
Risk Factors of Patient-Related Safety Events during Active Mobilization for Intubated Patients in Intensive Care Units—A Multi-Center Retrospective Observational Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
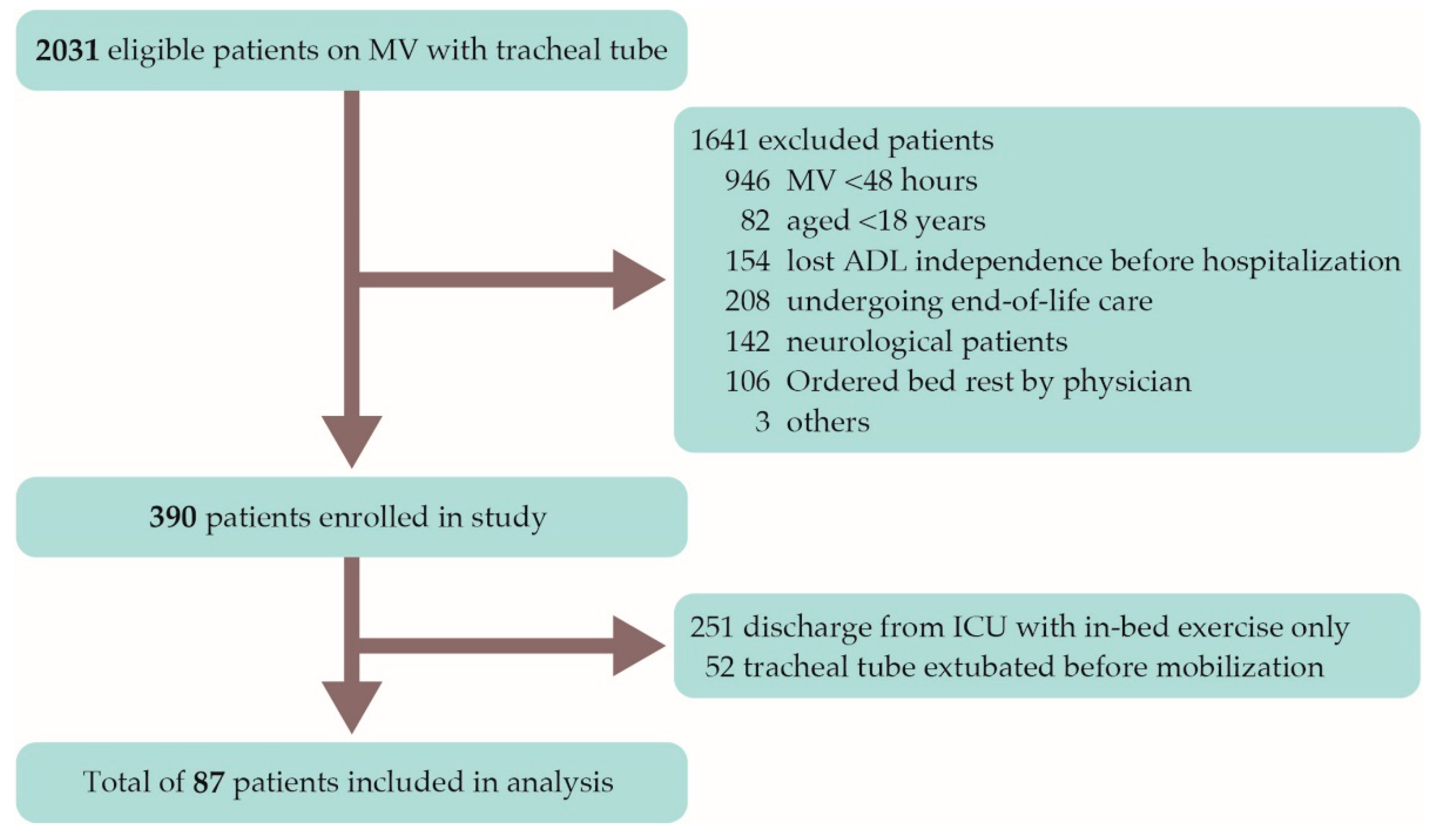
2.2. Patient Population
2.3. Study Outcomes
2.4. Definition of Patient-Related Safety Events
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Needham, D.M.; Davidson, J.; Cohen, H.; Hopkins, R.O.; Weinert, C.; Wunsch, H.; Zawistowski, C.; Bemis-Dougherty, A.; Berney, S.C.; Bienvenu, O.J.; et al. Improving long-term outcomes after discharge from intensive care unit: Report from a stakeholders’ conference. Crit. Care Med. 2012, 40, 502–509. [Google Scholar] [CrossRef]
- Morris, P.E.; Goad, A.; Thompson, C.; Taylor, K.; Harry, B.; Passmore, L.; Ross, A.; Anderson, L.; Baker, S.; Sanchez, M.; et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit. Care Med. 2008, 36, 2238–2243. [Google Scholar] [CrossRef] [Green Version]
- Schweickert, W.D.; Pohlman, M.C.; Pohlman, A.S.; Nigos, C.; Pawlik, A.J.; Esbrook, C.L.; Spears, L.; Miller, M.; Franczyk, M.; Deprizio, D.; et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: A randomised controlled trial. Lancet 2009, 30, 1874–1882. [Google Scholar] [CrossRef]
- Dantas, C.M.; Silva, P.F.; Siqueira, F.H.; Pinto, R.M.; Matias, S.; Maciel, C.; Oliveira, M.C.; Albuquerque, C.G.; Andrade, F.M.; Ramos, F.F.; et al. Influence of early mobilization on respiratory and peripheral muscle strength in critically ill patients. Rev. Bras. Ter. Intensiva 2012, 24, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.H.; Yu, B.X.; Sun, Y.B.; Fang, W.; Li, L. Effects of early rehabilitation therapy on patients with mechanical ventilation. World J. Emerg. Med. 2014, 5, 48–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaller, S.J.; Anstey, M.; Blobner, M.; Edrich, T.; Grabitz, S.D.; Gradwohl-Matis, I.; Heim, M.; Houle, T.; Kurth, T.; Latronico, N.; et al. Early, goal-directed mobilisation in the surgical intensive care unit: A randomised controlled trial. Lancet 2016, 388, 1377–1388. [Google Scholar] [CrossRef]
- Liu, K.; Ogura, T.; Takahashi, K.; Nakamura, M.; Ohtake, H.; Fujiduka, K.; Abe, E.; Oosaki, H.; Miyazaki, D.; Suzuki, H.; et al. A progressive early mobilization program is significantly associated with clinical and economic improvement: A single-center quality comparison study. Crit. Care Med. 2019, 47, e744–e752. [Google Scholar] [CrossRef]
