
Differentiation of Idiopathic Pulmonary Fibrosis from Connective Tissue Disease-Related Interstitial Lung Disease Using Quantitative Imaging

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Clinical Data
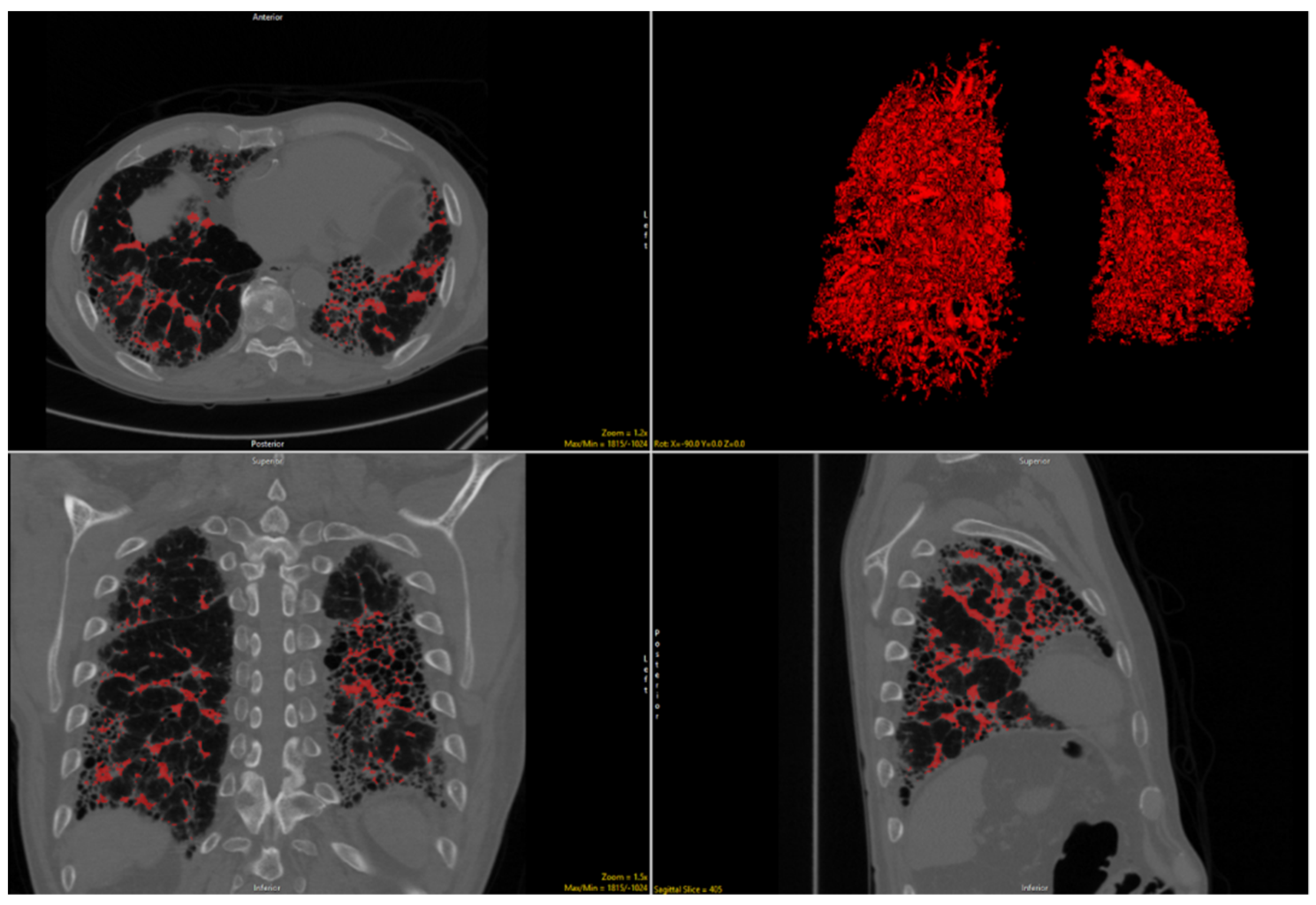
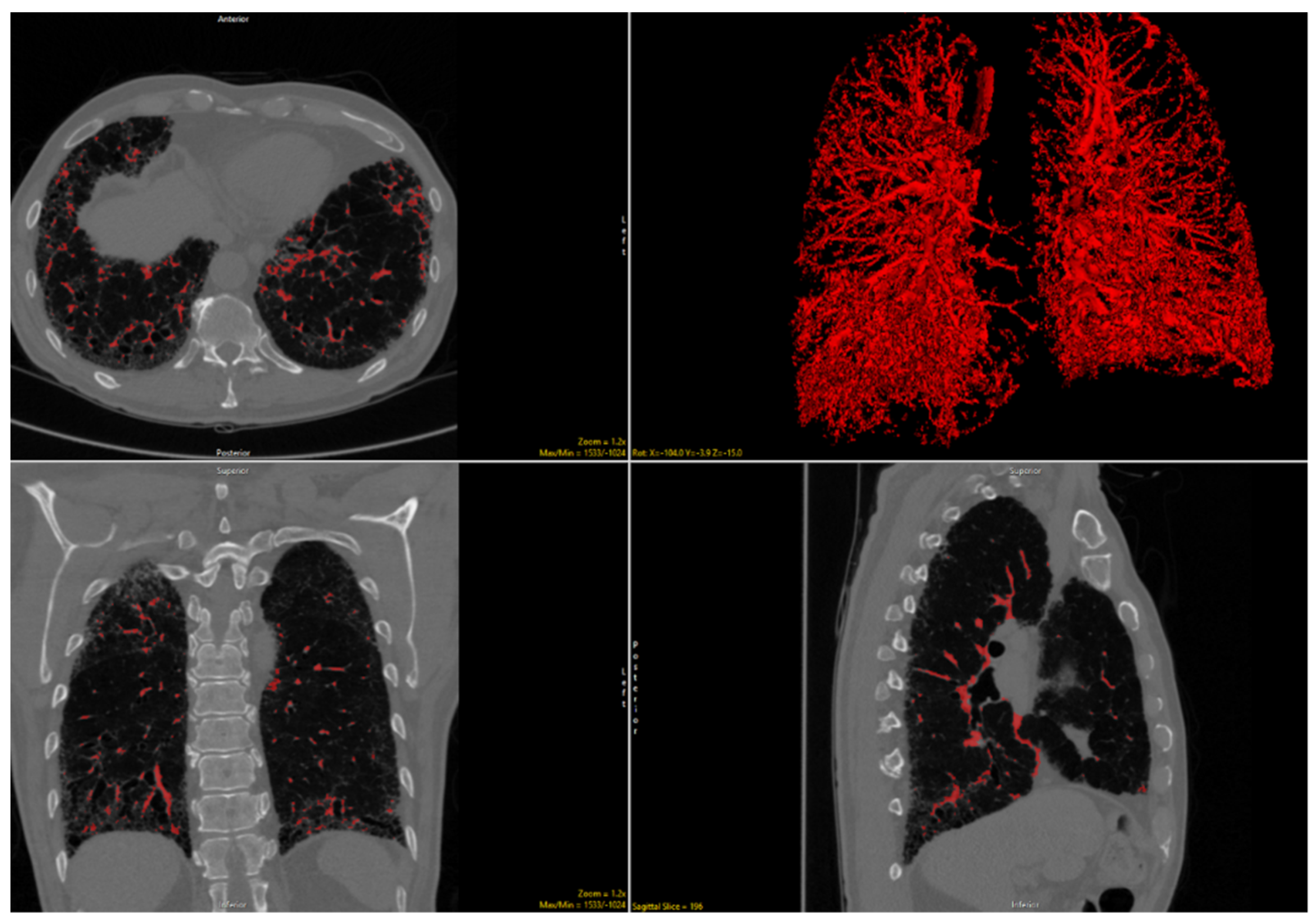
2.2. Imaging Analysis
2.3. Statistical Analysis
3. Results
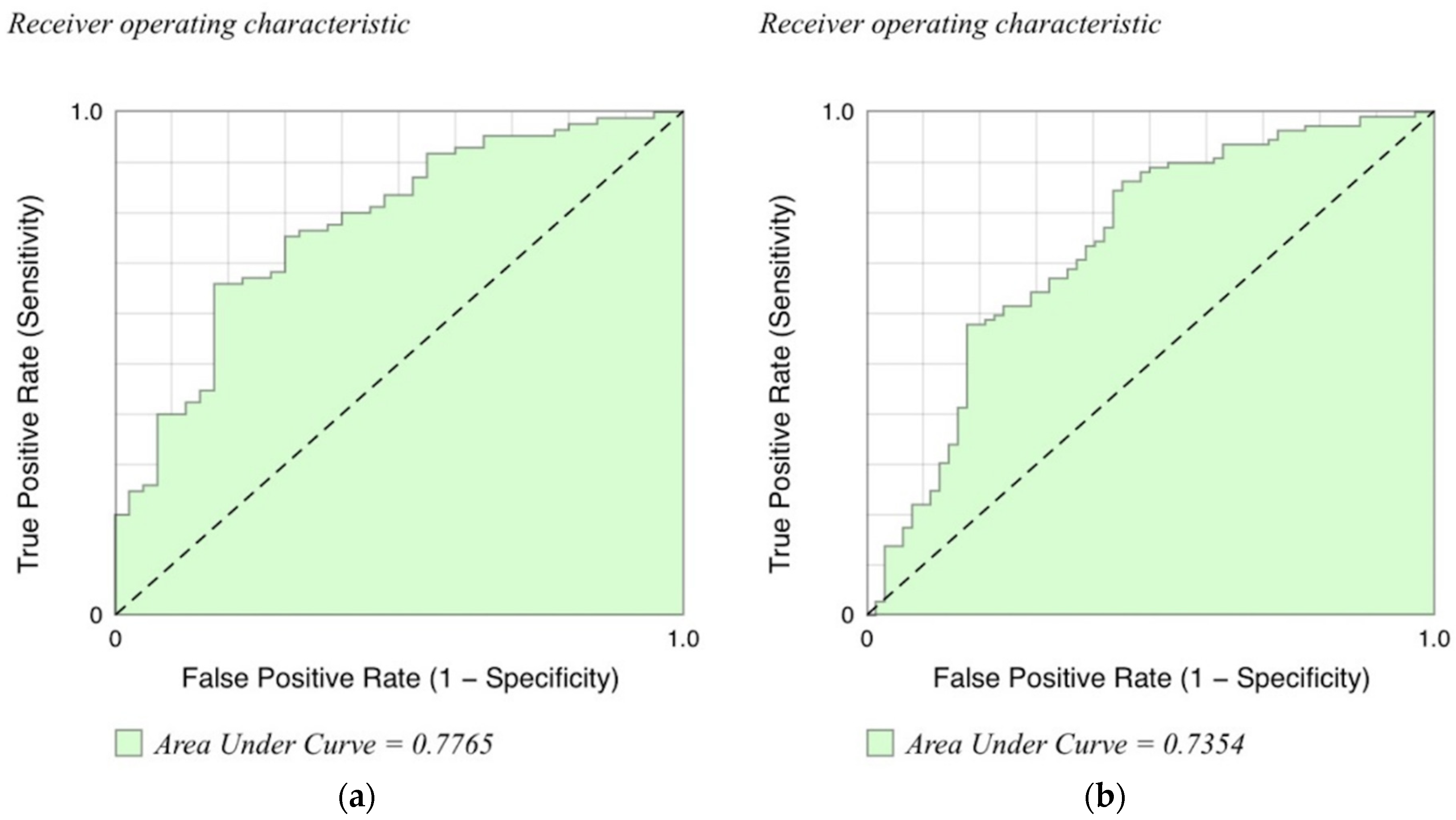
3.1. CALIPER Diagnostic Analysis
3.1.1. Univariate Analysis
3.1.2. Multivariable Analysis
3.2. CALIPER Functional Analysis
3.2.1. Univariate Analysis
3.2.2. Multivariable Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| CALIPER | Computer-Aided Lung Informatics for Pathology Evaluation and Rating |
| CTD-ILD | connective tissue disease-related interstitial lung disease |
| DLCO | diffusion capacity of the lung for carbon monoxide |
| DLCO% | percent predicted diffusing capacity of the lungs for carbon monoxide |
| FVC | forced vital capacity |
| FVC% | percent predicted forced vital capacity |
| IPF | idiopathic pulmonary fibrosis |
| TLC | total lung capacity |
| UIP | usual interstitial pneumonitis |
| VRS | vessel-related structure |
References
- Richeldi, L.; Du Bois, R.M.; Raghu, G.; Azuma, A.; Brown, K.K.; Costabel, U.; Cottin, V.; Flaherty, K.R.; Hansell, D.M.; Inoue, Y.; et al. Efficacy and Safety of Nintedanib in Idiopathic Pulmonary Fibrosis. N. Engl. J. Med. 2014, 370, 2071–2082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, T.E.; Bradford, W.Z.; Castro-Bernardini, S.; Fagan, E.A.; Glaspole, I.; Glassberg, M.K.; Gorina, E.; Hopkins, P.M.; Kardatzke, D.; Lancaster, L.; et al. A Phase 3 Trial of Pirfenidone in Patients with Idiopathic Pulmonary Fibrosis. N. Engl. J. Med. 2014, 370, 2083–2092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Idiopathic Pulmonary Fibrosis Clinical Research Network; Raghu, G.; Anstrom, K.J.; King, T.E., Jr.; Lasky, J.A.; Martinez, F.J. Prednisone, azathioprine, and N-acetylcysteine for pulmonary fibrosis. N. Engl. J. Med. 2012, 366, 1968–1977. [Google Scholar] [PubMed]
