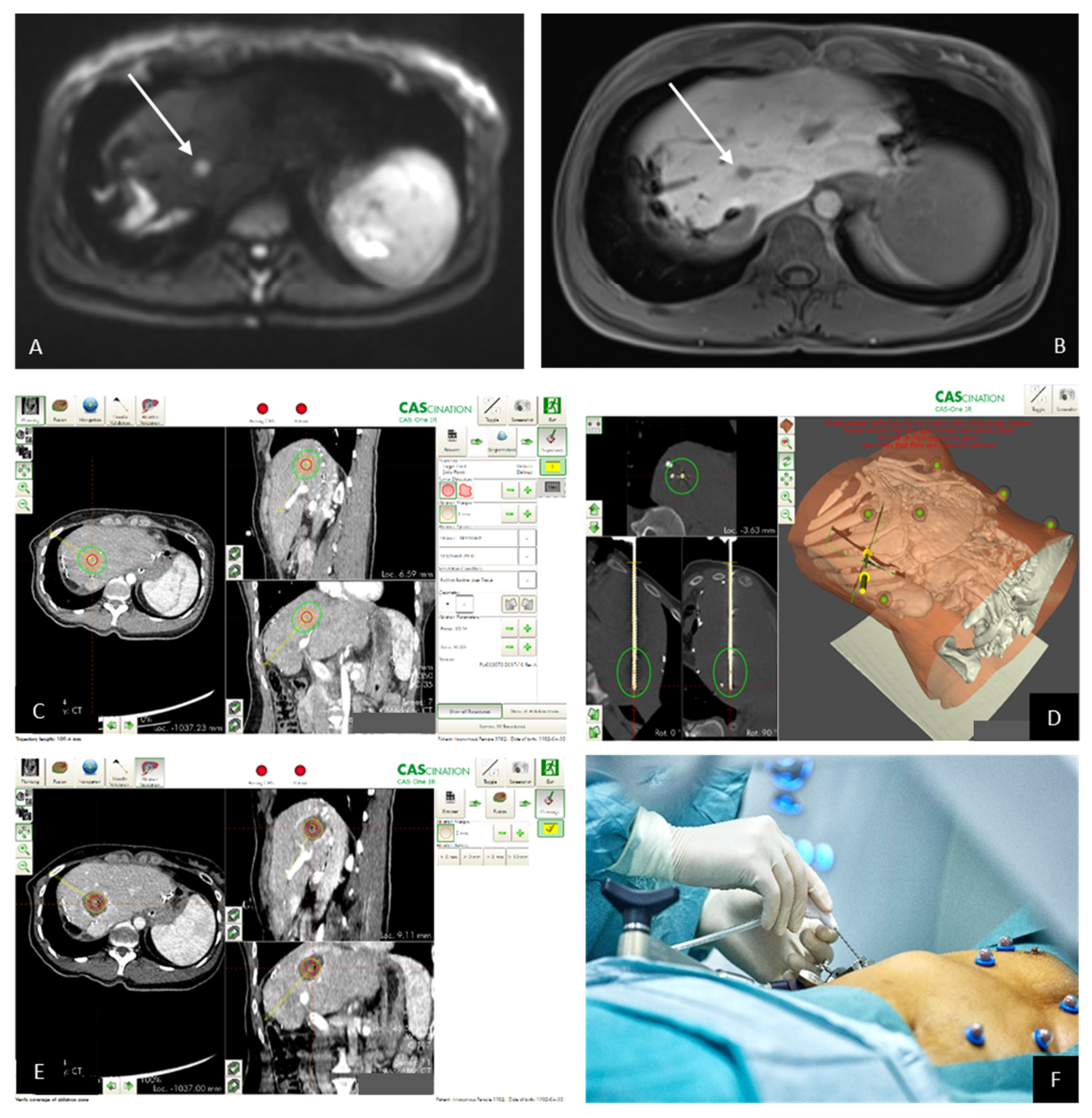
3.6. Stereotactic Microwave Ablation (SMWA)
3.7. ICCA and Stereotactic MWA: Clinical Trials
3.8. Own Patients with ICCA Treated by SMWA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, H.; Yang, T.; Wu, M.; Shen, F. Intrahepatic cholangiocarcinoma: Epidemiology, risk factors, diagnosis and surgical management. Cancer Lett. 2016, 379, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Banales, J.M.; Cardinale, V.; Carpino, G.; Marzioni, M.; Andersen, J.B.; Invernizzi, P.; Lind, G.E.; Folseraas, T.; Forbes, S.J.; Fouassier, L.; et al. Expert consensus document: Cholangiocarcinoma: Current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA). Nature reviews. Gastroenterol. Hepatol. 2016, 13, 261–280. [Google Scholar]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 577–588. [Google Scholar] [CrossRef]
- Zhang, A.; Liu, B.; Xu, D.; Sun, Y. Advanced intrahepatic cholangiocarcinoma treated using anlotinib and microwave ablation: A case report. Medicine 2019, 98, e18435. [Google Scholar] [CrossRef] [PubMed]
- Neeff, H.P.; Holzner, P.A.; Menzel, M.; Bronsert, P.; Klock, A.; Lang, S.A.; Fichtner-Feigl, S.; Hopt, U.T.; Makowiec, F. Intrahepatic cholangiocarcinoma: Results after 84 resections. Chirurg. Z. Geb. Oper. Medizen. 2018, 89, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Vidili, G.; Rengo, M.; Bujanda, L.; Ponz-Sarvisé, M.; Lamarca, A. Clinical presentation, diagnosis and staging of cholangiocarcinoma. Liver Int. 2019, 39, 98–107. [Google Scholar] [CrossRef] [Green Version]
- Van Vugt, J.L.A.; Gaspersz, M.P.; Coelen, R.J.S.; Vugts, J.; Labeur, T.A.; de Jonge, J.; Polak, W.G.; Busch, O.R.C.; Besselink, M.G.; IJzermans, J.N.M.; et al. The prognostic value of portal vein and hepatic artery involvement in patients with perihilar cholangiocarcinoma. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2018, 20, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, Y.-I.; Shirabe, K.; Beppu, T.; Eguchi, S.; Nanashima, A.; Ohta, M.; Ueno, S.; Kondo, K.; Kitahara, K.; Shiraishi, M.; et al. Surgical management of recurrent intrahepatic cholangiocarcinoma: Predictors, adjuvant chemotherapy, and surgical therapy for recurrence: A multi-institutional study by the Kyushu Study Group of Liver Surgery. Ann. Gastroenterol. Surg. 2017, 1, 136–142. [Google Scholar] [CrossRef]