- Schujmann, D.S.; Gomes, T.T.; Lunardi, A.C.; Lamano, M.Z.; Fragoso, A.; Pimentel, M.; Peso, C.N.; Araujo, P.; Fu, C. Impact of a progressive mobility program on the functional status, respiratory, and muscular systems of ICU patients: A randomized and controlled trial. Crit. Care Med. 2020, 48, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Nydahl, P.; Sricharoenchai, T.; Chandra, S.; Kundt, F.S.; Huang, M.; Fischill, M.; Needham, D.M. Safety of patient mobilization and rehabilitation in the Intensive Care Unit. Systematic Review with Meta-Analysis. Ann. Am. Thorac. Soc. 2017, 14, 766–777. [Google Scholar] [CrossRef]
- Costa, D.K.; Valley, T.S.; Miller, M.A.; Manojlovich, M.; Watson, S.R.; McLellan, P.; Pope, C.; Hyzy, R.C.; Iwashyna, T.J. ICU team composition and its association with ABCDE implementation in a quality collaborative. J. Crit. Care 2018, 44, 1–6. [Google Scholar] [CrossRef]
- Anekwe, D.E.; Koo, K.K.; Marchie, M.D.; Goldberg, P.; Jayaraman, D.; Spahija, J. Interprofessional survey of perceived barriers and facilitators to early mobilization of critically ill patients in Montreal, Canada. J. Intensive Care Med. 2019, 34, 218–226. [Google Scholar] [CrossRef]
- Sakai, T.; Hoshino, C.; Okawa, A.; Wakabayashi, K.; Shigemitsu, H. The safety and effect of early mobilization in the Intensive Care Unit according to cancellation criteria. Prog. Rehabil. Med. 2020, 5, 20200016. [Google Scholar] [CrossRef]
- Stiller, K.; Phillips, A.C.; Lambert, P. The safety of mobilisation and its effect on haemodynamic and respiratory status of intensive care patients. Physiother. Theory Pract. 2004, 20, 175–185. [Google Scholar] [CrossRef]
- Burtin, C.; Clerckx, B.; Robbeets, C.; Ferdinande, P.; Langer, D.; Troosters, T.; Hermans, G.; Decramer, M.; Gosselink, R. Early exercise in critically ill patients enhances short-term functional recovery. Crit. Care Med. 2009, 37, 2499–2505. [Google Scholar] [CrossRef]
- Zanni, J.M.; Korupolu, R.; Fan, E.; Pradhan, P.; Janjua, K.; Palmer, J.B.; Brower, R.G.; Needham, D.M. Rehabilitation therapy and outcomes in acute respiratory failure: An observational pilot project. J. Crit. Care 2010, 25, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Pohlman, M.C.; Schweickert, W.D.; Pohlman, A.S.; Nigos, C.; Pawlik, A.J.; Esbrook, C.L.; Spears, L.; Miller, M.; Franczyk, M.; Deprizio, D.; et al. Feasibility of physical and occupational therapy beginning from initiation of mechanical ventilation. Crit. Care Med. 2010, 38, 2089–2094. [Google Scholar] [CrossRef] [PubMed]
- Damluji, A.; Zanni, J.M.; Mantheiy, E.; Colantuoni, E.; Kho, M.E.; Needham, D.M. Safety and feasibility of femoral catheters during physical rehabilitation in the intensive care unit. J. Crit. Care 2013, 28, e9–e15. [Google Scholar] [CrossRef]