- Kim, E.J.; Collard, H.R.; King, T.E. Rheumatoid Arthritis-Associated Interstitial Lung Disease: The Relevance of Histopathologic and Radiographic Pattern. Chest 2009, 136, 1397–1405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, N.; Kim, J.S.; Newell, J.D.; Brown, K.K.; Cool, C.D.; Meehan, R.; Emoto, T.; Matsumoto, T.; Lynch, D.A. Rheumatoid Arthritis–related Lung Diseases: CT Findings. Radiology 2004, 232, 81–91. [Google Scholar] [CrossRef]
- Chung, J.H.; Cox, C.W.; Montner, S.M.; Adegunsoye, A.; Oldham, J.M.; Husain, A.N.; Vij, R.; Noth, I.; Lynch, D.A.; Strek, M.E. CT Features of the Usual Interstitial Pneumonia Pattern: Differentiating Con-nective Tissue Disease-Associated Interstitial Lung Disease from Idiopathic Pulmonary Fibrosis. Am. J. Roentgenol. 2018, 210, 307–313. [Google Scholar] [CrossRef]
- Walkoff, L.; White, D.B.; Chung, J.H.; Asante, D.; Cox, C.W. The Four Corners Sign: A Specific Imaging Feature in Differen-tiating Systemic Sclerosis-related Interstitial Lung Disease from Idiopathic Pulmonary Fibrosis. J. Thorac. Imaging 2018, 33, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Zhan, X.; Koelsch, T.; Montner, S.M.; Zhu, A.; Vij, R.; Swigris, J.J.; Chung, J.H. Differentiating Usual Interstitial Pneumonia from Nonspecific Interstitial Pneumonia Using High-resolution Computed Tomography: The “Straight-edge Sign”. J. Thorac. Imaging 2018, 33, 266–270. [Google Scholar] [CrossRef]
- Watadani, T.; Sakai, F.; Johkoh, T.; Noma, S.; Akira, M.; Fujimoto, K.; Bankier, A.A.; Lee, K.S.; Müller, N.L.; Song, J.-W.; et al. Interobserver Variability in the CT Assessment of Honeycombing in the Lungs. Radiology 2013, 266, 936–944. [Google Scholar] [CrossRef] [PubMed]