- Wright, G.P.; Perkins, S.; Jones, H.; Zureikat, A.H.; Marsh, J.W.; Holtzman, M.P.; Zeh, H.J.; Bartlett, D.L.; Pingpank, J.F. Surgical Resection Does Not Improve Survival in Multifocal Intrahepatic Cholangiocarcinoma: A Comparison of Surgical Resection with Intra-Arterial Therapies. Ann. Surg. Oncol. 2017, 25, 83–90. [Google Scholar] [CrossRef]
- Zhang, X.; Beal, E.W.; Bagante, F.; Chakedis, J.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; et al. Early versus late recurrence of intrahepatic cholangiocarcinoma after resection with curative intent. Br. J. Surg. 2018, 105, 848–856. [Google Scholar] [CrossRef]
- Lang, H.; Sotiropoulos, G.C.; Sgourakis, G.; Schmitz, K.J.; Paul, A.; Hilgard, P.; Zöpf, T.; Trarbach, T.; Malagó, M.; Baba, H.A.; et al. Operations for Intrahepatic Cholangiocarcinoma: Single-Institution Experience of 158 Patients. J. Am. Coll. Surg. 2009, 208, 218–228. [Google Scholar] [CrossRef] [PubMed]
- Guglielmi, A.; Ruzzenente, A.; Campagnaro, T.; Pachera, S.; Valdegamberi, A.; Nicoli, P.; Cappellani, A.; Malfermoni, G.; Iacono, C. Intrahepatic Cholangiocarcinoma: Prognostic Factors After Surgical Resection. World J. Surg. 2009, 33, 1247–1254. [Google Scholar] [CrossRef] [PubMed]
- Tamandl, D.; Herberger, B.; Gruenberger, B.; Puhalla, H.; Klinger, M.; Gruenberger, T. Influence of Hepatic Resection Margin on Recurrence and Survival in Intrahepatic Cholangiocarcinoma. Ann. Surg. Oncol. 2008, 15, 2787–2794. [Google Scholar] [CrossRef]
- Shaib, Y.; El-Serag, H.B. The Epidemiology of Cholangiocarcinoma. Semin. Liver Dis. 2004, 24, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Massironi, S.; Pilla, L.; Elvevi, A.; Longarini, R.; Rossi, R.E.; Bidoli, P.; Invernizzi, P. New and Emerging Systemic Therapeutic Options for Advanced Cholangiocarcinoma. Cells 2020, 9, 688. [Google Scholar] [CrossRef] [Green Version]
