
Vaccine Effects on Susceptibility and Symptomatology Can Change the Optimal Allocation of COVID-19 Vaccines: South Korea as an Example


Abstract
:1. Introduction
2. Methods
2.1. Epidemiological Data
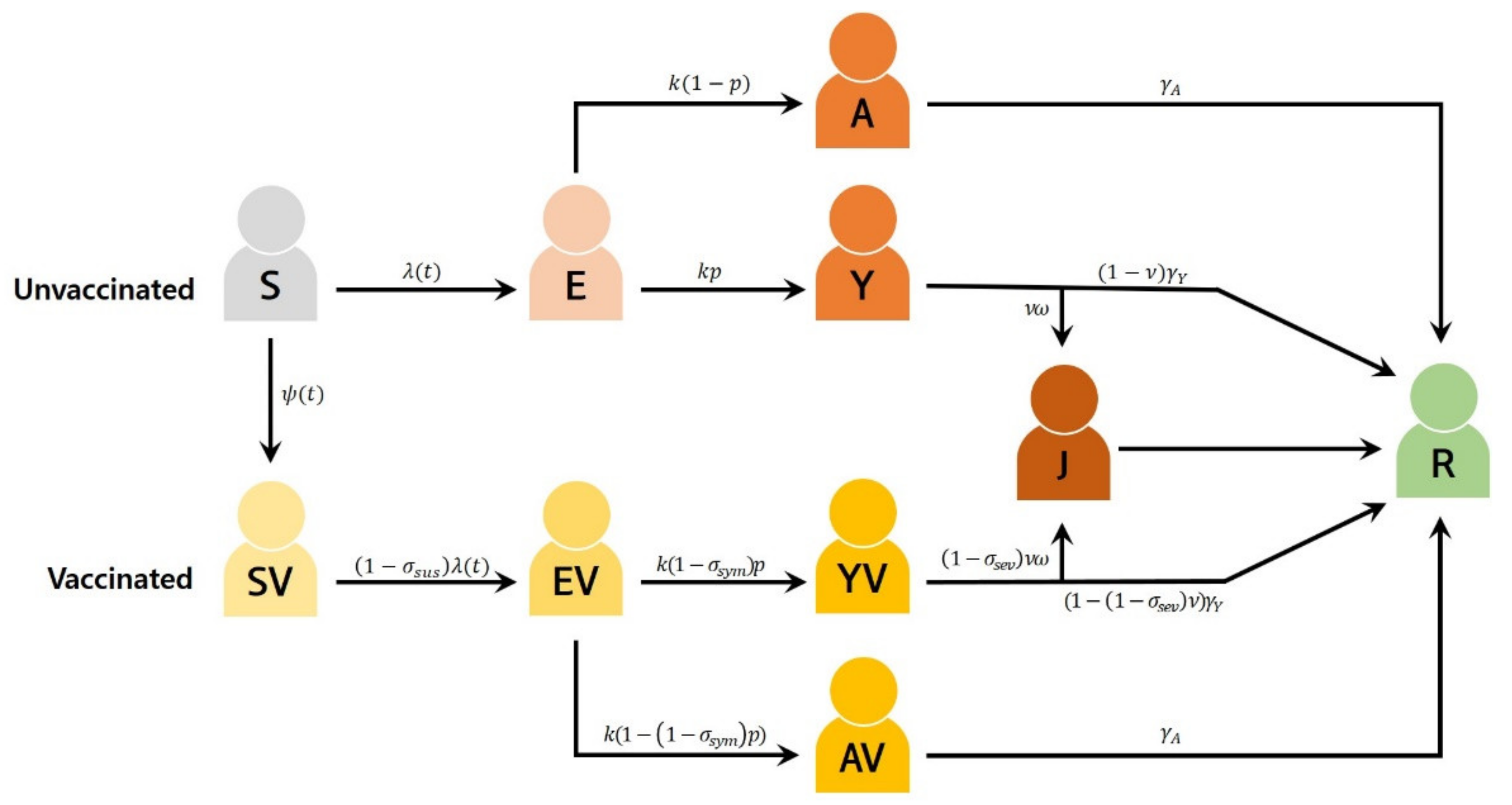
2.2. Mathematical Model of COVID-19 Transmission and Vaccination
2.3. Basic Reproduction Number
2.4. Vaccination Scenarios
2.5. Formulation of the Optimal Control Problem
3. Results
3.1. Optimal Immunization Strategy with Vaccines That Reduces the Risk of COVID-19 by 70%
3.2. Impact of a Higher Vaccine Efficacy
3.3. Impact of Higher Vaccine Supply Level
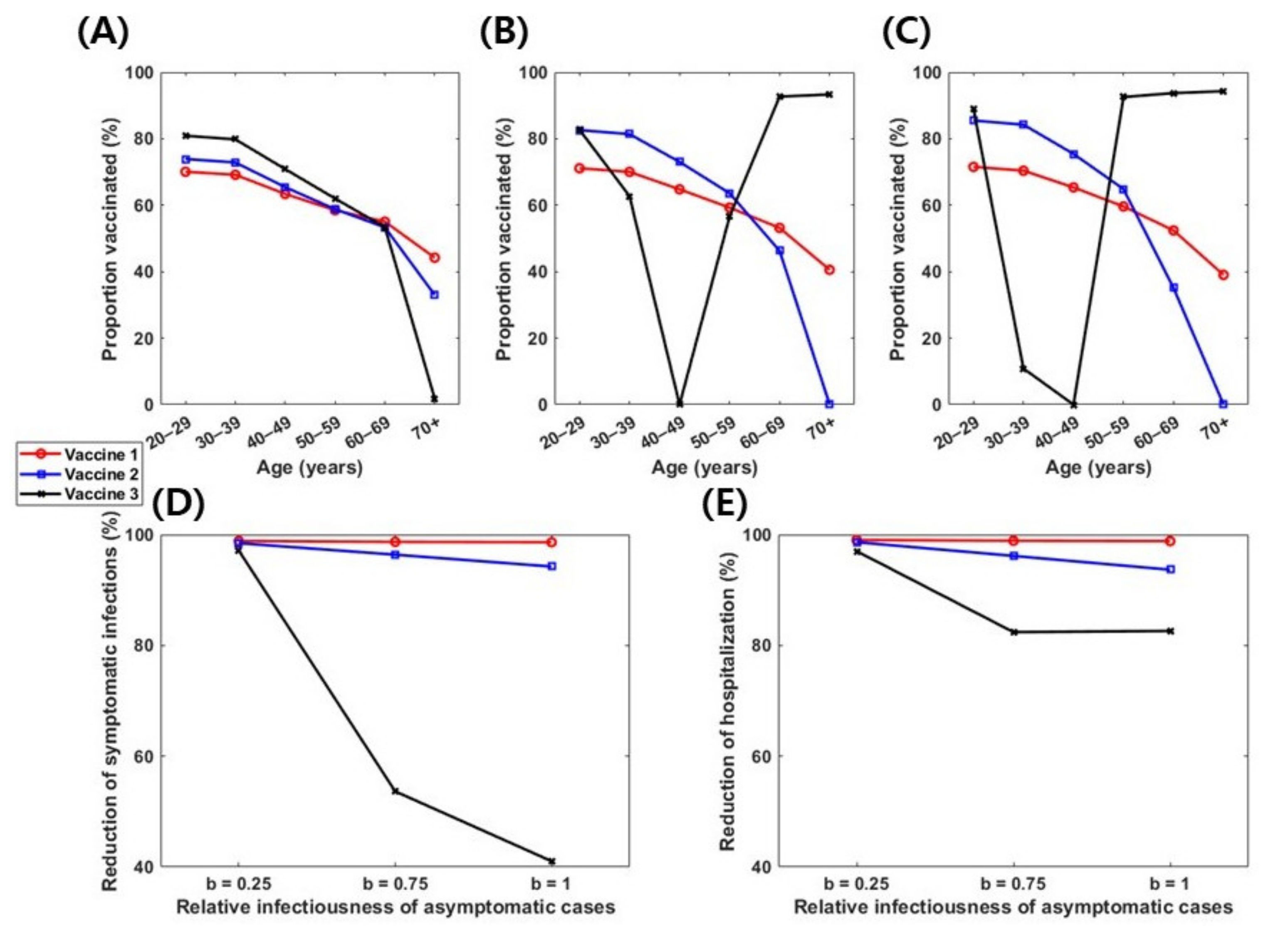