- Walsh, S.L.F.; Calandriello, L.; Sverzellati, N.; Wells, A.U.; Hansell, D.M. Interobserver agreement for the ATS/ERS/JRS/ALAT criteria for a UIP pattern on CT. Thorax 2015, 71, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Thomeer, M.; Demedts, M.; Behr, J.; Buhl, R.; Costabel, U.; Flower, C.D.R.; Verschakelen, J.; Laurent, F.; Nicholson, A.G.; Verbeken, E.K.; et al. Multidisciplinary interobserver agreement in the diagnosis of idiopathic pulmonary fibrosis. Eur. Respir. J. 2008, 31, 585–591. [Google Scholar] [CrossRef] [Green Version]
- Jacob, J.; Bartholmai, B.J.; Rajagopalan, S.; Egashira, R.; Brun, A.L.; Kokosi, M.; Nair, A.; Walsh, S.L.; Karwoski, R.; Nicholson, A.G.; et al. Unclassifiable-interstitial lung disease: Outcome prediction using CT and functional indices. Respir. Med. 2017, 130, 43–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob, J.; Bartholmai, B.J.; Brun, A.L.; Egashira, R.; Rajagopalan, S.; Karwoski, R.; Kouranos, V.; Kokosi, M.; Hansell, D.M.; Wells, A.U. Evaluation of visual and computer-based CT analysis for the identification of functional patterns of obstruction and restriction in hypersensitivity pneumonitis. Respirology 2017, 22, 1585–1591. [Google Scholar] [CrossRef] [PubMed]
- Jacob, J.; Bartholmai, B.J.; Rajagopalan, S.; Kokosi, M.; Nair, A.; Karwoski, R.; Raghunath, S.M.; Walsh, S.L.F.; Wells, A.U.; Hansell, D.M. Automated Quantitative Computed Tomography Versus Visual Computed Tomography Scoring in Idiopathic Pulmonary Fibrosis: Validation Against Pulmonary Function. J. Thorac. Imaging 2016, 31, 304–311. [Google Scholar] [CrossRef] [Green Version]
- Jacob, J.; Bartholmai, B.J.; Rajagopalan, S.; Kokosi, M.; Egashira, R.; Brun, A.L.; Nair, A.; Walsh, S.L.F.; Karwoski, R.; Wells, A.U. Serial automated quantitative CT analysis in idiopathic pulmonary fibrosis: Functional correlations and comparison with changes in visual CT scores. Eur. Radiol. 2018, 28, 1318–1327. [Google Scholar] [CrossRef] [PubMed]
- Jacob, J.; Bartholmai, B.J.; Rajagopalan, S.; Kokosi, M.; Nair, A.; Karwoski, R.; Walsh, S.L.F.; Wells, A.U.; Hansell, D.M. Mortality prediction in idiopathic pulmonary fibrosis: Evaluation of comput-er-based CT analysis with conventional severity measures. Eur. Respir. J. 2017, 49, 1601011. [Google Scholar] [CrossRef] [Green Version]