- Sricharoenchai, T.; Parker, A.M.; Zanni, J.M.; Nelliot, A.; Dinglas, V.D.; Needham, D.M. Safety of physical therapy interventions in critically ill patients: A single-center prospective evaluation of 1110 intensive care unit admissions. J. Crit. Care 2014, 29, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Morris, P.E.; Berry, M.J.; Files, D.C.; Thompson, J.C.; Hauser, J.; Flores, L.; Dhar, S.; Chmelo, E.; Lovato, J.; Case, L.D.; et al. Standardized rehabilitation and hospital length of stay among patients with acute respiratory failure: A randomized clinical trial. JAMA 2016, 315, 2694–2702. [Google Scholar] [CrossRef]
- Wright, S.E.; Thomas, K.; Watson, G.; Baker, C.; Bryant, A.; Chadwick, T.J.; Shen, J.; Wood, R.; Wilkinson, J.; Mansfield, L.; et al. Intensive versus standard physical rehabilitation therapy in the critically ill (EPICC): A multicentre, parallel-group, randomised controlled trial. Thorax 2018, 73, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Eggmann, S.; Verra, M.L.; Luder, G.; Takala, J.; Jakob, S.M. Effects of early, combined endurance and resistance training in mechanically ventilated, critically ill patients: A randomised controlled trial. PLoS ONE. 2018, 13, e0207428. [Google Scholar] [CrossRef] [Green Version]
- Seo, Y.J.; Park, S.R.; Lee, J.H.; Jung, C.; Choi, K.H.; Hong, S.K.; Kim, W. Feasibility, safety, and functional recovery after active rehabilitation in critically ill surgical patients. Aust. Crit. Care 2020, 33, 281–286. [Google Scholar] [CrossRef]
- Watanabe, S.; Kotani, T.; Taito, S.; Ota, K.; Ishii, K.; Ono, M.; Katsukawa, H.; Kozu, R.; Morita, Y.; Arakawa, R.; et al. Determinants of gait independence after mechanical ventilation in the intensive care unit: A Japanese multicenter retrospective exploratory cohort study. J. Intensive Care 2019, 7, 53. [Google Scholar] [CrossRef]
- Lee, H.; Ko, Y.J.; Suh, G.Y.; Yang, J.H.; Park, C.M.; Jeon, K.; Park, Y.H.; Chung, C.R. Safety profile and feasibility of early physical therapy and mobility for critically ill patients in the medical intensive care unit: Beginning experiences in Korea. J. Crit. Care 2015, 30, 673–677. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Alaparthi, G.K.; Gatty, A.; Samuel, S.R.; Amaravadi, S.K. Effectiveness, safety, and barriers to early mobilization in the Intensive Care Unit. Crit. Care Res. Pract. 2020, 2020, 7840743. [Google Scholar]
- Rebel, A.; Marzano, V.; Green, M.; Johnston, K.; Wang, J.; Neeman, T.; Mitchell, I.; Bissett, B. Mobilisation is feasible in intensive care patients receiving vasoactive therapy: An observational study. Aust. Crit. Care 2019, 32, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Sarfati, C.; Moore, A.; Pilorge, C.; Amaru, P.; Mendialdua, P.; Rodet, E.; Stéphan, F.; Rezaiguia-Delclaux, S. Efficacy of early passive tilting in minimizing ICU-acquired weakness: A randomized controlled trial. J. Crit. Care 2018, 46, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.; Shannon, J.R.; Black, B.K.; Ali, Y.; Farley, M.; Costa, F.; Diedrich, A.; Robertson, R.M. The pressor response to water drinking in humans: A sympathetic reflex? Circulation 2000, 101, 504–509. [Google Scholar] [CrossRef]