3.4. Impact of Relative Infectiousness of Asymptomatic Infections
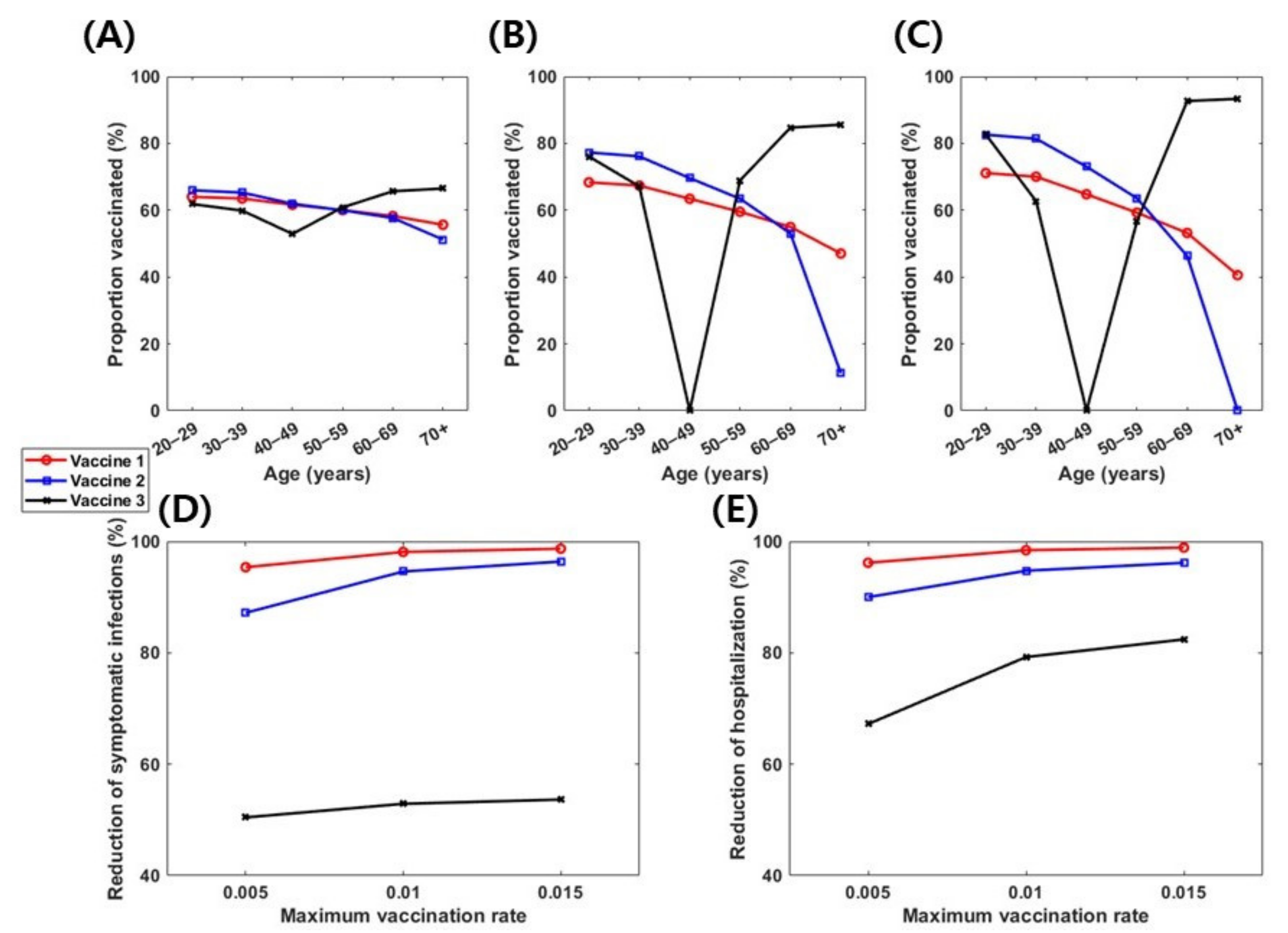
3.5. Impact of Daily Vaccination Capacity
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- WHO. Coronavirus disease 2019 (COVID-19): Situation Report; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- KDCA. The Updates of COVID-19 in Republic of Korea; Korea Disease Control and Prevention Agency: Cheongju, Korea, 2021. [Google Scholar]
- Shim, E.; Tariq, A.; Choi, W.; Lee, Y.; Chowell, G. Transmission potential and severity of COVID-19 in South Korea. Int. J. Infect. Dis. 2020, 93, 339–344. [Google Scholar] [CrossRef]
- Shim, E.; Tariq, A.; Chowell, G. Spatial variability in reproduction number and doubling time across two waves of the COVID-19 pandemic in South Korea, February to July, 2020. Int. J. Infect. Dis. 2020, 102, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Corey, L.; Mascola, J.R.; Fauci, A.S.; Collins, F.S. A strategic approach to COVID-19 vaccine R&D. Science 2020, 368, 948–950. [Google Scholar] [PubMed]
- Jonathan Corum, S.-L.W.a.C.Z. Coronavirus Vaccine Tracker. Available online: https://www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tracker.html (accessed on 17 April 2021).
