
Challenges in Patient Blood Management for Cardiac Surgery: A Narrative Review

 ,
,
Abstract
:1. Introduction: The Scope of the Problem
2. Challenges in Building an Adequate PBM Structure
2.1. PBM Coordinator
2.2. Stakeholders in PBM Applied to Cardiac Surgery
2.3. Funding
2.4. Education
2.5. Quality Monitoring
3. Overcoming Resistances to a Change
- Lack of knowledge or incorrect outcome expectancy: the physician simply ignores the recommendation or does not believe that it leads to a better outcome.
- Inertia in abandoning well rooted practice: this may result from active choices, motivated by skepticism or fear, or be simply intellectual idleness.
- Protocols may compromise “autonomy” of physicians: adherence to protocols may be perceived as a severe limitation of professional freedom, affecting self-perception and status.
- External barriers: inability to reconcile patient preferences with recommendations, lack of time or resources, organizational constraints.
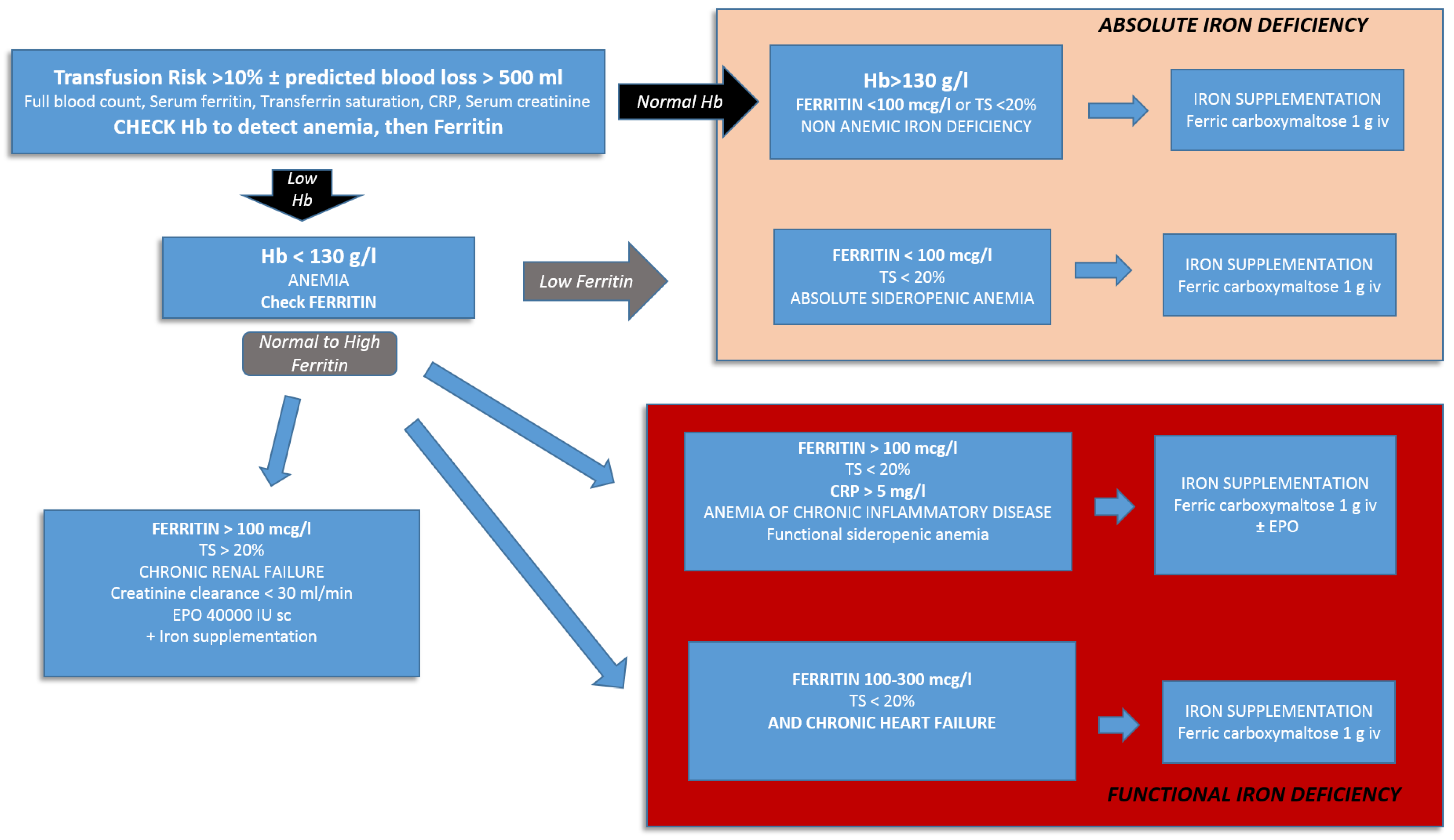
4. Challenges in Preoperative Anemia Correction: Barriers and Misconceptions
4.1. Anemia, Cardiac Surgery and Outcome in Women
4.2. When to Start Anemia Treatment?
5. Iron Deficiency: An Emerging Marker for Worse Outcome and a Target for Treatment
6. Are Erythropoiesis Stimulating Agents (ESA) Effective and Safe?
7. Optimizing Coagulation and Antithrombotic Treatment
7.1. Hemostatic Evaluation
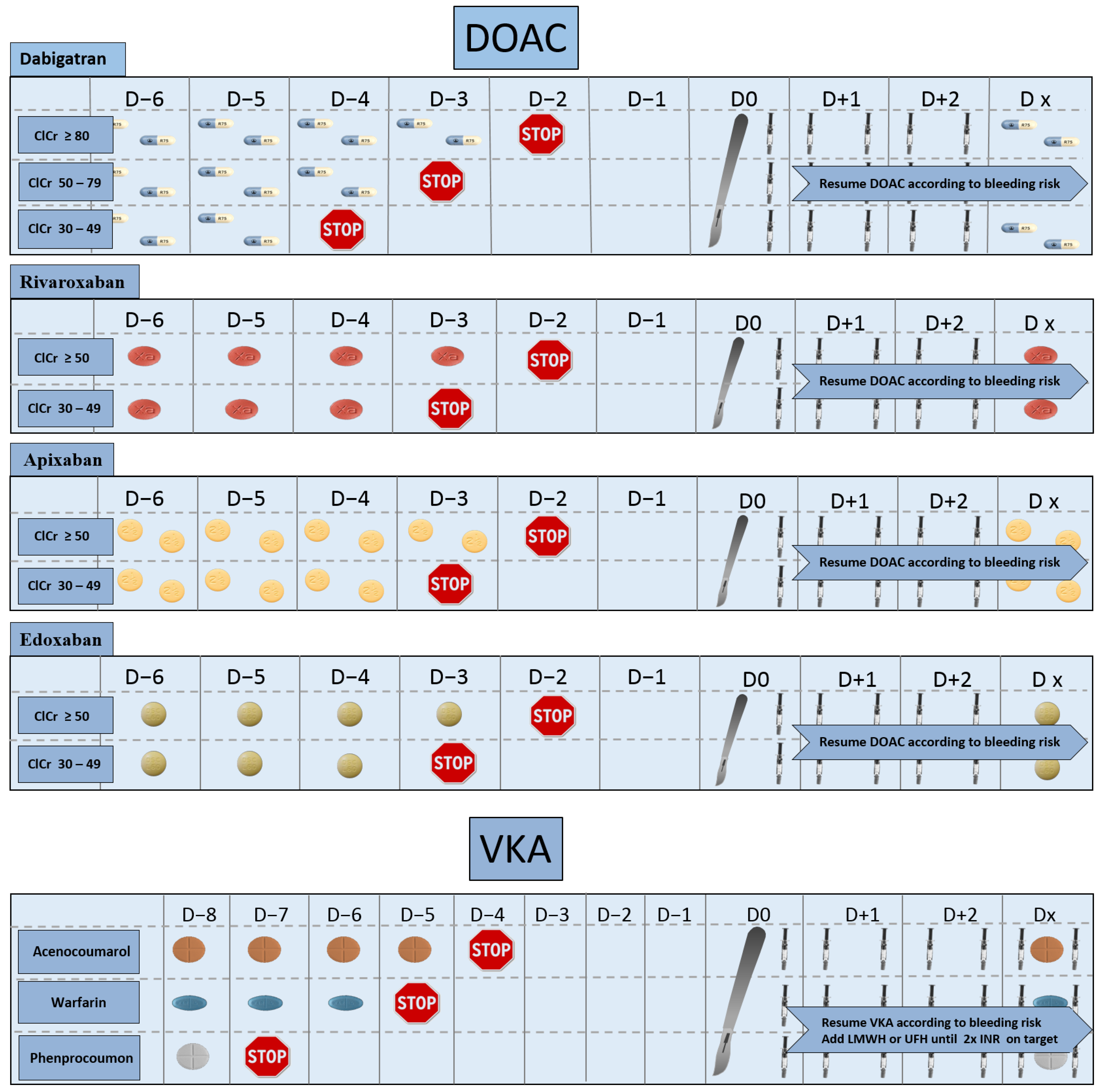
7.2. Discontinuation of Anticoagulants
7.3. Discontinuation of Antiaggregants
8. Challenges in the Intra-Operative Phase
8.1. Anesthetic Management
8.2. Management of Shed Blood and Cell Savage
8.3. Minimal Invasive Extracorporeal Circuits (MiECC)
8.4. Autologous Priming
8.5. Heparin/Protamine Management
8.6. Targeted Treatment of Coagulopathies
8.7. The Use of Factor Concentrates in Cardiac Surgery
8.8. Temperature
8.9. Off-Pump Surgical Revascularization
8.10. Acute Normovolemic Hemodilution
9. Postoperative Management: Applying Appropriate RBC Transfusion Triggers
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hartmann, M.; Sucker, C.; Boehm, O.; Koch, A.; Loer, S.S.; Zacharowski, K. Effects of cardiac surgery on hemostasis. Transfus. Med. Rev. 2006, 20, 230–241. [Google Scholar] [CrossRef] [PubMed]