- Mahipal, A.; Kommalapati, A.; Tella, S.H.; Lim, A.; Kim, R. Novel targeted treatment options for advanced cholangiocarcinoma. Expert Opin. Investig. Drugs 2018, 27, 709–720. [Google Scholar] [CrossRef]
- Mizrahi, J.D.; Shroff, R.T. New Treatment Options for Advanced Biliary Tract Cancer. Curr. Treat. Options Oncol. 2020, 21, 63. [Google Scholar] [CrossRef]
- Razumilava, N.; Gores, G.J. Cholangiocarcinoma. Lancet 2014, 383, 2168–2179. [Google Scholar] [CrossRef] [Green Version]
- Lachenmayer, A.; Tinguely, P.; Maurer, M.H.; Frehner, L.; Knöpfli, M.; Peterhans, M.; Weber, S.; Dufour, J.; Candinas, D.; Banz, V. Stereotactic image-guided microwave ablation of hepatocellular carcinoma using a computer-assisted navigation system. Liver Int. 2019, 39, 1975–1985. [Google Scholar] [CrossRef]
- Ferguson, C.D.; Luis, C.R.; Steinke, K. Safety and efficacy of microwave ablation for medically inoperable colorectal pulmonary metastases: Single-centre experience. J. Med. Imaging Radiat. Oncol. 2017, 61, 243–249. [Google Scholar] [CrossRef]
- Shiina, S.; Sato, K.; Tateishi, R.; Shimizu, M.; Ohama, H.; Hatanaka, T.; Takawa, M.; Nagamatsu, H.; Imai, Y. Percutaneous Ablation for Hepatocellular Carcinoma: Comparison of Various Ablation Techniques and Surgery. Can. J. Gastroenterol. Hepatol. 2018, 2018, 4756147. [Google Scholar] [CrossRef] [Green Version]
- Valle, J.W.; Borbath, I.; Khan, S.A.; Huguet, F.; Gruenberger, T.; Arnold, D. Biliary cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v28–v37. [Google Scholar] [CrossRef]
- Xu, H.-X.; Wang, Y.; Lu, M.-D.; Liu, L.-N. Percutaneous ultrasound-guided thermal ablation for intrahepatic cholangiocarcinoma. Br. J. Radiol. 2012, 85, 1078–1084. [Google Scholar] [CrossRef] [Green Version]
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.-W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hepatobiliary Cancers NCCN Guidelines. Version 12021. Available online: https://www.nccn.org/patients/guidelines/content/PDF/nccnquickguide-hepatobiliary-patient.pdf (accessed on 5 March 2021).
