
Echocardiography in Pulmonary Arterial Hypertension: Is It Time to Reconsider Its Prognostic Utility?

 , ,
, , 
Abstract
:1. Introduction
2. Right Ventricular Function in PAH
2.1. Pathophysiology of Right Ventricular Adaptation and Right Heart Failure
2.2. Prognostic Significance of Right Ventricular Function in PAH
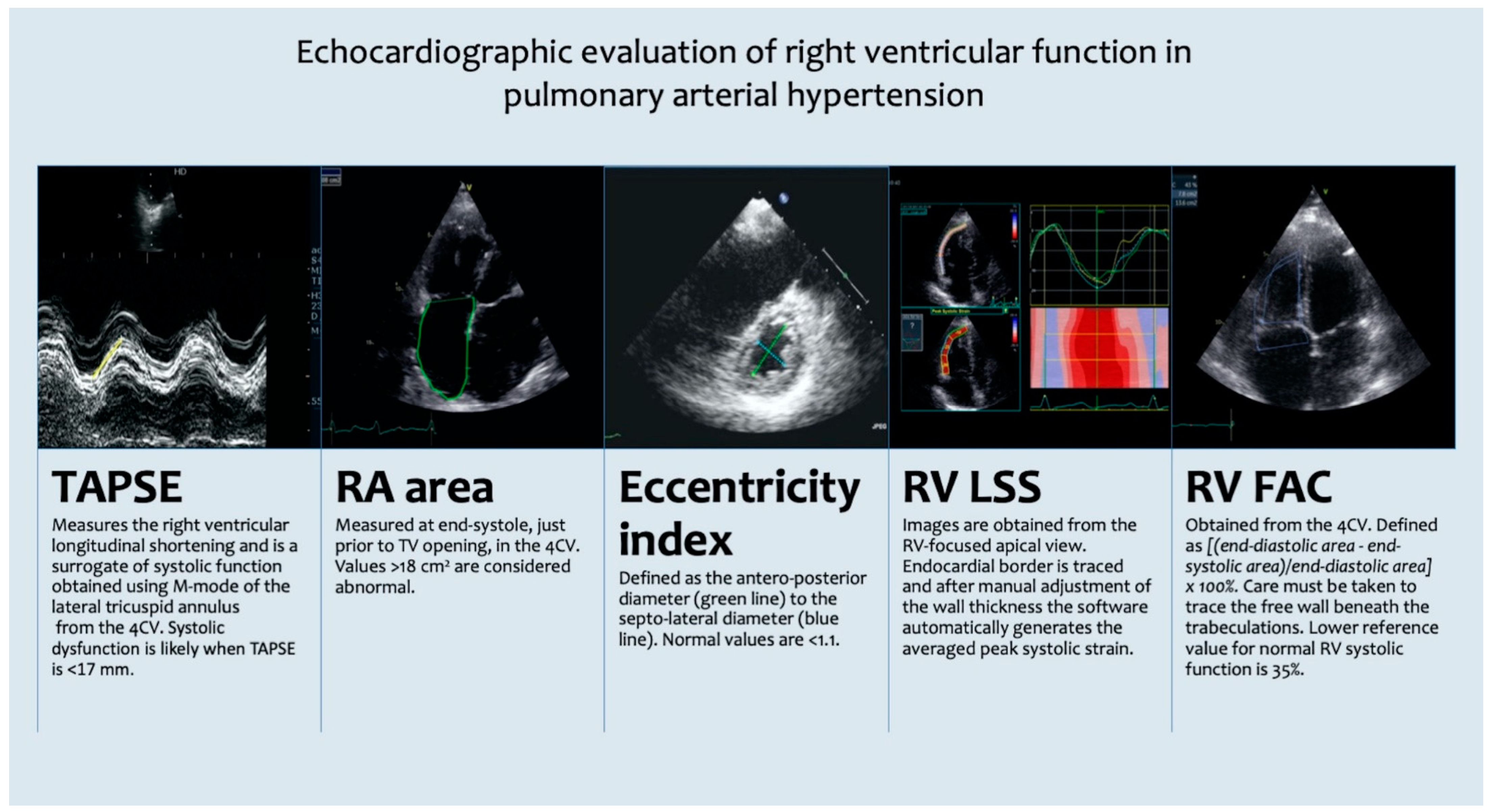
3. Echocardiographic Evaluation of Right Ventricular Function and Its Prognostic Relevance in PAH
4. Echocardiography in PAH
4.1. The Use of Echocardiography for Risk Stratification in PAH
4.2. Effects of PAH-Targeted Drug Therapy on the Right Ventricular Function
5. Follow-Up in PAH: Repeated Assessment with RHC or Echocardiography?
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Vonk-Noordegraaf, A.; Haddad, F.; Chin, K.M.; Forfia, P.R.; Kawut, S.M.; Lumens, J.; Naeije, R.; Newman, J.; Oudiz, R.J.; Provencher, S.; et al. Right Heart Adaptation to Pulmonary Arterial Hypertension: Physiology and Pathobiology. J. Am. Coll. Cardiol. 2013, 62, D22–D33. [Google Scholar] [CrossRef]
- Galiè, N.; Humbert, M.; Vachiery, J.-L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar]
- Champion, H.C.; Michelakis, E.D.; Hassoun, P.M. Comprehensive Invasive and Noninvasive Approach to the Right Ventricle–Pulmonary Circulation Unit. Circulation 2009, 120, 992–1007. [Google Scholar] [CrossRef] [Green Version]
- Vonk Noordegraaf, A.; Chin, K.M.; Haddad, F.; Hassoun, P.M.; Hemnes, A.R.; Hopkins, S.R.; Kawut, S.M.; Langleben, D.; Lumens, J.; Naeije, R. Pathophysiology of the right ventricle and of the pulmonary circulation in pulmonary hypertension: An update. Eur. Respir. J. 2019, 53, 1801900. [Google Scholar] [CrossRef]
- Vanderpool, R.R.; Pinsky, M.R.; Naeije, R.; Deible, C.; Kosaraju, V.; Bunner, C.; Mathier, M.A.; Lacomis, J.; Champion, H.C.; Simon, M.A. RV-pulmonary arterial coupling predicts outcome in patients referred for pulmonary hypertension. Heart Br. Card. Soc. 2015, 101, 37–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tello, K.; Seeger, W.; Naeije, R.; Vanderpool, R.; Ghofrani, H.A.; Richter, M.; Tedford, R.J.; Bogaard, H.J. Right heart failure in pulmonary hypertension: Diagnosis and new perspectives on vascular and direct right ventricular treatment. Br. J. Pharmacol. 2021, 178, 90–107. [Google Scholar] [CrossRef] [PubMed]
- Vonk Noordegraaf, A.; Westerhof, B.E.; Westerhof, N. The Relationship Between the Right Ventricle and its Load in Pulmonary Hypertension. J. Am. Coll. Cardiol. 2017, 69, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Gorter, T.M.; Willems, T.P.; van Melle, J.P. Ventricular interdependence in pulmonary arterial hypertension: Providing small pieces of a complex puzzle. Eur. J. Heart Fail. 2015, 17, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Hardziyenka, M.; Campian, M.E.; Reesink, H.J.; Surie, S.; Bouma, B.J.; Groenink, M.; Klemens, C.A.; Beekman, L.; Remme, C.A.; Bresser, P.; et al. Right ventricular failure following chronic pressure overload is associated with reduction in left ventricular mass: Evidence for atrophic remodeling. J. Am. Coll. Cardiol. 2011, 57, 921–928. [Google Scholar] [CrossRef] [Green Version]
- Gan, C.T.-J.; Lankhaar, J.-W.; Marcus, J.T.; Westerhof, N.; Marques, K.M.; Bronzwaer, J.G.F.; Boonstra, A.; Postmus, P.E.; Vonk-Noordegraaf, A. Impaired left ventricular filling due to right-to-left ventricular interaction in patients with pulmonary arterial hypertension. Am. J. Physiol. Heart Circ. Physiol. 2006, 290, H1528–H1533. [Google Scholar]
- Manders, E.; Bogaard, H.-J.; Handoko, M.L.; van de Veerdonk, M.C.; Keogh, A.; Westerhof, N.; Stienen, G.J.M.; dos Remedios, C.G.; Humbert, M.; Dorfmüller, P.; et al. Contractile Dysfunction of Left Ventricular Cardiomyocytes in Patients With Pulmonary Arterial Hypertension. J. Am. Coll. Cardiol. 2014, 64, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Han, J.-C.; Guild, S.-J.; Pham, T.; Nisbet, L.; Tran, K.; Taberner, A.J.; Loiselle, D.S. Left-Ventricular Energetics in Pulmonary Arterial Hypertension-Induced Right-Ventricular Hypertrophic Failure. Front. Physiol. 2018, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roca, G.Q.; Campbell, P.; Claggett, B.; Vazir, A.; Quinn, D.; Solomon, S.D.; Shah, A.M. Impact of lowering pulmonary vascular resistance on right and left ventricular deformation in pulmonary arterial hypertension. Eur. J. Heart Fail. 2015, 17, 63–73. [Google Scholar] [CrossRef] [Green Version]
- Mauritz, G.-J.; Vonk-Noordegraaf, A.; Kind, T.; Surie, S.; Kloek, J.J.; Bresser, P.; Saouti, N.; Bosboom, J.; Westerhof, N.; Marcus, J.T. Pulmonary endarterectomy normalizes interventricular dyssynchrony and right ventricular systolic wall stress. J. Cardiovasc. Magn. Reson. 2012, 14, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brewis, M.J.; Bellofiore, A.; Vanderpool, R.R.; Chesler, N.C.; Johnson, M.K.; Naeije, R.; Peacock, A.J. Imaging right ventricular function to predict outcome in pulmonary arterial hypertension. Int. J. Cardiol. 2016, 218, 206–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marc, H.; Olivier, S.; Ari, C.; Michèle, B.; Gilbert, H.; Virginie, G.; Azzedine, Y.; Emmanuel, W.; Jean-François, C.; François, C.; et al. Survival in Patients With Idiopathic, Familial, and Anorexigen-Associated Pulmonary Arterial Hypertension in the Modern Management Era. Circulation 2010, 122, 156–163. [Google Scholar]
- Lee, W.-T.N.; Ling, Y.; Sheares, K.K.; Pepke-Zaba, J.; Peacock, A.J.; Johnson, M.K. Predicting survival in pulmonary arterial hypertension in the UK. Eur. Respir. J. 2012, 40, 604–611. [Google Scholar] [CrossRef] [Green Version]
