
Steroid-Sparing Effect of Tocilizumab and Methotrexate in Patients with Polymyalgia Rheumatica: A Retrospective Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
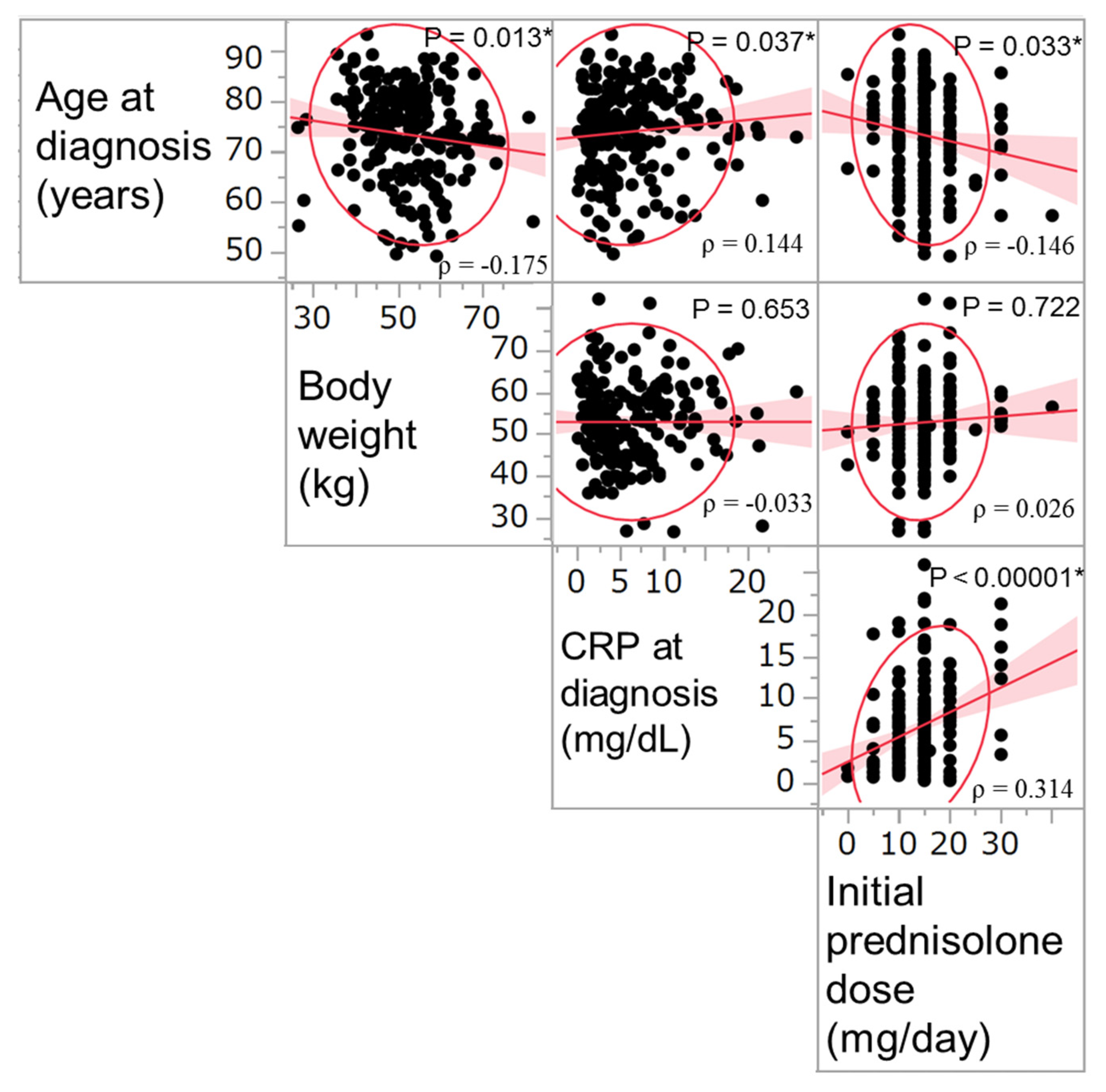
3.1. Patients’ Characteristics
3.2. Prednisolone Dose at the Last Visit
3.3. Factors Associated with Prednisolone Discontinuation
3.4. Adverse Events and Comorbidities
3.5. Relapses
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gonzalez-Gay, M.A.; Matteson, E.L.; Castaneda, S. Polymyalgia rheumatica. Lancet 2017, 390, 1700–1712. [Google Scholar] [CrossRef]
- Muller, S.; Hider, S.L.; Helliwell, T.; Lawton, S.; Barraclough, K.; Dasgupta, B.; Zwierska, I.; Mallen, C.D. Characterising those with incident polymyalgia rheumatica in primary care: Results from the PMR Cohort Study. Arthritis Res. Ther. 2016, 18, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasgupta, B.; Salvarani, C.; Schirmer, M.; Crowson, C.S.; Maradit-Kremers, H.; Hutchings, A.; Matteson, E.L.; Members of the American College of Rheumatology Work Group for Development of Classification Criteria for PMR. Developing classification criteria for polymyalgia rheumatica: Comparison of views from an expert panel and wider survey. J. Rheumatol. 2008, 35, 270–277. [Google Scholar] [PubMed]
- Salvarani, C.; Cantini, F.; Olivieri, I.; Barozzi, L.; Macchioni, L.; Boiardi, L.; Niccoli, L.; Padula, A.; Pulsatelli, L.; Meliconi, R. Corticosteroid injections in polymyalgia rheumatica: A double-blind, prospective, randomized, placebo-controlled study. J. Rheumatol. 2000, 27, 1470–1476. [Google Scholar]
- Stahn, C.; Buttgereit, F. Genomic and nongenomic effects of glucocorticoids. Nat. Clin. Pract. Rheumatol. 2008, 4, 525–533. [Google Scholar] [CrossRef]
- Van der Veen, M.J.; Dinant, H.J.; van Booma-Frankfort, C.; van Albada-Kuipers, G.A.; Bijlsma, J.W. Can methotrexate be used as a steroid sparing agent in the treatment of polymyalgia rheumatica and giant cell arteritis? Ann. Rheum. Dis. 1996, 55, 218–223. [Google Scholar] [CrossRef] [Green Version]
- Ferraccioli, G.; Salaffi, F.; De Vita, S.; Casatta, L.; Bartoli, E. Methotrexate in polymyalgia rheumatica: Preliminary results of an open, randomized study. J. Rheumatol. 1996, 23, 624–628. [Google Scholar]
- Caporali, R.; Cimmino, M.A.; Ferraccioli, G.; Gerli, R.; Klersy, C.; Salvarani, C.; Montecucco, C.; Systemic Vasculitis Study Group of the Italian Society for Rheumatology. Prednisone plus methotrexate for polymyalgia rheumatica: A randomized, double-blind, placebo-controlled trial. Ann. Intern. Med. 2004, 141, 493–500. [Google Scholar] [CrossRef]