- Yu, M.-A.; Liang, P.; Yu, X.-L.; Cheng, Z.-G.; Han, Z.-Y.; Liu, F.-Y.; Yu, J. Sonography-guided percutaneous microwave ablation of intrahepatic primary cholangiocarcinoma. Eur. J. Radiol. 2011, 80, 548–552. [Google Scholar] [CrossRef] [PubMed]
- Yousaf, A.; Kim, J.U.; Eliahoo, J.; Taylor-Robinson, S.D.; Khan, S.A. Ablative Therapy for Unresectable Intrahepatic Cholangiocarcinoma: A Systematic Review and Meta-Analysis. J. Clin. Exp. Hepatol. 2019, 9, 740–748. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.; Yu, J.; Yu, X.; Han, Z.; Cheng, Z.; Liu, F.; Liang, P. Clinical and survival outcomes of percutaneous microwave ablation for intrahepatic cholangiocarcinoma. Int. J. Hyperth. 2018, 34, 292–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giorgio, A.; Gatti, P.; Montesarchio, L.; Santoro, B.; Dell’Olio, A.; Crucinio, N.; Coppola, C.; Scarano, F.; De Biase, F.; Ciracì, E.; et al. Intrahepatic Cholangiocarcinoma and Thermal Ablation: Long-term Results of An Italian Retrospective Multicenter Study. J. Clin. Transl. Hepatol. 2019, 7, 1–6. [Google Scholar] [CrossRef]
- Díaz-González, Á.; Vilana, R.; Bianchi, L.; García-Criado, Á.; Rimola, J.; de Lope, C.R.; Ferrer, J.; Ayuso, C.; Da Fonseca, L.G.; Reig, M.; et al. Thermal Ablation for Intrahepatic Cholangiocarcinoma in Cirrhosis: Safety and Efficacy in Non-Surgical Patients. J. Vasc. Interv. Radiol. 2020, 31, 710–719. [Google Scholar] [CrossRef]
- Yang, H.; Cheng, Z.; Han, Z.; Liu, F.; Yu, X.; Yu, J.; Liang, P. Assessment of the Outcomes of Intrahepatic Cholangiocarcinoma After Ultrasound-Guided Percutaneous Microwave Ablation Based on Albumin–Bilirubin Grade. Cardiovasc. Interv. Radiol. 2021, 44, 261–270. [Google Scholar] [CrossRef]
- Takahashi, E.A.; Kinsman, K.A.; Schmit, G.D.; Atwell, T.D.; Schmitz, J.J.; Welch, B.T.; Callstrom, M.R.; Geske, J.R.; Kurup, A.N. Thermal ablation of intrahepatic cholangiocarcinoma: Safety, efficacy, and factors affecting local tumor progression. Abdom. Radiol. 2018, 43, 3487–3492. [Google Scholar] [CrossRef]
- Sweeney, J.; Parikh, N.; El-Haddad, G.; Kis, B. Ablation of Intrahepatic Cholangiocarcinoma. Semin. Interv. Radiol. 2019, 36, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Sparchez, Z.; Mocan, T.; Radu, P.; Nenu, I.; Comsa, M.; Al Hajjar, N.; Mois, E.; Bartos, A.; Kacso, G.; Sparchez, M. Microwave ablation in the treatment of liver tumors. A better tool or simply more power? Med. Ultrason. 2020, 22, 451. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Li, L.; Xu, W.; Du, C.; Yang, L.; Tong, J.; Yi, Y. Ultrasound-guided percutaneous microwave ablation versus surgical resection for recurrent intrahepatic cholangiocarcinoma: Intermediate-term results. Int. J. Hyperth. 2019, 36, 350–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni, J.-Y.; An, C.; Zhang, T.-Q.; Huang, Z.-M.; Jiang, X.-Y.; Huang, J.-H. Predictive value of the albumin-bilirubin grade on long-term outcomes of CT-guided percutaneous microwave ablation in intrahepatic cholangiocarcinoma. Int. J. Hyperth. 2019, 36, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Shen, L.; Zhao, L.; Guan, Z.; Chen, Q.; Li, W. Combined transarterial chemoembolization and microwave ablation versus transarterial chemoembolization in BCLC stage B hepatocellular carcinoma. Diagn. Interv. Radiol. 2018, 24, 219–224. [Google Scholar] [CrossRef] [Green Version]