- Jacob, J.; Bartholmai, B.J.; Rajagopalan, S.; van Moorsel, C.H.M.; van Es, H.W.; van Beek, F.T.; Struik, M.H.L.; Kokosi, M.; Egashira, R.; Brun, A.L.; et al. Predicting Outcomes in Idiopathic Pulmonary Fibrosis Using Automated CT Analysis. Am. J. Respir. Crit. Care Med. 2018, 198, 767–776. [Google Scholar] [CrossRef]
- Jacob, J.; Bartholmai, B.; Rajagopalan, S.; Brun, A.L.; Egashira, R.; Karwoski, R.; Kokosi, M.; Wells, A.U.; Hansell, D.M. Evaluation of computer-based computer tomography stratification against outcome models in connective tissue disease-related interstitial lung disease: A patient outcome study. BMC Med. 2016, 14, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Jacob, J.; Bartholmai, B.J.; Egashira, R.; Brun, A.L.; Rajagopalan, S.; Karwoski, R.; Kokosi, M.; Hansell, D.M.; Wells, A.U. Chronic hypersensitivity pneumonitis: Identification of key prognostic determi-nants using automated CT analysis. BMC Pulm. Med. 2017, 17, 81. [Google Scholar] [CrossRef]
- Moua, T.; Martinez, A.C.Z.; Baqir, M.; Vassallo, R.; Limper, A.H.; Ryu, J.H. Predictors of diagnosis and survival in idiopathic pulmonary fibrosis and connective tissue disease-related usual interstitial pneumonia. Respir. Res. 2014, 15, 154. [Google Scholar] [CrossRef] [Green Version]
- Navaratnam, V.; Ali, N.; Smith, C.; McKeever, T.; Fogarty, A.; Hubbard, R. Does the presence of connective tissue disease modify survival in patients with pulmonary fibrosis? Respir. Med. 2011, 105, 1925–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.H.; Kim, D.S.; Park, I.N.; Jang, S.J.; Kitaichi, M.; Nicholson, A.G.; Colby, T.V. Prognosis of fibrotic interstitial pneumonia: Idiopathic versus collagen vascular dis-ease-related subtypes. Am. J. Respir. Crit. Care Med. 2007, 175, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Aziz, Z.; Wells, A.U.; Hansell, D.M.; Bain, G.A.; Copley, S.J.; Desai, S.R.; Ellis, S.M.; Gleeson, F.V.; Grubnic, S.; Nicholson, A.G.; et