
Long-Term Hypermethylation of FcγR2B in Leukocytes of Patients with Kawasaki Disease


 , , ,
, , , 
Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Measurement of DNA Methylation Levels of FcγR2B Promoter Regions by Bisulfite Pyrosequencing
2.3. Cell Culture
2.4. Statistical Analysis
3. Results
3.1. Study Subjects
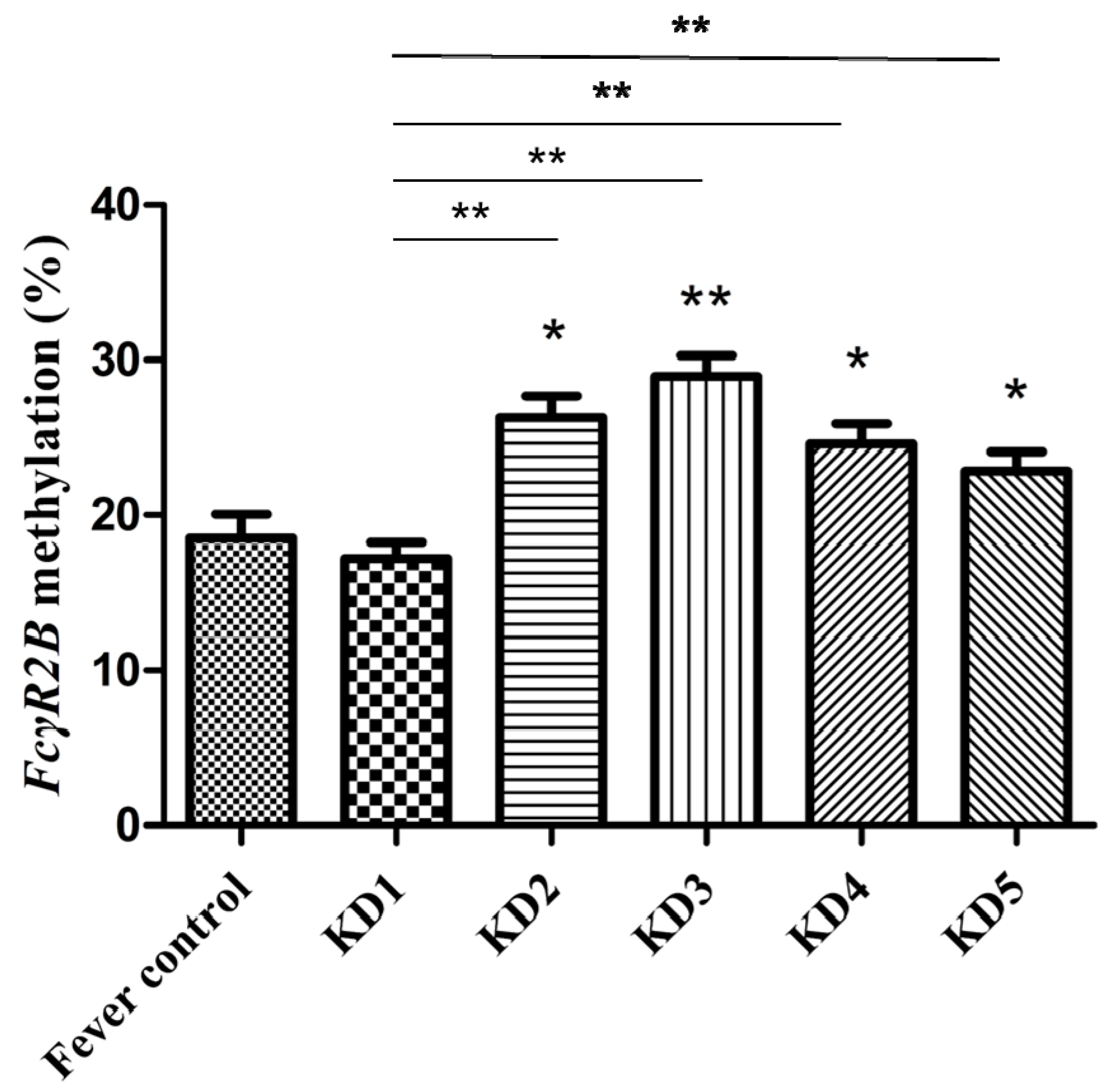
3.2. Methylation Levels of FcγR2B Promoter Regions on Leukocytes in Different Stages of Kawasaki Disease
3.3. FcγR2B Hypomethylation with IVIG Resistance in Kawasaki Disease
3.4. Association between FcγR2B Methylation and Blood Parameters in Kawasaki Disease
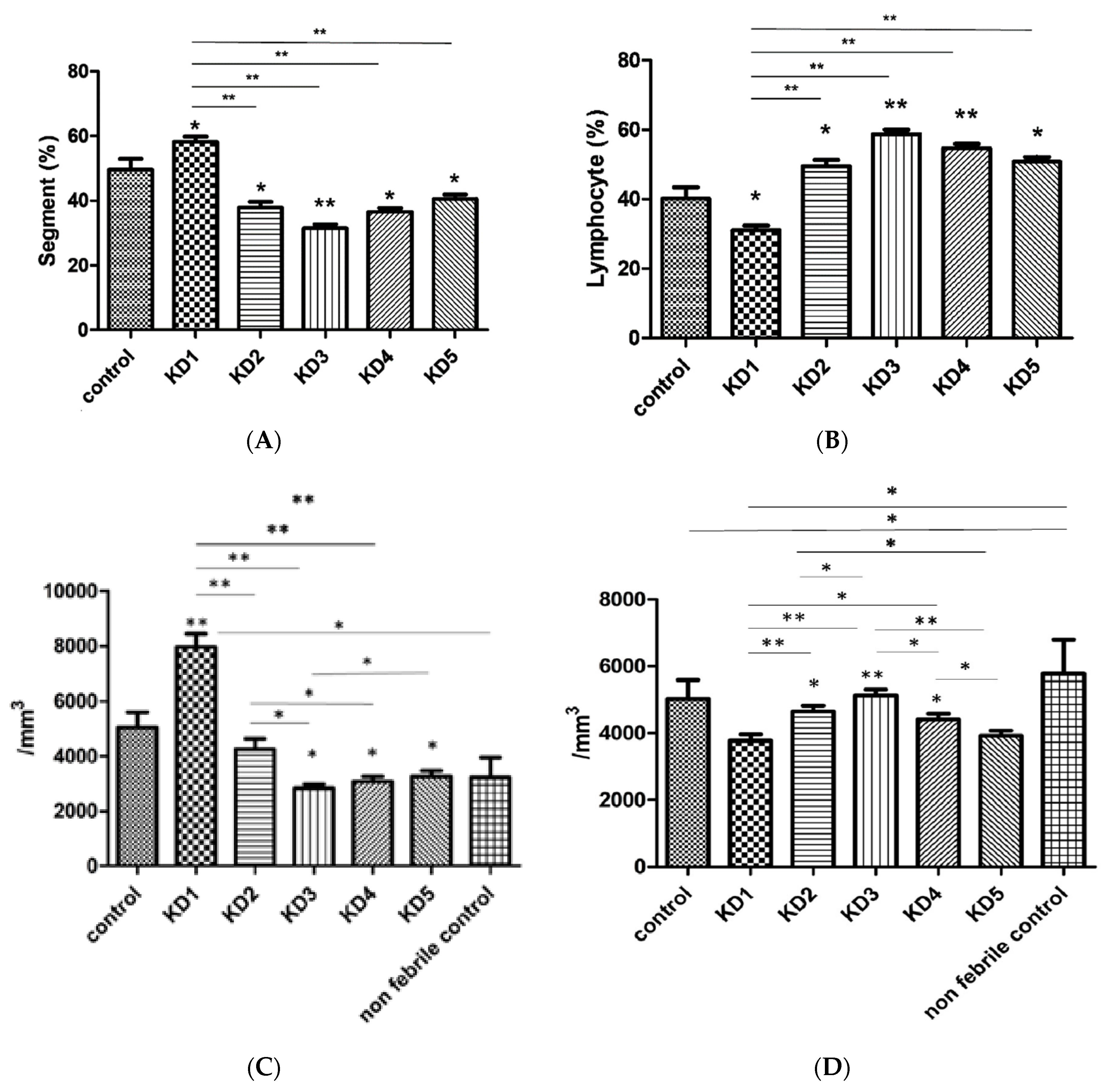
3.5. Hematological Changes in Kawasaki Disease
3.6. IVIG Regulates FcγR2B Methylation in THP-1 Cells
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kawasaki, T.; Kosaki, F.; Okawa, S.; Shigematsu, I.; Yanagawa, H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics 1974, 54, 271–276. [Google Scholar] [PubMed]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals from the American Heart Association. Circulation 2017, 135, e927–e999. [Google Scholar] [CrossRef] [PubMed]
- Nakatani, K.; Takeshita, S.; Tsujimoto, H.; Kawamura, Y.; Kawase, H.; Sekine, I. Regulation of the expression of Fc gamma receptor on circulating neutrophils and monocytes in Kawasaki disease. Clin. Exp. Immunol. 1999, 117, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.-S.; Guo, M.M.-H.; Lo, M.-H.; Kuo, H.-C. Identification of increased expression of activating Fc receptors and novel findings regarding distinct IgE and IgM receptors in Kawasaki disease. Pediatr. Res. 2021, 89, 191–197. [Google Scholar] [CrossRef]
- Smith, K.G.; Clatworthy, M.R. FcgammaRIIB in autoimmunity and infection: Evolutionary and therapeutic implications. Nat. Rev. Immunol. 2010, 10, 328–343. [Google Scholar] [CrossRef] [Green Version]
- Jhou, J.P.; Chen, S.J.; Huang, H.Y.; Lin, W.W.; Huang, D.Y.; Tzeng, S.J. Upregulation of FcgammaRIIB by resveratrol via NF-kappaB activation reduces B-cell numbers and ameliorates lupus. Exp. Mol. Med. 2017, 49, 144. [Google Scholar] [CrossRef] [Green Version]