- Smolock, A.R.; Cristescu, M.M.; Hinshaw, A.; Woo, K.M.; Wells, S.A.; Ziemlewicz, T.; Lubner, M.G.; Dalvie, P.S.; Hinshaw, J.L.; Brace, C.; et al. Combination transarterial chemoembolization and microwave ablation improves local tumor control for 3- to 5-cm hepatocellular carcinoma when compared with transarterial chemoembolization alone. Abdom. Radiol. 2018, 43, 2497–2504. [Google Scholar] [CrossRef]
- Yang, G.-W.; Zhao, Q.; Qian, S.; Zhu, L.; Qu, X.-D.; Zhang, W.; Yan, Z.-P.; Cheng, J.-M.; Liu, Q.-X.; Liu, R.; et al. Percutaneous microwave ablation combined with simultaneous transarterial chemoembolization for the treatment of advanced intrahepatic cholangiocarcinoma. OncoTargets Ther. 2015, 8, 1245–1250. [Google Scholar] [CrossRef] [Green Version]
- Schaible, J.; Lürken, L.; Wiggermann, P.; Verloh, N.; Einspieler, I.; Zeman, F.; Schreyer, A.G.; Bale, R.; Stroszczynski, C.; Beyer, L. Primary efficacy of percutaneous microwave ablation of malignant liver tumors: Comparison of stereotactic and conventional manual guidance. Sci. Rep. 2020, 10, 18835. [Google Scholar] [CrossRef]
- Xu, G.; Wang, N.; Ling, X.; Lu, H.; Lin, R.; Shi, Y.; Zhang, B. Diagnostic Value of Assessment of Cervical Involvement in Early-Stage Endometrial Adenocarcinoma: Comparison of Magnetic Resonance Imaging (MRI) Versus Hysteroscopy. Med. Sci. Monit. 2018, 24, 7952–7957. [Google Scholar] [CrossRef]
- Valle, J.W.; Kelley, R.K.; Nervi, B.; Oh, D.-Y.; Zhu, A.X. Biliary tract cancer. Lancet 2021, 397, 428–444. [Google Scholar] [CrossRef]
- Hartley-Blossom, Z.; Alam, M.; Stone, J.; Iannuccilli, J. Microwave Ablation in the Liver: An Update. Surg. Technol. Int. 2020, 37, 72–78. [Google Scholar]
- Bekaii-Saab, T.; Bridgewater, J.; Normanno, N. Practical considerations in screening for genetic alterations in cholangiocarcinoma. Ann. Oncol. 2021. [Google Scholar] [CrossRef]
- Kelley, R.K.; Bridgewater, J.; Gores, G.J.; Zhu, A.X. Systemic therapies for intrahepatic cholangiocarcinoma. J. Hepatol. 2020, 72, 353–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Reference of Original Publication | Year of Publication | Technique(s) Analyzed | Number of Patients Included | Number of Treated Lesions | Size (Range; cm) | OS 1, 3, 5 Years (%) | RFS 1, 3, 5 Years (%) |
|---|---|---|---|---|---|---|---|
| [26] | 2011 | MWA | 15 | 24 | 3.2 (1.3–9.9) | 60, -, - | - |
| [23] | 2012 | MWA | 18 (6) | 25 | 2.5 (0.7–4.3) | 36.3, 30.3, 30.3 | - |
| [27] | 2015 | MWA/TACE | 26 | 39 | 3.6 (2.5–6.5) | 69.2, 61.5, - | - |
| [28] | 2018 | MWA | 107 | 171 | 93.5, 39.6, 7.9 | 41.5, -, - | |
| [29] | 2018 | RFA vs. MWA | 20 | 50 | 1.8 (0.5–4.7) | - | - |
| [30] | 2019 | RFA vs. MWA | 71 (35) | 98 (50) | 3.6 ** (2.2–7.2) | 95, 75, 68 ** | 79, 59, 55 ** |