- Galbo, H.; Kall, L. Circadian variations in clinical symptoms and concentrations of inflammatory cytokines, melatonin, and cortisol in polymyalgia rheumatica before and during prednisolone treatment: A controlled, observational, clinical experimental study. Arthritis Res. Ther. 2016, 18, 174. [Google Scholar] [CrossRef] [Green Version]
- Izumi, K.; Kuda, H.; Ushikubo, M.; Kuwana, M.; Takeuchi, T.; Oshima, H. Tocilizumab is effective against polymyalgia rheumatica: Experience in 13 intractable cases. RMD Open 2015, 1, e000162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alegria, G.C.; Cornec, D.Y.K.; Renaudineau, Y.; Saraux, A.; Devauchelle-Pensec, Y. Inflammatory Markers are Quickly Improved by Tocilizumab in Early Polymyalgia Rheumatica and Might Predict Early Response to Interleukin-6 Blockade. Rheumatol. Ther. 2021. [Google Scholar] [CrossRef]
- Huwart, A.; Garrigues, F.; Jousse-Joulin, S.; Marhadour, T.; Guellec, D.; Cornec, D.; Gouillou, M.; Saraux, A.; Devauchelle-Pensec, V. Ultrasonography and magnetic resonance imaging changes in patients with polymyalgia rheumatica treated by tocilizumab. Arthritis Res. Ther. 2018, 20, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devauchelle-Pensec, V.; Berthelot, J.M.; Cornec, D.; Renaudineau, Y.; Marhadour, T.; Jousse-Joulin, S.; Querellou, S.; Garrigues, F.; De Bandt, M.; Gouillou, M.; et al. Efficacy of first-line tocilizumab therapy in early polymyalgia rheumatica: A prospective longitudinal study. Ann. Rheum. Dis. 2016, 75, 1506–1510. [Google Scholar] [CrossRef]
- Lally, L.; Forbess, L.; Hatzis, C.; Spiera, R. Brief report: A prospective open-label phase IIa trial of tocilizumab in the treatment of polymyalgia rheumatica. Arthritis Rheumatol. 2016, 68, 2550–2554. [Google Scholar] [CrossRef]
- Dasgupta, B.; Cimmino, M.A.; Maradit-Kremers, H.; Schmidt, W.A.; Schirmer, M.; Salvarani, C.; Bachta, A.; Dejaco, C.; Duftner, C.; Jensen, H.S.; et al. 2012 provisional classification criteria for polymyalgia rheumatica: A European League Against Rheumatism/American College of Rheumatology collaborative initiative. Arthritis Rheum. 2012, 64, 943–954. [Google Scholar] [CrossRef] [PubMed]
- Hunder, G.G.; Bloch, D.A.; Michel, B.A.; Stevens, M.B.; Arend, W.P.; Calabrese, L.H.; Edworthy, S.M.; Fauci, A.S.; Leavitt, R.Y.; Lie, J.T.; et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum. 1990, 33, 1122–1128. [Google Scholar] [CrossRef] [PubMed]