- MFDS. Available online: https://www.mfds.go.kr/eng/index.do (accessed on 16 April 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2020, 384, 403–416. [Google Scholar] [CrossRef]
- Thompson, M.G.; Burgess, J.L.; Naleway, A.L.; Tyner, H.L.; Yoon, S.K.; Meece, J.; Olsho, L.E.W.; Caban-Martinez, A.J.; Fowlkes, A.; Lutrick, K.; et al. Interim Estimates of Vaccine Effectiveness of BNT162b2 and mRNA-1273 COVID-19 Vaccines in Preventing SARS-CoV-2 Infection Among Health Care Personnel, First Responders, and Other Essential and Frontline Workers - Eight U.S. Locations, December 2020-March 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 495–500. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2020, 397, 99–111. [Google Scholar] [CrossRef]
- Tande, A.J.; Pollock, B.D.; Shah, N.D.; Farrugia, G.; Virk, A.; Swift, M.; Breeher, L.; Binnicker, M.; Berbari, E.F. Impact of the COVID-19 Vaccine on Asymptomatic Infection Among Patients Undergoing Pre-Procedural COVID-19 Molecular Screening. Clin. Infect.Dis. Off. Publ. Infect. Dis. Soc. Am. 2021. [Google Scholar] [CrossRef]
- Daniel, W.; Nivet, M.; Warner, J.; Podolsky, D.K. Early Evidence of the Effect of SARS-CoV-2 Vaccine at One Medical Center. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Amit, S.; Regev-Yochay, G.; Afek, A.; Kreiss, Y.; Leshem, E. Early rate reductions of SARS-CoV-2 infection and COVID-19 in BNT162b2 vaccine recipients. Lancet 2021, 397, 875–877. [Google Scholar] [CrossRef]
- Haelle, T. Yes, Vaccines Block Most Transmission of COVID-19. Available online: https://www.nationalgeographic.com/science/article/yes-vaccines-block-most-transmission-of-covid-19 (accessed on 21 April 2021).
- FDA. In Vaccines and Related Biological Products Advisory Committee Meeting February 26; 2021. Available online: https://www.fda.gov/media/146217/download (accessed on 16 April 2021).
- Ekawati, A. Indonesia’s COVID Vaccination Campaign Prioritizes Workers. Available online: https://www.dw.com/en/indonesias-covid-vaccination-campaign-prioritizes-workers/a-56316852 (accessed on 17 April 2021).
- CDC. CDC’s COVID-19 Vaccine Rollout Recommendations. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations.html (accessed on 17 April 2021).
- Government of Canada. Vaccines and Treatments for COVID-19: Vaccine Rollout. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/prevention-risks/covid-19-vaccine-treatment/vaccine-rollout.html#a3 (accessed on 17 April 2021).
- Ministry of Health. Vaccines for Coronavirus. Available online: https://govextra.gov.il/ministry-of-health/covid19-vaccine/home-en/#vaccination (accessed on 17 April 2021).