al. HRCT diagnosis of diffuse parenchymal lung disease: Inter-observer variation. Thorax 2004, 59, 506–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peão, M.N.D.; Águas, A.P.; de Sá, C.M.; Grande, N.R. Neoformation of blood vessels in association with rat lung fibrosis induced by bleomycin. Anat. Rec. 1994, 238, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Kwon, K.Y.; Park, K.K.; Chang, E.S. Scanning electron microscopic study of capillary change in bleomycin-induced pulmonary fibrosis. J. Korean Med. Sci. 1991, 6, 234–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosgrove, G.P.; Brown, K.K.; Schiemann, W.P.; Serls, A.E.; Parr, J.E.; Geraci, M.W.; Schwarz, M.I.; Cool, C.D.; Worthen, G.S. Pigment epithelium-derived factor in idiopathic pulmonary fibrosis: A role in aberrant angiogenesis. Am. J. Respir. Crit. Care Med. 2004, 170, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; King, C.S.; Puri, N.; Shlobin, O.A.; Brown, A.W.; Ahmad, S.; Weir, N.A.; Nathan, S.D. Pulmonary artery size as a predictor of outcomes in idiopathic pulmonary fibrosis. Eur. Respir. J. 2016, 47, 1445–1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhamad, E.H.; Al-Boukai, A.A.; Al-Kassimi, F.A.; AlFaleh, H.F.; Alshamiri, M.Q.; Alzeer, A.H.; Al-Otair, H.A.; Ibrahim, G.F.; Shaik, S.A. Prediction of Pulmonary Hypertension in Patients with or without Interstitial Lung Disease: Reliability of CT Findings. Radiology 2011, 260, 875–883. [Google Scholar] [CrossRef]
- Edwards, P.D.; Bull, R.K.; Coulden, R. CT measurement of main pulmonary artery diameter. Br. J. Radiol. 1998, 71, 1018–1020. [Google Scholar] [CrossRef]
- A Lynch, D.; Sverzellati, N.; Travis, W.D.; Brown, K.K.; Colby, T.V.; Galvin, J.R.; Goldin, J.G.; Hansell, D.M.; Inoue, Y.; Johkoh, T.; et al. Diagnostic criteria for idiopathic pulmonary fibrosis: A Fleischner Society White Paper. Lancet Respir. Med. 2018, 6, 138–153. [Google Scholar] [CrossRef]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef]