- Robich, M.P.; Koch, C.G.; Johnston, D.R.; Schiltz, N.; Chandran Pillai, A.; Hussain, S.T.; Soltesz, E.G. Trends in blood utilization in United States cardiac surgical patients. Transfusion 2015, 55, 805–814. [Google Scholar] [CrossRef]
- Snyder-Ramos, S.A.; Mohnle, P.; Weng, Y.S.; Bottiger, B.W.; Kulier, A.; Levin, J.; Mangano, D.T.; Investigators of the Multicenter Study of Perioperative Ischemia; MCSPI Research Group. The ongoing variability in blood transfusion practices in cardiac surgery. Transfusion 2008, 48, 1284–1299. [Google Scholar] [CrossRef]
- D’Agostino, R.S.; Jacobs, J.P.; Badhwar, V.; Fernandez, F.G.; Paone, G.; Wormuth, D.W.; Shahian, D.M. The Society of Thoracic Surgeons Adult Cardiac Surgery Database: 2019 Update on Outcomes and Quality. Ann. Thorac. Surg. 2019, 107, 24–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Society of Anesthesiologists Task Force on Perioperative Blood Management. Practice guidelines for perioperative blood management: An updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Management*. Anesthesiology 2015, 122, 241–275. [Google Scholar] [CrossRef] [PubMed]
- Task, F.; Ferraris, V.A.; Brown, J.R.; Despotis, G.J.; Hammon, J.W.; Reece, T.B.; Saha, S.P.; Song, H.K.; Clough, E.R.; Blood, T.; et al. 2011 update to the Society of Thoracic Surgeons and the Society of Cardiovascular Anesthesiologists blood conservation clinical practice guidelines. Ann. Thorac. Surg. 2011, 91, 944–982. [Google Scholar] [CrossRef]
- Boer, C.; Meesters, M.I.; Milojevic, M. Task force on patient blood management for adult cardiac surgery of the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Cardiothoracic Anaesthesiology (EACTA)—2017 EACTS/EACTA Guidelines on patient blood management for adult cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2018, 32, 88–120. [Google Scholar] [CrossRef] [Green Version]
- Isbister, J. Why should health professionals be concerned about blood management and blood conservation? Updates Blood Conserv. Transfus. Altern. 2005, 2, 3–7. [Google Scholar]
- WHO. Sixty-Third World Health Assembly. Availability, Safety and Quality of Blood Products. Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA63/A63_R12-en.pdf (accessed on 24 February 2021).
