
Blinatumomab in Pediatric Acute Lymphoblastic Leukemia—From Salvage to First Line Therapy (A Systematic Review)


Abstract
:1. Introduction
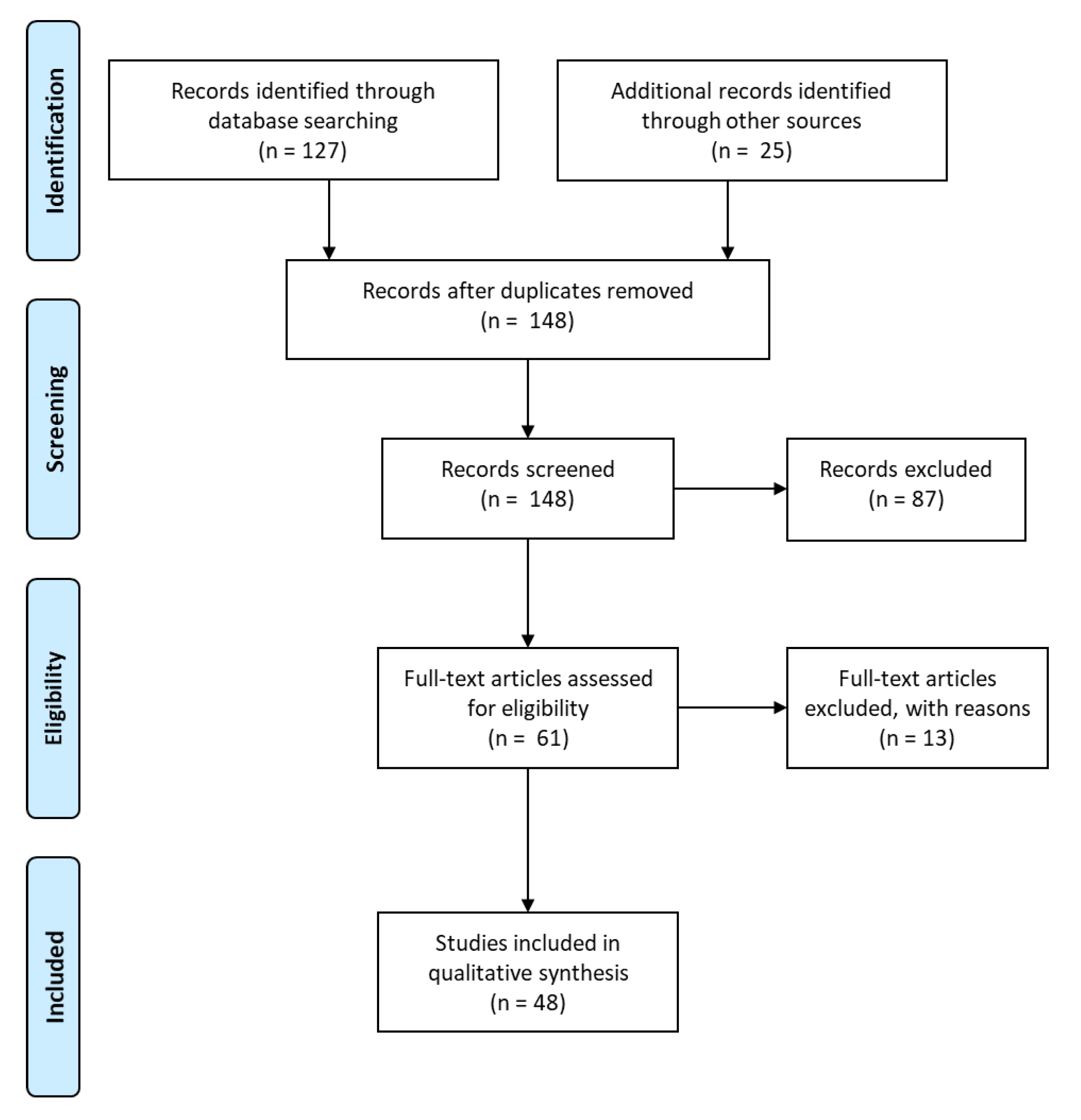
2. Materials and Methods
3. Results
3.1. Efficacy
3.2. Adverse Events
3.3. CD19 Expression
3.4. Clinical Trials
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Brischwein, K.; Schlereth, B.; Guller, B.; Steiger, C.; Wolf, A.; Lutterbuese, R.; Offner, S.; Locher, M.; Urbig, T.; Raum, T.; et al. MT110: A novel bispecific single-chain antibody construct with high efficacy in eradicating established tumors. Mol. Immunol. 2006, 43, 1129–1143. [Google Scholar] [CrossRef] [PubMed]
- Offner, S.; Hofmeister, R.; Romaniuk, A.; Kufer, P.; Baeuerle, P.A. Induction of regular cytolytic T cell synapses by bispecific single-chain antibody constructs on MHC class I-negative tumor cells. Mol. Immunol. 2006, 43, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, P.; Hofmeister, R.; Brischwein, K.; Brandl, C.; Crommer, S.; Bargou, R.; Itin, C.; Prang, N.; Baeuerle, P.A. Serial killing of tumor cells by cytotoxic T cells redirected with a CD19-/CD3-bispecific single-chain antibody construct. Int. J. Cancer 2005, 115, 98–104. [Google Scholar] [CrossRef]
- Pui, C.H.; Evans, W.E. Acute lymphoblastic leukemia. N. Engl. J. Med. 1998, 339, 605–615. [Google Scholar] [CrossRef] [Green Version]
- Greaves, M. Molecular genetics, natural history and the demise of childhood leukaemia. Eur. J. Cancer 1999, 35, 1941–1953. [Google Scholar] [CrossRef]
- Gokbuget, N.; Hoelzer, D. Recent approaches in acute lymphoblastic leukemia in adults. Rev. Clin. Exp. Hematol. 2002, 6, 114–141. [Google Scholar] [CrossRef] [PubMed]
- Schrappe, M.; Camitta, B.; Pui, C.H.; Eden, T.; Gaynon, P.; Gustafsson, G.; Janka-Schaub, G.E.; Kamps, W.; Masera, G.; Sallan, S.; et al. Long-term results of large prospective trials in childhood acute lymphoblastic leukemia. Leukemia 2000, 14, 2193–2194. [Google Scholar] [CrossRef] [Green Version]
- Gokbuget, N.; Dombret, H.; Ribera, J.M.; Fielding, A.K.; Advani, A.; Bassan, R.; Chia, V.; Doubek, M.; Giebel, S.; Hoelzer, D.; et al. International reference analysis of outcomes in adults with B-precursor Ph-negative relapsed/refractory acute lymphoblastic leukemia. Haematologica 2016, 101, 1524–1533. [Google Scholar] [CrossRef] [Green Version]
- Comans-Bitter, W.M.; de Groot, R.; van den Beemd, R.; Neijens, H.J.; Hop, W.C.; Groeneveld, K.; Hooijkaas, H.; van Dongen, J.J. Immunophenotyping of blood lymphocytes in childhood. Reference values for lymphocyte subpopulations. J. Pediatr. 1997, 130, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, L.M.; Gore, L. Blinatumomab, a Bi-Specific Anti-CD19/CD3 BiTE((R)) Antibody for the Treatment of Acute Lymphoblastic Leukemia: Perspectives and Current Pediatric Applications. Front. Oncol. 2014, 4, 63. [Google Scholar] [CrossRef] [Green Version]
- Franca, R.; Favretto, D.; Granzotto, M.; Decorti, G.; Rabusin, M.; Stocco, G. Epratuzumab and Blinatumomab as Therapeutic Antibodies for Treatment of Pediatric Acute Lymphoblastic Leukemia: Current Status and Future Perspectives. Curr. Med. Chem. 2017, 24, 1050–1065. [Google Scholar] [CrossRef] [PubMed]
- Algeri, M.; Del Bufalo, F.; Galaverna, F.; Locatelli, F. Current and future role of bispecific T-cell engagers in pediatric acute lymphoblastic leukemia. Expert Rev. Hematol. 2018, 11, 945–956. [Google Scholar] [CrossRef]