- Chung, J.H.; Montner, S.M.; Adegunsoye, A.; Oldham, J.M.; Husain, A.N.; Vij, R.; Noth, I.; Strek, M.E. CT findings associated with survival in chronic hypersensitivity pneu-monitis. Eur. Radiol. 2017, 27, 5127–5135. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.I.S.; Müller, N.L.; Lynch, D.A.; Curran-Everett, D.; Brown, K.K.; Lee, K.S.; Chung, M.P.; Churg, A. Chronic Hypersensitivity Pneumonitis: Differentiation from Idiopathic Pulmonary Fibrosis and Nonspecific Interstitial Pneumonia by Using Thin-Section CT. Radiology 2008, 246, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Clukers, J.; Lanclus, M.; Mignot, B.; Van Holsbeke, C.; Roseman, J.; Porter, S.; Gorina, E.; Kouchakji, E.; Lipson, K.E.; De Backer, W.; et al. Quantitative CT analysis using functional imaging is superior in describing disease progression in idiopathic pulmonary fibrosis compared to forced vital capacity. Respir. Res. 2018, 19, 213. [Google Scholar] [CrossRef] [PubMed]
- Humphries, S.M.; Yagihashi, K.; Huckleberry, J.; Rho, B.-H.; Schroeder, J.D.; Strand, M.; Schwarz, M.I.; Flaherty, K.R.; Kazerooni, E.A.; Van Beek, E.J.R.; et al. Idiopathic Pulmonary Fibrosis: Data-driven Textural Analysis of Extent of Fibrosis at Baseline and 15-Month Follow-up. Radiology 2017, 285, 270–278. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | CTD-ILD (n = 40) Derivation | IPF (n = 85) Derivation | p-Value Derivation | CTD-ILD (n = 62) Validation | IPF (n = 109) Validation | p-Value Validation | |
|---|---|---|---|---|---|---|---|
| Mean years of age | 56.9 (15.7) | 70.4 (8.0) | <0.001 | 61.9 (13.0) | 69.5 (8.3) | <0.001 | |
| Sex | Female | 80.0% | 20.0% | <0.001 | 70.0% | 10.0% | <0.001 |
| Male | 20.0% | 80.0% | 30.0% | 90.0% | |||
| Race | White | 65.0% | 84.7% | <0.001 | 56.5% | 85.3% | <0.001 |
| Black | 27.5% | 2.4% | 25.8% | 4.6% | |||
| Asian | 7.5% | 5.9% | 8.1% | 7.3% | |||