- Benza, R.L.; Miller, D.P.; Gomberg-Maitland, M.; Frantz, R.P.; Foreman, A.J.; Coffey, C.S.; Frost, A.; Barst, R.J.; Badesch, D.B.; Elliott, C.G.; et al. Predicting survival in pulmonary arterial hypertension: Insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation 2010, 122, 164–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thenappan, T.; Shah, S.J.; Rich, S.; Tian, L.; Archer, S.L.; Gomberg-Maitland, M. Survival in pulmonary arterial hypertension: A reappraisal of the NIH risk stratification equation. Eur. Respir. J. 2010, 35, 1079–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Veerdonk, M.C.; Kind, T.; Marcus, J.T.; Mauritz, G.-J.; Heymans, M.W.; Bogaard, H.-J.; Boonstra, A.; Marques, K.M.J.; Westerhof, N.; Vonk-Noordegraaf, A. Progressive Right Ventricular Dysfunction in Patients With Pulmonary Arterial Hypertension Responding to Therapy. J. Am. Coll. Cardiol. 2011, 58, 2511–2519. [Google Scholar] [CrossRef] [Green Version]
- Vanderpool, R.R.; Rischard, F.; Naeije, R.; Hunter, K.; Simon, M.A. Simple functional imaging of the right ventricle in pulmonary hypertension: Can right ventricular ejection fraction be improved? Int. J. Cardiol. 2016, 223, 93–94. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.; Pan, Z.; Wang, D.; Lv, J.; Fang, J.; Xu, R.; Ding, J.; Cui, X.; Xie, X.; Wang, X.; et al. Prognostic Value of Cardiac Magnetic Resonance–Derived Right Ventricular Remodeling Parameters in Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2020, 13, e010568. [Google Scholar] [CrossRef] [PubMed]
- Mouratoglou, S.A.; Kallifatidis, A.; Pitsiou, G.; Grosomanidis, V.; Kamperidis, V.; Chalikias, G.; Kristo, D.; Tziakas, D.; Konstantinides, S.; Hadjimiltiades, S.; et al. Duration of interventricular septal shift toward the left ventricle is associated with poor clinical outcome in precapillary pulmonary hypertension: A cardiac magnetic resonance study. Hell. J. Cardiol. HJC Hell. Kardiol. Ep. 2020, 61, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Hardegree, E.L.; Sachdev, A.; Fenstad, E.R.; Villarraga, H.R.; Frantz, R.P.; McGoon, M.D.; Oh, J.K.; Ammash, N.M.; Connolly, H.M.; Eidem, B.W.; et al. Impaired Left Ventricular Mechanics in Pulmonary Arterial Hypertension. Circ. Heart Fail. 2013, 6, 748–755. [Google Scholar] [CrossRef] [Green Version]
- Kishiki, K.; Singh, A.; Narang, A.; Gomberg-Maitland, M.; Goyal, N.; Maffessanti, F.; Besser, S.A.; Mor-Avi, V.; Lang, R.M.; Addetia, K. Impact of Severe Pulmonary Arterial Hypertension on the Left Heart and Prognostic Implications. J. Am. Soc. Echocardiogr. 2019, 32, 1128–1137. [Google Scholar] [CrossRef]
- Padervinskienė, L.; Krivickienė, A.; Hoppenot, D.; Miliauskas, S.; Basevičius, A.; Nedzelskienė, I.; Jankauskas, A.; Šimkus, P.; Ereminienė, E. Prognostic Value of Left Ventricular Function and Mechanics in Pulmonary Hypertension: A Pilot Cardiovascular Magnetic Resonance Feature Tracking Study. Medicina 2019, 55, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazar, J.M.; Flores, A.R.; Grandis, D.J.; Orie, J.E.; Schulman, D.S. Effects of chronic right ventricular pressure overload on left ventricular diastolic function. Am. J. Cardiol. 1993, 72, 1179–1182. [Google Scholar] [CrossRef]
- Tonelli, A.R.; Plana, J.C.; Heresi, G.A.; Dweik, R.A. Prevalence and prognostic value of left ventricular diastolic dysfunction in idiopathic and heritable pulmonary arterial hypertension. Chest 2012, 141, 1457–1465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knight, D.S.; Steeden, J.A.; Moledina, S.; Jones, A.; Coghlan, J.G.; Muthurangu, V. Left ventricular diastolic dysfunction in pulmonary hypertension predicts functional capacity and clinical worsening: A tissue phase mapping study. J. Cardiovasc. Magn. Reson. 2015, 17, 116. [Google Scholar] [CrossRef] [Green Version]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2010, 23, 685–713, quiz 786–788. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [Green Version]
- Hagger, D.; Condliffe, R.; Woodhouse, N.; Elliot, C.A.; Armstrong, I.J.; Davies, C.; Hill, C.; Akil, M.; Wild, J.M.; Kiely, D.G. Ventricular mass index correlates with pulmonary artery pressure and predicts survival in suspected systemic sclerosis-associated pulmonary arterial hypertension. Rheumatol. Oxf. Engl. 2009, 48, 1137–1142. [Google Scholar] [CrossRef] [Green Version]
- Vonk, M.C.; Sander, M.H.; van den Hoogen, F.H.J.; van Riel, P.L.C.M.; Verheugt, F.W.A.; van Dijk, A.P.J. Right ventricle Tei-index: A tool to increase the accuracy of non-invasive detection of pulmonary arterial hypertension in connective tissue diseases. Eur. J. Echocardiogr. J. Work. Group Echocardiogr. Eur. Soc. Cardiol. 2007, 8, 317–321. [Google Scholar] [CrossRef] [Green Version]
- Ghio, S.; Klersy, C.; Magrini, G.; D’Armini, A.M.; Scelsi, L.; Raineri, C.; Pasotti, M.; Serio, A.; Campana, C.; Viganò, M. Prognostic relevance of the echocardiographic assessment of right ventricular function in patients with idiopathic pulmonary arterial hypertension. Int. J. Cardiol. 2010, 140, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Ghio, S.; Pazzano, A.S.; Klersy, C.; Scelsi, L.; Raineri, C.; Camporotondo, R.; D’Armini, A.; Visconti, L.O. Clinical and prognostic relevance of echocardiographic evaluation of right ventricular geometry in patients with idiopathic pulmonary arterial hypertension. Am. J. Cardiol. 2011, 107, 628–632. [Google Scholar] [CrossRef]