- Shukla, N.; Sulis, M.L. Blinatumomab for Treatment of Children With High-risk Relapsed B-Cell Acute Lymphoblastic Leukemia. JAMA 2021, 325, 830–832. [Google Scholar] [CrossRef] [PubMed]
- Inaba, H.; Pui, C.H. Immunotherapy in pediatric acute lymphoblastic leukemia. Cancer Metastasis Rev. 2019, 38, 595–610. [Google Scholar] [CrossRef] [PubMed]
- Foster, J.B.; Maude, S.L. New developments in immunotherapy for pediatric leukemia. Curr. Opin. Pediatr. 2018, 30, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Bautista, F.; Van der Lugt, J.; Kearns, P.R.; Mussai, F.J.; Zwaan, C.M.; Moreno, L. The development of targeted new agents to improve the outcome for children with leukemia. Expert Opin. Drug Discov. 2016, 11, 1111–1122. [Google Scholar] [CrossRef] [PubMed]
- Jasinski, S.; De Los Reyes, F.A.; Yametti, G.C.; Pierro, J.; Raetz, E.; Carroll, W.L. Immunotherapy in Pediatric B-Cell Acute Lymphoblastic Leukemia: Advances and Ongoing Challenges. Paediatr. Drugs 2020, 22, 485–499. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Handgretinger, R.; Zugmaier, G.; Henze, G.; Kreyenberg, H.; Lang, P.; von Stackelberg, A. Complete remission after blinatumomab-induced donor T-cell activation in three pediatric patients with post-transplant relapsed acute lymphoblastic leukemia. Leukemia 2011, 25, 181–184. [Google Scholar] [CrossRef] [Green Version]
- Schlegel, P.; Lang, P.; Zugmaier, G.; Ebinger, M.; Kreyenberg, H.; Witte, K.E.; Feucht, J.; Pfeiffer, M.; Teltschik, H.M.; Kyzirakos, C.; et al. Pediatric posttransplant relapsed/refractory B-precursor acute lymphoblastic leukemia shows durable remission by therapy with the T-cell engaging bispecific antibody blinatumomab. Haematologica 2014, 99, 1212–1219. [Google Scholar] [CrossRef] [Green Version]
- von Stackelberg, A.; Locatelli, F.; Zugmaier, G.; Handgretinger, R.; Trippett, T.M.; Rizzari, C.; Bader, P.; O’Brien, M.M.; Brethon, B.; Bhojwani, D.; et al. Phase I/Phase II Study of Blinatumomab in Pediatric Patients With Relapsed/Refractory Acute Lymphoblastic Leukemia. J. Clin. Oncol. 2016, 34, 4381–4389. [Google Scholar] [CrossRef] [Green Version]
- Gore, L.; Locatelli, F.; Zugmaier, G.; Handgretinger, R.; O’Brien, M.M.; Bader, P.; Bhojwani, D.; Schlegel, P.G.; Tuglus, C.A.; von Stackelberg, A. Survival after blinatumomab treatment in pediatric patients with relapsed/refractory B-cell precursor acute lymphoblastic leukemia. Blood Cancer J. 2018, 8, 80. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.A.; Ji, L.; Xu, X.; Devidas, M.; Hogan, L.; Borowitz, M.J.; Raetz, E.A.; Zugmaier, G.; Sharon, E.; Gore, L.; et al. A Randomized Phase 3 Trial of Blinatumomab Vs. Chemotherapy As Post-Reinduction Therapy in High and Intermediate Risk (HR/IR) First Relapse of B-Acute Lymphoblastic Leukemia (B-ALL) in Children and Adolescents/Young Adults (AYAs) Demonstrates Superior Efficacy and Tolerability of Blinatumomab: A Report from Children’s Oncology Group Study AALL1331. Blood 2019, 134, LBA-1. [Google Scholar] [CrossRef]
- Locatelli, F.; Whitlock, J.A.; Peters, C.; Chen-Santel, C.; Chia, V.; Dennis, R.M.; Heym, K.M.; Katz, A.J.; Kelsh, M.A.; Sposto, R.; et al. Blinatumomab versus historical standard therapy in pediatric patients with relapsed/refractory Ph-negative B-cell precursor acute lymphoblastic leukemia. Leukemia 2020, 34, 2473–2478. [Google Scholar] [CrossRef]