- Goodnough, L.T.; Shieh, L.; Hadhazy, E.; Cheng, N.; Khari, P.; Maggio, P. Improved blood utilization using real-time clinical decision support. Transfusion 2014, 54, 1358–1365. [Google Scholar] [CrossRef]
- Gross, I.; Seifert, B.; Hofmann, A.; Spahn, D.R. Patient blood management in cardiac surgery results in fewer transfusions and better outcome. Transfusion 2015, 55, 1075–1081. [Google Scholar] [CrossRef]
- Oliver, J.C.; Griffin, R.L.; Hannon, T.; Marques, M.B. The success of our patient blood management program depended on an institution-wide change in transfusion practices. Transfusion 2014, 54, 2617–2624. [Google Scholar] [CrossRef]
- Theusinger, O.M.; Kind, S.L.; Seifert, B.; Borgeat, L.; Gerber, C.; Spahn, D.R. Patient blood management in orthopaedic surgery: A four-year follow-up of transfusion requirements and blood loss from 2008 to 2011 at the Balgrist University Hospital in Zurich, Switzerland. Blood Transfus. 2014, 12, 195–203. [Google Scholar] [CrossRef] [Green Version]
- Australia National Blood Authority. National Patient Blood Management Guidelines Implementation Strategy 2013–2017. Available online: https://blood.gov.au/system/files/documents/pbm-guidelines-implementationstrategy-november.pdf (accessed on 24 February 2021).
- European Commission, Consumers, Health, Agriculture and Food Executive Agency. Building national programmes of Patient Blood Management (PBM) in the EU. In A Guide for Health Authorities; Publications Office of the European Union: Luxembourg, 2017. [Google Scholar]
- Meybohm, P.; Richards, T.; Isbister, J.; Hofmann, A.; Shander, A.; Goodnough, L.T.; Munoz, M.; Gombotz, H.; Weber, C.F.; Choorapoikayil, S.; et al. Patient Blood Management Bundles to Facilitate Implementation. Transfus. Med. Rev. 2017, 31, 62–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shander, A.; Goobie, S.M.; Warner, M.A.; Aapro, M.; Bisbe, E.; Perez-Calatayud, A.A.; Callum, J.; Cushing, M.M.; Dyer, W.B.; Erhard, J.; et al. Essential Role of Patient Blood Management in a Pandemic: A Call for Action. Anesth. Analg. 2020, 131, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, A.; Ozawa, S.; Farrugia, A.; Farmer, S.L.; Shander, A. Economic considerations on transfusion medicine and patient blood management. Best Pract. Res. Clin. Anaesthesiol. 2013, 27, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Kaserer, A.; Rossler, J.; Braun, J.; Farokhzad, F.; Pape, H.C.; Dutkowski, P.; Plass, A.; Horisberger, T.; Volbracht, J.; Manz, M.G.; et al. Impact of a Patient Blood Management monitoring and feedback programme on allogeneic blood transfusions and related costs. Anaesthesia 2019, 74, 1534–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehra, T.; Seifert, B.; Bravo-Reiter, S.; Wanner, G.; Dutkowski, P.; Holubec, T.; Moos, R.M.; Volbracht, J.; Manz, M.G.; Spahn, D.R. Implementation of a patient blood management monitoring and feedback program significantly reduces transfusions and costs. Transfusion 2015, 55, 2807–2815. [Google Scholar] [CrossRef]
- Spahn, D.R.; Theusinger, O.M.; Hofmann, A. Patient blood management is a win-win: A wake-up call. Br. J. Anaesth. 2012, 108, 889–892. [Google Scholar] [CrossRef] [Green Version]
- Burnes, B. The origins of Lewin’s Three-step Model of Change. J. Appl. Behav. Sci. 2020, 56, 32–59. [Google Scholar] [CrossRef]
- Cabana, M.D.; Rand, C.S.; Powe, N.R.; Wu, A.W.; Wilson, M.H.; Abboud, P.A.; Rubin, H.R. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999, 282, 1458–1465. [Google Scholar] [CrossRef]
- Meybohm, P.; Westphal, S.; Ravn, H.B.; Ranucci, M.; Agarwal, S.; Choorapoikayil, S.; Spahn, D.R.; Ahmed, A.B.; Froessler, B.; Zacharowski, K. Perioperative Anemia Management as Part of PBM in Cardiac Surgery—A Narrative Updated Review. J. Cardiothorac. Vasc. Anesth. 2020, 34, 1060–1073. [Google Scholar] [CrossRef]
- Klein, A.A.; Collier, T.J.; Brar, M.S.; Evans, C.; Hallward, G.; Fletcher, S.N.; Richards, T. The incidence and importance of anaemia in patients undergoing cardiac surgery in the UK—the first Association of Cardiothoracic Anaesthetists national audit. Anaesthesia 2016, 71, 627–635. [Google Scholar] [CrossRef]
- Kulier, A.; Levin, J.; Moser, R.; Rumpold-Seitlinger, G.; Tudor, I.C.; Snyder-Ramos, S.A.; Moehnle, P.; Mangano, D.T.; Investigators of the Multicenter Study of Perioperative Ischemia Research Group; Ischemia, R.; et al. Impact of preoperative anemia on outcome in patients undergoing coronary artery bypass graft surgery. Circulation 2007, 116, 471–479. [Google Scholar] [CrossRef] [Green Version]
- Munoz, M.; Gomez-Ramirez, S.; Campos, A.; Ruiz, J.; Liumbruno, G.M. Pre-operative anaemia: Prevalence, consequences and approaches to management. Blood Transfus. 2015, 13, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Von Heymann, C.; Kaufner, L.; Sander, M.; Spies, C.; Schmidt, K.; Gombotz, H.; Wernecke, K.D.; Balzer, F. Does the severity of preoperative anemia or blood transfusion have a stronger impact on long-term survival after cardiac surgery? J. Thorac. Cardiovasc. Surg. 2016, 152, 1412–1420. [Google Scholar] [CrossRef] [Green Version]