- Sachdev, A.; Villarraga, H.R.; Frantz, R.P.; McGoon, M.D.; Hsiao, J.-F.; Maalouf, J.F.; Ammash, N.M.; McCully, R.B.; Miller, F.A.; Pellikka, P.A.; et al. Right ventricular strain for prediction of survival in patients with pulmonary arterial hypertension. Chest 2011, 139, 1299–1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forfia, P.R.; Fisher, M.R.; Mathai, S.C.; Housten-Harris, T.; Hemnes, A.R.; Borlaug, B.A.; Chamera, E.; Corretti, M.C.; Champion, H.C.; Abraham, T.P.; et al. Tricuspid annular displacement predicts survival in pulmonary hypertension. Am. J. Respir. Crit. Care Med. 2006, 174, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Grapsa, J.; Nunes, M.C.P.; Tan, T.C.; Cabrita, I.Z.; Coulter, T.; Smith, B.C.F.; Dawson, D.; Gibbs, J.S.R.; Nihoyannopoulos, P. Echocardiographic and Hemodynamic Predictors of Survival in Precapillary Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2015, 8, e002107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moriyama, H.; Murata, M.; Kataoka, M.; Kawakami, T.; Endo, J.; Kohno, T.; Itabashi, Y.; Seo, Y.; Iwao, Y.; Fukuda, K. Right Ventricle-Specific Three-Dimensional Wall Motion Tracking for Visualization of Regional Wall Motion Abnormality in Patients With Pulmonary Arterial Hypertension. Circ. Cardiovasc. Imaging 2019, 12, e008795. [Google Scholar] [CrossRef]
- Anavekar, N.S.; Gerson, D.; Skali, H.; Kwong, R.Y.; Yucel, E.K.; Solomon, S.D. Two-dimensional assessment of right ventricular function: An echocardiographic-MRI correlative study. Echocardiography (Mt. Kisco N.Y.) 2007, 24, 452–456. [Google Scholar] [CrossRef]
- Tei, C.; Dujardin, K.S.; Hodge, D.O.; Bailey, K.R.; McGoon, M.D.; Tajik, A.J.; Seward, J.B. Doppler echocardiographic index for assessment of global right ventricular function. J. Am. Soc. Echocardiogr. 1996, 9, 838–847. [Google Scholar] [CrossRef]
- Cabrita, I.Z.; Ruisanchez, C.; Dawson, D.; Grapsa, J.; North, B.; Howard, L.S.; Pinto, F.J.; Nihoyannopoulos, P.; Gibbs, J.S.R. Right ventricular function in patients with pulmonary hypertension; the value of myocardial performance index measured by tissue Doppler imaging. Eur. J. Echocardiogr. J. Work. Group Echocardiogr. Eur. Soc. Cardiol. 2010, 11, 719–724. [Google Scholar] [CrossRef] [Green Version]
- Sato, T.; Tsujino, I.; Ohira, H.; Oyama-Manabe, N.; Yamada, A.; Ito, Y.M.; Goto, C.; Watanabe, T.; Sakaue, S.; Nishimura, M. Validation study on the accuracy of echocardiographic measurements of right ventricular systolic function in pulmonary hypertension. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2012, 25, 280–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindqvist, P.; Waldenström, A.; Henein, M.; Mörner, S.; Kazzam, E. Regional and global right ventricular function in healthy individuals aged 20-90 years: A pulsed Doppler tissue imaging study: Umeå General Population Heart Study. Echocardiography (Mt. Kisco N.Y.) 2005, 22, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Ernande, L.; Cottin, V.; Leroux, P.-Y.; Girerd, N.; Huez, S.; Mulliez, A.; Bergerot, C.; Ovize, M.; Mornex, J.-F.; Cordier, J.-F.; et al. Right Isovolumic Contraction Velocity Predicts Survival in Pulmonary Hypertension. J. Am. Soc. Echocardiogr. 2013, 26, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Naeije, R.; Arena, R.; Corrà, U.; Ghio, S.; Forfia, P.; Rossi, A.; Cahalin, L.P.; Bandera, F.; Temporelli, P. Echocardiography of Right Ventriculoarterial Coupling Combined with Cardiopulmonary Exercise Testing to Predict Outcome in Heart Failure. Chest 2015, 148, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Tello, K.; Axmann, J.; Ghofrani, H.A.; Naeije, R.; Narcin, N.; Rieth, A.; Seeger, W.; Gall, H.; Richter, M.J. Relevance of the TAPSE/PASP ratio in pulmonary arterial hypertension. Int. J. Cardiol. 2018, 266, 229–235. [Google Scholar] [CrossRef]
- Tello, K.; Wan, J.; Dalmer, A.; Vanderpool, R.; Ghofrani, H.A.; Naeije, R.; Roller, F.; Mohajerani, E.; Seeger, W.; Herberg, U.; et al. Validation of the Tricuspid Annular Plane Systolic Excursion/Systolic Pulmonary Artery Pressure Ratio for the Assessment of Right Ventricular-Arterial Coupling in Severe Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2019, 12, e009047. [Google Scholar] [CrossRef]
- Prins, K.W.; Weir, E.K.; Archer, S.L.; Markowitz, J.; Rose, L.; Pritzker, M.; Madlon-Kay, R.; Thenappan, T. Pulmonary Pulse Wave Transit Time is Associated with Right Ventricular–Pulmonary Artery Coupling in Pulmonary Arterial Hypertension. Pulm. Circ. 2016, 6, 576–585. [Google Scholar] [CrossRef] [Green Version]
- French, S.; Amsallem, M.; Ouazani, N.; Li, S.; Kudelko, K.; Zamanian, R.T.; Haddad, F.; Chung, L. Non-invasive right ventricular load adaptability indices in patients with scleroderma-associated pulmonary arterial hypertension. Pulm. Circ. 2018, 8, 2045894018788268. [Google Scholar] [CrossRef] [Green Version]
- Boulate, D.; Amsallem, M.; Kuznetsova, T.; Zamanian, R.T.; Fadel, E.; Mercier, O.; Haddad, F. Echocardiographic evaluations of right ventriculo–arterial coupling in experimental and clinical pulmonary hypertension. Physiol. Rep. 2019, 7, e14322. [Google Scholar] [CrossRef] [PubMed]
- Levy, P.T.; El Khuffash, A.; Woo, K.V.; Singh, G.K. Right Ventricular-Pulmonary Vascular Interactions: An Emerging Role for Pulmonary Artery Acceleration Time by Echocardiography in Adults and Children. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2018, 31, 962–964. [Google Scholar] [CrossRef] [Green Version]
- Longobardo, L.; Suma, V.; Jain, R.; Carerj, S.; Zito, C.; Zwicke, D.L.; Khandheria, B.K. Role of Two-Dimensional Speckle-Tracking Echocardiography Strain in the Assessment of Right Ventricular Systolic Function and Comparison with Conventional Parameters. J. Am. Soc. Echocardiogr. 2017, 30, 937–946.e6. [Google Scholar] [CrossRef]