- Locatelli, F.; Zugmaier, G.; Mergen, N.; Bader, P.; Jeha, S.; Schlegel, P.G.; Bourquin, J.P.; Handgretinger, R.; Brethon, B.; Rossig, C.; et al. Blinatumomab in pediatric patients with relapsed/refractory acute lymphoblastic leukemia: Results of the RIALTO trial, an expanded access study. Blood Cancer J. 2020, 10, 77. [Google Scholar] [CrossRef] [PubMed]
- Mouttet, B.; Vinti, L.; Ancliff, P.; Bodmer, N.; Brethon, B.; Cario, G.; Chen-Santel, C.; Elitzur, S.; Hazar, V.; Kunz, J.; et al. Durable remissions in TCF3-HLF positive acute lymphoblastic leukemia with blinatumomab and stem cell transplantation. Haematologica 2019, 104, e244–e247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keating, A.K.; Gossai, N.; Phillips, C.L.; Maloney, K.; Campbell, K.; Doan, A.; Bhojwani, D.; Burke, M.J.; Verneris, M.R. Reducing minimal residual disease with blinatumomab prior to HCT for pediatric patients with acute lymphoblastic leukemia. Blood Adv. 2019, 3, 1926–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadhwa, A.; Kutny, M.A.; Xavier, A.C. Blinatumomab activity in a patient with Down syndrome B-precursor acute lymphoblastic leukemia. Pediatr. Blood Cancer 2018, 65. [Google Scholar] [CrossRef] [PubMed]
- Elitzur, S.; Arad-Cohen, N.; Barzilai-Birenboim, S.; Ben-Harush, M.; Bielorai, B.; Elhasid, R.; Feuerstein, T.; Gilad, G.; Gural, A.; Kharit, M.; et al. Blinatumomab as a bridge to further therapy in cases of overwhelming toxicity in pediatric B-cell precursor acute lymphoblastic leukemia: Report from the Israeli Study Group of Childhood Leukemia. Pediatr. Blood Cancer 2019, 66, e27898. [Google Scholar] [CrossRef] [PubMed]
- Pieters, R.; Schrappe, M.; De Lorenzo, P.; Hann, I.; De Rossi, G.; Felice, M.; Hovi, L.; LeBlanc, T.; Szczepanski, T.; Ferster, A.; et al. A treatment protocol for infants younger than 1 year with acute lymphoblastic leukaemia (Interfant-99): An observational study and a multicentre randomised trial. Lancet 2007, 370, 240–250. [Google Scholar] [CrossRef]
- Pieters, R.; De Lorenzo, P.; Ancliffe, P.; Aversa, L.A.; Brethon, B.; Biondi, A.; Campbell, M.; Escherich, G.; Ferster, A.; Gardner, R.A.; et al. Outcome of Infants Younger Than 1 Year With Acute Lymphoblastic Leukemia Treated With the Interfant-06 Protocol: Results From an International Phase III Randomized Study. J. Clin. Oncol. 2019, 37, 2246–2256. [Google Scholar] [CrossRef]
- Clesham, K.; Rao, V.; Bartram, J.; Ancliff, P.; Ghorashian, S.; O’Connor, D.; Pavasovic, V.; Rao, A.; Samarasinghe, S.; Cummins, M.; et al. Blinatumomab for infant acute lymphoblastic leukemia. Blood 2020, 135, 1501–1504. [Google Scholar] [CrossRef]
- Contreras, C.F.; Higham, C.S.; Behnert, A.; Kim, K.; Stieglitz, E.; Tasian, S.K. Clinical utilization of blinatumomab and inotuzumab immunotherapy in children with relapsed or refractory B-acute lymphoblastic leukemia. Pediatr. Blood Cancer 2021, 68, e28718. [Google Scholar] [CrossRef]
- Ampatzidou, M.; Kattamis, A.; Baka, M.; Paterakis, G.; Anastasiou, T.; Tzanoudaki, M.; Kaisari, A.; Avgerinou, G.; Doganis, D.; Papadakis, V.; et al. Insights from the Greek experience of the use of Blinatumomab in pediatric relapsed and refractory acute lymphoblastic leukemia patients. Neoplasma 2020, 67, 1424–1430. [Google Scholar] [CrossRef]
- Horibe, K.; Morris, J.D.; Tuglus, C.A.; Dos Santos, C.; Kalabus, J.; Anderson, A.; Goto, H.; Ogawa, C. A phase 1b study of blinatumomab in Japanese children with relapsed/refractory B-cell precursor acute lymphoblastic leukemia. Int. J. Hematol. 2020, 112, 223–233. [Google Scholar] [CrossRef]