- Bicker, L. South Korea coronavirus: PM aims for ‘herd immunity by autumn’. BBC, 23 February 2021. [Google Scholar]
- Piguillem, F.; Shi, L. The Optimal COVID-19 Quarantine and Testing Policies; Einaudi Institute for Economics and Finance (EIEF): Rome, Italy, 2020. [Google Scholar]
- Moore, S.; Hill, E.M.; Dyson, L.; Tildesley, M.J.; Keeling, M.J. Modelling optimal vaccination strategy for SARS-CoV-2 in the UK. PLoS Comput. Biol. 2021, 17, e1008849. [Google Scholar] [CrossRef]
- Richard, Q.; Alizon, S.; Choisy, M.; Sofonea, M.T.; Djidjou-Demasse, R. Age-structured non-pharmaceutical interventions for optimal control of COVID-19 epidemic. PLoS Comput. Biol. 2021, 17, e1008776. [Google Scholar] [CrossRef]
- Choi, W.; Shim, E. Optimal Strategies for Social Distancing and Testing to Control COVID-19. J. Theor. Biol. 2020, 512, 110568. [Google Scholar] [CrossRef]
- Matrajt, L.; Eaton, J.; Leung, T.; Brown, E.R. Vaccine optimization for COVID-19: Who to vaccinate first? Sci. Adv. 2020, 7. [Google Scholar] [CrossRef]
- Meehan, M.T.; Cocks, D.G.; Caldwell, J.M.; Trauer, J.M.; Adekunle, A.I.; Ragonnet, R.R.; McBryde, E.S. Age-targeted dose allocation can halve COVID-19 vaccine requirements. medRxiv 2020. [Google Scholar] [CrossRef]
- Buckner, J.H.; Chowell, G.; Springborn, M.R. Dynamic prioritization of COVID-19 vaccines when social distancing is limited for essential workers. Proc. Natl. Acad. Sci. USA 2021, 118, e2025786118. [Google Scholar] [CrossRef] [PubMed]
- Bubar, K.M.; Reinholt, K.; Kissler, S.M.; Lipsitch, M.; Cobey, S.; Grad, Y.H.; Larremore, D.B. Model-informed COVID-19 vaccine prioritization strategies by age and serostatus. Science 2021, 371, 916–921. [Google Scholar] [CrossRef]
- Shim, E. Optimal Allocation of the Limited COVID-19 Vaccine Supply in South Korea. J. Clin. Med. 2021, 10, 591. [Google Scholar] [CrossRef]
- Prem, K.; Cook, A.R.; Jit, M. Projecting social contact matrices in 152 countries using contact surveys and demographic data. PLoS Comput. Biol. 2017, 13, e1005697. [Google Scholar] [CrossRef]
- Mizumoto, K.; Kagaya, K.; Zarebski, A.; Chowell, G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Eurosurveillance 2020, 25, 2000180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishiura, H.; Kobayashi, T.; Miyama, T.; Suzuki, A.; Jung, S.-M.; Hayashi, K.; Kinoshita, R.; Yang, Y.; Yuan, B.; Akhmetzhanov, A.R.; et al. Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19). Int. J. Infect. Dis. 2020, 94, 154–155. [Google Scholar] [CrossRef] [PubMed]
- Kimball, A.; Hatfield, K.M.; Arons, M.; James, A.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; Tanwar, S.; Chisty, Z. Asymptomatic and presymptomatic SARS-CoV-2 infections in residents of a long-term care skilled nursing facility—King County, Washington, March 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 377. [Google Scholar] [CrossRef] [Green Version]
- Moghadas, S.M.; Vilches, T.N.; Zhang, K.; Wells, C.R.; Shoukat, A.; Singer, B.H.; Meyers, L.A.; Neuzil, K.M.; Langley, J.M.; Fitzpatrick, M.C.; et al. The Impact of Vaccination on Coronavirus Disease 2019 (COVID-19) Outbreaks in the United States. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application. Ann. Intern. Med. 2020, 172, 577–582. [Google Scholar] [CrossRef] [Green Version]
- Team, C.C.-R.; Team, C.C.-R.; Team, C.C.-R.; Chow, N.; Fleming-Dutra, K.; Gierke, R.; Hall, A.; Hughes, M.; Pilishvili, T.; Ritchey, M. Preliminary estimates of the prevalence of selected underlying health conditions among patients with coronavirus disease 2019—United States, February 12–March 28, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 382–386. [Google Scholar]