| Other | 0.0% | 7.0% | 6.5% | 2.8% | |||
| Median pack-years smoking | 21 (20.5) | 20 (24) | <0.001 | 0 (22) | 20 (28) | <0.001 | |
| Mean % predicted FVC | 61.5 (15.9) | 62.1 (16.2) | 0.847 | 63.5 (15.3) | 64.1 (18.0) | 0.814 | |
| Mean % predicted DLCO | 40.7 (15.6) | 39.7 (14.2) | 0.742 | 45.0 (20.3) | 43.9 (17.8) | 0.709 | |
| Variable | CTD-ILD Derivation (n = 40) | IPF Derivation (n = 85) | p-Value Derivation | CTD-ILD Validation (n = 62) | IPF Validation (n = 109) | p-Value Validation |
|---|---|---|---|---|---|---|
| Total honeycombing, median (±IQR) | 0.5 (1.3) | 2.4 (8.1) | <0.001 | 3.6 (14.3) | 7.4 (17.8) | 0.087 |
| Total reticulation, median (±IQR) | 163.7 (185.8) | 193.6 (153.5) | 0.032 | 116.9 (106.5) | 169.3 (106.5) | 0.003 |
| Total ground-glass opacity, median (±IQR) | 769.5 (649.7) | 790.8 (724.9) | 0.501 | 381.0 (550.7) | 614.2 (660.9) | <0.001 |
| Total VRS, median (±IQR) | 114.6 (59.8) | 174.7 (84.9) | <0.001 | 142.7 (86.5) | 211.3 (78.4) | <0.001 |
| Total normal, median (±IQR) | 1527.9 (975.5) | 1487.8 (923.2) | 0.882 | 1411.8 (814.2) | 1764.6 (940.6) | 0.005 |
| Variable | OR Derivation | 95% CI Derivation | p-Value Derivation | OR Validation | 95% CI Validation | p-Value Validation |
|---|---|---|---|---|---|---|
| Total honeycombing | 0.995 | 0.972–1.019 | 0.687 | 1.000 | 0.996–1.004 | 0.954 |
| Total reticulation | 1.002 | 0.998–1.005 | 0.327 | 1.003 | 0.999–1.006 | 0.185 |
| Total ground-glass opacity | 0.999 | 0.997–1.000 | 0.018 | 1.000 | 0.999–1.002 | 0.379 |
| Total VRS | 1.026 | 1.014–1.037 | <0.001 | 1.008 | 1.000–1.017 | 0.047 |
| Total normal | 1.000 | 0.999–1.000 | 0.365 | 1.001 | 1.000–1.001 | 0.009 |
| Constant | 1.000 | 0.999–1.000 | 0.365 | 0.048 | 0.011–0.208 | <0.001 |
| Variable | Correlation Coefficient Derivation | SD Derivation | p-Value Derivation | Correlation Coefficient Validation | SD Validation | p-Value Validation |
|---|---|---|---|---|---|---|
| FVC: | ||||||
| Total honeycombing | 0.132 | 0.047 | 0.006 | 0.003 | 0.016 | 0.873 |