- Queudeville, M.; Schlegel, P.; Heinz, A.T.; Lenz, T.; Doring, M.; Holzer, U.; Hartmann, U.; Kreyenberg, H.; von Stackelberg, A.; Schrappe, M.; et al. Blinatumomab in pediatric patients with relapsed/refractory B-cell precursor acute lymphoblastic leukemia. Eur. J. Haematol. 2021, 106, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Sutton, R.; Pozza, L.D.; Khaw, S.L.; Fraser, C.; Revesz, T.; Chamberlain, J.; Mitchell, R.; Trahair, T.N.; Bateman, C.M.; Venn, N.C.; et al. Outcomes for Australian children with relapsed/refractory acute lymphoblastic leukaemia treated with blinatumomab. Pediatr. Blood Cancer 2021, 68, e28922. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.A.; Ji, L.; Xu, X.; Devidas, M.; Hogan, L.E.; Borowitz, M.J.; Raetz, E.A.; Zugmaier, G.; Sharon, E.; Bernhardt, M.B.; et al. Effect of Postreinduction Therapy Consolidation With Blinatumomab vs Chemotherapy on Disease-Free Survival in Children, Adolescents, and Young Adults With First Relapse of B-Cell Acute Lymphoblastic Leukemia: A Randomized Clinical Trial. JAMA 2021, 325, 833–842. [Google Scholar] [CrossRef]
- Locatelli, F.; Zugmaier, G.; Rizzari, C.; Morris, J.D.; Gruhn, B.; Klingebiel, T.; Parasole, R.; Linderkamp, C.; Flotho, C.; Petit, A.; et al. Effect of Blinatumomab vs Chemotherapy on Event-Free Survival Among Children With High-risk First-Relapse B-Cell Acute Lymphoblastic Leukemia: A Randomized Clinical Trial. JAMA 2021, 325, 843–854. [Google Scholar] [CrossRef] [PubMed]
- Mejstrikova, E.; Hrusak, O.; Borowitz, M.J.; Whitlock, J.A.; Brethon, B.; Trippett, T.M.; Zugmaier, G.; Gore, L.; von Stackelberg, A.; Locatelli, F. CD19-negative relapse of pediatric B-cell precursor acute lymphoblastic leukemia following blinatumomab treatment. Blood Cancer J. 2017, 7, 659. [Google Scholar] [CrossRef] [PubMed]
- Zoghbi, A.; Zur Stadt, U.; Winkler, B.; Muller, I.; Escherich, G. Lineage switch under blinatumomab treatment of relapsed common acute lymphoblastic leukemia without MLL rearrangement. Pediatr. Blood Cancer 2017, 64. [Google Scholar] [CrossRef]
- Wolfl, M.; Rasche, M.; Eyrich, M.; Schmid, R.; Reinhardt, D.; Schlegel, P.G. Spontaneous reversion of a lineage switch following an initial blinatumomab-induced ALL-to-AML switch in MLL-rearranged infant ALL. Blood Adv. 2018, 2, 1382–1385. [Google Scholar] [CrossRef] [Green Version]
- Mikhailova, E.; Gluhanyuk, E.; Illarionova, O.; Zerkalenkova, E.; Kashpor, S.; Miakova, N.; Diakonova, Y.; Olshanskaya, Y.; Shelikhova, L.; Novichkova, G.; et al. Immunophenotypic changes of leukemic blasts in children with relapsed/refractory B-cell precursor acute lymphoblastic leukemia, who have been treated with Blinatumomab. Haematologica 2020. [Google Scholar] [CrossRef] [PubMed]
- Brethon, B.; Lainey, E.; Caye-Eude, A.; Grain, A.; Fenneteau, O.; Yakouben, K.; Roupret-Serzec, J.; Le Mouel, L.; Cave, H.; Baruchel, A. Case Report: Targeting 2 Antigens as a Promising Strategy in Mixed Phenotype Acute Leukemia: Combination of Blinatumomab With Gemtuzumab Ozogamicin in an Infant With a KMT2A-Rearranged Leukemia. Front. Oncol. 2021, 11, 637951. [Google Scholar] [CrossRef]
- Aldoss, I.; Song, J.Y. Extramedullary relapse of KMT2A(MLL)-rearranged acute lymphoblastic leukemia with lineage switch following blinatumomab. Blood 2018, 131, 2507. [Google Scholar] [CrossRef]
- Kiyoi, H.; Morris, J.D.; Oh, I.; Maeda, Y.; Minami, H.; Miyamoto, T.; Sakura, T.; Iida, H.; Tuglus, C.A.; Chen, Y.; et al. Phase 1b/2 study of blinatumomab in Japanese adults with relapsed/refractory acute lymphoblastic leukemia. Cancer Sci. 2020, 111, 1314–1323. [Google Scholar] [CrossRef]