- Birra, D.; Bosello, S.L.; Peluso, G.; Zoli, A. Sixth-month remission as a predictor for twelve-month remission in polymyalgia rheumatica. Clin. Exp. Rheumathol. 2020, 38, 436–441. [Google Scholar]
- Cutolo, M.; Montecucco, C.M.; Cavagna, L.; Caporali, R.; Capellino, S.; Montagna, P.; Fazzuoli, L.; Villaggio, B.; Seriolo, B.; Sulli, A. Serum cytokines and steroidal hormones in polymyalgia rheumatica and elderly-onset rheumatoid arthritis. Ann. Rheum. Dis. 2006, 65, 1438–1443. [Google Scholar] [CrossRef] [Green Version]
- Nishina, N.; Kaneko, Y.; Kameda, H.; Kuwana, M.; Takeuchi, T. Reduction of plasma IL-6 but not TNF-α by methotrexate in patients with early rheumatoid arthritis: A potential biomarker for radiographic progression. Clin. Rheumatol. 2013, 32, 1661–1666. [Google Scholar] [CrossRef]
- Dejaco, C.; Singh, Y.P.; Perel, P.; Hutchings, A.; Camellino, D.; Mackie, S.; Abril, A.; Bachta, A.; Balint, P.; Barraclough, K.; et al. 2015 recommendations for the management of polymyalgia rheumatica: A European League Against Rheumatism/American College of Rheumatology collaborative initiative. Arthritis Rheumatol. 2015, 67, 2569–2580. [Google Scholar] [CrossRef]
- Toussirot, É.; Martin, A.; Soubrier, M.; Redeker, S.; Régent, A. Rapid and sustained response to tocilizumab in patients with polymyalgia rheumatica resistant or intolerant to glucocorticoids: A multicenter open-label study. J. Rheumatol. 2016, 43, 249–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, E.; Inoue, E.; Hoshi, D.; Shimizu, Y.; Kobayashi, A.; Sugimoto, N.; Shidara, K.; Sato, E.; Seto, Y.; Nakajima, A.; et al. Cost-effectiveness of tocilizumab, a humanized anti-interleukin-6 receptor monoclonal antibody, versus methotrexate in patients with rheumatoid arthritis using real-world data from the IORRA observational cohort study. Mod. Rheumatol. 2015, 25, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, C.; Kaneko, Y.; Okano, Y.; Taguchi, H.; Oshima, H.; Izumi, K.; Yamaoka, K.; Takeuchi, T. Association of erythrocyte methotrexate-polyglutamate levels with the efficacy and hepatotoxicity of methotrexate in patients with rheumatoid arthritis: A 76-week prospective study. RMD Open 2017, 3, e000363. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Prednisolone Group (N = 177) | Methotrexate Group (N = 32) | Tocilizumab Group (N = 15) | p-Values | |||
|---|---|---|---|---|---|---|
| PSL vs. MTX | PSL vs. TCZ | MTX vs. TCZ | ||||
| At diagnosis | ||||||
| Women, N (%) | 130 (73.5) | 25 (78.1) | 11 (73.3) | 0.57 | 0.99 | 0.53 |
| Age, year | 74.1 (67.5–79.5) | 74.4 (64.0–79.7) | 74.7 (66.0–83.5) | 0.71 | 0.71 | 0.40 |