- Li, Y.; Wang, T.; Haines, P.; Li, M.; Wu, W.; Liu, M.; Chen, Y.; Jin, Q.; Xie, Y.; Wang, J.; et al. Prognostic Value of Right Ventricular Two-Dimensional and Three-Dimensional Speckle-Tracking Strain in Pulmonary Arterial Hypertension: Superiority of Longitudinal Strain over Circumferential and Radial Strain. J. Am. Soc. Echocardiogr. 2020, 33, 985–994.e1. [Google Scholar] [CrossRef]
- Vitarelli, A.; Mangieri, E.; Terzano, C.; Gaudio, C.; Salsano, F.; Rosato, E.; Capotosto, L.; D’Orazio, S.; Azzano, A.; Truscelli, G.; et al. Three-Dimensional Echocardiography and 2D-3D Speckle-Tracking Imaging in Chronic Pulmonary Hypertension: Diagnostic Accuracy in Detecting Hemodynamic Signs of Right Ventricular (RV) Failure. J. Am. Heart Assoc. 2015, 4, e001584. [Google Scholar] [CrossRef] [Green Version]
- Fine, N.M.; Chen, L.; Bastiansen, P.M.; Frantz, R.P.; Pellikka, P.A.; Oh, J.K.; Kane, G.C. Outcome Prediction by Quantitative Right Ventricular Function Assessment in 575 Subjects Evaluated for Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2013, 6, 711–721. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, M.; Mercurio, V.; Tedford, R.J.; Shah, A.A.; Hsu, S.; Mullin, C.J.; Sato, T.; Damico, R.; Kolb, T.M.; Mathai, S.C.; et al. Right ventricular longitudinal strain is diminished in systemic sclerosis compared with idiopathic pulmonary arterial hypertension. Eur. Respir. J. 2017, 50, 1701436. [Google Scholar] [CrossRef]
- Hulshof, H.G.; Eijsvogels, T.M.H.; Kleinnibbelink, G.; van Dijk, A.P.; George, K.P.; Oxborough, D.L.; Thijssen, D.H.J. Prognostic value of right ventricular longitudinal strain in patients with pulmonary hypertension: A systematic review and meta-analysis. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 475–484. [Google Scholar] [CrossRef]
- Badagliacca, R.; Pezzuto, B.; Papa, S.; Poscia, R.; Manzi, G.; Pascaretta, A.; Miotti, C.; Luongo, F.; Scoccia, G.; Ciciarello, F.; et al. Right Ventricular Strain Curve Morphology and Outcome in Idiopathic Pulmonary Arterial Hypertension. JACC Cardiovasc. Imaging 2021, 14, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Badagliacca, R.; Poscia, R.; Pezzuto, B.; Papa, S.; Gambardella, C.; Francone, M.; Mezzapesa, M.; Nocioni, M.; Nona, A.; Rosati, R.; et al. Right ventricular dyssynchrony in idiopathic pulmonary arterial hypertension: Determinants and impact on pump function. J. Heart Lung Transplant. 2015, 34, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Lamia, B.; Muir, J.-F.; Molano, L.-C.; Viacroze, C.; Benichou, J.; Bonnet, P.; Quieffin, J.; Cuvelier, A.; Naeije, R. Altered synchrony of right ventricular contraction in borderline pulmonary hypertension. Int. J. Cardiovasc. Imaging 2017, 33, 1331–1339. [Google Scholar] [CrossRef]
- Badagliacca, R.; Reali, M.; Poscia, R.; Pezzuto, B.; Papa, S.; Mezzapesa, M.; Nocioni, M.; Valli, G.; Giannetta, E.; Sciomer, S.; et al. Right Intraventricular Dyssynchrony in Idiopathic, Heritable, and Anorexigen-Induced Pulmonary Arterial Hypertension: Clinical Impact and Reversibility. JACC Cardiovasc. Imaging 2015, 8, 642–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badagliacca, R.; Papa, S.; Valli, G.; Pezzuto, B.; Poscia, R.; Reali, M.; Manzi, G.; Giannetta, E.; Berardi, D.; Sciomer, S.; et al. Right ventricular dyssynchrony and exercise capacity in idiopathic pulmonary arterial hypertension. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef] [PubMed]
- Grapsa, J.; O’Regan, D.P.; Pavlopoulos, H.; Durighel, G.; Dawson, D.; Nihoyannopoulos, P. Right ventricular remodelling in pulmonary arterial hypertension with three-dimensional echocardiography: Comparison with cardiac magnetic resonance imaging. Eur. J. Echocardiogr. 2010, 11, 64–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leibundgut, G.; Rohner, A.; Grize, L.; Bernheim, A.; Kessel-Schaefer, A.; Bremerich, J.; Zellweger, M.; Buser, P.; Handke, M. Dynamic Assessment of Right Ventricular Volumes and Function by Real-Time Three-Dimensional Echocardiography: A Comparison Study With Magnetic Resonance Imaging in 100 Adult Patients. J. Am. Soc. Echocardiogr. 2010, 23, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Maffessanti, F.; Muraru, D.; Esposito, R.; Gripari, P.; Ermacora, D.; Santoro, C.; Tamborini, G.; Galderisi, M.; Pepi, M.; Badano, L.P. Age-, body size-, and sex-specific reference values for right ventricular volumes and ejection fraction by three-dimensional echocardiography: A multicenter echocardiographic study in 507 healthy volunteers. Circ. Cardiovasc. Imaging 2013, 6, 700–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grapsa, J.; Gibbs, J.S.R.; Dawson, D.; Watson, G.; Patni, R.; Athanasiou, T.; Punjabi, P.P.; Howard, L.S.G.E.; Nihoyannopoulos, P. Morphologic and Functional Remodeling of the Right Ventricle in Pulmonary Hypertension by Real Time Three Dimensional Echocardiography. Am. J. Cardiol. 2012, 109, 906–913. [Google Scholar] [CrossRef]
- Sukmawan, R.; Watanabe, N.; Ogasawara, Y.; Yamaura, Y.; Yamamoto, K.; Wada, N.; Kume, T.; Okura, H.; Yoshida, K. Geometric Changes of Tricuspid Valve Tenting in Tricuspid Regurgitation Secondary to Pulmonary Hypertension Quantified by Novel System with Transthoracic Real-time 3-Dimensional Echocardiography. J. Am. Soc. Echocardiogr. 2007, 20, 470–476. [Google Scholar] [CrossRef]