- Bader, P.; Kreyenberg, H.; Henze, G.H.; Eckert, C.; Reising, M.; Willasch, A.; Barth, A.; Borkhardt, A.; Peters, C.; Handgretinger, R.; et al. Prognostic value of minimal residual disease quantification before allogeneic stem-cell transplantation in relapsed childhood acute lymphoblastic leukemia: The ALL-REZ BFM Study Group. J. Clin. Oncol. 2009, 27, 377–384. [Google Scholar] [CrossRef]
- Tallen, G.; Ratei, R.; Mann, G.; Kaspers, G.; Niggli, F.; Karachunsky, A.; Ebell, W.; Escherich, G.; Schrappe, M.; Klingebiel, T.; et al. Long-term outcome in children with relapsed acute lymphoblastic leukemia after time-point and site-of-relapse stratification and intensified short-course multidrug chemotherapy: Results of trial ALL-REZ BFM 90. J. Clin. Oncol. 2010, 28, 2339–2347. [Google Scholar] [CrossRef] [PubMed]
- von Stackelberg, A.; Volzke, E.; Kuhl, J.S.; Seeger, K.; Schrauder, A.; Escherich, G.; Henze, G.; Tallen, G.; Group, A.-R.B.S. Outcome of children and adolescents with relapsed acute lymphoblastic leukaemia and non-response to salvage protocol therapy: A retrospective analysis of the ALL-REZ BFM Study Group. Eur. J. Cancer 2011, 47, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Buitenkamp, T.D.; Izraeli, S.; Zimmermann, M.; Forestier, E.; Heerema, N.A.; van den Heuvel-Eibrink, M.M.; Pieters, R.; Korbijn, C.M.; Silverman, L.B.; Schmiegelow, K.; et al. Acute lymphoblastic leukemia in children with Down syndrome: A retrospective analysis from the Ponte di Legno study group. Blood 2014, 123, 70–77. [Google Scholar] [CrossRef] [Green Version]
- Minson, K.A.; Prasad, P.; Vear, S.; Borinstein, S.; Ho, R.; Domm, J.; Frangoul, H. t(17;19) in Children with Acute Lymphocytic Leukemia: A Report of 3 Cases and a Review of the Literature. Case Rep. Hematol. 2013, 2013, 563291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biondi, A.; Schrappe, M.; De Lorenzo, P.; Castor, A.; Lucchini, G.; Gandemer, V.; Pieters, R.; Stary, J.; Escherich, G.; Campbell, M.; et al. Imatinib after induction for treatment of children and adolescents with Philadelphia-chromosome-positive acute lymphoblastic leukaemia (EsPhALL): A randomised, open-label, intergroup study. Lancet Oncol. 2012, 13, 936–945. [Google Scholar] [CrossRef]
- Dixon, S.B.; Chen, Y.; Yasui, Y.; Pui, C.H.; Hunger, S.P.; Silverman, L.B.; Ness, K.K.; Green, D.M.; Howell, R.M.; Leisenring, W.M.; et al. Reduced Morbidity and Mortality in Survivors of Childhood Acute Lymphoblastic Leukemia: A Report From the Childhood Cancer Survivor Study. J. Clin. Oncol. 2020, 38, 3418–3429. [Google Scholar] [CrossRef] [PubMed]
- Tambaro, F.P.; Khazal, S.; Nunez, C.; Ragoonanan, D.; Tewari, P.; Petropoulos, D.; Kebriaei, P.; Wierda, W.G.; Mahadeo, K.M. Complete remission in refractory acute lymphoblastic leukemia using blinatumomab after failure of response to CD-19 chimeric antigen receptor T-cell therapy. Clin. Case Rep. 2020, 8, 1678–1681. [Google Scholar] [CrossRef] [PubMed]
- Danylesko, I.; Chowers, G.; Shouval, R.; Besser, M.J.; Jacoby, E.; Shimoni, A.; Nagler, A.; Avigdor, A. Treatment with anti CD19 chimeric antigen receptor T cells after antibody-based immunotherapy in adults with acute lymphoblastic leukemia. Curr. Res. Transl. Med. 2020, 68, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Sigmund, A.M.; Sahasrabudhe, K.D.; Bhatnagar, B. Evaluating Blinatumomab for the Treatment of Relapsed/Refractory ALL: Design, Development, and Place in Therapy. Blood Lymphat. Cancer 2020, 10, 7–20. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Year | Ref. 1 | Patients | Title |