- Xia, Y.; Tian, X.; Li, Q.; Wang, G.; Li, C.; Yang, J. Expression of FcRs on monocytes among Kawasaki disease patients with coronary artery lesions. Int. Immunopharmacol. 2017, 45, 1–5. [Google Scholar] [CrossRef]
- Anthony, R.M.; Kobayashi, T.; Wermeling, F.; Ravetch, J.V. Intravenous gammaglobulin suppresses inflammation through a novel T(H)2 pathway. Nature 2011, 475, 110–113. [Google Scholar] [CrossRef]
- Shrestha, S.; Wiener, H.W.; Olson, A.K.; Edberg, J.C.; Bowles, N.E.; Patel, H.; Portman, M.A. Functional FCGR2B gene variants influence intravenous immunoglobulin response in patients with Kawasaki disease. J. Allergy Clin. Immunol. 2011, 128, 677–680.e1. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Ptacek, T.S.; Brown, E.E.; Edberg, J.C. Fcγ receptors: Structure, function and role as genetic risk factors in SLE. Genes Immun. 2009, 10, 380–389. [Google Scholar] [CrossRef] [Green Version]
- Su, K.; Wu, J.; Edberg, J.C.; Li, X.; Ferguson, P.; Cooper, G.S.; Langefeld, C.D.; Kimberly, R.P. A promoter haplotype of the immunoreceptor tyrosine-based inhibitory motif-bearing FcgammaRIIb alters receptor expression and associates with autoimmunity. I. Regulatory FCGR2B polymorphisms and their association with systemic lupus erythematosus. J. Immunol. 2004, 172, 7186–7191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, L.S.; Lo, M.H.; Li, S.C.; Yang, M.Y.; Hsieh, K.S.; Kuo, H.C. The effect of FcgammaRIIA and FcgammaRIIB on coronary artery lesion formation and intravenous immunoglobulin treatment responses in children with Kawasaki disease. Oncotarget 2017, 8, 2044–2052. [Google Scholar] [CrossRef] [Green Version]
- Ichiyama, T.; Ueno, Y.; Hasegawa, M.; Ishikawa, Y.; Matsubara, T.; Furukawa, S. Intravenous immunoglobulin does not increase FcgammaRIIB expression on monocytes/macrophages during acute Kawasaki disease. Rheumatology 2005, 44, 314–317. [Google Scholar] [CrossRef] [Green Version]