| Body weight, kg | 52.4 (47.0–59.2) | 54.0 (44.3–59.2) | 52.0 (42.5–60.7) | 0.91 | 0.80 | 0.99 |
| CRP, mg/dL | 4.58 (2.30–8.31) | 6.40 (3.60–10.46) | 6.90 (3.35–10.33) | 0.07 | 0.24 | 1.00 |
| PSL dose, mg/day | 15.0 (10.0–15.0) | 15.0 (15.0–20.0) | 15.0 (15.0–20.0) | 0.02 * | 0.06 | 0.90 |
| At the initiation of the combination therapy | ||||||
| Age, year | – | 76.4 (68.1–81.9) | 76.4 (67.4–84.8) | – | – | 0.78 |
| Disease duration, month | – | 8.9 (3.6–41.7) | 21.3 (3.6–35.8) | – | – | 0.91 |
| CRP, mg/dL | – | 0.75 (0.20–1.71) | 0.86 (0.10–1.24) | – | – | 0.91 |
| PSL dose, mg/day | – | 8.5 (6.3–10.0) | 7.0 (5.0–8.0) | – | – | 0.08 |
| At the last follow-up | ||||||
| Disease duration, month | 63.1 (25.0–111) | 42.1 (20.5–88.8) | 47.0 (24.0–59.4) | 0.23 | 0.07 | 0.59 |
| Combination therapy duration, month | – | 26.6 (11.9–44.3) | 21.0 (15.0–31.0) | – | – | 0.59 |
| Discontinuation of PSL, N (%) | 49 (27.7) | 6 (18.8) | 12 (80.0) | 0.38 | <0.0001 * | <0.0001 * |
| PSL dose, mg/day | 3.0 (0–5.0) | 3.5 (1.6–6.0) | 0 (0–0) | 0.16 | <0.001 * | <0.001 * |
| Prednisolone Discontinuation at the Last Visit | p-Value | ||
|---|---|---|---|
| (+) N = 67 | (−) N = 157 | ||
| Women, N (%) | 47 (70.1) | 119 (75.8) | 0.407 |
| Age at diagnosis, year | 74.2 (66.3–80.4) | 74.4 (66.9–79.6) | 0.874 |
| Body weight at diagnosis, kg | 51.9 (45.1–60.0) | 53.0 (47.0–59.0) | 0.815 |
| CRP at diagnosis, mg/dL | 3.93 (2.23–7.35) | 5.55 (3–9.14) | 0.056 |
| Initial prednisolone dose, mg/day | 15.0 (10.0–15.0) | 15.0 (10.0–15.0) | 0.048 * |
| Prednisolone dose at the last visit, mg/day | 0 | 4 (2.75–6) | <0.0001 * |
| Treatment group, N (%) | Prednisolone 49 (73.1) Methotrexate 6 (9.0) Tocilizumab 12 (17.9) | Prednisolone 128 (81.5) Methotrexate 26 (16.6) Tocilizumab 3 (1.9) | <0.0001 * |
| Observation period, months | 56.1 (27.0–83.8) | 59.2 (22.8–113.8) | 0.479 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Sex (female/male) | 0.7504 (0.3989–1.4367) | 0.381 | ||
| Age at diagnosis, years | 0.9948 (0.9634–1.0277) | 0.753 | ||
| Body weight at diagnosis, kg | 0.9961 (0.9633–1.0296) | 0.816 | ||
| CRP at diagnosis, mg/dL | 0.9433 (0.8784–1.0062) | 0.077 | 0.9529 (0.9921–1.0293) | 0.221 |
| Initial prednisolone dose, mg/day | 0.9348 (0.8772–0.9962) | 0.028 * | 0.9080 (0.8409–0.9805) | 0.034 * |
| Disease duration at last visit, month | 0.9982 (0.9920–1.0019) | 0.248 | ||
| Tocilizumab use | 11.200 (3.4081–50.500) | <0.0001 * | 15.490 (3.1472–76.243) | <0.0001 * |
| Methotrexate use | 0.4956 (0.1772–1.1938) | 0.122 | ||
| Prednisolone Discontinuation at the Last Visit | p-Value | ||