- Karkouti, K.; Wijeysundera, D.N.; Beattie, W.S. Risk associated with preoperative anemia in cardiac surgery: A multicenter cohort study. Circulation 2008, 117, 478–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munoz, M.; Gomez-Ramirez, S.; Kozek-Langeneker, S.; Shander, A.; Richards, T.; Pavia, J.; Kehlet, H.; Acheson, A.G.; Evans, C.; Raobaikady, R.; et al. ‘Fit to fly’: Overcoming barriers to preoperative haemoglobin optimization in surgical patients. Br. J. Anaesth. 2015, 115, 15–24. [Google Scholar] [CrossRef] [Green Version]
- Rogers, M.A.; Blumberg, N.; Heal, J.M.; Hicks, G.L., Jr. Increased risk of infection and mortality in women after cardiac surgery related to allogeneic blood transfusion. J. Womens Health 2007, 16, 1412–1420. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.A.; Blumberg, N.; Saint, S.K.; Kim, C.; Nallamothu, B.K.; Langa, K.M. Allogeneic blood transfusions explain increased mortality in women after coronary artery bypass graft surgery. Am. Heart J. 2006, 152, 1028–1034. [Google Scholar] [CrossRef]
- Bechtel, A.J.; Huffmyer, J.L. Gender Differences in Postoperative Outcomes After Cardiac Surgery. Anesthesiol. Clin. 2020, 38, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Munoz, M.; Acheson, A.G.; Auerbach, M.; Besser, M.; Habler, O.; Kehlet, H.; Liumbruno, G.M.; Lasocki, S.; Meybohm, P.; Rao Baikady, R.; et al. International consensus statement on the peri-operative management of anaemia and iron deficiency. Anaesthesia 2017, 72, 233–247. [Google Scholar] [CrossRef] [Green Version]
- Yoo, Y.C.; Shim, J.K.; Kim, J.C.; Jo, Y.Y.; Lee, J.H.; Kwak, Y.L. Effect of single recombinant human erythropoietin injection on transfusion requirements in preoperatively anemic patients undergoing valvular heart surgery. Anesthesiology 2011, 115, 929–937. [Google Scholar] [CrossRef]
- Spahn, D.R.; Schoenrath, F.; Spahn, G.H.; Seifert, B.; Stein, P.; Theusinger, O.M.; Kaserer, A.; Hegemann, I.; Hofmann, A.; Maisano, F.; et al. Effect of ultra-short-term treatment of patients with iron deficiency or anaemia undergoing cardiac surgery: A prospective randomised trial. Lancet 2019, 393, 2201–2212. [Google Scholar] [CrossRef]
- Ranucci, M.; Pavesi, M.; Pistuddi, V.; Baryshnikova, E. Preoperative Anemia Correction in Cardiac Surgery: A Propensity-Matched Study. J. Cardiothorac. Vasc. Anesth. 2021, 35, 874–881. [Google Scholar] [CrossRef]
- Beard, J.L. Iron biology in immune function, muscle metabolism and neuronal functioning. J. Nutr. 2001, 131, 568S–579S. [Google Scholar] [CrossRef]
- Tacke, F.; Nuraldeen, R.; Koch, A.; Strathmann, K.; Hutschenreuter, G.; Trautwein, C.; Strnad, P. Iron Parameters Determine the Prognosis of Critically Ill Patients. Crit. Care Med. 2016, 44, 1049–1058. [Google Scholar] [CrossRef]
- Von Haehling, S.; Ebner, N.; Evertz, R.; Ponikowski, P.; Anker, S.D. Iron Deficiency in Heart Failure: An Overview. JACC Heart Fail. 2019, 7, 36–46. [Google Scholar] [CrossRef]
- Rossler, J.; Schoenrath, F.; Seifert, B.; Kaserer, A.; Spahn, G.H.; Falk, V.; Spahn, D.R. Iron deficiency is associated with higher mortality in patients undergoing cardiac surgery: A prospective study. Br. J. Anaesth. 2020, 124, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Johnson-Wimbley, T.D.; Graham, D.Y. Diagnosis and management of iron deficiency anemia in the 21st century. Therap. Adv. Gastroenterol. 2011, 4, 177–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganzoni, A.M. Intravenous iron-dextran: Therapeutic and experimental possibilities. Schweiz. Med. Wochenschr. 1970, 100, 301–303. [Google Scholar] [PubMed]
- Weltert, L.; D’Alessandro, S.; Nardella, S.; Girola, F.; Bellisario, A.; Maselli, D.; De Paulis, R. Preoperative very short-term, high-dose erythropoietin administration diminishes blood transfusion rate in off-pump coronary artery bypass: A randomized blind controlled study. J. Thorac. Cardiovasc. Surg. 2010, 139, 621–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weltert, L.; Rondinelli, B.; Bello, R.; Falco, M.; Bellisario, A.; Maselli, D.; Turani, F.; De Paulis, R.; Pierelli, L. A single dose of erythropoietin reduces perioperative transfusions in cardiac surgery: Results of a prospective single-blind randomized controlled trial. Transfusion 2015, 55, 1644–1654. [Google Scholar] [CrossRef]
- Stowell, C.P.; Jones, S.C.; Enny, C.; Langholff, W.; Leitz, G. An open-label, randomized, parallel-group study of perioperative epoetin alfa versus standard of care for blood conservation in major elective spinal surgery: Safety analysis. Spine 2009, 34, 2479–2485. [Google Scholar] [CrossRef] [PubMed]