- Grapsa, J.; Gibbs, J.S.R.; Cabrita, I.Z.; Watson, G.F.; Pavlopoulos, H.; Dawson, D.; Gin-Sing, W.; Howard, L.S.G.E.; Nihoyannopoulos, P. The association of clinical outcome with right atrial and ventricular remodelling in patients with pulmonary arterial hypertension: Study with real-time three-dimensional echocardiography. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 666–672. [Google Scholar] [CrossRef] [Green Version]
- Jone, P.-N.; Khoo, N. Innovation in 3D Echocardiographic Imaging. Curr. Treat. Options Cardiovasc. Med. 2018, 20, 1. [Google Scholar] [CrossRef]
- Nakaya, T.; Tsujino, I.; Nakamura, J.; Chiba, Y.; Iwano, H. Right ventricular pressure–volume loop produced with simultaneous application of three-dimensional echocardiography and high-fidelity micromanometry in a patient with pulmonary arterial hypertension. Echocardiography 2021, 38, 805–807. [Google Scholar] [CrossRef]
- Galiè, N.; Channick, R.N.; Frantz, R.P.; Grünig, E.; Jing, Z.C.; Moiseeva, O.; Preston, I.R.; Pulido, T.; Safdar, Z.; Tamura, Y.; et al. Risk stratification and medical therapy of pulmonary arterial hypertension. Eur. Respir. J. 2019, 53. [Google Scholar] [CrossRef]
- Mouratoglou, S.A.; Bayoumy, A.A.; Noordegraaf, A.V. Prediction Models and Scores in Pulmonary Hypertension: A Systematic Review. Curr. Pharm. Des. 2020, 27, 1266–1276. [Google Scholar] [CrossRef] [PubMed]
- Kylhammar, D.; Kjellström, B.; Hjalmarsson, C.; Jansson, K.; Nisell, M.; Söderberg, S.; Wikström, G.; Rådegran, G. A comprehensive risk stratification at early follow-up determines prognosis in pulmonary arterial hypertension. Eur. Heart J. 2018, 39, 4175–4181. [Google Scholar] [CrossRef] [PubMed]
- Hoeper, M.M.; Kramer, T.; Pan, Z.; Eichstaedt, C.A.; Spiesshoefer, J.; Benjamin, N.; Olsson, K.M.; Meyer, K.; Vizza, C.D.; Vonk-Noordegraaf, A.; et al. Mortality in pulmonary arterial hypertension: Prediction by the 2015 European pulmonary hypertension guidelines risk stratification model. Eur. Respir. J. 2017, 50, 1700740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boucly, A.; Weatherald, J.; Savale, L.; Jaïs, X.; Cottin, V.; Prevot, G.; Picard, F.; de Groote, P.; Jevnikar, M.; Bergot, E.; et al. Risk assessment, prognosis and guideline implementation in pulmonary arterial hypertension. Eur. Respir. J. 2017, 50, 1700889. [Google Scholar] [CrossRef] [Green Version]
- Benza, R.L.; Gomberg-Maitland, M.; Elliott, C.G.; Farber, H.W.; Foreman, A.J.; Frost, A.E.; McGoon, M.D.; Pasta, D.J.; Selej, M.; Burger, C.D.; et al. Predicting Survival in Patients With Pulmonary Arterial Hypertension: The REVEAL Risk Score Calculator 2.0 and Comparison With ESC/ERS-Based Risk Assessment Strategies. Chest 2019, 156, 323–337. [Google Scholar] [CrossRef] [Green Version]
- Hinderliter, A.L.; Willis, P.W.; Barst, R.J.; Rich, S.; Rubin, L.J.; Badesch, D.B.; Groves, B.M.; McGoon, M.D.; Tapson, V.F.; Bourge, R.C.; et al. Effects of long-term infusion of prostacyclin (epoprostenol) on echocardiographic measures of right ventricular structure and function in primary pulmonary hypertension. Primary Pulmonary Hypertension Study Group. Circulation 1997, 95, 1479–1486. [Google Scholar] [CrossRef]
- Raymond, R.J.; Hinderliter, A.L.; Willis, P.W.; Ralph, D.; Caldwell, E.J.; Williams, W.; Ettinger, N.A.; Hill, N.S.; Summer, W.R.; de Boisblanc, B.; et al. Echocardiographic predictors of adverse outcomes in primary pulmonary hypertension. J. Am. Coll. Cardiol. 2002, 39, 1214–1219. [Google Scholar] [CrossRef] [Green Version]
- Hinderliter, A.L.; Willis, P.W.; Long, W.; Clarke, W.R.; Ralph, D.; Caldwell, E.J.; Williams, W.; Ettinger, N.A.; Hill, N.S.; Summer, W.R.; et al. Frequency and prognostic significance of pericardial effusion in primary pulmonary hypertension. PPH Study Group. Primary pulmonary hypertension. Am. J. Cardiol. 1999, 84, 481–484, A10. [Google Scholar] [CrossRef]
- Liu, K.; Zhang, C.; Chen, B.; Li, M.; Zhang, P. Association between right atrial area measured by echocardiography and prognosis among pulmonary arterial hypertension: A systematic review and meta-analysis. BMJ Open 2020, 10, e031316. [Google Scholar] [CrossRef] [PubMed]
- Mouratoglou, S.A.; Dimopoulos, K.; Kamperidis, V.; Feloukidis, C.; Kallifatidis, A.; Pitsiou, G.; Stanopoulos, I.; Grosomanidis, V.; Hadjimiltiades, S.; Karvounis, H.; et al. Right Atrial Function Predicts Clinical Outcome in Patients with Precapillary Pulmonary Hypertension. J. Am. Soc. Echocardiogr. 2018, 31, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Hasselberg, N.E.; Kagiyama, N.; Soyama, Y.; Sugahara, M.; Goda, A.; Ryo-Koriyama, K.; Batel, O.; Chakinala, M.; Simon, M.A.; Gorcsan, J. The Prognostic Value of Right Atrial Strain Imaging in Patients with Pre-Capillary Pulmonary Hypertension. J. Am. Soc. Echocardiogr. 2021. [Google Scholar] [CrossRef]
- Miotti, C.; Papa, S.; Manzi, G.; Scoccia, G.; Luongo, F.; Toto, F.; Malerba, C.; Cedrone, N.; Sciomer, S.; Ciciarello, F.; et al. The Growing Role of Echocardiography in Pulmonary Arterial Hypertension Risk Stratification: The Missing Piece. J. Clin. Med. 2021, 10, 619. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; Manes, A.; Negro, L.; Palazzini, M.; Bacchi-Reggiani, M.L.; Branzi, A. A meta-analysis of randomized controlled trials in pulmonary arterial hypertension. Eur. Heart J. 2009, 30, 394–403. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Yu, M.; Zheng, X.; Dong, S. A Bayesian network meta-analysis on the efficacy and safety of eighteen targeted drugs or drug combinations for pulmonary arterial hypertension. Drug Deliv. 2018, 25, 1898–1909. [Google Scholar] [CrossRef]