- Kuo, H.-C.; Chang, J.-C.; Kuo, H.-C.; Yu, H.-R.; Wang, C.-L.; Lee, C.-P.; Huang, L.-T.; Yang, K.D. Identification of an Association Between Genomic Hypomethylation ofFCGR2Aand Susceptibility to Kawasaki Disease and Intravenous Immunoglobulin Resistance by DNA Methylation Array. Arthritis Rheumatol. 2014, 67, 828–836. [Google Scholar] [CrossRef]
- Kuo, H.-C.; Chang, W.-C.; Yang, K.D.; Yu, H.-R.; Wang, C.-L.; Ho, S.-C.; Yang, C.-Y. Kawasaki disease and subsequent risk of allergic diseases: A population-based matched cohort study. BMC Pediatr. 2013, 13, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, P.-Y.; Huang, Y.-H.; Guo, M.M.-H.; Chang, L.-S.; Kuo, H.-C. Kawasaki Disease and Allergic Diseases. Front. Pediatr. 2021, 8, 614386. [Google Scholar] [CrossRef]
- Swamy, R.S.; Reshamwala, N.; Hunter, T.; Vissamsetti, S.; Santos, C.B.; Baroody, F.M.; Hwang, P.H.; Hoyte, E.G.; Garcia, M.A.; Nadeau, K.C. Epigenetic modifications and improved regulatory T-cell function in subjects undergoing dual sublingual immunotherapy. J. Allergy Clin. Immunol. 2012, 130, 215–224.e7. [Google Scholar] [CrossRef] [Green Version]
- Figge, D.A.; Jaunarajs, K.L.E.; Standaert, D.G. Dynamic DNA Methylation Regulates Levodopa-Induced Dyskinesia. J. Neurosci. 2016, 36, 6514–6524. [Google Scholar] [CrossRef] [Green Version]
- Kuo, H.-C.; Hsu, Y.-W.; Wu, M.-S.; Chien, S.-C.; Liu, S.-F.; Chang, W.-C. Intravenous immunoglobulin, pharmacogenomics, and Kawasaki disease. J. Microbiol. Immunol. Infect. 2016, 49, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Newburger, J.W.; Takahashi, M.; Gerber, M.A.; Gewitz, M.H.; Tani, L.Y.; Burns, J.C.; Shulman, S.T.; Bolger, A.F.; Ferrieri, P.; Baltimore, R.S.; et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Statement for Health Professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation 2004, 110, 2747–2771. [Google Scholar] [CrossRef] [Green Version]
- Huang, E.-Y.; Chang, J.-C.; Chen, H.-H.; Hsu, C.-Y.; Hsu, H.-C.; Wu, K.-L. Carcinoembryonic antigen as a marker of radioresistance in colorectal cancer: A potential role of macrophages. BMC Cancer 2018, 18, 321. [Google Scholar] [CrossRef] [Green Version]