- Garg, S.; Kim, L.; Whitaker, M.; O’Halloran, A.; Cummings, C.; Holstein, R.; Prill, M.; Chai, S.J.; Kirley, P.D.; Alden, N.B. Hospitalization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019—COVID-NET, 14 States, March 1–30, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 458. [Google Scholar] [CrossRef] [PubMed]
- Shoukat, A.; Wells, C.R.; Langley, J.M.; Singer, B.H.; Galvani, A.P.; Moghadas, S.M. Projecting demand for critical care beds during COVID-19 outbreaks in Canada. Cmaj 2020, 192, E489–E496. [Google Scholar] [CrossRef] [Green Version]
- Moghadas, S.M.; Shoukat, A.; Fitzpatrick, M.C.; Wells, C.R.; Sah, P.; Pandey, A.; Sachs, J.D.; Wang, Z.; Meyers, L.A.; Singer, B.H. Projecting hospital utilization during the COVID-19 outbreaks in the United States. Proc. Natl. Acad. Sci. USA 2020, 117, 9122–9126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.-C.; Cui, C.; Shin, K.-R.; Bae, J.-Y.; Kweon, O.-J.; Lee, M.-K.; Choi, S.-H.; Jung, S.-Y.; Park, M.-S.; Chung, J.-W. Duration of Culturable SARS-CoV-2 in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 671–673. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, T.; Lee, E.; Lee, C.; Kim, H.; Rhee, H.; Park, S.Y.; Son, H.-J.; Yu, S.; Park, J.W. Clinical course and molecular viral shedding among asymptomatic and symptomatic patients with SARS-CoV-2 infection in a community treatment center in the Republic of Korea. JAMA Intern. Med. 2020, 180, 1447–1452. [Google Scholar] [CrossRef]
- Novavax. Novavax Confirms High Levels of Efficacy Against Original and Variant COVID-19 Strains in United Kingdom and South Africa Trials. Available online: https://ir.novavax.com/news-releases/news-release-details/novavax-confirms-high-levels-efficacy-against-original-and-0 (accessed on 17 April 2021).
- Seo, J.-W.; Lim, S.-H.; Kim, Y.-J.; Lee, E.-J. COVID-19 treatment in Korea cost $57,562 per critically-ill, bill charged on state. Pulse, 8 May 2020. [Google Scholar]
- MOIS. Status of Resident Registration Population and Generation. Available online: https://jumin.mois.go.kr/index.jsp# (accessed on 17 April 2021).
- Matrajt, L.; Eaton, J.; Leung, T.; Dimitrov, D.; Schiffer, J.T.; Swan, D.A.; Janes, H. Optimizing vaccine allocation for COVID-19 vaccines: Critical role of single-dose vaccination. medRxiv 2021. [Google Scholar] [CrossRef]
- Lee, S.; Morales, R.; Castillo-Chavez, C. A note on the use of influenza vaccination strategies when supply is limited. Math. Biosci. Eng 2011, 8, 171–182. [Google Scholar]
- Lenhart, S.; Workman, J.T. Optimal Control Applied to Biological Models; CRC Press: Boca Raton, FL, USA, 2007. [Google Scholar]
- Buitrago-Garcia, D.; Egli-Gany, D.; Counotte, M.J.; Hossmann, S.; Imeri, H.; Ipekci, A.M.; Salanti, G.; Low, N. Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: A living systematic review and meta-analysis. PLoS Med. 2020, 17, e1003346. [Google Scholar] [CrossRef] [PubMed]
- Shim, E. Optimal strategies of social distancing and vaccination against seasonal influenza. Math. Biosci. Eng. 2013, 10, 1615–1634. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kwon, H.-D.; Lee, J. Constrained optimal control applied to vaccination for influenza. Comput. Math. Appl. 2016, 71, 2313–2329. [Google Scholar] [CrossRef] [PubMed]
- Prosper, O.; Saucedo, O.; Thompson, D.; Torres-Garcia, G.; Wang, X.; Castillo-Chavez, C. Modeling control strategies for concurrent epidemics of seasonal and pandemic H1N1 influenza. Math. Biosci. Eng. 2011, 8, 141. [Google Scholar]
- Hogan, A.; Winskill, P.; Watson, O.; Walker, P.; Whittaker, C.; Baguelin, M.; Haw, D.; Lochen, A.; Gaythorpe, K.; Ainslie, K. Report 33: Modelling the Allocation and Impact of a COVID-19 Vaccine. 2020. Available online: http://hdl.handle.net/10044/1/82822 (accessed on 17 April 2021).