- Gaine, S.; McLaughlin, V. Pulmonary arterial hypertension: Tailoring treatment to risk in the current era. Eur. Respir. Rev. Off. J. Eur. Respir. Soc. 2017, 26, 170095. [Google Scholar] [CrossRef] [Green Version]
- Peacock, A.J.; Crawley, S.; McLure, L.; Blyth, K.G.; Vizza, C.D.; Poscia, R.; Francone, M.; Iacucci, I.; Olschewski, H.; Kovacs, G.; et al. Changes in right ventricular function measured by cardiac magnetic resonance imaging in patients receiving pulmonary arterial hypertension-targeted therapy: The EURO-MR study. Circ. Cardiovasc. Imaging 2014, 7, 107–114. [Google Scholar] [CrossRef] [Green Version]
- D’Alto, M.; Badagliacca, R.; Argiento, P.; Romeo, E.; Farro, A.; Papa, S.; Sarubbi, B.; Russo, M.G.; Vizza, C.D.; Golino, P.; et al. Risk Reduction and Right Heart Reverse Remodeling by Upfront Triple Combination Therapy in Pulmonary Arterial Hypertension. Chest 2020, 157, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Saggar, R.; Khanna, D.; Vaidya, A.; Derhovanessian, A.; Maranian, P.; Duffy, E.; Belperio, J.A.; Weigt, S.S.; Dua, S.; Shapiro, S.S.; et al. Changes in right heart haemodynamics and echocardiographic function in an advanced phenotype of pulmonary hypertension and right heart dysfunction associated with pulmonary fibrosis. Thorax 2014, 69, 123–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mercurio, V.; Mukherjee, M.; Tedford, R.J.; Zamanian, R.T.; Khair, R.M.; Sato, T.; Minai, O.A.; Torres, F.; Girgis, R.E.; Chin, K.; et al. Improvement in Right Ventricular Strain with Ambrisentan and Tadalafil Upfront Therapy in Scleroderma-associated Pulmonary Arterial Hypertension. Am. J. Respir. Crit. Care Med. 2018, 197, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Taran, I.N.; Belevskaya, A.A.; Saidova, M.A.; Martynyuk, T.V.; Chazova, I.E. Initial Riociguat Monotherapy and Transition from Sildenafil to Riociguat in Patients with Idiopathic Pulmonary Arterial Hypertension: Influence on Right Heart Remodeling and Right Ventricular-Pulmonary Arterial Coupling. Lung 2018, 196, 745–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonelli, A.R.; Conci, D.; Tamarappoo, B.; Newman, J.; Dweik, R.A. Prognostic value of echocardiographic changes in patients with pulmonary arterial hypertension receiving parenteral prostacyclin therapy. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2014, 27, 733–741.e2. [Google Scholar] [CrossRef] [Green Version]
- Nath, J.; Demarco, T.; Hourigan, L.; Heidenreich, P.A.; Foster, E. Correlation between right ventricular indices and clinical improvement in epoprostenol treated pulmonary hypertension patients. Echocardiography (Mt. Kisco N.Y.) 2005, 22, 374–379. [Google Scholar] [CrossRef]
- Kaya, M.G.; Lam, Y.-Y.; Erer, B.; Ayhan, S.; Vatankulu, M.A.; Nurkalem, Z.; Meric, M.; Eren, M.; Eryol, N.K. Long-term effect of bosentan therapy on cardiac function and symptomatic benefits in adult patients with Eisenmenger syndrome. J. Card. Fail. 2012, 18, 379–384. [Google Scholar] [CrossRef]
- Kim, H.; Lee, J.B.; Park, J.-H.; Yoo, B.-S.; Son, J.-W.; Yang, D.H.; Lee, B.-R. A comparison of echocardiographic variables of right ventricular function with exercise capacity after bosentan treatment in patients with pulmonary arterial hypertension: Results from a multicenter, prospective, cohort study. J. Clin. Ultrasound 2017, 45, 28–34. [Google Scholar] [CrossRef]
- Borges, A.C.; Knebel, F.; Eddicks, S.; Panda, A.; Schattke, S.; Witt, C.; Baumann, G. Right Ventricular Function Assessed by Two-Dimensional Strain and Tissue Doppler Echocardiography in Patients With Pulmonary Arterial Hypertension and Effect of Vasodilator Therapy. Am. J. Cardiol. 2006, 98, 530–534. [Google Scholar] [CrossRef]
- Galiè, N.; Hinderliter, A.L.; Torbicki, A.; Fourme, T.; Simonneau, G.; Pulido, T.; Espinola-Zavaleta, N.; Rocchi, G.; Manes, A.; Frantz, R.; et al. Effects of the oral endothelin-receptor antagonist bosentan on echocardiographic and doppler measures in patients with pulmonary arterial hypertension. J. Am. Coll. Cardiol. 2003, 41, 1380–1386. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, M.J.; Escribano, P.; Delgado, J.F.; Jiménez, C.; Tello, R.; Gómez, M.A.; de la Calzada, C.S. Efficacy of sildenafil as a rescue therapy for patients with severe pulmonary arterial hypertension and given long-term treatment with prostanoids: 2-year experience. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2006, 25, 1353–1357. [Google Scholar] [CrossRef]
- López-Guarch, C.J.; Subias, P.E.; de Meneses, R.T.; Jiménez, J.F.D.; Pérez, D.S.; Martín, M.T.V.; Sánchez, M.A.G.; de la Calzada, C.S. Efficacy of oral sildenafil as rescue therapy in patients with severe pulmonary arterial hypertension chronically treated with prostacyclin. Long-term results. Rev. Esp. Cardiol. 2004, 57, 946–951. [Google Scholar] [CrossRef]
- Shah, A.M.; Campbell, P.; Rocha, G.Q.; Peacock, A.; Barst, R.J.; Quinn, D.; Solomon, S.D.; IMPRES Investigators. Effect of imatinib as add-on therapy on echocardiographic measures of right ventricular function in patients with significant pulmonary arterial hypertension. Eur. Heart J. 2015, 36, 623–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giusca, S.; Jurcut, R.; Coman, I.M.; Ghiorghiu, I.; Catrina, D.; Popescu, B.A.; Dima, L.; Ginghina, C. Right ventricular function predicts clinical response to specific vasodilator therapy in patients with pulmonary hypertension. Echocardiography (Mt. Kisco N.Y.) 2013, 30, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.-H.; Chen, J.-S.; Chen, R.J.; Ko, W.-J.; Kuo, S.-W.; Wu, E.-T.; Wu, M.-H.; Wang, J.-K.; Lee, Y.-C. Long-term outcome and effects of oral bosentan therapy in Taiwanese patients with advanced idiopathic pulmonary arterial hypertension. Respir. Med. 2007, 101, 1556–1562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassoun, P.M.; Zamanian, R.T.; Damico, R.; Lechtzin, N.; Khair, R.; Kolb, T.M.; Tedford, R.J.; Hulme, O.L.; Housten, T.; Pisanello, C.; et al. Ambrisentan and Tadalafil Up-front Combination Therapy in Scleroderma-associated Pulmonary Arterial Hypertension. Am. J. Respir. Crit. Care Med. 2015, 192, 1102–1110. [Google Scholar] [CrossRef] [Green Version]