- De Andrade, J.R.; Jove, M.; Landon, G.; Frei, D.; Guilfoyle, M.; Young, D.C. Baseline hemoglobin as a predictor of risk of transfusion and response to Epoetin alfa in orthopedic surgery patients. Am. J. Orthop. 1996, 25, 533–542. [Google Scholar]
- Corwin, H.L.; Gettinger, A.; Fabian, T.C.; May, A.; Pearl, R.G.; Heard, S.; An, R.; Bowers, P.J.; Burton, P.; Klausner, M.A.; et al. Efficacy and safety of epoetin alfa in critically ill patients. N. Engl. J. Med. 2007, 357, 965–976. [Google Scholar] [CrossRef] [Green Version]
- Kei, T.; Mistry, N.; Curley, G.; Pavenski, K.; Shehata, N.; Tanzini, R.M.; Gauthier, M.F.; Thorpe, K.; Schweizer, T.A.; Ward, S.; et al. Efficacy and safety of erythropoietin and iron therapy to reduce red blood cell transfusion in surgical patients: A systematic review and meta-analysis. Can. J. Anaesth. 2019, 66, 716–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozek-Langenecker, S.A.; Ahmed, A.B.; Afshari, A.; Albaladejo, P.; Aldecoa, C.; Barauskas, G.; De Robertis, E.; Faraoni, D.; Filipescu, D.C.; Fries, D.; et al. Management of severe perioperative bleeding: Guidelines from the European Society of Anaesthesiology: First update 2016. Eur. J. Anaesthesiol. 2017, 34, 332–395. [Google Scholar] [CrossRef] [Green Version]
- Bonhomme, F.; Ajzenberg, N.; Schved, J.F.; Molliex, S. Pre-interventional haemostatic assessment: Guidelines from the French Society of Anaesthesia and Intensive Care. Eur. J. Anaesthesiol. 2013, 30, 142–162. [Google Scholar] [CrossRef] [PubMed]
- Bryson, G.L.; Wyand, A.; Bragg, P.R. Preoperative testing is inconsistent with published guidelines and rarely changes management. Can. J. Anaesth. 2006, 53, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Elbatarny, M.; Mollah, S.; Grabell, J.; Bae, S.; Deforest, M.; Tuttle, A.; Hopman, W.; Clark, D.S.; Mauer, A.C.; Bowman, M.; et al. Normal range of bleeding scores for the ISTH-BAT: Adult and pediatric data from the merging project. Haemophilia 2014, 20, 831–835. [Google Scholar] [CrossRef]
- Bonhomme, F.; Boehlen, F.; Clergue, F.; de Moerloose, P. Preoperative hemostatic assessment: A new and simple bleeding questionnaire. Can. J. Anaesth. 2016, 63, 1007–1015. [Google Scholar] [CrossRef]
- Sousa-Uva, M.; Head, S.J.; Milojevic, M.; Collet, J.P.; Landoni, G.; Castella, M.; Dunning, J.; Gudbjartsson, T.; Linker, N.J.; Sandoval, E.; et al. 2017 EACTS Guidelines on perioperative medication in adult cardiac surgery. Eur. J. Cardiothorac. Surg. 2018, 53, 5–33. [Google Scholar] [CrossRef] [Green Version]
- Douketis, J.D.; Berger, P.B.; Dunn, A.S.; Jaffer, A.K.; Spyropoulos, A.C.; Becker, R.C.; Ansell, J. The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2008, 133, 299S–339S. [Google Scholar] [CrossRef] [Green Version]
- Douketis, J.D.; Spyropoulos, A.C.; Duncan, J.; Carrier, M.; Le Gal, G.; Tafur, A.J.; Vanassche, T.; Verhamme, P.; Shivakumar, S.; Gross, P.L.; et al. Perioperative Management of Patients with Atrial Fibrillation Receiving a Direct Oral Anticoagulant. JAMA Intern. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Auer, J.; Huber, K.; Granger, C.B. Interruption of non-vitamin K antagonist anticoagulants in patients undergoing planned invasive procedures: How long is long enough? Eur. Heart J. 2017, 38, 2440–2443. [Google Scholar] [CrossRef] [PubMed]
- Albaladejo, P.; Bonhomme, F.; Blais, N.; Collet, J.P.; Faraoni, D.; Fontana, P.; Godier, A.; Llau, J.; Longrois, D.; Marret, E.; et al. Management of direct oral anticoagulants in patients undergoing elective surgeries and invasive procedures: Updated guidelines from the French Working Group on Perioperative Hemostasis (GIHP)–September 2015. Anaesth. Crit. Care Pain Med. 2017, 36, 73–76. [Google Scholar] [CrossRef]
- Hornor, M.A.; Duane, T.M.; Ehlers, A.P.; Jensen, E.H.; Brown, P.S., Jr.; Pohl, D.; da Costa, P.M.; Ko, C.Y.; Laronga, C. American College of Surgeons’ Guidelines for the Perioperative Management of Antithrombotic Medication. J. Am. Coll. Surg. 2018, 227, 521–536.e521. [Google Scholar] [CrossRef]
- Keeling, D.; Tait, R.C.; Watson, H. Peri-operative management of anticoagulation and antiplatelet therapy. Br. J. Haematol. 2016, 175, 602–613. [Google Scholar] [CrossRef] [PubMed]
- Prisco, D.; Ageno, W.; Becattini, C.; D’Angelo, A.; Davi, G.; De Cristofaro, R.; Dentali, F.; Di Minno, G.; Falanga, A.; Gussoni, G.; et al. Italian intersociety consensus on DOAC use in internal medicine. Intern. Emerg. Med. 2017, 12, 387–406. [Google Scholar] [CrossRef]
- Steffel, J.; Verhamme, P.; Potpara, T.S.; Albaladejo, P.; Antz, M.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur. Heart J. 2018, 39, 1330–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canada, T. NOACS/DOACS Perioperative Management. Available online: https://thrombosiscanada.ca/wp-uploads/uploads/2021/01/22.-NOACs-DOACs-Perioperative-Management-17May2020.pdf (accessed on 28 February 2021).