- Makata, H.; Ichiyama, T.; Uchi, R.; Takekawa, T.; Matsubara, T.; Furukawa, S. Anti-inflammatory effect of intravenous immunoglobulin in comparison with dexamethasone in vitro: Implication for treatment of Kawasaki disease. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2006, 373, 325–332. [Google Scholar] [CrossRef]
- Chang, L.; Guo, M.M.; Yan, J.; Huang, Y.; Lo, M.; Kuo, H. Low FCMR mRNA expression in leukocytes of patients with Kawasaki disease six months after disease onset. Pediatr. Allergy Immunol. 2020, 31, 554–559. [Google Scholar] [CrossRef]
- Basu, S.K.; Pradhan, S.; Jacobs, M.B.; Said, M.; Kapse, K.; Murnick, J.; Whitehead, M.T.; Chang, T.; du Plessis, A.J.; Limperopoulos, C. Age and Sex Influences Gamma-aminobutyric Acid Concentrations in the Developing Brain of Very Premature Infants. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Huang, L.-H.; Kuo, H.-C.; Pan, C.-T.; Lin, Y.-S.; Huang, Y.-H.; Li, S.-C. Multiomics analyses identified epigenetic modulation of the S100A gene family in Kawasaki disease and their significant involvement in neutrophil transendothelial migration. Clin. Epigenetics 2018, 10, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.-H.; Chen, K.-D.; Lo, M.-H.; Cai, X.-Y.; Chang, L.-S.; Kuo, Y.-H.; Huang, W.-D.; Kuo, H.-C. Decreased DNA methyltransferases expression is associated with coronary artery lesion formation in Kawasaki disease. Int. J. Med. Sci. 2019, 16, 576–582. [Google Scholar] [CrossRef] [Green Version]
- Chang, L.-S.; Lin, Y.-J.; Yan, J.-H.; Guo, M.M.-H.; Lo, M.-H.; Kuo, H.-C. Neutrophil-to-lymphocyte ratio and scoring system for predicting coronary artery lesions of Kawasaki disease. BMC Pediatr. 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Li, S.-C.; Chan, W.-C.; Huang, Y.-H.; Guo, M.M.-H.; Yu, H.-R.; Huang, F.-C.; Kuo, H.-C.; Kuo, H.-C. Major methylation alterations on the CpG markers of inflammatory immune associated genes after IVIG treatment in Kawasaki disease. BMC Med. Genom. 2016, 9 (Suppl. 1), 37. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-C.; Shen, C.-T.; Wang, N.-K.; Huang, Y.-L.; Chiu, H.-H.; Chen, C.-A.; Chiu, S.-N.; Lin, M.-T.; Wang, J.-K.; Wu, M.-H. High Sensitivity C Reactive Protein (hs-CRP) in Adolescent and Young Adult Patients with History of Kawasaki Disease. Acta Cardiol. Sin. 2015, 31, 473–477. [Google Scholar]