- Agapito, A.F.; Sousa, L.; Oliveira, J.A.; Feliciano, J.; Cacela, D.; Quininha, J. Eisenmenger syndrome in the adult—Experience with new drugs for the treatment of pulmonary hypertension. Rev. Port. Cardiol. Orgao Of. Soc. Port. Cardiol. Port. J. Cardiol. Off. J. Port. Soc. Cardiol. 2005, 24, 421–431. [Google Scholar]
- Taçoy, G.; Başer, H.D.; Türkoğlu, S.; Cengel, A. The management of adult female patients with Eisenmenger syndrome and advanced pulmonary arterial hypertension treatment: Single center experience and follow-up for 5 years. Turk Kardiyol. Dernegi Arsivi Turk Kardiyol. Derneginin Yayin Organidir 2014, 42, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Hansmann, G.; Meinel, K.; Bukova, M.; Chouvarine, P.; Wåhlander, H.; Koestenberger, M.; European Pediatric Pulmonary Vascular Disease Network (EPPVDN). Selexipag for the treatment of children with pulmonary arterial hypertension: First multicenter experience in drug safety and efficacy. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2020, 39, 695–706. [Google Scholar] [CrossRef]
- Badagliacca, R.; Raina, A.; Ghio, S.; D’Alto, M.; Confalonieri, M.; Correale, M.; Corda, M.; Paciocco, G.; Lombardi, C.; Mulè, M.; et al. Influence of various therapeutic strategies on right ventricular morphology, function and hemodynamics in pulmonary arterial hypertension. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2018, 37, 365–375. [Google Scholar] [CrossRef]
- Gabrielli, L.; Ocaranza, M.P.; Sitges, M.; Kanacri, A.; Saavedra, R.; Sepulveda, P.; Sepulveda, L.; Rossel, V.; Zagolin, M.; Verdejo, H.E.; et al. Acute effect of iloprost inhalation on right atrial function and ventricular dyssynchrony in patients with pulmonary artery hypertension. Echocardiography (Mt. Kisco N.Y.) 2017, 34, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Cha, K.S.; Cho, K.I.; Seo, J.S.; Choi, J.H.; Park, Y.H.; Yang, D.H.; Hong, G.R.; Kim, D.S. Effects of inhaled iloprost on exercise capacity, quality of life, and cardiac function in patients with pulmonary arterial hypertension secondary to congenital heart disease (the Eisenmenger syndrome) (from the EIGER Study). Am. J. Cardiol. 2013, 112, 1834–1839. [Google Scholar] [CrossRef]
- Marra, A.M.; Halank, M.; Benjamin, N.; Bossone, E.; Cittadini, A.; Eichstaedt, C.A.; Egenlauf, B.; Harutyunova, S.; Fischer, C.; Gall, H.; et al. Right ventricular size and function under riociguat in pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension (the RIVER study). Respir. Res. 2018, 19, 258. [Google Scholar] [CrossRef] [PubMed]
- Hardegree, E.L.; Sachdev, A.; Villarraga, H.R.; Frantz, R.P.; McGoon, M.D.; Kushwaha, S.S.; Hsiao, J.-F.; McCully, R.B.; Oh, J.K.; Pellikka, P.A.; et al. Role of serial quantitative assessment of right ventricular function by strain in pulmonary arterial hypertension. Am. J. Cardiol. 2013, 111, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, J.A.; Vaidya, A.; Mathai, S.C.; Roberts, J.D.; Forfia, P.R. Follow-up tricuspid annular plane systolic excursion predicts survival in pulmonary arterial hypertension. Pulm. Circ. 2017, 7, 361–371. [Google Scholar] [CrossRef] [Green Version]
- Shelburne, N.J.; Parikh, K.S.; Chiswell, K.; Shaw, L.K.; Sivak, J.; Arges, K.; Tomfohr, J.; Velazquez, E.J.; Kisslo, J.; Samad, Z.; et al. Echocardiographic Assessment of Right Ventricular Function and Response to Therapy in Pulmonary Arterial Hypertension. Am. J. Cardiol. 2019, 124, 1298–1304. [Google Scholar] [CrossRef]
- Sebbag, I.; Rudski, L.G.; Therrien, J.; Hirsch, A.; Langleben, D. Effect of chronic infusion of epoprostenol on echocardiographic right ventricular myocardial performance index and its relation to clinical outcome in patients with primary pulmonary hypertension. Am. J. Cardiol. 2001, 88, 1060–1063. [Google Scholar] [CrossRef]
- Ogihara, Y.; Yamada, N.; Dohi, K.; Matsuda, A.; Tsuji, A.; Ota, S.; Ishikura, K.; Nakamura, M.; Ito, M. Utility of right ventricular Tei-index for assessing disease severity and determining response to treatment in patients with pulmonary arterial hypertension. J. Cardiol. 2014, 63, 149–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeper, M.M.; Pittrow, D.; Opitz, C.; Gibbs, J.S.R.; Rosenkranz, S.; Grünig, E.; Olsson, K.M.; Huscher, D. Risk assessment in pulmonary arterial hypertension. Eur. Respir. J. 2018, 51, 1702606. [Google Scholar] [CrossRef]
- Van de Veerdonk, M.C.; Marcus, J.T.; Westerhof, N.; de Man, F.S.; Boonstra, A.; Heymans, M.W.; Bogaard, H.-J.; Vonk Noordegraaf, A. Signs of right ventricular deterioration in clinically stable patients with pulmonary arterial hypertension. Chest 2015, 147, 1063–1071. [Google Scholar] [CrossRef]