- Figueroa, J.J.; Basford, J.R.; Low, P.A. Preventing and treating orthostatic hypotension: As easy as A, B, C. Cleve. Clin. J. Med. 2010, 77, 298–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwasaki, K.; Zhang, R.; Perhonen, M.A.; Zuckerman, J.H.; Levine, B.D. Reduced baroreflex control of heart period after bed rest is normalized by acute plasma volume restoration. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2004, 287, R1256–R1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podoleanu, C.; Maggi, R.; Brignole, M.; Croci, F.; Incze, A.; Solano, A.; Puggioni, E.; Carasca, E. Lower limb and abdominal compression bandages prevent progressive orthostatic hypotension in elderly persons: A randomized single-blind controlled study. J. Am. Coll. Cardiol. 2006, 48, 1425–1432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorelik, O.; Shteinshnaider, M.; Tzur, I.; Feldman, L.; Cohen, N.; Almoznino-Sarafian, D. Factors associated with prevention of postural hypotension by leg compression bandaging. Blood Press 2014, 23, 248–254. [Google Scholar] [CrossRef]
- Bruïne, E.S.D.; Reijnierse, E.M.; Trappenburg, M.C.; Pasma, J.H.; Vries, O.J.D.; Meskers, C.G.; Maier, A.B. Standing up slowly antagonises initial blood pressure decrease in older adults with orthostatic hypotension. Gerontology 2017, 63, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Goswami, N.; Blaber, A.P.; Hinghofer-Szalkay, H.; Montani, J.P. Orthostatic intolerance in older persons: Etiology and countermeasures. Front. Physiol. 2017, 8, 803. [Google Scholar] [CrossRef] [Green Version]
- Berney, S.C.; Harrold, M.; Webb, S.A.; Seppelt, I.; Patman, S.; Thomas, P.J.; Denehy, L. Intensive care unit mobility practices in Australia and New Zealand: A point prevalence study. Crit. Care Resusc. 2013, 15, 260–265. [Google Scholar] [PubMed]
- Hashem, M.D.; Nelliot, A.; Needham, D.M. Early mobilization and rehabilitation in the ICU: Moving back to the future. Respir. Care 2016, 61, 971–979. [Google Scholar] [CrossRef]
- Liu, K.; Nakamura, K.; Katsukawa, H.; Elhadi, M.; Nydahl, P.; Ely, E.W.; Kudchadkar, S.R.; Takahashi, K.; Inoue, S.; Lefor, A.K.; et al. ABCDEF Bundle and supportive ICU practices for patients with coronavirus disease 2019 infection: An international point prevalence study. Crit. Care Explor. 2021, 3, e0353. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All Patients (n = 87) | Group without Patient-Related Safety Events (n = 77) | Group with Patient-Related Safety Events (n = 10) | p-Value | |
|---|---|---|---|---|