|---|---|---|---|---|
| Handgretinger | 2011 | [19] | 3 R/R-ALL patients post-HSCT | CR after blinatumomab-induced donor T-cell activation in three pediatric patients with post-transplant relapsed ALL |
| Schlegel | 2014 | [20] | 9 R/R-ALL patients post-HSCT | Pediatric post-transplant R/R BCP ALL leukemia shows durable remission by therapy with the T-cell engaging bispecific antibody blinatumomab |
| Von Stackelberg | 2016 | [21] | 93 R/R patients (70 with recommended dosage) | Phase I/phase II study of blinatumomab in pediatric patients with R/R ALL |
| Mejstríková | 2017 | [40] | 18 patients (4 with CD19-negative relapse) | CD19-negative relapse of pediatric BCP-ALL following blinatumomab treatment |
| Zoghbi | 2017 | [41] | case report | Lineage switch under blinatumomab treatment of relapsed common ALL without MLL rearrangement |
| Wadhwa | 2018 | [28] | case report | Blinatumomab activity in a patient with Down syndrome BCP-ALL |
| Gore | 2018 | [22] | 70 R/R-ALL patients | Survival after blinatumomab treatment in pediatric patients with R/R BCP-ALL |
| Wölfl | 2018 | [42] | case report | Spontaneous reversion of a lineage switch following an initial blinatumomab-induced ALL-to-AML switch in MLL-rearranged infant ALL |
| Mouttet | 2019 | [26] | 9 TCF3/HLF | Durable remissions in TCF3-HLF positive acute lymphoblastic leukemia with blinatumomab and SCT |
| Keating | 2019 | [27] | 15 children MRD-positive before HSCT | Reducing minimal residual disease with blinatumomab prior to HSCT for pediatric patients with ALL |
| Elitzur | 2019 | [29] | 11 pediatric patients with overwhelming chemotherapy-associated toxicity | Blinatumomab as a bridge to further therapy in case of overwhelming toxicity in pediatric BCP-ALL |
| Brown | 2019 | [23] | 59 patients of the MT103-205 study (NCT01471782) | Day 15 bone marrow MRD predicts response to blinatumomab |
| Locatelli | 2020 | [24] | 70 patients of the MT103-205 study (NCT01471782) | Blinatumomab versus historical standard therapy in pediatric patients with R/R Ph-negative BCP-ALL |
| Locatelli | 2020 | [25] | 110 R/R-ALL patients | Blinatumomab in pediatric patients with R/R ALL: results of the RIALTO trial, an expanded access study |
| Mikhailova | 2020 | [43] | 90 patients | Immunophenotypic changes of leukemic blasts in children with R/R- ALL who have been treated with blinatumomb |
| Contreras | 2020 | [33] | 27 children/young adults treated with blinatumomab and/or inotuzumab | Clinical utilization of blinatumomab and inotuzumab immunotherapy in children with relapsed or refractory B-ALL |
| Clesham | 2020 | [32] | 11 infants | Blinatumomab for infant ALL |
| Horibe | 2020 | [35] | 9 children | A phase 1 study of blinatumomab in Japanese children |
| Ampatzidou | 2020 | [34] | 9 children | Insights from the Greek experience of the use of Blinatumomab in pediatric R/R ALL |
| Queudeville | 2021 | [36] | 38 R/R-ALL patients | Blinatumomab in pediatric patients with relapsed/refractory B-cell precursor acute lymphoblastic leukemia |
| Sutton | 2021 | [37] | 24 R/R-ALL patients outside of clinical trials | Outcomes for Australian children with relapsed/refractory acute lymphoblastic leukaemia treated with blinatumomab |