- Haddad, F.; Spruijt, O.A.; Denault, A.Y.; Mercier, O.; Brunner, N.; Furman, D.; Fadel, E.; Bogaard, H.J.; Schnittger, I.; Vrtovec, B.; et al. Right Heart Score for Predicting Outcome in Idiopathic, Familial, or Drug- and Toxin-Associated Pulmonary Arterial Hypertension. JACC Cardiovasc. Imaging 2015, 8, 627–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amsallem, M.; Sweatt, A.J.; Aymami, M.C.; Kuznetsova, T.; Selej, M.; Lu, H.; Mercier, O.; Fadel, E.; Schnittger, I.; McConnell, M.V.; et al. Right Heart End-Systolic Remodeling Index Strongly Predicts Outcomes in Pulmonary Arterial Hypertension. Circ. Cardiovasc. Imaging 2017, 10, e005771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stolfo, D.; Albani, S.; Biondi, F.; Luca, A.D.; Barbati, G.; Howard, L.; Giudice, F.L.; Tsampasian, V.; Pasanisi, E.M.; Airò, E.; et al. Global Right Heart Assessment with Speckle-Tracking Imaging Improves the Risk Prediction of a Validated Scoring System in Pulmonary Arterial Hypertension. J. Am. Soc. Echocardiogr. 2020, 33, 1334–1344.e2. [Google Scholar] [CrossRef] [PubMed]
- Ghio, S.; Mercurio, V.; Fortuni, F.; Forfia, P.R.; Gall, H.; Ghofrani, A.; Mathai, S.C.; Mazurek, J.A.; Mukherjee, M.; Richter, M.; et al. A comprehensive echocardiographic method for risk stratification in pulmonary arterial hypertension. Eur. Respir. J. 2020, 56. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.-H.; Gong, S.-G.; Jiang, R.; Li, C.; Chen, G.-F.; Luo, C.-J.; Qiu, H.-L.; Liu, J.-M.; Wang, L.; Zhang, R. Echocardiographic Prognosis Relevance of Attenuated Right Heart Remodeling in Idiopathic Pulmonary Arterial Hypertension. Front. Cardiovasc. Med. 2021, 8, 650848. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | N of Patients | Treatment (Duration) | Effect on ECHO Parameters | Effect on Other Parameters |
|---|---|---|---|---|
| D’Alto et al. [89] [2020) | 21 | Ambrisentan + Tadalafil + Treprostinil (2 years) | ↓RAA ↓RVA ↓LV EI ↑RVFAC | ↑6MWD ↓RAP ↓mPAP ↓PVR ↓NT-proBNP ↑CI |
| Saggar et al. (2013) [90] | 15 | Treprostinil (12 weeks) | ↓RVEDA ↓LV EI ↑TAPSE | ↑6MWD ↓RAP ↓mPAP ↑CI ↓PVR ↓TPG ↓SVi ↓BNP |
| Mercurio et al. (2017) [91] | 23 (Scleroderma patients) | Tadalafil + Ambrisentan (36 weeks) | ↓RAA ↓RVA ↓RV FWT ↑RVFAC ↑TAPSE ↓RVSP ↓RVLSS | |
| Taran et al. (2018) [92] | 20 | Riociguat (12 weeks) | ↓RAA ↓RV basal diameter ↑TAPSE ↓Diastolic EI ↑RV FAC ↓PASP ↓RVEDV ↓RVESV ↑RVEF ↓RV-PA coupling ↓PA Ea | ↑6MWD ↑Peak VO2 |
| Tonelli et al. (2014) [93] | 48 | Parenteral prostacyclin analogues (12 months) | ↓RAA ↓RVA ↓TVR Vmax ↑TAPSE ↑RVOT VTI | |
| Nath et al. (2005) [94] | 20 | Epoprostenol (22.7 ± 9.3 months) | (−) RVMPI ↓TVR Vmax ↓PASP/PV VTI | |
| Hinderliter et al. (1997) [78] | 81 | Epoprostenol (12 weeks) | ↓RVEDA ↓RV EI ↓TVR jet (−) PE (−) RVFAC | |
| Kaya et al. (2012) [95] | 23 (Eisenmenger patients) | Bosentan (24 ± 9 months) | ↓PASP ↓MPI ↑Sa ↑Ea | ↑6MWD ↑Sat02 |
| Kim et al. (2016) [96] | 19 | Bosentan (6 months) | ↓RVSP ↑TAPSE ↑MPI (LV-RV) ↑RVFAC ↑RVEF | ↑6MWD |
| Borges et al. (2006) [97] | 37 | Vasodilators (8 ± 3 months) | ↓RV 2d-strain | |
| Galie et al. (2003) [98] | 56 | Bosentan (16 weeks) | ↓RV ESA ↓RV EDA ↓LV EDA ↓LV EI ↑CI ↑LV early Diastolic filling pressures Improves PE score | ↑6MWD |
| Ruiz et al. (2006) [99] | 20 | Prostanoids + Sildenafil * (2 years) | ↓RVEDD ↓LVEI ↓RAA | ↑6MWD |
| Jimenez Loper-Guarch et al. (2004) [100] | 11 | Prostacyclin + Sildenafil * (12 months) | ↓RVEDD ↓LV EI | ↑6MWD |
| Shat et al. (2015) [101] | 202 | Imatinib + 2 PAH specific Drugs (24 months) | ↑TA S’ RV Tei ↑Index (−) TAPSE | |
| Gusca et al. (2012) [102] | 32 (Eisenmenger patients) | Bosentan Sildenafil Bosentan + Sildenafil (14 months) | (−) RVFAC (−) RV global strain | |
| Hsu et al. (2007) [103] | 15 | Bosentan (12 months) | ↑RVEF | ↑6MWD ↓CTR |
| Hassoun et al. (2015) [104] | 24 (Scleroderma patients) | Ambrisentan + Tadalafil (36 weeks) | (−) RVEDV ↓RVESV ↑RVEF ↑LVEDV ↑LVESV ↑TAPSE | ↓RV mass ↓PVR ↓mPAP ↓RAP ↑CI ↑Sat O2 ↑NTproBNP ↑6MWD ↑SV/PP |
| Agapito et al. (2008) [105] | 5 (Eisenmenger patients) | Iloprost Sildenafil Bosentan | ↓RV-RA gr RV Tei ↓index | ↑6MWD |
| Tacoy et al. (2014) [106] | 12 (Eisenmenger patients) | Iloprost Sildenafil Bosentan (5 years) | ↓PASP ↓RVFWT ↓PV ac t ↑RAA/LAA ↑RVFAC | ↓RAP |
| Hansmann et al. (2020) [107] | 15 (children) | Selexipag (8 months) | ↑TAPSE | ↓RAP ↓TPG ↓mPAP |
| Badagliacca et al. (2018) [108] | 69 | ERA PDE5i Prostanoids (155 ± 65 days) | ↓RVEDA ↓RVESA ↑RVFAC ↑TAPSE ↑RAA ↓LVEDA ↓LVESA ↓LVEI | ↑6MWD ↓RAP ↓mPAP ↑CI ↓PVR |
| Gabrielli et al. (2016) [109] | 20 | Iloprost | ↑RVFAC ↓RV Dys in ↑RA res f | |
| Cha et al. (2013) [110] | 18 (Eisenmenger patients) | Iloprost (24 weeks) | ↓RVMPI (−) PASP | ↑MWD (−) PVR |
| Marra et al. (2018) [111] | 71 | Riociguat (12 months) | ↓RAA ↓RVA ↓RVFWT ↓TVR ↑TAPSE ↑RVFAC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farmakis, I.T.; Demerouti, E.; Karyofyllis, P.; Karatasakis, G.; Stratinaki, M.; Tsiapras, D.; Athanassopoulos, G.; Voudris, V.; Giannakoulas, G. Echocardiography in Pulmonary Arterial Hypertension: Is It Time to Reconsider Its Prognostic Utility? J. Clin. Med. 2021, 10, 2826. https://doi.org/10.3390/jcm10132826
Farmakis IT, Demerouti E, Karyofyllis P, Karatasakis G, Stratinaki M, Tsiapras D, Athanassopoulos G, Voudris V, Giannakoulas G. Echocardiography in Pulmonary Arterial Hypertension: Is It Time to Reconsider Its Prognostic Utility? Journal of Clinical Medicine. 2021; 10(13):2826. https://doi.org/10.3390/jcm10132826
Chicago/Turabian StyleFarmakis, Ioannis T., Eftychia Demerouti, Panagiotis Karyofyllis, George Karatasakis, Maria Stratinaki, Dimitrios Tsiapras, George Athanassopoulos, Vassilios Voudris, and George Giannakoulas. 2021. "Echocardiography in Pulmonary Arterial Hypertension: Is It Time to Reconsider Its Prognostic Utility?" Journal of Clinical Medicine 10, no. 13: 2826. https://doi.org/10.3390/jcm10132826