|---|---|---|---|
| (+) N = 49 | (−) N = 128 | ||
| Women, N (%) | 33 (67.4) | 97 (75.8) | 0.260 |
| Age at diagnosis, year | 73.0 (67.5–78.0) | 74.4 (67.3–79.7) | 0.529 |
| Body weight at diagnosis, kg | 51.6 (46.7–60.1) | 52.7 (47.0–57.6) | 0.941 |
| CRP at diagnosis, mg/dL | 3.76 (2.25–6.92) | 5.15 (2.40–8.80) | 0.099 |
| Initial prednisolone dose, mg/day | 10.0 (10.0–15.0) | 15.0 (10.0–15.0) | 0.040 * |
| Prednisolone dose at the last visit, mg/day | 0 | 4 (2.5–6) | <0.0001 * |
| Disease duration at the last visit, months | 61.0 (25.0–95.6) | 63.1 (25.0–117.8) | 0.521 |
| (A) Prednisolone Discontinuation Rates in Patients with CRP Levels of >5 or ≤5 mg/dL at the Time of Diagnosis | ||||||
| CRP Levels | Prednisolone Group | Methotrexate Group | Tocilizumab Group | p-Values | ||
| Prednisolone vs. Methotrexate | Prednisolone vs. Tocilizumab | Methotrexate vs. Tocilizumab | ||||
| >5 mg/dL (N = 103), N (%) | 15 (19.5) | 1 (5.9) | 7 (77.9) | 0.288 | 0.001 * | <0.0001 * |
| ≤5 mg/dL (N = 121), N (%) | 34 (34.0) | 5 (33.3) | 5 (83.3) | 1.000 | 0.025 * | 0.063 |
| (B) Prednisolone Discontinuation Rates in the Patients with Initial Prednisolone Dose of ≥15 or <15 mg/day | ||||||
| Initial Prednisolone Dose | Prednisolone Group | Methotrexate Group | Tocilizumab Group | p-Values | ||
| Prednisolone vs. Methotrexate | Prednisolone vs. Tocilizumab | Methotrexate vs. Tocilizumab | ||||
| ≥15 mg/day (N = 131), N (%) | 21 (22.1) | 4 (16.7) | 9 (75.0) | 0.551 | 0.0003 * | 0.0005 * |
| <15 mg/day (N = 77), N (%) | 25 (36.2) | 1 (16.7) | 2 (100) | 0.307 | 0.046 * | 0.022 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izumi, K.; Murata, O.; Higashida-Konishi, M.; Kaneko, Y.; Oshima, H.; Takeuchi, T. Steroid-Sparing Effect of Tocilizumab and Methotrexate in Patients with Polymyalgia Rheumatica: A Retrospective Cohort Study. J. Clin. Med. 2021, 10, 2948. https://doi.org/10.3390/jcm10132948
Izumi K, Murata O, Higashida-Konishi M, Kaneko Y, Oshima H, Takeuchi T. Steroid-Sparing Effect of Tocilizumab and Methotrexate in Patients with Polymyalgia Rheumatica: A Retrospective Cohort Study. Journal of Clinical Medicine. 2021; 10(13):2948. https://doi.org/10.3390/jcm10132948
Chicago/Turabian StyleIzumi, Keisuke, Okinori Murata, Misako Higashida-Konishi, Yuko Kaneko, Hisaji Oshima, and Tsutomu Takeuchi. 2021. "Steroid-Sparing Effect of Tocilizumab and Methotrexate in Patients with Polymyalgia Rheumatica: A Retrospective Cohort Study" Journal of Clinical Medicine 10, no. 13: 2948. https://doi.org/10.3390/jcm10132948