| Total reticulation | −0.027 | 0.009 | 0.003 | −0.028 | 0.012 | 0.017 |
| Total ground-glass opacity | 0.001 | 0.003 | 0.736 | −0.008 | 0.004 | 0.039 |
| Total VRS | −0.043 | 0.025 | 0.088 | −0.005 | 0.028 | 0.859 |
| Total normal lung | 0.008 | 0.002 | <0.001 | 0.006 | 0.002 | 0.009 |
| constant | 60.039 | 5.237 | 0.000 | 66.125 | 4.644 | <0.001 |
| DLCO: | ||||||
| Total honeycombing | 0.020 | 0.045 | 0.659 | −0.014 | 0.017 | 0.395 |
| Total reticulation | −0.007 | 0.012 | 0.539 | −0.017 | 0.012 | 0.176 |
| Total ground-glass opacity | −0.001 | 0.003 | 0.786 | −0.007 | 0.004 | 0.079 |
| Total VRS | −0.079 | 0.026 | 0.003 | −0.048 | 0.029 | 0.098 |
| Total normal lung | 0.006 | 0.002 | 0.003 | 0.009 | 0.002 | <0.001 |
| constant | 45.435 | 5.125 | <0.001 | 48.161 | 4.845 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, J.H.; Adegunsoye, A.; Cannon, B.; Vij, R.; Oldham, J.M.; King, C.; Montner, S.M.; Thirkateh, P.; Barnett, S.; Karwoski, R.; et al. Differentiation of Idiopathic Pulmonary Fibrosis from Connective Tissue Disease-Related Interstitial Lung Disease Using Quantitative Imaging. J. Clin. Med. 2021, 10, 2663. https://doi.org/10.3390/jcm10122663
Chung JH, Adegunsoye A, Cannon B, Vij R, Oldham JM, King C, Montner SM, Thirkateh P, Barnett S, Karwoski R, et al. Differentiation of Idiopathic Pulmonary Fibrosis from Connective Tissue Disease-Related Interstitial Lung Disease Using Quantitative Imaging. Journal of Clinical Medicine. 2021; 10(12):2663. https://doi.org/10.3390/jcm10122663
Chicago/Turabian StyleChung, Jonathan H., Ayodeji Adegunsoye, Brenna Cannon, Rekha Vij, Justin M. Oldham, Christopher King, Steven M. Montner, Prahasit Thirkateh, Scott Barnett, Ronald Karwoski, and et al. 2021. "Differentiation of Idiopathic Pulmonary Fibrosis from Connective Tissue Disease-Related Interstitial Lung Disease Using Quantitative Imaging" Journal of Clinical Medicine 10, no. 12: 2663. https://doi.org/10.3390/jcm10122663