| Brethon | 2021 | [44] | case report | Targeting 2 antigens as a promising strategy in mixed phenotype acute leukemia: combination with blinatumomab with gemtuzumab ozogamicin in an infant with KMT2A-rearraged leukemia |
| Brown | 2021 | [38] | 208 pts, 1 to 30 years | Effect of Postreinduction Therapy Consolidation with Blinatumomab vs. Chemotherapy on Disease-Free Survival in Children, Adolescents, and Young Adults with First relapse of B-Cell Acute Lymphoblastic Leukemia NCT02101853 |
| Locatelli | 2021 | [39] | 108 pts, 28 days to 18 years | Effect of Blinatumomab vs. Chemotherapy on Event-Free Survival Among Children with High-risk First-Relapse B-Cell Acute Lymphoblastic Leukemia: A Randomized Clinical Trial NCT02393859 |
| Clinical Trials Identifier | Other Study ID Numbers | Ref. 1 | Title | Age | Status |
|---|---|---|---|---|---|
| NCT01471782 | MT103-205 2010-024264-18 (Eudra-CT) | [21] | Clinical Study With Blinatumomab in Pediatric and Adolescent Patients With Relapsed/Refractory B-precursor Acute Lymphoblastic Leukemia | Up to 17 years (child) | completed |
| NCT02187354 | RIALTO 2014-001700-21 (EudraCT) | [25] | Expanded Access Protocol-Blinatumomab in Pediatric & Adolescent Subjects with Relapsed/Refractory B-precursor ALL (RIALTO) | Up to 17 years (child) | completed |
| NCT02783651 | 20150253 | A Study of Patients with Ph- Chromosome-negative Relapsed or Refractory Acute Lymphoblastic Leukemia in the US | Child, adult | completed | |
| NCT02879695 | NCI-2016-01300 (CTRP) | Blinatumomab and Nivolumab With or Without Ipilimumab in Treating Patients With Poor-Risk Relapsed or Refractory CD19+ Precursor B-Lymphoblastic Leukemia | 16 years and older | recruiting | |
| NCT02393859 | 2014-002476-92 (EudraCT) | [39] | Phase 3 Trial of Blinatumomab vs. Standard Chemotherapy in Pediatric Subjects With High-Risk (HR) First Relapse B-precursor Acute Lymphoblastic Leukemia (ALL) | Up to 17 years (child) | active, not recruiting |
| NCT04546399 | NCI-2020-06813 (CTRP) | A Study to Compare Blinatumomab Alone to Blinatumomab With Nivolumab in Patients Diagnosed With First Relapse B-Cell Acute Lymphoblastic Leukemia (B-ALL) | 1 to 31 years (child, adult) Including Down syndrome patients | recruiting | |
| NCT03914625 | NCI-2019-02187 (CTRP) | A Study to Investigate Blinatumomab in Combination With Chemotherapy in Patients With Newly Diagnosed B-Lymphoblastic Leukemia | 1 to 31 years (child, adult) Including Down syndrome patients | recruiting | |
| NCT02101853 | NCI-2014-00631 (CTRP) COG-AALL1331 | [38] | Blinatumomab in Treating Younger Patients With Relapsed B-cell Acute Lymphoblastic Leukemia | 1 to 31 years (child, adult) | Active, not recruiting |
| NCT02877303 | NCI-2017-00596 (CTRP) | Blinatumomab and Combination Chemotherapy as Frontline Therapy in Treating Patients With B Acute Lymphoblastic Leukemia | 14 years and older | recruiting | |
| NCT02790515 | REF2HCT NCI-2016-00812 (CTRP) | Provision of TCRγδ T Cells and Memory T Cells Plus Selected Use of Blinatumomab in Naïve T-cell Depleted Haploidentical Donor Hematopoietic Cell Transplantation for Hematologic Malignancies Relapsed or Refractory Despite Prior Transplantation | Up to 21 years | recruiting | |
| NCT03849651 | HAP2HCT | TCRαβ-depleted Progenitor Cell Graft With Additional Memory T-cell DLI, Plus Selected Use of Blinatumomab, in Naive T-cell Depleted Haploidentical Donor Hematopoietc Cell Transplantation for Hematologic Malignancies | Up to 21 years | recruiting | |