- Riess, H.; Prandoni, P.; Harder, S.; Kreher, S.; Bauersachs, R. Direct oral anticoagulants for the treatment of venous thromboembolism in cancer patients: Potential for drug-drug interactions. Crit. Rev. Oncol. Hematol. 2018, 132, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Godier, A.; Martin, A.C.; Leblanc, I.; Mazoyer, E.; Horellou, M.H.; Ibrahim, F.; Flaujac, C.; Golmard, J.L.; Rosencher, N.; Gouin-Thibault, I. Peri-procedural management of dabigatran and rivaroxaban: Duration of anticoagulant discontinuation and drug concentrations. Thromb. Res. 2015, 136, 763–768. [Google Scholar] [CrossRef]
- Testa, S.; Tripodi, A.; Legnani, C.; Pengo, V.; Abbate, R.; Dellanoce, C.; Carraro, P.; Salomone, L.; Paniccia, R.; Paoletti, O.; et al. Plasma levels of direct oral anticoagulants in real life patients with atrial fibrillation: Results observed in four anticoagulation clinics. Thromb. Res. 2016, 137, 178–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaw, J.R.; Li, N.; Vanassche, T.; Coppens, M.; Spyropoulos, A.C.; Syed, S.; Radwi, M.; Duncan, J.; Schulman, S.; Douketis, J.D. Predictors of preprocedural direct oral anticoagulant levels in patients having an elective surgery or procedure. Blood Adv. 2020, 4, 3520–3527. [Google Scholar] [CrossRef]
- Dubois, V.; Dincq, A.S.; Douxfils, J.; Ickx, B.; Samama, C.M.; Dogne, J.M.; Gourdin, M.; Chatelain, B.; Mullier, F.; Lessire, S. Perioperative management of patients on direct oral anticoagulants. Thromb. J. 2017, 15, 14. [Google Scholar] [CrossRef]
- Hongo, R.H.; Ley, J.; Dick, S.E.; Yee, R.R. The effect of clopidogrel in combination with aspirin when given before coronary artery bypass grafting. J. Am. Coll. Cardiol. 2002, 40, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [Green Version]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Juni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–260. [Google Scholar] [CrossRef]
- Schomig, A. Ticagrelor–is there need for a new player in the antiplatelet-therapy field? N. Engl. J. Med. 2009, 361, 1108–1111. [Google Scholar] [CrossRef]
- Mahla, E.; Suarez, T.A.; Bliden, K.P.; Rehak, P.; Metzler, H.; Sequeira, A.J.; Cho, P.; Sell, J.; Fan, J.; Antonino, M.J.; et al. Platelet function measurement-based strategy to reduce bleeding and waiting time in clopidogrel-treated patients undergoing coronary artery bypass graft surgery: The timing based on platelet function strategy to reduce clopidogrel-associated bleeding related to CABG (TARGET-CABG) study. Circ. Cardiovasc. Interv. 2012, 5, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Ranucci, M.; Baryshnikova, E.; Soro, G.; Ballotta, A.; De Benedetti, D.; Conti, D. Multiple electrode whole-blood aggregometry and bleeding in cardiac surgery patients receiving thienopyridines. Ann. Thorac. Surg. 2011, 91, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Ranucci, M.; Colella, D.; Baryshnikova, E.; Di Dedda, U. Effect of preoperative P2Y12 and thrombin platelet receptor inhibition on bleeding after cardiac surgery. Br. J. Anaesth. 2014, 113, 970–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunst, G.; Milojevic, M.; Boer, C.; De Somer, F.M.; Gudbjartsson, T.; Goor, J.V.D.; Jones, T.J.; Lomivorotov, V.; Merkle, F.; Ranucci, M.; et al. 2019 EACTS/EACTA/EBCP guidelines on cardiopulmonary bypass in adult cardiac surgery. Br. J. Anaesth. 2019, 123, 713–757. [Google Scholar] [CrossRef]
- Anastasiadis, K.; Argiriadou, H.; Deliopoulos, A.; Antonitsis, P. Minimal invasive extracorporeal circulation (MiECC): The state-of-the-art in perfusion. J. Thorac. Dis. 2019, 11, S1507–S1514. [Google Scholar] [CrossRef] [PubMed]
- Anastasiadis, K.; Murkin, J.; Antonitsis, P.; Bauer, A.; Ranucci, M.; Gygax, E.; Schaarschmidt, J.; Fromes, Y.; Philipp, A.; Eberle, B.; et al. Use of minimal invasive extracorporeal circulation in cardiac surgery: Principles, definitions and potential benefits. A position paper from the Minimal invasive Extra-Corporeal Technologies international Society (MiECTiS). Interact. Cardiovasc. Thorac. Surg. 2016, 22, 647–662. [Google Scholar] [CrossRef]
- Anastasiadis, K.; Antonitsis, P.; Haidich, A.B.; Argiriadou, H.; Deliopoulos, A.; Papakonstantinou, C. Use of minimal extracorporeal circulation improves outcome after heart surgery; a systematic review and meta-analysis of randomized controlled trials. Int. J. Cardiol. 2013, 164, 158–169. [Google Scholar] [CrossRef]
- Aziz, K.A.; Masood, O.; Hoschtitzky, J.A.; Ronald, A. Does use of the Hepcon point-of-care coagulation monitor to optimise heparin and protamine dosage for cardiopulmonary bypass decrease bleeding and blood and blood product requirements in adult patients undergoing cardiac surgery? Interact. Cardiovasc. Thorac. Surg. 2006, 5, 469–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoenicka, M.; Rupp, P.; Muller-Eising, K.; Deininger, S.; Kunert, A.; Liebold, A.; Gorki, H. Anticoagulation management during multivessel coronary artery bypass grafting: A randomized trial comparing individualized heparin management and conventional hemostasis management. J. Thromb. Haemost. 2015, 13, 1196–1206. [Google Scholar] [CrossRef]
- Noui, N.; Zogheib, E.; Walczak, K.; Werbrouck, A.; Amar, A.B.; Dupont, H.; Caus, T.; Remadi, J.P. Anticoagulation monitoring during extracorporeal circulation with the Hepcon/HMS device. Perfusion 2012, 27, 214–220. [Google Scholar] [CrossRef]
- Pappalardo, F.; Franco, A.; Crescenzi, G.; De Simone, F.; Torracca, L.; Zangrillo, A. Anticoagulation management in patients undergoing open heart surgery by activated clotting time and whole blood heparin concentration. Perfusion 2006, 21, 285–290. [Google Scholar] [CrossRef]