- Foy, B.H.; Wahl, B.; Mehta, K.; Shet, A.; Menon, G.I.; Britto, C. Comparing COVID-19 vaccine allocation strategies in India: A mathematical modelling study. Int. J. Infect. Dis. 2021, 103, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Cartocci, A.; Cevenini, G.; Barbini, P. A compartment modeling approach to reconstruct and analyze gender and age-grouped CoViD-19 Italian data for decision-making strategies. J. Biomed. Inform. 2021, 118, 103793. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Confirmed Cases | ||
|---|---|---|
| Total | 112,789 | |
| Age Group | ≥70 | 13,257 |
| 60–69 | 17,431 | |
| 50–59 | 20,887 | |
| 40–49 | 16,586 | |
| 30–39 | 15,161 | |
| 20–29 | 16,817 | |
| 10–19 | 7813 | |
| 0–9 | 4837 | |
| Parameter | Description | Value | References |
|---|---|---|---|
| Basic reproduction number | 1.3 | ||
| Transmission probability | - | Estimated from | |
| Age-specific susceptibility | [0.26; 0.15; 0.3; 0.24; 0.22; 0.29; 0.66; 0.8] | Fitted | |
| Number of age- individuals contacted by an age- individual per day | Table S1 | [31] | |
| Age-specific proportion of symptomatic infection | [0.66; 0.62; 0.67; 0.67; 0.67; 0.67; 0.75; 0.81] | [32,33,34,35] | |
| Latent period (day) | 3.1 | [36] | |
| Relative infectiousness of asymptomatic individuals compared with symptomatic individuals | 0.75 | [26,30] | |
| Age-specific hospitalization ratio of symptomatic individuals (%) | [0.23; 0.33; 0.76; 0.76; 0.76; 3.13; 5.64; 8.14] | [35,37,38,39,40] | |
| Average duration from diagnosis to hospitalization because of severe symptoms (day) | 7 | [2] | |
| Infectious period of asymptomatic infections (day) | 7 | [41,42] | |
| Infectious period of symptomatic infections (day) | 7 | [41,42] | |
| Time spent in hospital (day) | 22 | [2] | |
| Vaccine efficacy in reducing the probability that the infection progresses to severe or critical disease | 0.90 | [9,10,12,43] | |
| Upper bound of daily vaccination rate | 0.015 | Assumption | |
| Cost of vaccination for COVID-19 (USD *) | 35 | [2] | |
| Daily cost of treatment for mild infections (USD *) | 197 | [44] | |
| Daily cost of treatment during hospitalization (USD *) | 583 | [44] | |
| Proportion of people in age group ( |
= 0.08,
= 0.10, = 0.13, = 0.14, = 0.16, = 0.17, = 0.12, = 0.10. | [45] |
| Vaccine Efficacy Scenarios | Vaccine 1 | Vaccine 2 | Vaccine 3 | Vaccine 4 | Vaccine 5 | Vaccine 6 |
|---|---|---|---|---|---|---|
| Reduction in susceptibility () | 0.70 | 0.40 | 0.00 | 0.95 | 0.50 | 0.00 |
| Reduction in the probability of disease progression to symptomatic disease () | 0.00 | 0.50 | 0.70 | 0.00 | 0.90 | 0.95 |
|
Direct impact of reduction in the number of symptomatic infections () | 0.70 | 0.95 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, W.; Shim, E. Vaccine Effects on Susceptibility and Symptomatology Can Change the Optimal Allocation of COVID-19 Vaccines: South Korea as an Example. J. Clin. Med. 2021, 10, 2813. https://doi.org/10.3390/jcm10132813
Choi W, Shim E. Vaccine Effects on Susceptibility and Symptomatology Can Change the Optimal Allocation of COVID-19 Vaccines: South Korea as an Example. Journal of Clinical Medicine. 2021; 10(13):2813. https://doi.org/10.3390/jcm10132813
Chicago/Turabian StyleChoi, Wongyeong, and Eunha Shim. 2021. "Vaccine Effects on Susceptibility and Symptomatology Can Change the Optimal Allocation of COVID-19 Vaccines: South Korea as an Example" Journal of Clinical Medicine 10, no. 13: 2813. https://doi.org/10.3390/jcm10132813