| [31] | 2019 | MWA | 78 | 106 | 3.1 (0.8–5) | 78.9, 52.2, 35 | 78.9, 19.9, - |
| [32] | 2019 | MWA vs. surgery | 121 (56) | 136 (62) | 2.7 (0.8–5) | 81.2, 42.5, 23.7 ** | 70.3, 33.1, - ** |
| [33] | 2020 | MWA/TACE | 275 (92) | - | 5.7 | 50, 21.5, 6.1 | 41.1, 21.5, 6.1 |
| [34] | 2020 | MWA | 221 {32} | 285 | - | - | - |
| [35] | 2020 | MWA/RFA | 27 (3) * | 33 | 2.1 (2.0–2.8) | 88.9, 40.7, 14.8 | - |
| [36] | 2021 | MWA | 52 | 74 | 3.1 (0.8–5) | 87.4, 51.4, 35.2 | 68.9, 56.9, 56.9 |
| Patient | Age at SMWA | Gender | Child Score | Underlying Liver Disease | Segment | Tumor Size (mm) | Previous Treatment | Complications > Dindo IIIa | Local Recurrence | Time to Recurrence (Months) | Treatment of Recurrence | Death | OS (Months) | Time to Transplant (Months) | Overall Disease Progression |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 31 | M | B7 | PSC | V | 20 | no | no | no | no | 31.5 | 10 | no | ||
| 2 | 58 | M | A6 | HCV | VIII | 23 | no | no | yes | 18 | TAE + MWA planned | no | 19 | N/A | no |
| 3 | 64 | M | A6 | ASH/NASH | VIII | 15 | TAE | no | no | no | 12 | N/A | no | ||
| 4 | 58 | M | A5 | NASH | VI | 24 | no | no | no | no | 10 | on waiting list | yes (HCC) | ||
| 5 | 81 | M | A5 | Unknown | V/VIII | 27 | No | no | no | no | 6 | no |
| Patient | Age at SMWA | Gender | Tumor Stage | Previous Treatment | Adjuvant CTX | Location Metastasis Segment | Size of Ablated Metastasis | Complications > Dindo IIIa |
| 1 | 72 | W | T2aN1M0 L0V0Pn1 G1 R0 | ALPPS | Gemcitabine | II | 32 | no |
| 2 | 37 | W | T1N0M1 L0V0Pn0 R0 G3 | Right hepatectomy + metastectomy left liver | Xeloda | II | 15 | no |
| 3 | 58 | M | T1N0M0 Ln1V0Pn0R1 G3 | ALPPS | Gemcitabine/ Capecitabine | IVb | 26 & 25 | no |
| 4 | 66 | W | T2N0M0 Ln0V1Pn0R1 G2 | Extended left hepatectomy | none | VIII | 17 | no |
| 5 | 56 | M | T2aN0M0 Ln0V0Pn1R0 G1 | ALLPS | none | III | 6 | abscess |
| Patient | Local Recurrence | Time to Recurrence (Months) | Treatment of Recurrence | Death | OS after SMWA (Months) | OS after Initial Diagnosis | Overall Disease Progression | |
| 1 | yes | 5 | SBRT | yes | 19 | 45 | yes | |
| 2 | no | no | 20 | 34 | no | |||
| 3 | yes | 3 | CTX | yes | 5.5 | 35 | yes | |
| 4 | no | yes | 6.5 | 15 | no | |||
| 5 | no | no | 1 | 25 | no | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim-Fuchs, C.; Candinas, D.; Lachenmayer, A. The Role of Conventional and Stereotactic Microwave Ablation for Intrahepatic Cholangiocarcinoma. J. Clin. Med. 2021, 10, 2963. https://doi.org/10.3390/jcm10132963
Kim-Fuchs C, Candinas D, Lachenmayer A. The Role of Conventional and Stereotactic Microwave Ablation for Intrahepatic Cholangiocarcinoma. Journal of Clinical Medicine. 2021; 10(13):2963. https://doi.org/10.3390/jcm10132963
Chicago/Turabian StyleKim-Fuchs, Corina, Daniel Candinas, and Anja Lachenmayer. 2021. "The Role of Conventional and Stereotactic Microwave Ablation for Intrahepatic Cholangiocarcinoma" Journal of Clinical Medicine 10, no. 13: 2963. https://doi.org/10.3390/jcm10132963