- Wang, D.S.; Mazer, C.D.; Orser, B.A. Tranexamic Acid in Patients Undergoing Coronary-Artery Surgery. N. Engl. J. Med. 2017, 376, 1891–1892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vonk, A.B.; Veerhoek, D.; van den Brom, C.E.; van Barneveld, L.J.; Boer, C. Individualized heparin and protamine management improves rotational thromboelastometric parameters and postoperative hemostasis in valve surgery. J. Cardiothorac. Vasc. Anesth. 2014, 28, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, B.; Bushnaq, H.; Kraus, F.B.; Raspe, C.; Simm, A.; Silber, R.E.; Ludwig-Kraus, B. Immediate effects of individualized heparin and protamine management on hemostatic activation and platelet function in adult patients undergoing cardiac surgery with tranexamic acid antifibrinolytic therapy. Perfusion 2013, 28, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Scala, E.; Marcucci, C. Massive Hemorrhage: The Role of Whole Blood Viscoelastic Assays. Hamostaseologie 2020, 40, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Karkouti, K.; Callum, J.; Wijeysundera, D.N.; Rao, V.; Crowther, M.; Grocott, H.P.; Pinto, R.; Scales, D.C.; Investigators, T. Point-of-Care Hemostatic Testing in Cardiac Surgery: A Stepped-Wedge Clustered Randomized Controlled Trial. Circulation 2016, 134, 1152–1162. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Zhao, Q.; Yang, K.; Jiang, L.; Yu, J. Thromboelastography or rotational thromboelastometry for bleeding management in adults undergoing cardiac surgery: A systematic review with meta-analysis and trial sequential analysis. J. Thorac. Dis. 2019, 11, 1170–1181. [Google Scholar] [CrossRef]
- Lodewyks, C.; Heinrichs, J.; Grocott, H.P.; Karkouti, K.; Romund, G.; Arora, R.C.; Tangri, N.; Rabbani, R.; Abou-Setta, A.; Zarychanski, R. Point-of-care viscoelastic hemostatic testing in cardiac surgery patients: A systematic review and meta-analysis. Can. J. Anaesth. 2018, 65, 1333–1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wikkelso, A.; Wetterslev, J.; Moller, A.M.; Afshari, A. Thromboelastography (TEG) or thromboelastometry (ROTEM) to monitor haemostatic treatment versus usual care in adults or children with bleeding. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [Green Version]
- Bolliger, D.; Lancé, M.D. Factor Concentrate-Based Approaches to Blood Conservation in Cardiac Surgery: European Perspectives in 2020. Curr. Anesthesiol. Rep. 2020, 10, 137–146. [Google Scholar] [CrossRef]
- Li, J.Y.; Gong, J.; Zhu, F.; Moodie, J.; Newitt, A.; Uruthiramoorthy, L.; Cheng, D.; Martin, J. Fibrinogen Concentrate in Cardiovascular Surgery: A Meta-analysis of Randomized Controlled Trials. Anesth. Analg. 2018, 127, 612–621. [Google Scholar] [CrossRef]
- Erdoes, G.; Koster, A.; Meesters, M.I.; Ortmann, E.; Bolliger, D.; Baryshnikova, E.; Ahmed, A.; Lance, M.D.; Ravn, H.B.; Ranucci, M.; et al. The role of fibrinogen and fibrinogen concentrate in cardiac surgery: An international consensus statement from the Haemostasis and Transfusion Scientific Subcommittee of the European Association of Cardiothoracic Anaesthesiology. Anaesthesia 2019, 74, 1589–1600. [Google Scholar] [CrossRef]
- Nemeth, E.; Varga, T.; Soltesz, A.; Racz, K.; Csikos, G.; Berzsenyi, V.; Tamaska, E.; Lang, Z.; Molnar, G.; Benke, K.; et al. Perioperative Factor Concentrate Use is Associated with More Beneficial Outcomes and Reduced Complication Rates Compared with a Pure Blood Product-Based Strategy in Patients Undergoing Elective Cardiac Surgery: A Propensity Score-Matched Cohort Study. J. Cardiothorac. Vasc. Anesth. 2021. [Google Scholar] [CrossRef]
- Simpson, E.; Lin, Y.; Stanworth, S.; Birchall, J.; Doree, C.; Hyde, C. Recombinant factor VIIa for the prevention and treatment of bleeding in patients without haemophilia. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef] [Green Version]
- Tonz, M.; Mihaljevic, T.; von Segesser, L.K.; Schmid, E.R.; Joller-Jemelka, H.I.; Pei, P.; Turina, M.I. Normothermia versus hypothermia during cardiopulmonary bypass: A randomized, controlled trial. Ann. Thorac. Surg. 1995, 59, 137–143. [Google Scholar] [CrossRef]
- Van Poucke, S.; Stevens, K.; Marcus, A.E.; Lance, M. Hypothermia: Effects on platelet function and hemostasis. Thromb. J. 2014, 12, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortmann, E.; Klein, A.A.; Sharples, L.D.; Walsh, R.; Jenkins, D.P.; Luddington, R.J.; Besser, M.W. Point-of-care assessment of hypothermia and protamine-induced platelet dysfunction with multiple electrode aggregometry (Multiplate(R)) in patients undergoing cardiopulmonary bypass. Anesth. Analg. 2013, 116, 533–540. [Google Scholar] [CrossRef]
- Rohrer, M.J.; Natale, A.M. Effect of hypothermia on the coagulation cascade. Crit. Care Med. 1992, 20, 1402–1405. [Google Scholar] [CrossRef]
- Dirkmann, D.; Hanke, A.A.; Gorlinger, K.; Peters, J. Hypothermia and acidosis synergistically impair coagulation in human whole blood. Anesth. Analg. 2008, 106, 1627–1632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campos, J.M.; Paniagua, P. Hypothermia during cardiac surgery. Best Pract. Res. Clin. Anaesthesiol. 2008, 22, 695–709. [Google Scholar] [CrossRef] [PubMed]
- Saad, H.; Aladawy, M. Temperature management in cardiac surgery. Glob. Cardiol. Sci. Pract. 2013, 2013, 44–62. [Google Scholar] [CrossRef]