| Baseline characteristics | ||||
| Age in years; median (IQR) | 72.0 (61.0–79.0) | 69.0 (60.0–79.0) | 76.0 (70.0–80.0) | 0.401 |
| Sex: male; n (%) | 55 (63%) | 49 (64%) | 6 (60%) | 1 |
| BMI; kg/m2; median (IQR) | 22.8 (19.8–26.1) | 23.1 (20.0–27.0) | 20.7(19.5–23.0) | 0.084 |
| Charlson Comorbidity Index; median (IQR) | 2 (1–2) | 2 (1–2) | 2 (0–2) | 0.508 |
| Barthel Index prior to hospital admission; median (IQR) | 100.0 (90.0-100.0) | 100.0 (95.0-100.0) | 100.0 (25.0-100.0) | 0.325 |
| ICU admission diagnosis | 0.837 | |||
| Sepsis; n | 23 | 21 | 2 | |
| Gastrointestinal condition; n | 21 | 17 | 4 | |
| Cardiac failure including post cardiosurgery; n | 16 | 15 | 1 | |
| Respiratory failure; n | 13 | 11 | 2 | |
| Trauma; n | 5 | 5 | 0 | |
| Other; n | 9 | 8 | 1 | |
| APACHE II score; median (IQR) | 27.0 (21.0–30.0) | 25.0 (21.0–30.0) | 27.0 (23.0–29.0) | 0.995 |
| SOFA at ICU admission; median (IQR) | 10.0 (8.0–14.0) | 10.0 (8.0–14.0) | 9.00 (8.0–10.0) | 0.161 |
| Outcomes | ||||
| Time to first mobility session in days; median (IQR) | 2.0 (1.0–3.0) | 2.0 (1.0–4.0) | 1.0 (0.0–1.0) | 0.002 * |
| Time to first getting out of bed in days; median (IQR) | 4.0 (3.0–6.0) | 4.0 (3.0–7.0) | 2.5 (2.0–4.5) | 0.041 * |
| Time from first mobility session to first getting out of bed in days; median (IQR) | 1.0 (1.0–3.0) | 1.0 (0.0–3.0) | 1.5 (1.0–5.0) | 0.397 |
| Length of mechanical ventilation in days; median (IQR) | 6.0 (4.0–10.0) | 6.0 (4.0–10.0) | 5.7 (4.0–11.3) | 0.882 |
| Length of ICU stay in days; median (IQR) | 10.0 (7.0–14.0) | 10.0 (6.0–14.0) | 14.0 (7.0–17.0) | 0.219 |
| Length of hospital stay in days; median (IQR) | 42.0 (26.0–71.0) | 41.0 (25.5–70.5) | 53.5 (26.8–119.3) | 0.354 |
| Barthel Index at the time of hospital discharge; median (IQR) | 70.0 (10.0–100.0) | 65.0 (5.0–100.0) | 75.0 (65.0–95.0) | 0.262 |
| Reintubation during hospital stay; n (%) | 15 (17%) | 14 (18%) | 1 (10%) | 1 |
| ICU re-admission; n (%) | 10 (11%) | 10 (13%) | 0 (0%) | 0.638 |
| Parameters | Mobility Sessions without Patient-Related Safety Event(s) (n = 185) | Mobility Sessions with Patient-Related Safety Event(s) (n = 13) | p-Value |
|---|---|---|---|
| Mode of mechanical ventilation | 0.475 | ||
| Assist and Control; n | 29 | 4 | |
| SIMV; n | 37 | 1 | |
| PEEP and PS; n | 115 | 8 | |
| Other; n | 4 | 0 | |
| Parameters of mechanical ventilation | |||
| FIO2 (102); median (IQR) | 35 (30–40) | 35 (35–40) | 0.495 |
| PEEP; median (IQR) | 6 (5–8) | 8 (5–8) | 0.529 |
| Treatment | |||
| Patients on vasopressors before active mobilization; n (%) | 33 (18%) | 6 (46%) | 0.024 * |
| Undergoing CRRT; n (%) | 13 (7%) | 0 (0%) | 0.606 |
| RASS; median (IQR) | −1 (–1–0) | 0 (0–0) | 0.045 * |
| Highest activity level | 3 (3–3) | 4 (4–4) | <0.001 * |