- Chantasiriwan, N.; Silvilairat, S.; Makonkawkeyoon, K.; Pongprot, Y.; Sittiwangkul, R. Predictors of intravenous immunoglobulin resistance and coronary artery aneurysm in patients with Kawasaki disease. Paediatr. Int. Child Health 2018, 38, 1–4. [Google Scholar] [CrossRef]
- Li, X.; Chen, Y.; Tang, Y.; Ding, Y.; Xu, Q.; Sun, L.; Qian, W.; Qian, G.; Qin, L.; Lv, H. Predictors of intravenous immunoglobulin-resistant Kawasaki disease in children: A meta-analysis of 4442 cases. Eur. J. Nucl. Med. Mol. Imaging 2018, 177, 1279–1292. [Google Scholar] [CrossRef] [Green Version]
- Matsubara, T.; Ichiyama, T.; Furukawa, S. Immunological profile of peripheral blood lymphocytes and monocytes/macrophages in Kawasaki disease. Clin. Exp. Immunol. 2005, 141, 381–387. [Google Scholar] [CrossRef]
- Furukawa, S.; Matsubara, T.; Yabuta, K. Mononuclear cell subsets and coronary artery lesions in Kawasaki disease. Arch. Dis. Child. 1992, 67, 706–708. [Google Scholar] [CrossRef]
- Lee, H.K.; Kim, D.S.; Noh, G.W.; Lee, K.Y. Effects of intravenous immune globulin on the peripheral lymphocyte phenotypes in Kawasaki disease. Yonsei Med. J. 1996, 37, 357–363. [Google Scholar] [CrossRef] [Green Version]
- Hall, P.D. Immunomodulation with intravenous immunoglobulin. Pharmacother. J. Hum. Pharmacol. Drug Ther. 1993, 13, 564–573. [Google Scholar]
- Bonnerot, C.; Daëron, M.; Varin, N.; Amigorena, S.; Hogarth, P.M.; Even, J.; Fridman, W.H. Methylation in the 5’ region of the murine beta Fc gamma R gene regulates the expression of Fc gamma receptor II. J. Immunol. 1988, 141, 1026–1033. [Google Scholar]
- Bonnerot, C.; Choukroun, V.; Marloie, M.A.; Fridman, W.H. Two distinct regions of the mouse beta Fc gamma R gene control its transcription. Immunobiology 1992, 185, 222–234. [Google Scholar] [CrossRef]