- Touati, G.D.; Marticho, P.; Farag, M.; Carmi, D.; Szymanski, C.; Barry, M.; Trojette, F.; Caus, T. Totally normothermic aortic arch replacement without circulatory arrest. Eur. J. Cardiothorac. Surg. 2007, 32, 263–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paparella, D.; Semeraro, F.; Scrascia, G.; Galeone, A.; Ammollo, C.T.; Kounakis, G.; de Luca Tupputi Schinosa, L.; Semeraro, N.; Colucci, M. Coagulation-fibrinolysis changes during off-pump bypass: Effect of two heparin doses. Ann. Thorac. Surg. 2010, 89, 421–427. [Google Scholar] [CrossRef]
- Deppe, A.C.; Arbash, W.; Kuhn, E.W.; Slottosch, I.; Scherner, M.; Liakopoulos, O.J.; Choi, Y.H.; Wahlers, T. Current evidence of coronary artery bypass grafting off-pump versus on-pump: A systematic review with meta-analysis of over 16,900 patients investigated in randomized controlled trialsdagger. Eur. J. Cardiothorac. Surg. 2016, 49, 1031–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puskas, J.D.; Martin, J.; Cheng, D.C.; Benussi, S.; Bonatti, J.O.; Diegeler, A.; Ferdinand, F.D.; Kieser, T.M.; Lamy, A.; Mack, M.J.; et al. ISMICS Consensus Conference and Statements of Randomized Controlled Trials of Off-Pump versus Conventional Coronary Artery Bypass Surgery. Innovations 2015, 10, 219–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaefi, S.; Mittel, A.; Loberman, D.; Ramakrishna, H. Off-Pump Versus On-Pump Coronary Artery Bypass Grafting-A Systematic Review and Analysis of Clinical Outcomes. J. Cardiothorac. Vasc. Anesth. 2019, 33, 232–244. [Google Scholar] [CrossRef] [PubMed]
- Diegeler, A.; Borgermann, J.; Kappert, U.; Breuer, M.; Boning, A.; Ursulescu, A.; Rastan, A.; Holzhey, D.; Treede, H.; Riess, F.C.; et al. Off-pump versus on-pump coronary-artery bypass grafting in elderly patients. N. Engl. J. Med. 2013, 368, 1189–1198. [Google Scholar] [CrossRef] [Green Version]
- Lamy, A.; Devereaux, P.J.; Prabhakaran, D.; Taggart, D.P.; Hu, S.; Paolasso, E.; Straka, Z.; Piegas, L.S.; Akar, A.R.; Jain, A.R.; et al. Off-pump or on-pump coronary-artery bypass grafting at 30 days. N. Engl. J. Med. 2012, 366, 1489–1497. [Google Scholar] [CrossRef] [Green Version]
- Flom-Halvorsen, H.I.; Ovrum, E.; Oystese, R.; Brosstad, F. Quality of intraoperative autologous blood withdrawal used for retransfusion after cardiopulmonary bypass. Ann. Thorac. Surg. 2003, 76, 744–748. [Google Scholar] [CrossRef]
- Loubser, P.G. Clot formation in a blood-collection bag used for acute normovolemic hemodilution. J. Cardiothorac. Vasc. Anesth. 2008, 22, 801–802. [Google Scholar] [CrossRef]
- Barile, L.; Fominskiy, E.; Di Tomasso, N.; Alpizar Castro, L.E.; Landoni, G.; De Luca, M.; Bignami, E.; Sala, A.; Zangrillo, A.; Monaco, F. Acute Normovolemic Hemodilution Reduces Allogeneic Red Blood Cell Transfusion in Cardiac Surgery: A Systematic Review and Meta-analysis of Randomized Trials. Anesth. Analg. 2017, 124, 743–752. [Google Scholar] [CrossRef]
- Hajjar, L.A.; Vincent, J.L.; Galas, F.R.; Nakamura, R.E.; Silva, C.M.; Santos, M.H.; Fukushima, J.; Kalil Filho, R.; Sierra, D.B.; Lopes, N.H.; et al. Transfusion requirements after cardiac surgery: The TRACS randomized controlled trial. JAMA 2010, 304, 1559–1567. [Google Scholar] [CrossRef] [PubMed]
- Mazer, C.D.; Whitlock, R.P.; Fergusson, D.A.; Hall, J.; Belley-Cote, E.; Connolly, K.; Khanykin, B.; Gregory, A.J.; de Medicis, E.; McGuinness, S.; et al. Restrictive or Liberal Red-Cell Transfusion for Cardiac Surgery. N. Engl. J. Med. 2017, 377, 2133–2144. [Google Scholar] [CrossRef] [PubMed]
- Murphy, G.J.; Pike, K.; Rogers, C.A.; Wordsworth, S.; Stokes, E.A.; Angelini, G.D.; Reeves, B.C.; Investigators, T.I. Liberal or restrictive transfusion after cardiac surgery. N. Engl. J. Med. 2015, 372, 997–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shehata, N.; Mistry, N.; da Costa, B.R.; Pereira, T.V.; Whitlock, R.; Curley, G.F.; Scott, D.A.; Hare, G.M.T.; Juni, P.; Mazer, C.D. Restrictive compared with liberal red cell transfusion strategies in cardiac surgery: A meta-analysis. Eur. Heart J. 2019, 40, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Li, F.; Hu, H.; Liu, B.; Zheng, S.; Yang, L.; Gao, R.; Li, Y.; Xi, R.; He, J. Anemia and perioperative mortality in non-cardiac surgery patients: A secondary analysis based on a single-center retrospective study. BMC Anesthesiol. 2020, 20, 112. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Preoperative patient blood management for cardiac surgery | |
| Identify and correct anemia to optimize red blood cells mass |
|
| Optimize coagulation |
|
| Intraoperative patient blood management for cardiac surgery | |
| Optimize coagulation |
|
| CPB management |
|
| Surgical management |
|
| Postoperative patient blood management in cardiac surgery | |
| Harness anemia tolerance Apply appropriate transfusion triggers |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rancati, V.; Scala, E.; Ltaief, Z.; Gunga, M.Z.; Kirsch, M.; Rosner, L.; Marcucci, C. Challenges in Patient Blood Management for Cardiac Surgery: A Narrative Review. J. Clin. Med. 2021, 10, 2454. https://doi.org/10.3390/jcm10112454
Rancati V, Scala E, Ltaief Z, Gunga MZ, Kirsch M, Rosner L, Marcucci C. Challenges in Patient Blood Management for Cardiac Surgery: A Narrative Review. Journal of Clinical Medicine. 2021; 10(11):2454. https://doi.org/10.3390/jcm10112454
Chicago/Turabian StyleRancati, Valentina, Emmanuelle Scala, Zied Ltaief, Mohamed Ziyad Gunga, Matthias Kirsch, Lorenzo Rosner, and Carlo Marcucci. 2021. "Challenges in Patient Blood Management for Cardiac Surgery: A Narrative Review" Journal of Clinical Medicine 10, no. 11: 2454. https://doi.org/10.3390/jcm10112454