| Vital signs before mobility session | |||
| PaO2 (mmHg); median (IQR) | 94 (80–118) | 102 (93–120) | 0.473 |
| PaCO2 (mmHg); median (IQR) | 39 (36–44) | 39 (37–46) | 0.134 |
| SBP (mmHg); median (IQR) | 125 (111–140) | 111 (101–129) | 0.144 |
| Heart rate (beats/min); median (IQR) | 90 (80–100) | 90 (80–97) | 0.946 |
| Respiratory rate (breaths/min); median (IQR) | 18 (15–21) | 17 (14–20) | 0.68 |
| Body temperature (°C); median (IQR) | 37.3 (36.8–37.9) | 37.7 (36.8–38.4) | 0.26 |
| Profession of mobilization provider | |||
| Doctor; n (%) | 52 (28%) | 3 (23%) | 1 |
| Nurse; n (%) | 153 (83%) | 13 (100%) | 1 |
| Physical therapist; n (%) | 175 (95%) | 10 (77%) | 0.043 * |
| Occupational therapist; n (%) | 28 (15%) | 3 (23%) | 0.433 |
| Number of Patient-Related Safety Events; n | Timing of Patient-Related Safety Event Occurrence in Days; Median (IQR) | Event Rate per 1000 Sessions | |
|---|---|---|---|
| Type of patient-related safety event | |||
| Systolic blood pressure | 8 | 5 (3–7) | 40.4 |
| Heart rate | 3 | 2 (2–3) | 15.2 |
| Desaturation | 2 | 5.5 (5–6) | 10.1 |
| Timing of patient-related safety event | |||
| Level 3: Sitting on edge of bed | 4 | 4 (3–4) | 26.1 |
| Level 4: Standing | 8 | 5 (2–6) | 205.1 |
| Level 5: Walking | 1 | 7 (7–7) | 166.7 |
| Odds Ratio | p-Value | |
|---|---|---|
| Use of vasopressors | 2.46 (0.70–8.63) | 0.159 |
| RASS | 1.34 (0.63–2.86) | 0.448 |
| Highest activity level | 2.83 (1.13–7.04) | 0.026 * |
| Mobility session without Physical Therapist | 0.37 (0.08–1.79) | 0.218 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katsukawa, H.; Ota, K.; Liu, K.; Morita, Y.; Watanabe, S.; Sato, K.; Ishii, K.; Yasumura, D.; Takahashi, Y.; Tani, T.; et al. Risk Factors of Patient-Related Safety Events during Active Mobilization for Intubated Patients in Intensive Care Units—A Multi-Center Retrospective Observational Study. J. Clin. Med. 2021, 10, 2607. https://doi.org/10.3390/jcm10122607
Katsukawa H, Ota K, Liu K, Morita Y, Watanabe S, Sato K, Ishii K, Yasumura D, Takahashi Y, Tani T, et al. Risk Factors of Patient-Related Safety Events during Active Mobilization for Intubated Patients in Intensive Care Units—A Multi-Center Retrospective Observational Study. Journal of Clinical Medicine. 2021; 10(12):2607. https://doi.org/10.3390/jcm10122607
Chicago/Turabian StyleKatsukawa, Hajime, Kohei Ota, Keibun Liu, Yasunari Morita, Shinichi Watanabe, Kazuhiro Sato, Kenzo Ishii, Daisetsu Yasumura, Yo Takahashi, Takafumi Tani, and et al. 2021. "Risk Factors of Patient-Related Safety Events during Active Mobilization for Intubated Patients in Intensive Care Units—A Multi-Center Retrospective Observational Study" Journal of Clinical Medicine 10, no. 12: 2607. https://doi.org/10.3390/jcm10122607