| NCT04307576 | ALLTogether1 2018-001795-38 (EudraCT) | ALLTogether1—A Treatment Study Protocol of the ALLTogether Consortium for Children and Young Adults (1–45 Years of Age) With Newly Diagnosed Acute Lymphoblastic Leukaemia (ALL) | 1 to 45 years | recruiting | |
| NCT03643276 | AIEOP-BFM ALL 2017 2016-001935-12 (EudraCT) | Treatment Protocol for Children and Adolescents With Acute Lymphoblastic Leukemia-AIEOP-BFM ALL 2017 | Up to 17 years | recruiting | |
| NCT03117751 | TOT17 NCI-2017-00582 (CTRP) | Total Therapy XVII for Newly Diagnosed Patients With Acute Lymphoblastic Leukemia and Lymphoma | 1 to 18 years | recruiting | |
| 2016-004674-17 (EudraCT) ML59901.078.17 | A pilot study to test the feasibility, safety and efficacy of the addition of the BiTE antibody Blinatumomab to the Interfant-06 backbone in infants with MLL-rearranged acute lymphoblastic leukemia. A collaborative study of the Interfant network | Up to 17 years | recruiting | ||
| NCT04604691 | Blinatumomab in Pediatric B-cell Acute Lymphoblastic Leukemia (ALL) with Minimal Residual Disease (MRD) | Not yet recruiting | |||
| NCT03605589 | Pembro and Blina combination in Pediatric and Young Adult Patients With Relapsed/Refractory Acute Leukemia or Lymphoma | 1 to 40 years | Suspended, slow recruitment, amendment pending | ||
| NCT04723342 | ALL-MB 2019 Pilot | Treatment of Children and Adolescents With Primary B-precursor Acute Lymphoblastic Leukemia With Combination Chemotherapy and Immunotherapy | 1–18 years | recruiting | |
| NCT04556084 | Blina Part 1 | Blinatumomab Bridging Therapy | Up to 25 years | recruiting | |
| NCT04746209 | Blina Part 2 | Blinatumomab After TCR Alpha Beta/CD19 Depleted HCT | Up to 25 years | not yet recruiting | |
| NCT02807883 | NCI-2016-01182 | Blinatumomab Maintenance Following Allogeneic Hematopoietic Cell Transplantation for Patients With Acute Lymphoblastic Leukemia | 1 to 70 years | active, not recruiting | |
| NCT02412306 | 20130265 | Study of Blinatumomab in Japanese Patients With Relapsed/Refractory B-precursor Acute Lymphoblastic Leukemia | <18 years for pediatric subjects | recruiting | |
| NCT02877303 | 2014-0845 NCI-2017-00596 | Blinatumomab, Inotuzumab Ozogamicin, and Combination Chemotherapy as Frontline Therapy in Treating Patients With B Acute Lymphoblastic Leukemia | 14 years and older | recruiting | |
| NCT04044560 | H19-00893 CTTC 1902 | Blinatumomab for MRD in Pre-B-ALL Patients Following Stem Cell Transplant (OZM-097) | 1 year and older (children and adults) | not yet recruiting | |
| NCT04785547 | FORUM Add-on Blina post TX | ALL SCTped 2012 FORUM Add-on Study Blina Post HSCT | 6 months to 21 years | recruiting |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Queudeville, M.; Ebinger, M. Blinatumomab in Pediatric Acute Lymphoblastic Leukemia—From Salvage to First Line Therapy (A Systematic Review). J. Clin. Med. 2021, 10, 2544. https://doi.org/10.3390/jcm10122544
Queudeville M, Ebinger M. Blinatumomab in Pediatric Acute Lymphoblastic Leukemia—From Salvage to First Line Therapy (A Systematic Review). Journal of Clinical Medicine. 2021; 10(12):2544. https://doi.org/10.3390/jcm10122544
Chicago/Turabian StyleQueudeville, Manon, and Martin Ebinger. 2021. "Blinatumomab in Pediatric Acute Lymphoblastic Leukemia—From Salvage to First Line Therapy (A Systematic Review)" Journal of Clinical Medicine 10, no. 12: 2544. https://doi.org/10.3390/jcm10122544