- Lei, W.-T.; Lin, C.-Y.; Kao, Y.-H.; Lee, C.-H.; Lin, C.-H.; Shyur, S.-D.; Yang, K.-D.; Chen, J.-H. The risk of hospitalization for respiratory tract infection (RTI) in children who are treated with high-dose IVIG in Kawasaki Disease: A nationwide population-based matched cohort study. PeerJ 2018, 6, e4539. [Google Scholar] [CrossRef]
- Wang, L.-J.; Kuo, H.-C. Cognitive Development After Kawasaki Disease—Clinical Study and Validation Using a Nationwide Population-Based Cohort. Circ. J. 2018, 82, 517–523. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A | |||
| Kawasaki Disease n = 76 | Controls n = 40 | p | |
| Age | 1.79 ± 0.14 | 2.29 ± 0.26 | 0.10 |
| Gender Female/male | 34/42 | 19/21 | 0.78 |
| Data are presented as mean with standard errors. | |||
| B | |||
| Diagnosis | Number | Diagnosis | Number |
| Low respiratory infection/bronchitis, bronchiolitis | 6 | Acute gastritis | 1 |
| Low respiratory infection/pneumonia, bronchopneumonia | 10 | Rotavirus infection | 1 |
| Upper respiratory infection/tonsillitis, pharyngitis | 5 | Bacteremia | 1 |
| Influenza A | 1 | Urinary tract infection | 1 |
| Acute otitis media | 3 | Acute enteritis with salmonella infection | 1 |
| Acute sinusitis | 4 | Hand-foot-mouth disease | 1 |
| Croup | 1 | Infectious mononucleosis | 1 |
| Acute mastoiditis | 1 | Herpetic gingivostomatitis | 1 |
| Acute arthritis | 1 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, L.-S.; Yu, H.-R.; Chu, C.-L.; Chen, K.-D.; Huang, Y.-H.; Guo, M.M.-H.; Weng, K.-P.; Kuo, H.-C. Long-Term Hypermethylation of FcγR2B in Leukocytes of Patients with Kawasaki Disease. J. Clin. Med. 2021, 10, 2347. https://doi.org/10.3390/jcm10112347
Chang L-S, Yu H-R, Chu C-L, Chen K-D, Huang Y-H, Guo MM-H, Weng K-P, Kuo H-C. Long-Term Hypermethylation of FcγR2B in Leukocytes of Patients with Kawasaki Disease. Journal of Clinical Medicine. 2021; 10(11):2347. https://doi.org/10.3390/jcm10112347
Chicago/Turabian StyleChang, Ling-Sai, Hong-Ren Yu, Chiao-Lun Chu, Kuang-Den Chen, Ying-Hsien Huang, Mindy Ming-Huey Guo, Ken-Pen Weng, and Ho-Chang Kuo. 2021. "Long-Term Hypermethylation of FcγR2B in Leukocytes of Patients with Kawasaki Disease" Journal of Clinical Medicine 10, no. 11: 2347. https://doi.org/10.3390/jcm10112347